Brazilian
Journal
of
OTORHINOLARYNGOLOGY
www.bjorl.org
REVIEW
ARTICLE
Review
of
experimental
models:
sinusitis
in
rabbits
夽
,
夽夽
André
Coura
Perez
a,b,
Guilherme
Pietrucci
Buzatto
b,c,
Ivan
de
Picole
Dantas
b,d,
João
Vicente
Dorgam
b,
Fabiana
Cardoso
Pereira
Valera
e,
Edwin
Tamashiro
e,
Wilma
Terezinha
Anselmo
Lima
e,∗aFundac¸ãoArnaldoVieiradeCarvalho,FaculdadedeCiênciasMédicasdaSantaCasadeSãoPaulo(FCMSCSP),SãoPaulo,SP,Brazil bFaculdadedeMedicinadeRibeirãoPreto(FMRP),UniversidadedeSãoPaulo(USP),RibeirãoPreto,SP,Brazil
cHospitaldasClínicas,FaculdadedeMedicinadeRibeirãoPreto(FMRP),UniversidadedeSãoPaulo(USP),RibeirãoPreto,SP, Brazil
dIrmandadedeMisericórdiadeCampinas,Campinas,SP,Brazil
eDepartmentofOphthalmology,OtorhinolaryngologyandHeadandNeckSurgery,FaculdadedeMedicinadeRibeirãoPreto (FMRP),UniversidadedeSãoPaulo(USP),RibeirãoPreto,SP,Brazil
Received28January2014;accepted23March2014 Availableonline22July2014
KEYWORDS Sinusitis; Rabbits; Polyps
Abstract
Introduction:In order to better understand the pathophysiology of rhinosinusitis, several attemptshavebeenmadetocreatethediseaseinananimalmodel.Amongthestudiedrodents eachhasitsadvantagesanddisadvantages.Rabbitsareconsideredmoreappropriateforstudies thatrequiresurgicalmanipulationorinvasiveprocedures.
Objectives: Toevaluatethemostviableexperimentalmodelofrhinosinusitisinrabbitstobe adoptedinfuturestudies.
Methods:Anelectronicsearchforstudieswithexperimentalmodelsofrhinosinusitisinrabbits publishedinEnglishandPortuguesebetweenJulyof1967andJanuaryof2013wasconductedin Medline,PubMed,Cochrane,andCAPESdatabases,usingthekeywords‘‘sinusitis’’,‘‘rabbits’’, and‘‘polyps’’.
Results:Atotalof256studieswereretrieved,butinaccordancewiththeinclusionand exclu-sioncriteria,onlytenstudieswereselected.Manydifferentmethodsofresponseassessment wereusedinthesestudies.
Conclusion: Todate, thereisnoidealexperimentalmodelforinductionofacuteorchronic rhinosinusitisinrabbits,buttherhinogenicmodelappearstobethemostviableoptionforthe continuityofstudiesofthedisease.
© 2014Associac¸ãoBrasileira de Otorrinolaringologiae CirurgiaCérvico-Facial. Publishedby ElsevierEditoraLtda.Allrightsreserved.
夽 Pleasecitethisarticleas:PerezAC,BuzattoGP,DantasIP,DorgamJV,ValeraFC,TamashiroE,etal.Reviewofexperimentalmodels:
sinusitisinrabbits.BrazJOtorhinolaryngol.2014;80:435---40.
夽夽Institution:FaculdadedeMedicinadeRibeirãoPretodaUniversidadedeSãoPaulo,RibeirãoPreto,SP,Brazil. ∗Correspondingauthor.
E-mail:[email protected](W.T.A.Lima).
http://dx.doi.org/10.1016/j.bjorl.2014.07.011
1808-8694/©2014Associac¸ão Brasileirade OtorrinolaringologiaeCirurgiaCérvico-Facial.Published byElsevierEditoraLtda.Allrights
PALAVRAS-CHAVE Sinusite;
Coelhos; Pólipos
Revisãodosmodelosexperimentais:sinusiteemcoelhos
Resumo
Introduc¸ão:Comoformadetornarpossíveloentendimentodafisiopatologiadarinossinusiteé fundamentalatransposic¸ãodadoenc¸aemanimais.Oscoelhossão,dentreosroedores estu-dados,osanimaisconsideradosmaisadequadosparaoestudoqueexijamanipulac¸ãocirúrgica ouprocedimentosinvasivos.Cadamodeloexperimentaltemseuspontosfavoráveise desfa-voráveis.
Objetivo:Avaliar,emcoelhos,omodeloexperimentalderinossinusitemaisviávelaseradotado emestudosfuturos.
Método: Foirealizadabuscaeletrônicadeestudoscommodelosexperimentaisderinossinusite emcoelhosusandoaspalavras-chave(sinusite/coelhos/pólipos)eminglêseportuguêsnas prin-cipaisbasesdedadoseletrônicas:Medline,PubMed,CochraneeCAPES,publicadosnoperíodo dejulhode1967ajaneirode2013.
Resultados: Foramencontrados 256 artigos, mas de acordo comos critérios de inclusão e exclusão apenas 10 foramselecionados. Muitosmétodos distintos deavaliac¸ão de resposta foramutilizadosnessesestudos.
Conclusão:Nãoexiste,atéomomento,ummodeloexperimentalidealparaainduc¸ãode rinoss-inusiteagudaoucrônicaemcoelhos,porémomodelorinogênicopareceserapropostamais viávelparaacontinuidadedosestudossobreadoenc¸a.
©2014Associac¸ãoBrasileira deOtorrinolaringologiaeCirurgiaCérvico-Facial.Publicadopor ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Chronic rhinosinusitis (CRS) is one of the most common health problems in the world, with significant medical costs.AccordingtoBhattacharyya,thecostofCRS/yearper patientisaround$1539US,accountingfor4.8daysof absen-teeism. In the United States, approximately135 of every 1000 people, or 31 million individuals, are affected each year,withatotalcostof$6billion.1---3
ThepathophysiologyofCRSremainsuncleartodate,and themostacceptedhypothesisisofamultifactorialchronic inflammatorydisease,withprobablegeneticpredisposition. Some relatedfactors include: biofilms, osteitis,allergies, immunedisorders,intrinsicupperairwayfactors, superanti-gensofStaphylococcusaureus,fungalcolonization-induced eosinophilicinflammation,andmetabolicdisorders,suchas hypersensitivitytoacetylsalicylic acid.3Itis believedthat
severalinflammatorypatternsareinvolved,someofwhich canunfavorablyinfluencepostoperativeprognosis.3,4
In order to better understand the pathophysiology of acuteand chronic rhinosinusitis, severalattempts to cre-aterhinosinusitisin animal modelshave been reportedin theliterature.Studieswithrodentsarethemostfrequent; thepathophysiologyintheseanimalsmaybesimilarsince boththeiranatomyandnasalphysiologyresemblethatseen inhumans.5
Among the studied rodents, rabbits, guinea pigs, and albino Wistar and Sprague-Dawley rats are the most fre-quent; the first is considered more suitable for studies involvingsurgeryorotherinvasiveprocedures.5
StudiestoinduceanexperimentalmodelofCRSsuggest maneuverssuchasobliterationofnasalfossaanddrainage ofsinusostia,instillationofinflammatoryprocessmediators
intotheparanasalsinuses,andplacementofmaterialsthat act asaculture mediumin thenasal passages.6,7In
addi-tionto theseaseptic methods, therearestudies that use invivoinoculationofinfectiousfungal,bacterial,andviral agents.6,7
Each modelhas itsfavorable and unfavorableaspects. However,thereisnoconsensusonwhatwouldbetheideal modeltouseinexperimentalstudies.
This study aimed to identify the most viable experi-mental model of induced rhinosinusitis in rabbits to be recommendedforfutureresearchonacuteandchronic rhi-nosinusitis.
Materials
and
methods
Ethicalconsiderations
ThisstudywasapprovedbytheEthicsCommitteeonAnimal Experimentation,ProtocolNo.132/2010.
Literaturesearch
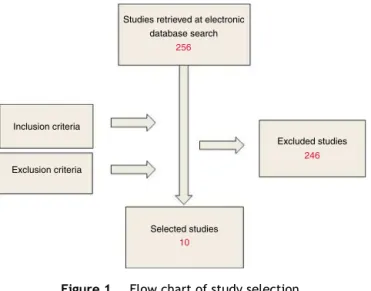
Studies retrieved at electronic database search
256
246
10
Inclusion criteria
Exclusion criteria
Excluded studies
Selected studies
Figure1 Flowchartofstudyselection.
Studyselection
Prospectivestudiesthatincludedsomeexperimentalmodel forinductionofacuteorchronicrhinosinusitiswithoriginal methodologypublishedin Englishand/or Portuguese were included. Publications in languages other than English or Portuguesewereexcluded.Studieswithrepeated method-ologies in other publications were also excluded. A total of 256 articles were retrieved in the Medline/PudMed databases,andtwowereretrievedintheLilacsdatabase; accordingtotheinclusionandexclusioncriteria,tenstudies wereselected(Fig.1).
Datacollection
Materialsandmethodsusedintheinductionofrhinosinusitis andtheassessmentoftheresponse,aswellasresults,were analyzedandareshownbelow.
The selected studies assessed the response to several stimuliinthedevelopmentofacuteandchronic rhinosinusi-tis.Sincetheperiodduringwhichthestudieswerepublished waslong(1941---2010),manydifferentmethodsforresponse assessment were found, including themacroscopic obser-vationof thepresenceofsecretions and/orinflammation, histologicalandmicrobiological analysis,analysisofblood flow in the tissue,and more modern techniques, such as opticaland electron microscopyandendoscopy. The time periodofevaluationbeforethedevelopmentofsignsof rhi-nosinusitis[RS(+)orabsenceofsignsRS(−)]rangedfrom
fivedaysto16weeks.
Results
Hilding8studiedfourgroups,withthreesubjectseach,and
acontrol group,withsix subjects.Group Iwassubmitted toenlargementofthenaturalostiuminthemaxillarysinus. In Group II, awindow was created in the medial floorof thesinus;inGroupIII,amedialandupperwindow;andin GroupIV,awindowwascreatedintheanteriorrecessofthe maxillarysinus(Table1).
Macroscopic parameters, such as patency of the cre-ated ostium and presence of secretion were analyzed.
Table 1 Incidence ofrhinosinusitis in the groups ofthe studybyHilding(1941).
GroupI:wideningofnaturalostium 3RS(+)/0RS(−)
GroupII:windowinthemedialsinus floor
2RS(+)/1RS(−)
GroupIII:medialandupperwindow 0RS(+)/3RS(−)
GroupIV:windowintheanterior recess
0RS(+)/3RS(−)
Control 0RS(+)/6RS(−)
RS,rhinosinusitis.
Throughdissection,theysoughttoidentifysignsofmucosal inflammationandbonethickening.Thewindowscreatedby enlargementofthenaturalostiumandnearthesinusfloor showedmoresignificantinflammationthanthosecreatedin theanteriorandupperportions.
Maeyama9 evaluated two groups, both with 38
sub-jects.Group I receivedintradermal albumin and albumin withStaphylococcusaureusinthemaxillarysinus.GroupII receivedthesamecombinationofGroupI,butwiththe addi-tionofproteolyticenzymeinthemaxillarysinus(Table2).
Inthisreport,macroscopicanalysiswasconductedafter twoweeksand,withtheaidofopticalmicroscopy,the pres-enceof eosinophilicinfiltration, goblet cells, and overall degreeofepithelialdegenerationwerealsoassessed. Elec-tronmicroscopy wasusedtoanalyze the degenerationof theciliarylayer.
Accordingtotheassessedparameters,thereweresigns ofacutediseaseinthemaxillarysinussamplesfromGroup I,buttheadministrationofproteolyticenzymeinGroupII decreasedmacroscopicandcellulardamage,suggestingthat thegreatertheamountofproteolyticenzymes,thegreater thedamagereduction.
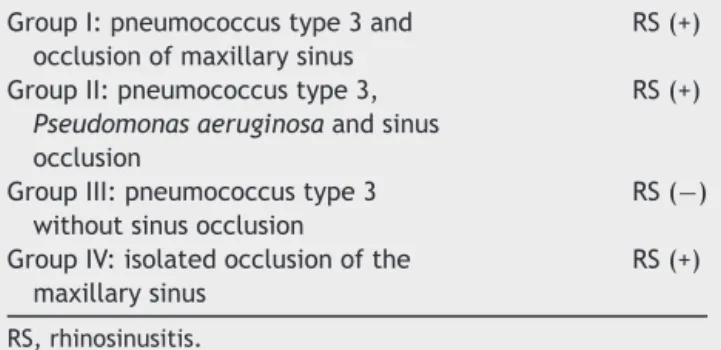
Drettneretal.10 analyzedtheassociationbetween
bac-terialinoculationandocclusionofthenaturalostiuminthe maxillary sinuses in four distinct groups. Group I (n=17) received type 3 Pneumococcus and subsequently under-went maxillary sinus occlusion. Group II (n=10) received type 3 Pneumococcus and Pseudomonas aeruginosa, and, subsequently,underwent maxillary sinus occlusion. Group III (n=12) received type 3 Pneumococcus, without sinus occlusion,and Group IV (n=25) underwent isolated sinus occlusion(Table3).
Macroscopicappearance,histology,andbloodflowwere evaluatedfive days after the initial procedures. Bacteria were found in all groups, even in Group IV, which was notinoculatedwithbacteria.Signsofsinuspathologywere presentinallsamplesthatunderwentsinusocclusion,but innone without the occlusion. Therefore,the association
Table 2 Incidenceofrhinosinusitesinthegroups ofthe studybyMaeyama(1981).
GroupI:albumin+Staphyloccocus aureus
RS(+)
GroupII:albumin+Staphyloccocus aureus+proteolyticenzyme
RS(−)
Table3 Incidence ofrhinosinusitis in the groups ofthe studybyDrettneretal.(1987).
GroupI:pneumococcustype3and occlusionofmaxillarysinus
RS(+)
GroupII:pneumococcustype3,
Pseudomonasaeruginosaandsinus occlusion
RS(+)
GroupIII:pneumococcustype3 withoutsinusocclusion
RS(−)
GroupIV:isolatedocclusionofthe maxillarysinus
RS(+)
RS,rhinosinusitis.
Table4 Incidence ofrhinosinusitis in the groups ofthe studybyMarks(1997).
GroupI:polyvinylsponge+S.pneumoniae 83%RS(+) GroupII:control(nosponge) RS(−)
RS,rhinosinusitis.
of inflammation with procedures that occluded the sinus ostiumwashigherthanthatofthenon-occlusionprocedure. Hinnieetal.11 performed earlyassessmentofthe
max-illarysinus afternaturalostium occlusion.They compared theinoculationofbacteriaandisotonicsalinesolutioninto themaxillarysinus.Theyusedfourgroupswithfivesubjects each. Group I was submitted to the introduction of iso-tonicsalinepriortosinusocclusion,GroupIIwasinoculated withStreptococcuspneumoniae,GroupIIIwithHaemophilus influenzae,andGroupIVwithP.aeruginosa.
Usingelectron microscopytheyanalyzed ciliarymotion andhaircelldestruction.Salinesolution,evenwhen associ-atedwithsinusocclusion,didnotinducefunctionallossof ciliarymotionortissueinjuryasdidthesamplesinoculated withbacteria.
Marks12introducedapolyvinylspongeimpregnatedwith
pathogenicbacteria(S.pneumoniae)inthenasalcavityof rabbits;acombination ofmacroscopicand bacteriological analysiswasperformedonetotenweeksafterthis proce-dure.Signsofinflammationinsinusalmucosawerefoundin 83%of histological samplesand in over 50% of thecases, bacteria were identified after one week. The inflamma-tory response was greater in the first two weeks of the experiment, and the control group showed no significant alterations(Table4).
Cetinetal.13alsousedamodelofpolyvinylintroduction
inthenasalcavityofrabbits,andemployedfive-inchlong cathetersoftwodifferentdiameters(8and12mmFrench). Theauthors studiedtwogroups throughmacroscopic, his-tological,tomographic,andbacteriologicalanalysisatone, two,andfourweeks(Table5).
Table5 Incidence ofrhinosinusitis in the groups ofthe studybyCetinetal.(2002).
GroupI:catheter12Fr. 8RS(+)/1RS(−)
GroupII:catheter8Fr. 5RS(+)/4RS(−)
RS,rhinosinusitis;Fr.,French.
Table 6 Incidenceof rhinosinusitis in thegroups ofthe studybyDufouretal.(2005).
GroupI:A.fumigatus RS(−)
GroupII:A.fumigates+mucosallesion RS(+)20% GroupIII:A.fumigates+sinusocclusion RS(+)57%
RS,rhinosinusitis.
Escherichiacoliwasthemostcommonlyfound microor-ganism in thefirst week, but other pathogens, such asP. aeruginosa, Proteus sp., and Enterococcus sp., appeared insubsequentweeks.Macroscopicfindingswerecorrelated withcomputedtomography (CT)findingsinallcases.High ratesofasevereinflammatoryresponsewereobservedwith therhinogenicmodel.Thenumberofpositivesampleswas greaterwiththelargerdiametercatheter.
Dufouretal.14 triedtoinducethedevelopmentof
fun-gal sinusitis in the maxillary sinus, by the inoculation of Aspergillusfumigatusintothreegroupsofanimals.InGroup I(n=10),onlythefunguswasinoculated;inGroupII(n=10), mucosaldamagewasinducedandthefunguswasinoculated intheinjuredarea;andinGroupIII(n=17),thefunguswas inoculatedandthedrainageostiumwasoccluded(Table6). The evaluationwasperformed throughbacteriological, mycological, endoscopic,andhistologicalanalysis 30days aftertheinitialprocedure.Samplesinoculatedwithfungus alonedidnotshowthesameresultsoftheinoculated sam-plesthatweresubmittedtomucosalinjuryorsinusalostium occlusion, which showed positivity rates of 20% and 57%, respectively.
Costaetal.5studiedfourgroupsofrabbits,eachwithfive
subjects. Procedures were performed toelicit an inflam-matory responsein oneof the maxillary sinuses, and the contralateralsinuswasusedasacontrol.InGroupI,a sec-tionof spongebath wasintroduced into thenasal cavity; in Group II, cyanoacrylate was instilled in the infundibu-lumforocclusionofthemaxillarysinusostium;inGroupIII, theperipheralbloodoftheanimalitselfwaspercutaneously manipulatedinthemaxillarysinus;andinGroupIV,a prepa-rationofstaphylococcalandstreptococcaltoxoidwasused (Table7).
After15days,thepresenceofhistologicalsignsof inflam-mation wasassessed. Significant results were observed in allgroups,exceptthecontrol,butthemostintense inflam-mationwasfoundinthesamplessubmittedtospongebath introductionintothenasalcavity.
Liang et al.15 introduced Merocel® sponge (Medtronic,
Xomed) in one of the nasal cavities of two groups of rabbits for a period of two weeks. In Group I, Merocel®
wasintroducedintooneofthenasalcavities;theopposite
Table 7 Incidenceof rhinosinusitis in thegroups ofthe studybyCostaetal.(2007).
GroupI:bathsponge RS(+)/intenseinflammation GroupII:cyanoacrylate RS(+)/moderateinflammation GroupIII:peripheralblood RS(+)/slightinflammation GroupIV:toxoids RS(+)/slightinflammation Maxillarysinuses---controls RS(−)
Table8 Incidenceofrhinosinusitis inthe groups of the studybyLiangetal.(2008).
GroupI:Merocel® RS(+)50% GroupII:Merocel®+PMA RS(+)60---70% Controlgroup:contralateral
maxillarysinuses
RS(+)16%
PMA,phorbolmyristateacetate.
sidewasleftunalteredasacontrol.InGroupII, thesame protocol wasperformed after each nasal cavity hadbeen treatedwithphorbolmyristateacetate(PMA),abiologically activecompoundcapableofactivatingproteinkinaseCand altering cellpermeability. The authors usedmacroscopic, endoscopic,CTmandmicrobiologicalanalysisat12and16 weeks(Table8).
ThepresenceofMerocel®inducedsignsofan
inflamma-toryresponsein50%of samplesthatreceivednoPMAand upto70% of thosethatreceived it.Only 16%of the con-trol paranasal sinuses showed an inflammatory response. Between the 12th and 16th weeks, the authors initiated treatmentwithintravenousceftriaxonerandomizedtohalf of the rabbits showing signs of rhinosinusitis. Those that receivedtreatmentshowedsignsofresolutionoftheclinical picturecomparedtothosethatdidnotreceiveceftriaxone (p=0.00043),demonstratingtreatmentefficacy.
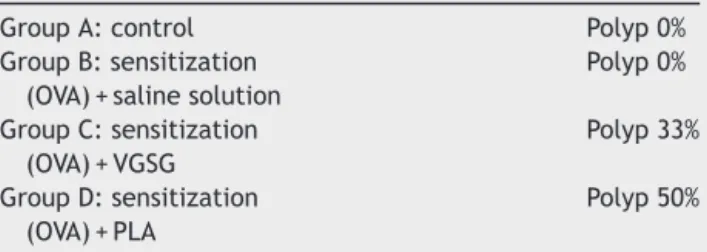
Sejimaetal.16evaluatedfourgroupsofanimalsand
pro-posedamodelforinductionofeosinophilicpolyps.GroupA was a control group and consisted of four rabbits (n=4), whereas Groups B---D had six rabbits each. In that study, the rabbits fromGroups B---D weresensitized by subcuta-neousinjectionofovalbumin(OVA)ondays0and7;onday 14,theyweresubmittedtoasurgicalproceduretoocclude thedrainageostiumofthemaxillarysinus.Twoweeksafter obstruction of theostium, they oncemorereceived oval-bumin directly into the maxillary sinuses, three times a weekfortwoweeks,followedbyinjectionofsalinesolution in GroupB;saline with40g/mLof valine-glycine-serine-glutamicacid (VGSG) wasinjectedin Group C;and saline solutionwithpoly-l-arginine(PLA)wasinjectedinGroupD, allthreetimesaweekforfourweeks(Table9).
Twenty-four hours after the last administration of polyp-inducing agents, the rabbits were euthanized for histopathological assessment of the left maxillary sinus mucosa using hematoxylin and eosin; the right maxillary sinus mucosa was subjected to genetic assessment. It was observed that Groups A and B did not exhibit polyp
Table9 Incidenceofrhinosinusitis inthe groups of the studybySejimaetal.(2010).
GroupA:control Polyp0% GroupB:sensitization
(OVA)+salinesolution
Polyp0%
GroupC:sensitization (OVA)+VGSG
Polyp33%
GroupD:sensitization (OVA)+PLA
Polyp50%
OVA, ovalbumin; VGSG, valine-glycine-serine-glutamic acid; PLA,poly-l-arginine.
formation; large polyps were observed in two of the six rabbitsinGroupC,andmiddle-sizedpolypswereobserved inthreerabbitsfromGroupD.
GroupsCandDshowedasignificantlyincreasednumber ofeosinophils inthemucosawithGroupDexhibitingmore eosinophilsthanGroupC.Athickenedlaminapropriaofthe animalsinGroup D comparedtoGroupsAand Bwasalso noted,butitwasnotsignificantlydifferentthanthatofthe animalsofGroupC.Thus,theauthorscreatedan experimen-talmodelforinduction ofeosinophilicpolyps thatmaybe appropriateforthestudyofchronicrhinosinusitisinhumans.
Discussion
Thecurrentdifficultyinunderstandingthepathophysiology of chronic rhinosinusitis is evident. Potential pathological agentsandseveralothercausalfactorsaredescribedinthe literature every day, making the study of new therapeu-ticalternativescrucial.Studiesonnewdrugsareextremely importantandneedreliableexperimentalmodels.
Theanalysisofsomeofthemainstudiesonexperimental modelspublishedover the yearsallowed us tomake sev-eralobservations.Perhapsduetothetechnicaldifficulties inherentinthelong-termanimalsresearch,mostofthese studiespresentmodelsofacuterhinosinusitis,andonlythe study by Sejima et al.16 for the induction of eosinophilic
polypsinmaxillarysinusofrabbitshadalongertimeframe. However,theirmethodologywasextremelydifficultandthe authorsusedonlyasmallnumberofanimalsinthegroups thatsuccessfullyinducedpolypformation.
Theanalysisalsodiscoveredonlytwomainalternatives toinducesinusitisinrabbits,eachwithitsadvantagesand disadvantages.Thefirstconsistedofintroducingculturesof bacteria,fungi, or other inducingagents in theparanasal sinusesbypercutaneousinjection,orthroughasurgical pro-cedurewiththe openingand exposureof themucosaand subsequentinoculationofinfectiousagents.Insomecases, thisprocedurewasassociatedwithocclusionofthedrainage ostiumoftheparanasalsinuses.
Theocclusionofsinusesinoculatedwithbacteriaorfungi wasasuperiormethodcomparedtotheisolatedpathogen inoculation,10,12,14 therefore confirming thatalterations of
thenasal fossaand itscommunication withtheparanasal sinuseshaveadecisiveroleintheoriginofrhinosinusitis.
The studiesthat performedearly analyses,suchasthe studybyHinni,11 didnotclearlydemonstratethe
superior-ityofa particular methodof sinus occlusion.Perhapsthe processesthatcharacterizethedevelopmentof rhinosinusi-tisinoccludedsinusesrequirealongertimeofexposureto thestimulus.
Thesecondmethod,termed‘‘rhinogenicrhinosinusitis’’, is generated by the introduction of foreign bodies in the nasalcavitiesofrabbits.Thismethod,asitroutinelyoccurs withforeign bodiesin the nasalcavities of children, was responsiblefortheappearanceofabundantpurulent rhinor-rheainmostsamplesintheevaluatedstudies.Obstructionof thenasalcavityandformationofpurulentsecretionresulted innasalsinusinvolvement.5,12,13,15
Bathsponges,fragmentsofpolyvinyl,cyanoacrylate,and evenMerocel® catheters were amongthematerials used.
total occlusion of the nasal cavity, as well as placement restrictedtotheinfundibular region.Foreignbodieswere highlyeffectiveininducingtheonsetofsignsof inflamma-tionandrhinosinusitis.
Bothmethodsproposeaninterventioninsinonasal phys-iologyof rabbits,but the rhinogenic modelwas shown to bemorepracticalandeasiertoperform.Thehighresponse rateswithintenseinflammation5suggestahigh
reproducibil-ityofthemethod,averydesirablefactorinexperimental models.
Standardization of the technique tointroduce the for-eignmaterial,aswellasthedimensionsandtheexposure time,arethenextstepstobetakeninordertoattaina reli-ableandeasilyreproducibleexperimentalmodel;thiswill facilitateimportantadvancesinrhinosinusitisresearchand bettercomparisonparametersbetweenstudies.
Theremovalofmaterialfromtherabbitmaxillarysinus for post-study examination is a simple procedure, espe-cially with the use of decalcification and paraffin-block embedding.16 The rhinogenic method reversibility
proce-dureperformedbyLiangetal.15presentsthepossibilityof
usingittostudynewdrugs.
The model of pathogen introduction and complemen-tary procedures, such as mucosal lesions or occlusion of drainageostia,hastheadvantageofallowingthestudyof specific pathogens. However, the need for surgical viola-tionofthesinuses tointroducethepathogens constitutes amajordisadvantage,sinceit caninfluenceinflammatory response-inducing factors. The rhinogenic models (intro-duction of foreignbodies intothe nasal cavities) areless expensive, require less complex laboratory facilities, and do not depend on invasive procedures to be performed. Moreover,theyaremoreeasilyimplementedandarehighly reproducible.
Conclusion
To date, there is no ideal experimental model to induce acuteorchronicrhinosinusitisinrabbits,buttherhinogenic modelappearstobethemostviableproposalforthe con-tinuationofstudiesonthedisease,basedonourliterature review.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.BenningerMS,FergusonBJ,HadleyJA,HamilosDL,JacobsM, Kennedy DW, et al. Adultchronic rhinosinusitis: definitions, diagnosis,epidemiology,andpathophysiology.OtolaryngolHead NeckSurg.2003;129:S1---32.
2.Bhattacharyya N. The economic burden and symptom man-ifestations of chronic rhinosinusitis. Am J Rhinol. 2003;17: 27---32.
3.Fokkens W, Lund V, Mullol J. European Position Paper on Rhinosinusitis and Nasal Polyps group. European position paperon rhinosinusitis and nasal polyps 2007. Rhinol Suppl. 2007;20:1---136.
4.VoegelsRL, de Melo PaduaFG. Expression ofinterleukins in patients with nasal polyposis. Otolaryngol Head Neck Surg. 2005;132:613---9.
5.CostaHO,RuschieLuchiGE,AugustoAG,CastroM,deSouza FC.Comparativestudyofseveralsinusitisexperimental mod-ellingtechniquesinrabbits.BrazJOtorhinolaryngol.2007;73: 627---31.
6.Schenkel EP, Simões CMO, MengueSS, Mentz LA, IrgangBE, StehmannJR.Oespac¸odasplantasmedicinaisesuasformas derivadasnamedicinacientífica.CadFarm.1985;1:65---72.
7.KrouseJH,KrouseHJ.Patientuseoftraditionaland comple-mentarytherapiesintreatingrhinosinusitisbeforeconsulting anotolaryngologist.Laryngoscope.1999;109:1223---7.
8.Hilding AC. Experimental sinus surgery: effects of opera-tive windows on normal sinuses. Ann Otol Rhinol Laryngol. 1941;50:379---92.
9.MaeyamaT.Astudyofexperimentalsinusitisinrabbits.Auris NasusLarynx.1981;8:87---97.
10.DrettnerB,JohanssonP,KumlienJ.Experimentalacute sinus-itisinrabbit.Astudyofmucosalbloodflow.ActaOtolaryngol. 1987;103:432---4.
11.Hinni ML, McCaffrey TV, Kasperbauer JL. Early mucosal changesinexperimentalsinusitis.OtolaryngolHeadNeckSurg. 1992;107:537---48.
12.MarksSC.Acutesinusitisintherabbit:anewrhinogenicmodel. Laryngoscope.1997;107:1579---85.
13.Cetin CB,Kara CO,Colakoglu N,Sengul M,Pinar HS. Exper-imental sinusitis in nasally catheterised rabbits. Rhinology. 2002;40:154---8.
14.DufourX,Kauffmann-LacroixC,GoujonJM,GrollierG,Rodier MH,KlossekJM.Experimentalmodeloffungalsinusitis:apilot studyinrabbits.AnnOtolRhinolLaryngol.2005;114:167---72.
15.LiangKL,JiangRS,Wang J,ShiaoJY,SuMC,HsinCH,et al. Developingarabbitmodelofrhinogenicchronicrhinosinusitis. Laryngoscope.2008;118:1076---81.