www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Characteristics
of
419
patients
with
acquired
middle
ear
cholesteatoma
夽
Letícia
Petersen
Schmidt
Rosito
a,b,∗,
Maurício
Noschang
Lopes
da
Silva
a,b,
Fábio
André
Selaimen
a,
Yuri
Petermann
Jung
c,
Marcos
Guilherme
Tibes
Pauletti
c,
Larissa
Petermann
Jung
c,
Luiza
Alexi
Freitas
c,
Sady
Selaimen
da
Costa
daHospitaldeClínicasdePortoAlegre,PortoAlegre,RS,Brazil
bUniversidadeFederaldoRioGrandedoSul(UFRGS),PortoAlegre,RS,Brazil
cUniversidadeFederaldoRioGrandedoSul(UFRGS),FaculdadedeMedicina,PortoAlegre,RS,Brazil
dUniversidadeFederaldoRioGrandedoSul(UFRGS),FaculdadedeMedicina,DepartamentodeOftalmologiae Otorrinolaringologia,PortoAlegre,RS,Brazil
Received12May2015;accepted2February2016 Availableonline3May2016
KEYWORDS
Cholesteatoma; Middleear; Bilateral; Classification; Surgery
Abstract
Introduction:Cholesteatoma is a destructive lesion that can result in life-threatening complications. Typically,itpresents withhypoacusis andcontinuous otorrheaas symptoms. Becauseitisararedisease,therearefewstudiesinBrazildescribingthecharacteristicsof patientswiththedisease.
Objective: Thisstudyaimedtodeterminetheprevalenceofcholesteatomainpatientswith chronicotitismediaanddescribeclinical,audiologicalandsurgicalcharacteristicsofpatients with acquiredmiddleearcholesteatomatreated atareferralhospital inthepublic health system.
Methods:Cross-sectional andprospective cohortstudy,including1710patients withchronic otitismedia,treatedbetweenAugust2000andJune2015,withoutpriorsurgery.Detailed clin-icalhistory,videotoscopy,andaudiometrywereperformed,inadditiontoreviewofmedical recordstosearchforsurgicaldata.Cholesteatomaswereclassifiedaccordingtotheirrouteof formation.
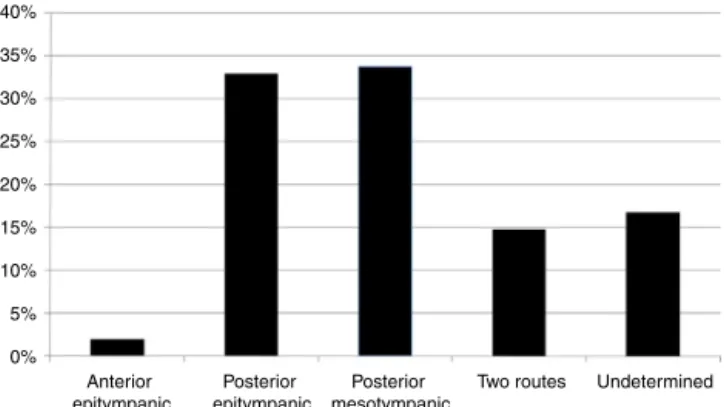
Results:Ofthepatientswithchronicotitismedia,419(24.5%)hadcholesteatoma;meanage of34.49years;53.5%femaleand63.8%adults.Bilateralcholesteatomawasobservedin17.1%. Anteriorepitympaniccholesteatomacorrespondedto1.9%;posteriorepitympanic,32.9%; pos-teriormesotympanic,33.7%;tworoutes,14.8%;andindeterminate,16.7%.Themeanair-bone
夽 Pleasecitethisarticleas:RositoLP,daSilvaMN,SelaimenFA,JungYP,PaulettiMG,JungLP,etal.Characteristicsof419patientswith acquiredmiddleearcholesteatoma.BrazJOtorhinolaryngol.2017;83:126---31.
∗Correspondingauthor.
E-mail:[email protected](L.P.Rosito).
PeerReviewundertheresponsibilityofAssociac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial.
http://dx.doi.org/10.1016/j.bjorl.2016.02.013
gap was 29.84dB and didnot differ between routes offormation. There were no correla-tionsbetweengapsizeandpatientageordurationofsymptoms.Ofthesurgicalcases,16.8% underwentclosedtympanomastoidectomyand75.2%opentympanomastoidectomy.
Conclusion: Theprevalenceofcholesteatomainpatientswithchronicotitismediawas24.5% anditwasmore commoninadultsthaninchildren.Posteriormesotympaniccholesteatoma was more frequent,with nodifference inmeanair-bonegap between thedifferent routes offormation.Inpatientsundergoingsurgery,opentympanomastoidectomywastheprocedure mostfrequentlychosen.
© 2016 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Published by Elsevier Editora Ltda. This is an open access article under the CC BY license (http:// creativecommons.org/licenses/by/4.0/).
PALAVRAS-CHAVE
Colesteatoma; Orelhamédia; Bilateral; Classificac¸ão; Cirurgia
Característicasde419pacientescomcolesteatomaadquiridodeorelhamédia
Resumo
Introduc¸ão: Colesteatomaéumalesãodestrutivaquepodedeterminarcomplicac¸ões poten-cialmenteletais.Tipicamente,apresentahipoacusiaeotorreiacontínuacomo sintomas.Por serumadoenc¸arara,existempoucosestudosnoBrasilquedescrevamascaracterísticasdos pacientesportadores.
Objetivo: Opresenteestudotevecomoobjetivosdeterminaraprevalênciadecolesteatoma entreospacientescomotite médiacrônica(OMC)edescrever característicasclínicas, audi-ológicasecirúrgicasdospacientescomcolesteatomaadquiridodeorelhamédiaatendidosem umhospitaldereferênciadosistemapúblicodesaúde.
Método: Estudotransversaledecoorteprospectivo,incluindo1.710pacientescomOMC, aten-didosentreagostode2000ejunhode2015,semtratamentocirúrgicoprévio.Foirealizada anamnesedetalhada,videotoscopiaeaudiometria,alémderevisãodeprontuáriosparabusca dedadoscirúrgicos.Oscolesteatomasforamclassificadosconformesuaviadeformac¸ão.
Resultados: Dospacientescomotitemédiacrônica,419(24,5%)apresentaramcolesteatoma. Média de idade de 34,49 anos; 53,5% do sexo feminino e 63,8% adultos. Colesteatoma foi observadobilateralmenteem17,1%.Osepitimpânicosanteriorescorresponderama1,9%;os epitimpânicosposterioresa32,9%;osmesotimpânicosposterioresa33,7%;duasviasa14,8% eindeterminadosa16,7%.Amédiatritonaldosgapsaero-ósseosfoide29,84dBenãodiferiu entreasviasdeformac¸ão.Nãoforamobservadascorrelac¸õesentretamanhodogapeidade do paciente ou durac¸ão dos sintomas. Dos pacientesoperados, 16,8% foram submetidos a timpanomastoidectomiafechadae75,2%atimpanomastoidectomiaaberta.
Conclusão:Aprevalênciadecolesteatomaempacientescomotitemédiacrônicafoide24,5%,e foimaisfrequenteemadultosdoqueemcrianc¸as.Osmesotimpânicosposterioresforammais frequentes, não sendoobservadadiferenc¸anamédia dosgaps aero-ósseosentrediferentes viasdeformac¸ão.Nospacientessubmetidosacirurgia,atimpanomastoidectomiaabertafoio procedimentoescolhido.
© 2016 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Publicado por Elsevier Editora Ltda. Este ´e um artigo Open Access sob uma licenc¸a CC BY (http:// creativecommons.org/licenses/by/4.0/).
Introduction
Cholesteatomaisconsideredabenignepitheliallesionwith agradualanddestructiveexpansion,whichaffectstheear canalandadjacentstructures.1Epithelialaccumulationand
boneerosion,characteristicofthedisease,typicallyresult in continuous otorrhea and hypoacusis. With the progres-sion of cholesteatoma, theremay also beinvolvement of the inner ear2,3 and facial nerve, in addition to serious
complicationssuchasmeningitisandbrainabscess.4
The estimated incidence in the general population is 3.7---13.9/100,000.5,6 This incidence is lower in children
(3/100,000)thaninadults(9/100,000).7Becauseitisarare
disease, epidemiological studies, especially in Brazil, are
scarce. This lack of data makes it impossible tocompare studiesperformedinBrazilwithothers,asit isnotknown whetherthepopulationsarereallysimilar.
Theobjectivesofthisstudyweretodeterminethe preva-lenceofcholesteatomainpatientswithchronicotitismedia (COM);describetheclinicalandaudiologicalcharacteristics ofpatientswithcholesteatoma;andverifythesurgical tech-niquesmostusedinareferralhospitalinthepublichealth system.
Methods
duringtheperiodfromAugust2000toJune2015attheClinic ofChronicOtitisMediaoftheHospitaldeClínicasdePorto Alegre.
The inclusion criterion for follow-up waspatients with COM with cholesteatoma diagnosed after videotoscopy. Exclusioncriteriawerehistoryofanypreviousearsurgery, except tympanostomy for placement of tympanostomy tubes, and inability to properlyclean the ears and/or to performvideotoscopyforproperdocumentation.
At thefirstassessment, adetailedmedicalhistory was taken,aswellasaclinicalexam.Aftercarefulcleaningof the ears, videotoscopy was performed with a fiber optic zero degree and 4mm telescope (Karl Stortz). Both ears wererecordedsequentiallyusingtheCyberlinkPower Direc-tor software (version 7, 2008). After the medical history andphysicalexamination,thepatientsunderwentpuretone audiometry,usingtheaudiometerInteracousticsAD27with supra-auralphonesTDH-39,fordeterminingtheair conduc-tionandboneconductionthresholds,andair-bonegap.The gap was calculated from the difference between the air andboneconductionthresholds. Broadbandmaskingnoise wasusedwhennecessary.Insmallchildren,playful condi-tionedaudiometrywasusedwithsupra-auralphones.When necessary, audiometry was completed after two sessions for confirmationof the obtained thresholds.Airway, bone conduction,andgapweredescribedbytritonalmean, calcu-latedbytheaverageofthresholdsat500,1000,and2000Hz, representingthespeechrecognitionarea.
Thevideotoscopieswereindependentlyreviewedduring aclinicalmeeting.Fortheevaluationoftheimages,specific protocolswereusedinasystematicmanner,inaccordance withthedefinitionsdescribedbelowbythesenior investi-gator.
Cholesteatomas were then classified according to the modifiedJacklerclassification,8accordingtotheirrouteof
formation:
1. Anteriorepitympanic:whenoriginatedanteriorlytothe headofthemalleus.
2. Posteriorepitympanic:whenoriginatedexclusivelyinthe parsflaccida.
3. Posteriormesotympanic:whenoriginatedexclusivelyin theposterior-superiorquadrantoftheparstensa. 4. Tworoutes:wheninvolvedboththeparsflaccidaandpars
tensa.
5. Undetermined:whenthecholesteatomarouteof forma-tioncouldnotbedeterminedbyvideotoscopyimage.
Patients aged under 18 were considered as children, accordingtothecriteriaoftheWorldHealthOrganization.
Medicalrecordsandsurgicaldescriptionsofpatientswho hadundergonesurgerywerereviewed.
The Research and Graduate Group of our institution approved the project in its ethical and scientific aspects (ProtocolNo.14918).Allpatientsincludedinthestudyhad previouslysignedan informedconsentauthorizingtheuse oftheirdataanonymouslyinthisscientificstudy.
Data were tabulated and analyzed using the SPSS software program (version 20). Statistical analysis was performedusingtheMann---Whitneytesttoevaluatethe dif-ferencebetweenthedurationof thedisease,andFisher’s exacttestforthedifferenceinprevalenceofpalataldefects
amongchildren and adults.ANOVAtest wasused to com-pare themeantritonal gapsbetweenthe differentroutes of cholesteatoma formation.Correlations wereperformed usingtheSpearmantest.p-values<0.05wereconsideredto bestatisticallysignificant.
Results
Of the 1710 patients with COM evaluated in the study, cholesteatomawaspresentin419(24.5%).Themeanageof patientswas34.49;standarddeviation(SD)19.8,and53.5% were female. White patients accounted for 86.5% of the studypopulationand5.9%wereblack.Adultscorresponded to63.8%.Cholesteatomawasidentifiedintherightearwas in234patients(55.8%).
Theprevalenceofpalatedefectsinthispopulationwas 4.3%. There was no difference in prevalence of palatal defectsbetweenchildrenandadults(3.4%vs.4.9%, respec-tively;p=0.59).
The average time from the onset of symptoms to the assessment was 13.73 years (SD=14.43). In children, the averagewas6.39yearsandmedianof6years,inadultsit wasof 17.63 yearsand medianof 12, respectively. There was a statistically significant difference between groups (p<0.001).
Theprevalenceofthedifferentroutesofcholesteatoma formationinthispopulationisshowninFig.1.Therewasno differencebetweenthedurationofsymptomsandtheroute offormation(p=0.28).
In the contralateral ear evaluation, only 150 of them (36.1%)werenormalandcholesteatomawasidentifiedin71 (17.1%). Theduration ofsymptoms waslongerin patients with changes in the contralateral ear than in those with normalcontralateralear(meanof14.99and11.69, respec-tively;p=0.007).Therewasnodifferenceintheprevalence ofcholesteatomainthecontralateralearbetweenchildren andadults(p=0.20)andbetweenpatientswithandwithout palatemalformation(p=0.19).
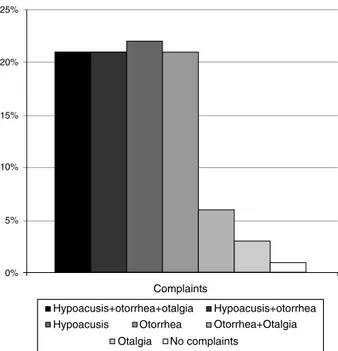
Themaincomplaintsofpatientsatthetimeofthefirst evaluationin thisserviceareshown inFig.2.Hypoacusis, withorwithoutotorrhea,wasthemaincomplaintof84.4% ofthestudypopulation,andotorrheawasobservedin87%. There were no differences regarding the main complaint whenwecomparedcholesteatomasclassifiedbytheroute offormation(p=0.27).
40%
35%
30%
25%
20%
15%
10%
5%
0%
Anterior epitympanic
Posterior epitympanic
Posterior mesotympanic
Two routes Undetermined
25%
20%
15%
10%
5%
0%
Complaints
Hypoacusis+otorrhea+otalgia Hypoacusis+otorrhea Hypoacusis Otorrhea Otorrhea+Otalgia
Otalgia No complaints
Figure2 Frequencyoftheprinciplecomplaints ofpatients withcholesteatomaatthetimeoffirstevaluation.
Among the evaluated patients, 92.41% underwent audiometry.Regardingboneconductionandairway thresh-olds,thetritonal meanwas17.08(SD)16.16dB and46.35 (SD)22.34dB,respectively.Regardinggapsizes,thetritonal mean was 29.84 (SD) 13.61. The prevalence of air-bone gap sizes in tritonal means is shown in Fig.3. There was no correlation between gap size and age of the patient atthetimeofevaluation(R=0.03;p=0.55)ordurationof symptoms(R=0.08;p=0.13).Nodifferenceswereobserved regardinggaptritonalmeanbetweenthedifferentroutesof cholesteatomaformation(p=0.13),asshowninFig.4.
Among all the patients, 205 (48.9%) had not under-gonesurgeryat thetimeofthe studyor hadbeen lostat follow-up.Ofthepatientswhounderwentsurgery,17(7.9%) underwenttympanoplasty;36(16.8%),closed tympanomas-toidectomy;and161(75.2%),opentympanomastoidectomy. Therewasnodifferenceinthe surgicaltechnique usedin childrenandadults(p=0.86).
Discussion
Descriptivestudiesoftheclinicalcharacteristicsofpatients withcholesteatoma in Brazil arescarce. Aprevious study
50% 45%
40%
35%
30%
25% 20%
15%
10%
5%
0%
Gap up to 20 dB Between 20 and 40 dB Over 40 dB
Figure3 Prevalenceoftheair-bonedifferencesizesin tri-tonalmeans.
40
35
30
25
20
15
10
5
0
Anterior epitympanic
Posterior epitympanic
Posterior mesotympanic
Two routes Undetermined
Figure4 Comparisonoftritonalmeansofair-bonegap(dB) betweenthedifferentroutesofcholesteatomaformation.
performedin thecountry, despite describinga large sam-ple of patients, was based on data and medical records collectedretrospectively,which canleadtoseveralbiases in the measurement.6 In the present study, all patients
underwent the same medical history, and the ears were cleanedand preparedfor propervideotoscopy.All images weretakenwithhighqualitytobesubsequentlyevaluated by the same senior investigator. The use of videotoscopy thereforeallowsfor better imagedefinition, better docu-mentation,andfinally,amoredetailedandaccuratedisease classification.
Inthepresentstudypopulation,therewasahigher preva-lenceofadultsthanchildren,whichcorroboratesprevious studies showing that the incidence of cholesteatomas is higherinadults.7 Hypoacusisand otorrheawerethe main
complaintsof mostpatients, and87%hadotorrhea atthe timeof evaluation. Complaints of hearing loss were con-firmedbyaudiometry,whichshowedthatthevastmajority ofpatientshadconductivehearinglosswithlargerair-bone gapof20dBinspeechrecognitionarea.
Theprevalenceof bilateralcholesteatomainthisstudy was17.1%;similartopreviousstudies.9However,wefound
nodifferencesintheprevalenceofbilateralcholesteatoma between patients with and without palatal defects or betweenchildrenandadults.Thesefindingssuggestthatthe mechanisminvolvedinthepathogenesisofcholesteatoma, initiated bythe Eustachiantube dysfunction,perpetuates withprogressiveretractionofthetympanicmembraneand increaseof gasexchangeinthe middleearcaused bythe inflammatoryprocessand,notnecessarily,bythe mainte-nanceoftheinitialdisorder.10Thus,thehighprevalenceof
bilaterality, evenin patients without palate changes, can beunderstood sinceauditory tubedisordersandsecretory otitismediaoftenaffectbothsidesinmostpatients.11,12
Posteriormesotympaniccholesteatomaswere themost frequentinthepresentpopulation,contrarytomost stud-iesreportingatticcholesteatomaasthemostprevalent.8,13
Furthermore, the documentation of anterior epitympanic cholesteatoma was very rare, and of cholesteatoma that developedconcurrentlyinboththeparstensaandpars flac-cida,whichwascalledtworoutes,correspondedto15%of cases.Inabout15%ofpatients,itwasnotpossibleto deter-mineaccuratelytherouteofcholesteatomaformationand thereforetheywereclassifiedasundetermined.
difficultiespatientswithcholesteatomahavetoaccess pub-licservice inBrazil.Althoughnocorrelation wasobserved between the duration of symptoms and the degree of conductive hearing loss, it was found that patients with changesinthecontralateralearhadbeensymptomaticfor alongertime.Accordingtootherauthorsdataregardingthe duration of disease, have poor reliability.14 They depend
on patient’s memory and often of previous symptoms of ear pain, otorrhea, or hypoacusis associated with a history of recurrent otitis media or chronic secretory otitis, which can be easily confused with the symptoms of cholesteatoma. A study by Aberg et al.15 compared
theclinical symptoms of patientswithcholesteatomatous and non-cholesteatomatous COM through a questionnaire betweentwogroupsandfoundnodifferenceinsymptoms. Thismayexplainthelargedifferenceinthemeantimefrom symptomonsetbetweenchildrenandadults,asmanyadults indicatethebeginningoftheircomplaintsinchildhood.
Palatedefectsareaknownriskfactorfor the develop-mentofcholesteatoma.Dominguezetal.16estimatedthat
the risk of cholesteatoma in a child with cleft palate is 2.6---9.2%. Spilsbrury et al.17 studied children who
under-went placement of a ventilation tube at least once and found that 6.9% of the children with cleft palate devel-opedcholesteatoma comparedwith1.5% ofthosewithout cleft palate. Harris et al.18 found that 2.2% of patients
undergoing palatoplasty between 5 and 18 years of age harbored cholesteatoma, an incidence 200 times greater than that observed in the general population. A previ-ousstudy withthisgroupshowed aprevalence of 6.4%of cholesteatomainpatientswithcleftlipandcleftpalateor cleft palate alone.19 Inthe present study,a frequency of
3.8%ofpatientswithpalataldefectswasobserved,withno differencebetweenchildrenandadults,whileKemppainen etal.5studied500patientswithcholesteatomaandfounda
prevalenceof8%.
In the present series, 51.1% of patients underwent surgeryinthestudyperiod.Asthisisareferralservicefor thetreatmentofCOM,duetomassivedemandforsurgery andlowsurgicalavailability,thereisoftenalongdelayfrom thefirstassessmenttosurgery.Thelongwaitingtimeforthe procedureandthemajorprogressionofthedisease result-ingfromthatdelay,associatedwiththelackofadherence andfollow-updifficultyofsome patients,makestheopen tympanomastoidectomy the surgical technique of choice. Currently in this service, open tympanomastoidectomy is indicatedinthefollowingsituations:locally advanced dis-ease,involvementoftheposterolateralupperquadrantsof themiddleearthatpreventspropercleaning ofthefacial nerverecessand tympanicsinus;a scleroticoreburnated mastoid; involvementof a singleear;and/or a contralat-eralear withadvanced cholesteatoma or previous cavity. The surgical technique indications were similar between children and adults. The present results are contrary to theinternational trend,currently more favorable to con-servativesurgeries,usingclosedtympanomastoidectomyor channelreconstructiontechnique.20---22
Epidemiologicalstudies,suchasthepresent,performed withalargenumberofpatients,providedataonthe Brazil-ianpopulation,especiallythatpopulationdependentonthe publichealthsystem.Thus,knowingtheclinical characteris-ticsandpeculiaritiesofthepatientswithcholesteatoma,it
canbeassessedwhethertheresultsofinternationalstudies canbereproducedandappliedintheBrazilianpopulation.
Conclusion
The prevalence of cholesteatoma in patients with COM was24.5%;itwasmorefrequentlyfoundin adultsthan in children. Bilateral disease wasfound in 17.1% of patients withcholesteatoma.Hypoacusis,withorwithoutotorrhea, wasthemaincomplaint,andthevast majorityofpatients had otorrheaat thetime ofthe firstevaluation. Ahigher prevalence of posterior mesotympaniccholesteatoma was observedinthepresentpopulation.Thefrequencyofpalatal defectswas3.8%,similarinchildrenandadults.Regarding air-bone audiometric gap sizes, the tritonal mean was 29.84dB and there were no differences when comparing the different routes of cholesteatoma formation. In most patients undergoingsurgery, open tympanomastoidectomy wastheprocedureofchoice.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.OlszewskaE,WagnerM,Bernal-SprekelsenM,EbmeyerJ,Dazert S,HildmannH,etal.Etiopathogenesisofcholesteatoma.Eur ArchOtorhinolaryngol.2004;261:6---24.
2.DeAzevedoAF,PintoCG,deSouzaNJA,GrecoDB,Gonc¸alves DU. Sensorineural hearing loss in chronic suppurative otitis media with or without cholesteatoma. Rev Bras Otorrino-laringol.2007;73:671---3.
3.CostaSS,RositoLPS,DornellesC.Sensorineuralhearinglossin patientswithchronicotitismedia.EurArchOtorhinolaryngol. 2009;266:221---4.
4.PenidoNdeO,ToledoRN,SilveiraPA,MunhozMS,TestaJR,Cruz OL.Sigmoidsinusthrombosisassociatedtochronicotitismedia. RevBrasOtorrinolaringol.2007;73:165---70.
5.KemppainenHO, PuhakkaHJ,Laippala PJ,SipiläMM, Manni-nenMP,Karma PH.Epidemiology and etiologyofmiddleear cholesteatoma.ActaOtolaryngol.1999;119:568---72.
6.deAquinoJEAP,CruzFilhoNA,deAquinoJNP.Epidemiologyof middleearandmastoidcholesteatomas:studyof1146cases. BrazJOtorhinolaryngol.2011;77:341---7.
7.DornellesCC,daCostaSS,MeurerL,SchweigerC.Some con-siderationsaboutacquiredadultandpediatriccholesteatoma. RevBrasOtorrinolaringol.2005;71:536---46.
8.JacklerRK.Thesurgicalanatomyofcholesteatoma.Otolaryngol ClinNorthAm.1989;22:883---96.
9.BlackB,GutteridgeI. Acquiredcholesteatoma: classification andoutcomes.OtolNeurotol.2011;32:992---5.
10.Ar A, Herman P, Lecain E, Wassef M, Huy PTB, Kania RE. Middle ear gas loss in inflammatory conditions: the role of mucosa thickness and blood flow. Respir Physiol Neurobiol. 2007;155:167---76.
11.RosenfeldRM,CulpepperL,DoyleKJ,GrundfastKM,Hoberman A,KennaMA,etal.Clinicalpracticeguideline:otitismediawith effusion.OtolaryngolHeadNeckSurg.2004;130:s95.
13.MarchioniD,Alicandri-CiufelliM, MolteniG,Artioli FL, Gen-ovese E, Presutti L. Selective epitympanic dysventilation syndrome.Laryngoscope.2010;120:028---33.
14.Jesic SD, Jotic AD, Babic BB. Predictors for sensorin-aural hearing loss in patients with tubotympanic otitis, cholesteatomaandtympanicmembraneretractions.Otol Neu-rotol.2012;33:934---40.
15.AbergB,WestinT,TjellsromA,EdstromS.Clinical characteris-ticsofcholesteatoma.AmJOtolaryngol.1991;12:254---8. 16.DominguezS,HarkerLA.Incidenceofcholesteatomawithcleft
palate.AnnOtolRhinolLaryngol.1988;97:659---60.
17.SpilsburyK,HaJF,SemmensJB,LanniganF.Cholesteatomain cleftlipandpalate:apopulation-basedfollow-upstudyof chil-drenafterventilationtubes.Laryngoscope.2013;123:2024---9. 18.HarrisL, CushingSL, HubbardB,Fisher D,PapsinBC,James
AL.Impactofcleftpalatetypeontheincidenceofacquired
cholesteatoma. Int J Pediatr Otorhinolaryngol. 2013;77: 695---8.
19.Carvalhal LHSK (Dissertac¸ão (mestrado)) Descric¸ão das alterac¸õesotológicasdepacientescomfissuralabiopalatinaou palatinaisolada.PortoAlegre:ProgramadePós-graduac¸ãoem CirurgiadaUniversidadeFederaldoRioGrandedoSul;2003. 20.PrasadSC,LaMeliaC,MedinaM,VincentiV,BacciuA,BacciuS,
etal.Long-termsurgicalandfunctionaloutcomesoftheintact canalwalltechniqueformiddleearcholesteatomainthe pae-diatricpopulation.ActaOtorhinolaryngolItal.2014;34:354---61. 21.WalkerPC,MowrySE,HansenMR,GantzBJ.Long-termresults ofcanalwallreconstructiontympanomastoidectomy.Otol Neu-rotol.2014;35:954---60.