www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Prevalence
of
dizziness
in
the
population
of
Minas
Gerais,
Brazil,
and
its
association
with
demographic
and
socioeconomic
characteristics
and
health
status
夽
Tiago
Ferreira
Martins
a,∗,
Patrícia
Cotta
Mancini
a,
Luiza
de
Marilac
de
Souza
b,
Juliana
Nunes
Santos
a,caUniversidadeFederaldeMinasGerais(UFMG),ProgramadePós-graduac¸ãoemCiênciasFonoaudiológicas,
BeloHorizonte,MG,Brazil
bFundac¸ãoJoãoPinheiro,BeloHorizonte,MG,Brazil
cUniversidadeFederaldosValesdoJequitinhonhaeMucuri(UFVJM),TeófiloOtoni,MG,Brazil
Received9September2015;accepted5January2016 Availableonline3May2016
KEYWORDS
Dizziness; Epidemiology; BrazilianUnified HealthSystem
Abstract
Introduction:ThestateofMinasGerais,Brazilhasnodataontheprevalenceofdizzinessin
thepopulationandthisinformationcanbefundamentalasthebasisofpublichealthpolicies, promotion,preventionandrehabilitationcampaigns.
Objective: InvestigatetheprevalenceofthesymptomofdizzinessinthepopulationofMinas
GeraisaccordingtoSampleSurveyofHouseholds,aswellasdescribetheprofileofinterviewed individualsandtheassociationbetweendizzinessandsocioeconomic,demographicfeatures andhealthstatus.
Methods:Thiswasacross-sectionalobservationalstudythatanalyzedindividualswithdizziness
symptomreportedinthepreviousmonth.ThedataenteredintheSampleSurveyofHouseholds of2011wereanalyzed.An independentstatistical associationwasdeterminedbetweenthe selectedvariablesanddizzinessthroughmultivariateanalysis.
Results:Dizzinesswasthethirdmajorcomplaintamongindividualswhomentionedanyhealth
problems inthe previousmonth, with anestimated populationof 209,025 individuals and reportedby 6.7%ofsymptomaticones, withhigherprevalencevaluesonlyreportedforthe
夽 Pleasecitethisarticleas:MartinsTF,ManciniPC,deSouzaLM,SantosJN.PrevalenceofdizzinessinthepopulationofMinasGerais, Brazil,anditsassociationwithdemographicandsocioeconomiccharacteristicsandhealthstatus.BrazJOtorhinolaryngol.2017;83:29---37.
∗Correspondingauthor.
E-mail:[email protected](T.F.Martins).
PeerReviewundertheresponsibilityofAssociac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial.
http://dx.doi.org/10.1016/j.bjorl.2016.01.015
symptomsoffeverandheadache.Amongindividualswhoreporteddizziness,94%wereadults or elderly (p≤0.001) and 63% were females (p=0.003). A statistically significant
associa-tion(p<0.001)wasobservedbetweentheresponsevariableandthevariables:self-perceived health, hypertension, heart disease, diabetes, depression, seeking or requiring medical or healthcareinthepreviousmonthandprivatehealthcareplanorinsurance.Amongindividuals withdizziness,84.2%soughtorrequiredmedicalorhealthcareand80.1%didnothaveaprivate healthplanorinsuranceintheassessedperiod.
Conclusion:ThedizzinesssymptomwashighlyprevalentinthepopulationofMinasGeraisduring
theassessedmonthoftheinvestigation.Dizzinesswasprevalentinadultsandtheelderlyand showedastatisticalassociationwithsocioeconomicanddemographiccharacteristics,aswell astheassessedhealthstatus.
© 2016 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Published by Elsevier Editora Ltda. This is an open access article under the CC BY license (http:// creativecommons.org/licenses/by/4.0/).
PALAVRAS-CHAVE
Tontura; Epidemiologia; SistemaÚnicode Saúde
Prevalênciadetonturanapopulac¸ãodoEstadodeMinasGerais,Brasil,esuas relac¸õescomascaracterísticassocioeconômicasdemográficasecondic¸õesdesaúde
Resumo
Introduc¸ão:OestadodeMinasGerais---Brasilnãopossuidadossobreaprevalênciadetonturana
populac¸ãoeestasinformac¸õespodemserfundamentaisparabasearpolíticasdesaúdepública, campanhasdepromoc¸ão,prevenc¸ãoeareabilitac¸ão.
Objetivo:Investigar a prevalênciado sintomade tontura napopulac¸ãodo estadode Minas
GeraissegundoaPesquisaporAmostradeDomicílio(PAD-MG),assimcomodescreveroperfil dos indivíduosentrevistados eas relac¸ões entretontura e características socioeconômicas, demográficaecondic¸õesdesaúde.
Método: Estudodecaráterobservacionaltransversalcomanálisedosindivíduoscomrelatode
sintomadetontura noúltimomês.Foramanalisados osdadosinseridosnaPAD-MGde2011. Determinou-seassociac¸ãoestatísticaindependenteentreasvariáveisselecionadaseatontura porintermédiodeanálisemultivariada.
Resultados: A tontura foi à terceira queixaprincipal entre osindivíduos que mencionaram
algumproblemadesaúdenoúltimomês,comestimativapopulacionalde209.025indivíduos erelatadapor6,7%dossintomáticos,comvaloresinferioressomenteaossintomasdefebree doresdecabec¸a,respectivamente.Dentreindivíduoscomrelatodetontura,94%sãoadultos ouidosos(p≤0,001)e63%dosexofeminino(p=0,003).Foiencontradaassociac¸ão estatistica-mentesignificante(p<0,001)entreavariávelrespostaeasvariáveisautopercepc¸ãodesaúde, hipertensão,doenc¸ascardíacas,diabetes,depressão,procuraounecessidadedeatendimento médicooudesaúdenoúltimomêsepresenc¸adecoberturadeplanoouseguro-saúde.Dentre osindivíduoscomtontura,84,2%procurououprecisoudeatendimentomédicooudesaúdee 80,1%nãopossuíamcoberturadeplanoouseguro-saúdenoperíodopesquisado.
Conclusão:Osintomadetonturasemostroualtamenteprevalentenapopulac¸ãodeMinasGerais
nomêsde referênciadapesquisa. A tontura foiprevalente nos indivíduosadultos eidosos eapresentou associac¸ão estatísticacomascaracterísticas socioeconômicas, demográficase condic¸õesdesaúdeestudadas.
© 2016 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Publicado por Elsevier Editora Ltda. Este ´e um artigo Open Access sob uma licenc¸a CC BY (http:// creativecommons.org/licenses/by/4.0/).
Introduction
Intheeventofaconflictintheintegrationofsensory
infor-mationthataidsposturalcontrol,wearefacedwithabody
balance dysfunction that can be translated as dizziness.
According to the Hearing and Balance Committee of the
American Academy of Otorhinolaryngology and Head and
Neck Surgery,dizziness is anyillusorysense of movement
withoutrealmovementinrelationtogravity.1Dizzinessmay
causefearofmovement, gaitalterations,anxiety,
insecu-rity,depressionandfear,inadditiontosecondaryautonomic
symptoms,suchassweating,nauseaandvomiting.2,3
Dizzi-ness often impairs social, family and work activities and
causes physical, financial and psychological damage, in
additiontoresultinginadecreaseinconcentrationand
alsoassociated withtheuse of fiveor more medications,
thepresenceofposturalhypotensionandahistoryofacute
myocardialinfarction.4
Dizziness has been characterized as a multifactorial
healthcondition thatarisesfromthecumulativeeffectof
multiple systemdeficits,resultingin increased
vulnerabil-ity, mainly among the elderly.4,5 There is an association
betweenchronic dizzinessanddepressivesymptoms,poor
self-perceivedhealthstatusandrestrictedparticipationin
social activities.4,6 In a two-year longitudinal study, the
main factors related to dizziness in the elderly were:
age, female gender, cardiovascular disease,
osteoporo-sis, depression, sleep and memory disorders, impaired
vision,incontinence,threeormorecomorbidities,
polyphar-macy,poorself-perceivedhealthstatus,fallsandmobility
problems.7
Dizziness is commonsymptom, that isoften
underesti-matedanduntreatedbyhealthprofessionals.Itisestimated
that23.3%ofpatientsaged18---64seekingageneral
prac-titioner have experienced some type of dizziness in the
previous monthand almost30% oftheseindividuals
expe-rienceddizzinessinthelastfiveyears.8Inastudyof1000
patientswithlongitudinalfollow-up,dizzinesswasthethird
most frequent clinical symptom in a general outpatient
clinic, second only to chest pain and fatigue.9 The
inci-dence of dizziness significantly increases with advancing
age.7,10---13 Inalongitudinal studyof620elderlyindividuals
fromGermany,itwasobservedthattheprevalenceof
dizzi-nesscomplaintinthe last6monthswas27%amongthose
aged up to70 years and 54% in those aged 90 years and
older.7 A Swedish National Study on Aging and Care with
1273individualsobservedaprevalence ofdizzinessin31%
ofindividualsaged>80years.14
Accordingtostudies,theannualratesofmedical
consul-tationbecauseofdizzinessinprimarycarerangefrom2.5%
in patients aged 25---44 yearsto 8.3% in patients aged 65
years or older, and is 18.2% in patients aged 85 years or
older.8,15 Muchofthecareprovidedtopatientswith
dizzi-nessisperformedinprimarycaresettings;inastudyinthe
Netherlands carried out from 1985 to1995, family
physi-ciansreportedthatonly3%oftheelderlywithdizzinessare
referredtoamedicalspecialist.16
In Brazil, there are few population-based studies in
the health area and very few of these investigate
symp-toms in the population. The PNAD (National Survey by
Household Sample of the Brazilian Institute of
Geogra-phy and Statistics --- Instituto Brasileiro de Geografia e
Estatística --- IBGE) has invested in issues directed at the
health status of the Brazilian population with a national
scopesince2004.17 Updatedpopulation-basedinformation
isessentialfor societalplanning andmonitoring invarious
geographic and socioeconomic settings, to allow
compli-ance with the constitutional principlesof health, such as
the right to equal access to and financing of health
ser-vices. The dissemination of this information by IBGE also
increases the possibility of incorporating health
informa-tionbydifferentareas ofgovernment,whichis important
tostrengthenintersectoral actions,inordertofollow the
policiesaimedtoimprovetheoverallhealthoftheBrazilian
population.18
Thepublicandprivatehealthcarenetworkinthestateof
MinasGerais,Brazil,doesnothavedataontheprevalence
ofdizzinesswithin thepopulation. Thus,the analysisand
disseminationofthisinformationcanhelpdefinetheprofile
of the symptomatic population, provide additional data
ondeterminant factors andassociated comorbidities that
maybe crucial to establish public health policies, obtain
resources,carryoutpromotion,preventionand
rehabilita-tioncampaignsaimedatthetargetpopulation.Considering
morethan170millionBraziliansdonothaveprivatehealth
care plans or insurance anddepend only onthe Brazilian
Unified Health System (SUS) for health care,17,19 studies
suchasthisinvestigationbecomeessential.
Thus,the present study aimstoinvestigate the
preva-lence of dizziness symptom within the population of the
stateofMinasGerais,Brazil,describetheprofileofthe
indi-vidualsinterviewedbythePAD-MGwhoreporteddizziness
inthelast30days,aswell asassessassociationsbetween
dizzinessanddemographicandsocioeconomic
characteris-ticsandhealthstatusofrespondents.
Methods
Thisisacross-sectional,observationalstudywiththe
anal-ysis of individuals from Minas Gerais that reported the
symptomofdizzinessinthelast30days.Thestudy
compre-hendstheanalysisofdatafromthePAD-MGofFundac¸ãoJoão
Pinheiro,whichiscarriedoutsimilartotheNationalSurvey
byHouseholdSamples,the IBGE-PNADandhasasampling
statisticaloperation.17
The Sample Surveyof Households(PAD-MG)was
devel-opedinthestate ofMinasGerais(MG); theprojectbegan
in 2007 and the first research was carried out in 2009,
designedtoproduceregionalizedinformationableto
coordi-natewiththemonitoringandassessmentofpublicpolicies.
The PAD aims toobtain informationon the population of
differentregionsof MGand tobea steptoward the
con-structionwithinthestateofanagileandflexiblestructure
capableofmeeting thespecific demandsof theiractions.
The PAD-MG is a key step in the consolidation of a state
conceptthataccompaniestheprocessesandtheresultsof
actions.20
The second round of the PAD-MG, held in 2011, was
a socioeconomic survey based on a sample of 18,000
households distributed in 1200 census sectors and 428
municipalities, with regional representation for the 12
mesoregionsofthestate.EverytwoyearsthePADcollects
informationonhealth,education,work,incomeand
bene-fits,characteristicsofhouseholdsandindividualsandother
subjects.Thedatahelpstodirecteffortsandresourcesthat
arespecificforthedifferentregionsofthestate.The
PAD-MGincludes the residentpopulation inpermanentprivate
households,butexcludesresidentsininstitutionalcollective
householdestablishments.20
The basic registration for the selection of census
sec-torsinPAD-MG2011wasobtainedfromtheAggregatedFiles
oftheDemographicCensusSynopsisSectorsof2010inthe
stateofMinasGerais,usingaprobabilisticsamplingmethod.
Inthefirststage,theinitialallocationofthehouseholdand
sectorsamples wasperformed using the power allocation
method,whilerespectingthelimitsof3000householdsfor
theruralpartofthesampleand15,000homesfortheurban
partofthesample.Inthesecondphase,adjustmentswere
ofstandarderrorsfromthePAD-MG2009microdata.
More-over,anadditionalstratification methodwasapplied,that
consistedoforganizingthesectorsbymicroregion,
munici-pality,district,subdistrictandneighborhood.20
Aftertheorganizationofthecensussectors,sampleareas
weredefined, which were asmany as the sample size of
sectorsinthestratumdividedbytwo,aimingtoselecttwo
sectorspersamplingzone.Theselectionoftwosectorsper
zonewas carriedoutby Poisson sequential sampling. The
totalnumberofhouseholdsinthesectorwasusedasa
mea-sureofsize.Itisnoteworthythatthisnumberwastruncated
at30atthelowerlimitand600attheupperlimittoreduce
thevariabilityofsectorinclusionprobability.Forthe
selec-tionofhouseholdsineachsamplesectorofthefirststage,
theinversesamplingofhouseholdswasproposed.This
pro-cedureallowedustocontrolthefinalsizeofthehousehold
sample that was actually interviewed, ensuring that the
effectivesamplesizewillbeequaltoorveryclosetothe
sizespecifiedintheinitialdesign.20
Data collection took place from 10/01/2011 to
29/02/2012, using a laptop during the face-to-face
interviews. The interviewers were hired and trained by
Fundac¸ãoJoãoPinheiroforthehomevisits.20
Thesurveyquestionnairewasdividedintotensections,
respectively: household characteristics; characteristics of
residents;education;health,workandchildlabor;income;
entrepreneurship;household’s collective expenses (eighth
and ninth); individual expenses of each resident of the
household. This study will emphasize the analysis of the
‘‘health’’ section questions, considering as the response
variable: feeling ill, with dizziness, in the last 30 days.
The explanatory variables were: gender, age, seeking
and requiring health care in the last 30 days, private
health plan or health insurance coverage, health
self-perception, followsnutritional guidelines,current smoker
andthepresenceofhealthproblemthatrequiresconstant
monitoring.
Forthedescriptionofthequestion‘‘Did[Name]feelill,
withahealthproblemsymptominthelast30days?(Name
themainsymptomin thisperiod.)’’,therespondent
men-tioneddizzinessor oneoffourteenother responseoptions
including‘‘nosymptoms’’.Asthestudyoftheresponse
vari-able was dizziness, the study subjects were divided into
twogroups,theoneswhoexperienceddizzinessduringthe
previous 30 daysandthose whodidnot. Forthe
descrip-tionofthevariablegender,therespondentansweredmale
or female. For the description of the variable age, the
respondentreportedhis/herageandlatertheinterviewer
classified it according to categories: adult (19---59 years)
andelderly(60yearsorolder). Forthe descriptionofthe
question on self-perceived health status, the respondent
answeredthequestion‘‘Howdoyouassessthehealth
sta-tus of [name]?’’, of which answers were provided using
a five-point Likert scale (very good/good/fair/poor/very
poor).
However,fordataanalysis,responsesweregroupedinto
good(very good and good) and poor (fair, poor and very
poor).Forthedescriptionofthequestions‘‘And[Name]
fol-lowedtheserecommendations(nutritionalguidelinesfrom
adoctorornutritionist)?’’,‘‘Does[Name]smokecigarettes
now?’’,‘‘Hasadoctororhealthcareprofessionalsaidthat
[Name] has cardiac diseases (heart diseases)?’’, ‘‘Has a
doctor or health care professional said that [Name] has
hypertension (high blood pressure)?’’, ‘‘Has a doctor or
healthcareprofessionalsaidthat[Name]hasdepression?’’,
‘‘Hasadoctororhealthcareprofessionalsaidthat[Name]
hasdiabetes?’’,‘‘Did[Name]needorseekmedicalorhealth
care in the last30 days?‘‘and’’ Does [Name]have a
pri-vate health planor insurancecoverage?’’, theanswers of
respondents were grouped into ‘‘yes’’ or ‘‘no’’ for data
analysis.
The responses to the PAD-MG questions about seeking
andrequiringhealthcareservicesconsideredSeptember1,
2011 asthereferencedate. Themonth ofAugust andthe
weekofAugust28---31toSeptember1---2wereconsidered,
respectively,thestudyreferencemonthandweek.
AtthePAD/MG,thefreeandinformedconsentformwas
replacedbyverbalconsentoftherespondent, obtainedat
the timeof the interview. The interviewersinformed the
residentsaboutaspectsoftheresearch,itsbenefits,impact
andimportanceintheevaluationofstatepoliciesandasked
for theirconsenttoparticipateintheresearch.Residents
werefreetoacceptortorefusetoparticipate.This study
wasapprovedbytheResearchEthicsCommitteeunderETIC
protocolnumber0347.0.203.000-10.
Basedontherespondents’answers,adatabasewas
gen-eratedusingSPSS(StatisticalPackageforSocialSciences),
version19.0.Throughthesamplingprocessusedinthe
PAD-MG,thepopulation estimateforthestate ofMinas Gerais
wascarriedout.20 First,adescriptiveanalysisof thedata
wasperformed.Then,theanalysisoffactorsassociatedwith
dizzinesswasperformed,withaninferentialanalysisusing
Pearson’sChi-squaretestforcategoricalvariables,
consid-eringasstatisticalsignificancethe95%confidenceinterval
(first phase). Subsequently, all the variables associated
withdizzinessat p≤0.10were tested.The variables that
remainedstatisticallyassociatedwithdizzinessat p≤0.05
remainedinthefinalmodel.Thisanalysiswasperformedin
twostages,usingbinarylogisticregression.
Results
InapopulationestimatebasedonthePAD/MG2011sample,
ofatotalof19,442,971individuals,3,586,973(18.44%)had
ahealthproblemsymptomintheprevious30days,withthe
mostcommonsymptomsbeingshowninTable1.
Themeanageofthesubjectswithsymptomswas41.08
yearsandforthetotalsample,35.8years.Thedistribution
of the stratified percentagein a 10-year scale of
individ-uals that haddizziness in the previous month, comparing
the populationof individualswhoreporteda health
prob-lemsymptomandthetotalsamplepopulationcanbeseen
inFig.1.
In the univariate analysis, all assessed variables
(gen-der,age, poorhealth self-perception,presenceof chronic
diseases,seekinghealthcareservices,lackofhealth
insur-ance, lack of physical activity, current smoker, does not
follow nutritionalguidelines)showed astatistical
associa-tion (p<0.001) withthe response variable. However, the
variables gender and diabetes showed no statistical
asso-ciation in the multivariate analysis, even with a higher
prevalence of the female gender and presence of
Table1 Populationestimateofindividualsinterviewedin the PAD-MG 2011 who felt ill and had a health problem symptomoverthepast30days,mentioningonlythemain symptomexperiencedinthisperiod.
Symptom n Relative frequency (%)
Cumulative frequency (%)
Fever 316,004 7.88 7.88
Diarrhea 109,900 2.87 10.75 Toothache 70,035 1.93 12.68
Headaches 611,080 16.13 28.81
Chestpain 99,983 3.29 32.10 Abdominalpain 178,654 4.97 37.06 Earache 29,953 0.93 37.99 Breathlessness 109,370 3.16 41.15 Bleeding 16,805 0.53 41.68
Dizziness 209,025 6.70 48.38
Cough 136,264 3.65 52.03 Vomiting 51,523 1.42 53.45 Other 1,648,377 46.55 100.00 Total 3,586,973 100.00
Source:SampleSurveyofHouseholdsofMinasGerais(PAD-MG). Fundac¸ãoJoãoPinheiro,2011.
18
16
14
12
10
8
6
4
2
0 0-9
years years years years years years years years years 10-19 20-29 30-39 40-49 50-59 60-70 71-80 81-90 Above
90 years
P
ercentage of individuals with dizziness
Symptomatic population General population
Figure1 Prevalenceofdizzinessaccordingtoage.
Source:SampleSurveyofHouseholdsofMinasGerais(PAD-MG).
Fundac¸ãoJoãoPinheiro,2011.
population, being respectively 131,686 (63%) and 37,209 (17.9%)amongindividualswithdizzinessinpopulation esti-mates.
Themultivariateanalysisofthepresenceofdizzinessin the previous month and its association with demographic variables,health status andsocioeconomiccharacteristics thatdisclosedastatisticalassociationcanbeseeninTable2.
Discussion
The interviewed population is representativeof the state
of Minas Gerais and the dizziness symptom wasthe third
mostprevalentmaincomplaintamongindividualswho
men-tionedsometypeofhealthprobleminthepreviousmonth,
reported by 6.7% of symptomatic individuals, with lower
values only when compared to the symptoms of fever
and headache, respectively. It is estimated that of the
populationof19,442,871 individuals;209,025experienced
dizzinessas the most prevalent symptom in the assessed
month.AccordingtoKroenkeetal.,9 dizzinessisthethird
most common clinical symptom in a general outpatient
clinic.Authorsofinternationalpopulationstudiesindicate
thatdizzinessprevalencerangefrom11%to32.5%.8,15,21,22
Bittaretal.23 establishedaprevalenceofdizzinessas42%
instudy carriedoutin SãoPaulo, Brazil, ahigher
propor-tionthan thatfoundin otherstudies. However,in astudy
of 4869 individuals, the prevalence of dizziness of
vesti-bularorigininadultswasestimatedat7.4%.11Thisvariation
inprevalencecanbeinfluencedbymethodologicalbiases,
includinghowthedatawascollected,symptomdescription,
andmainlytheprevalencemeasureused;somestudiesused
theprevalencethroughoutlife,withconsequenthigher
val-ues,whereas the present study used the prevalence only
duringthestudyperiod.Individualsinterviewedinthe
PAD-MGonly answered about the main health problem in the
previousmonthandmightalsohavefeltdizzinessasa
sec-ondarysymptom and thus, theydidnot mentionitin the
survey.
The present study found that 94% of patients with
reporteddizzinessare adult or elderly individuals,
repre-senting 196,548 individuals. Of these, the elderly have a
1.111-foldhigher chance of having dizziness asthe main
healthproblemthan adults,witha statisticallysignificant
association (p<0.001) between theresponse variableand
theage variable.The studyobserved thatthe prevalence
ofdizzinessincreasesindirectproportionwithage,witha
peakbetween71and80years,corroboratingthefindingsof
Charlesetal.10andNeuhauseretal.,11whoreportedapeak
between65and75years.Moraesetal.24foundaprevalence
ofdizzinessof 45%in astudy with391 elderlyindividuals
andOlsson Mölleretal.14 found aprevalence of dizziness
of 17.8% and 31% in individuals aged <80 and >80 years,
respectively. The findings of higher prevalence of
dizzi-nessintheelderlyagreewithseveralworldwideliterature
reports10,15,21---23,25---27andcanbeexplainedbytheaging
pro-cessofthebalancesystem,multiplesensorydeficits,which
arecommoninelderlypatientsandaccumulationof
comor-bidities,suchascardiovascular,metabolicandneurological
diseases. In a study performed at the University Hospital
ofZurich,Switzerland,with266 individualswithdizziness
olderthan65 years,37.6%werediagnosed with
multisen-sorydizziness,5whichreinforcestheimpactofagingonthe
increasingprevalenceofthissymptom.
Amongtheindividualswhoreporteddizziness,63%were
females, representing 131,686 individuals in the state of
MinasGeraisandthisdistributionisinagreementwiththe
literature.25,26 The prevalence of dizzinessin females has
beenreportedinseveralotherstudies,8,10---12,22---24,28---31which
can be explained by the hormonal variations responsible
forovariancyclesandmenopause,32,33higherprevalenceof
migraine,12,29thefactthatwomenmoreoftenseekmedical
care23,28 anda higherprevalenceof womenin theelderly
population worldwide. However, as in this study, some
researchers also found no statistical association between
dizzinessand gender,15,27 asshown in theEnglishstudy of
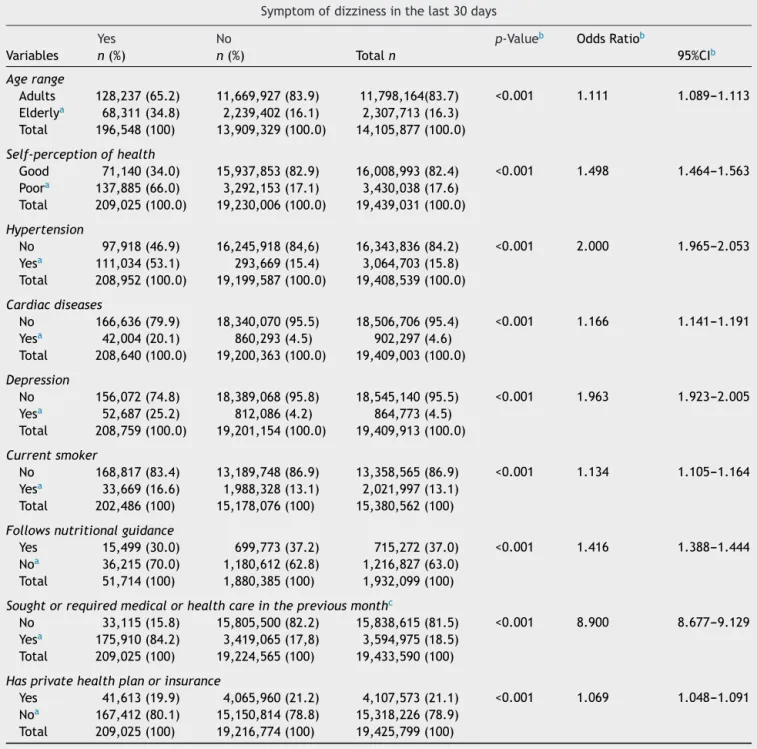
Table2 Multivariatebinarylogisticregressionoffactorsassociatedwiththepresenceofdizzinessinthe30dayspreceding theinterviewofPAD-MG,2011.
Symptomofdizzinessinthelast30days
Yes No p-Valueb OddsRatiob
Variables n(%) n(%) Totaln 95%CIb
Agerange
Adults 128,237(65.2) 11,669,927(83.9) 11,798,164(83.7) <0.001 1.111 1.089---1.113
Elderlya 68,311(34.8) 2,239,402(16.1) 2,307,713(16.3)
Total 196,548(100) 13,909,329(100.0) 14,105,877(100.0)
Self-perceptionofhealth
Good 71,140(34.0) 15,937,853(82.9) 16,008,993(82.4) <0.001 1.498 1.464---1.563
Poora 137,885(66.0) 3,292,153(17.1) 3,430,038(17.6)
Total 209,025(100.0) 19,230,006(100.0) 19,439,031(100.0)
Hypertension
No 97,918(46.9) 16,245,918(84,6) 16,343,836(84.2) <0.001 2.000 1.965---2.053
Yesa 111,034(53.1) 293,669(15.4) 3,064,703(15.8)
Total 208,952(100.0) 19,199,587(100.0) 19,408,539(100.0)
Cardiacdiseases
No 166,636(79.9) 18,340,070(95.5) 18,506,706(95.4) <0.001 1.166 1.141---1.191
Yesa 42,004(20.1) 860,293(4.5) 902,297(4.6)
Total 208,640(100.0) 19,200,363(100.0) 19,409,003(100.0)
Depression
No 156,072(74.8) 18,389,068(95.8) 18,545,140(95.5) <0.001 1.963 1.923---2.005
Yesa 52,687(25.2) 812,086(4.2) 864,773(4.5)
Total 208,759(100.0) 19,201,154(100.0) 19,409,913(100.0)
Currentsmoker
No 168,817(83.4) 13,189,748(86.9) 13,358,565(86.9) <0.001 1.134 1.105---1.164
Yesa 33,669(16.6) 1,988,328(13.1) 2,021,997(13.1)
Total 202,486(100) 15,178,076(100) 15,380,562(100)
Followsnutritionalguidance
Yes 15,499(30.0) 699,773(37.2) 715,272(37.0) <0.001 1.416 1.388---1.444
Noa 36,215(70.0) 1,180,612(62.8) 1,216,827(63.0)
Total 51,714(100) 1,880,385(100) 1,932,099(100)
Soughtorrequiredmedicalorhealthcareinthepreviousmonthc
No 33,115(15.8) 15,805,500(82.2) 15,838,615(81.5) <0.001 8.900 8.677---9.129
Yesa 175,910(84.2) 3,419,065(17,8) 3,594,975(18.5)
Total 209,025(100) 19,224,565(100) 19,433,590(100)
Hasprivatehealthplanorinsurance
Yes 41,613(19.9) 4,065,960(21.2) 4,107,573(21.1) <0.001 1.069 1.048---1.091
Noa 167,412(80.1) 15,150,814(78.8) 15,318,226(78.9)
Total 209,025(100) 19,216,774(100) 19,425,799(100)
Source:SampleSurveyofHouseholdsofMinasGerais(PAD-MG).Fundac¸ãoJoãoPinheiro,2011. aCategoriesofreference.
b Resultsobtainedaftermultivariateanalysis;thefinalmodelincludesthemaindependentvariableadjustedforothervariablesthat
remainedinthefinalmodel. c Medicalorhealthcare.
#Numberofinformationdiffersfromthetotalsampleduetomissingdata.
Whenanalyzingtheassociationbetweenthehealth
sta-tusofindividualswiththeresponsevariable,astatistically
significantassociationwasobserved(p<0.001)inthe
mul-tivariateanalysiswiththevariablesself-perceivedhealth,
hypertension,heartdiseaseanddepression.It isobserved
that66%ofindividualswhoreporteddizzinessinthe
previ-ousmonthshowedpoorself-perceivedhealth,representing
137,885individuals,wellabovethe17.1%ofindividualsthat
had other health problems symptoms,indicating a
signifi-cantnegativeimpactofdizzinessonpatientqualityoflife.
It was also verified that individuals with poor
self-perceivedhealth hada1.498-foldhigherchanceofhaving
dizziness as the main health problem than those who
of health associated with the complaint of dizziness
corroborates other studies.7,24,34 As for individuals with
hypertension, heart disease and depression they had,
respectively,a100%,16.6%and96.3%higherchancetohave
dizziness as the main health problem when compared to
those who did not have this symptom. In a study of 493
elderlyindividuals, Lopes etal.28 found a statistical
asso-ciation between dizziness and hypertension. Dros et al.30
studied417elderlypatientswithdizzinessinprimarycare
in the Netherlands and found that 49% hadheart disease
and 57% had hypertension. The findings agree withother
studies,32,35,36 whichreportedthat dizzinesscan bea
sec-ondary effect of arterial hypertension and heart disease.
Studieswiththeelderlyfoundanassociationbetween
dizzi-ness and a positive score for depressive symptoms.6,13,30
In the 7-year follow-up of a prospective cohort with681
elderly, Maarsingh et al.31 found anxiety or depression
in 33.6% of patients with dizziness and in only 15.1% of
individuals withoutdizziness, which showeda statistically
significantassociation.AccordingtoEkwalletal.,13thereis
evidencethatneurotologicaldisordersarerelatedtoanxiety
andincreaseinpsychologicalproblems,which,inturn,can
aggravatetheintensityofthedizzinesscomplaint.Inastudy
byNeuhauseretal.,11depressionandseveralcardiovascular
diseaseswereassociatedwithvestibularvertigo.
Althoughthisstudydemonstratesthatthehealthstatus
is multifactorialand aresultof the cumulativeeffectsof
multiple system deficits, making individuals more
vulner-able during the aging process and subject to inadequate
changesinbalancephysiology,therewasnostatistically
sig-nificantassociationinthemultivariateanalysisbetweenthe
responsevariableandthepresenceofdiabetes,which
cor-roborates other studies.30,36 In a Brazilian study with391
individuals older than 65 years, Moraes et al.24 found no
statistical association of dizziness withdiabetes and
obe-sity.This study founda statisticallysignificant association
(p<0.001)betweentheresponsevariableandthevariable
current smoker, in which 16.6%of subjects withdizziness
reported being smokers and they showed a 13.4% higher
chancetohavedizzinessasthemainhealthproblemwhen
compared to individuals whodid not smoke. This finding
agreeswithacommunity-basedstudycarriedoutina
uni-versityoutpatientclinic.36InthestudybyCruzetal.37with
751young adultsandusingmultivariate analysis,an
asso-ciation wasfound between smokingand dynamic balance
testalterations.Pereiraetal.38 suggeststhatnicotinecan
induce imbalance in the vestibular-ocular and
vestibular-spinal reflexes; however epidemiological investigationsof
this association arestillveryincipient. Although a
Brazil-ian study did not find an association between dizziness
andsmoking,24 itisknownthatsmokingisassociatedwith
increasedrisk of chronicnon-communicable diseases such
ascardiovascularandpulmonarydiseases andcancer,with
a consequent impact on the physiology of the vestibular
system.
When assessing the association between the variable
patientfollowsnutritionalguidelineswiththeresponse
vari-able, a statistically significant association was observed
(p<0.001) and individuals who did not follow nutritional
guidelineshada 1.416-foldhigherchance ofhaving
dizzi-nessasthemain healthproblemwhen comparedtothose
whofollowed the guidelines.No studies were found with
statisticalassociationsbetweenfollowingnutritional
guide-linesandsymptoms of dizziness,but some authorsreport
theimportanceof nutritionalcounseling inthe treatment
in patients withdizziness toavoid or change poor eating
habits,39,40whichfacilitatesbetterbalance,cardiovascular
healthandmetabolicdiseasecontrol.
Theassociationbetweenthevariablessoughtorneeded
medicalorhealthcareinthepreviousmonthandhadhealth
careplanorinsurancecoveragewiththeresponsevariable
showedastatistically significant association (p<0.001).It
wasobservedthatamongindividualswithdizziness,84.2%
sought or needed medical or health care, a muchhigher
number than the 17.8% of individuals that had another
healthproblemsymptomandsoughtorneededhealthcare
service.Theserepresent175,910individualswithdizziness
in MGand theyhave an 8.9-foldhigher chance of having
dizzinessas the main health problem when compared to
individualswhodidnotseekcare.
InastudybyBittaretal.,2354%ofsymptomaticpatients
didnotseekmedicalattention,evenafterdizzinessstarted
affectingthequalityoflife.However,inastudyinGermany,
80%ofpatientswithdizzinessunderwentmedical
examina-tion,interruptionofdailyactivitiesorwentonsickleave.11
Thisdifferencecanbeexplainedbyculturalvaluesandeasy
accessibilitytohealthcareindifferentcountries.
Regarding thesocioeconomic variable,it wasobserved
that80.1%ofpatientswhohaddizzinessdidnothavea
pri-vatehealthcareplanorhealthinsurance,whichrepresents
167,412individualstreatedbySUSintheeventofdemand
forservicesduringthatperiodandtheconsequentimpact
ofpublic spending onhealth. These datacorroborate the
informationfromJune/2014oftheSupplementaryNational
HealthAgency,19thatonly26.1%oftheBrazilianpopulation
hasprivatehealthplan/insurance.Thus,itcanbeobserved
thatSUSremainsthemainproviderofhealthservicesused
bytheBrazilianpopulationandthatdizzinesshasa
conse-quenthighimpactonthehealthsystemdemandduetoits
prevalence.
Among the study limitations, it can be observed that
theresearchsubjectsonlyrespondedconcerningthemain
healthprobleminthepreviousmonth.Othersubjectsmay
haveexperienceddizzinessasasecondarysymptomandfor
this reason theymight not have mentioned it during the
investigationand theyalso might have experienced
dizzi-nessinotherperiodspriortothestudyreferencemonth;in
bothcasesthiswould result,innincreasedprevalence of
dizzinessintheinvestigation.
Conclusion
Thedizzinesssymptom asthemain health probleminthe
symptomaticpopulationwasshown tobehighlyprevalent
andaffects6.7%ofthepopulationofMinasGerais,whichis
estimatedat morethan209,000individuals withdizziness
symptomduringthereferencemonthoftheinvestigation.
Among individuals with dizziness, 94% are adults or
elderly, withthe elderly showing an 11.1% higher chance
ofhavingdizzinessasthemainhealthproblemthanadults.
Theincidenceofdizzinessincreasesindirectproportionto
age,withapeakprevalencebetween71and80yearsanda
withdizziness,66%reportedpoorself-perceivedhealthand
these had a 1.498-fold higher chance of having dizziness
asthemainhealthproblemthanthosewhoreportedgood
self-perceivedhealth. There wasastatistically significant
associationof dizzinesswiththe variablesbloodpressure,
heart disease, depression and being a current smoker
in the multivariate analysis and these individuals were
morelikelytohavedizzinessasthemain healthproblem.
Individualswhodidnotfollownutritionalguidelineshavea
49.8%higherchanceofhavingdizzinessasthemainhealth
probleminrelationtothosewhofollowtheguidelines.
Of the individuals with dizziness, 84.2% sought or
requiredmedicalorhealthcare,representing175,910
indi-vidualsin Minas Gerais. Itis also estimated that of those
symptomatic individuals with dizziness, 80.1% or 160,412
individuals had no private health care plan or insurance
coverageintheassessedperiod.
Therefore, we observe a great impact of dizziness in
SUS and demonstrated the importance of health
promo-tionprojectsandactions,aimedatdizzinesspreventionand
interventioninthevulnerablepopulation.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.CommitteeonHearingandEquilibriumguidelinesforthe diag-nosisandevaluationoftherapyinMenière’sdisease.American Academy of Otolaryngology-Head and Neck Foundation, Inc. OtolaryngolHeadNeckSurg.1995;113:181---5.
2.PedaliniMEB,BittarRSM.Reabilitac¸ãovestibular:umaproposta detrabalho.Pró-fono.1999;11:140---4.
3.Nishino LK, Gananc¸a CF, Manso A, Campos CAH, Korn GP. Reabilitac¸ão vestibular personalizada: levantamento de prontuáriosdospacientesatendidosnoambulatóriode otoneu-rologia da I.S.C.M.S.P. Braz J Otorhinolaryngol. 2005;71: 440---7.
4.TinettiME,WilliamsCS,GillTM.Dizzinessamongolderadults: a possible geriatric syndrome. Ann Intern Med. 2000;132: 337---44.
5.Geser R, Straumann D. Referral and final diagnoses of patientsassessedinanacademicvertigocenter.FrontNeurol. 2012;3:169.
6.Gazzola JM, Aratani MC, Dona F, Macedo C, Fukujima MM, GanancaMM, et al.Factors relatingtodepressive symptoms amongelderlypeoplewithchronicvestibulardysfunction.Arq Neuropsiquiatr.2009;67:416---22.
7.GassmannKG, RupprechtR.Dizzinessinanoldercommunity dwellingpopulation:amultifactorialsyndrome.JNutrHealth Aging.2009;13:278---82.
8.YardleyL,OwenN,NazarethI,LuxonL.Prevalenceand presen-tationofdizzinessinageneralpracticecommunitysampleof workingagepeople.BrJGenPract.1998;48:1131---5.
9.KroenkeK,MangelsdorffAD.Commonsymptomsinambulatory care:incidence,evaluation,therapy,andoutcome.AmJMed. 1989;86:262---6.
10.CharlesJ,FahridinS,BrittH.Vertiginoussyndrome.AustFam Phys.2008;37:299.
11.NeuhauserHK, vonBrevernM,Radtke A,LeziusF,Feldmann M,ZieseT,etal.Epidemiologyofvestibularvertigo:a neuro-tologicsurveyofthegeneralpopulation.Neurology.2005;65: 898---904.
12.Neuhauser HK. Epidemiology of vertigo. Curr Opin Neurol. 2007;20:40---6.
13.EkwallA, Lindberg A,Magnusson M. Dizzy--- whynot takea walk?Lowlevelphysicalactivityimprovesqualityoflifeamong elderlywithdizziness.Gerontology.2009;55:652---9.
14.OlssonMöllerU,MidlövP,KristenssonJ,EkdahlC,BerglundJ, JakobssonU.Prevalenceandpredictorsoffallsanddizzinessin peopleyoungerandolderthan80yearsofage---alongitudinal cohortstudy.ArchGerontolGeriatr.2013;56:160---8.
15.Colledge NR, Wilson JA, Macintyre CC, MacLennan WJ. The prevalenceandcharacteristicsofdizzinessinanelderly com-munity.AgeAgeing.1994;23:117---20.
16.OkkesIM,OskamSK,LambertsH.FromComplainttoDiagnosis. EpisodeDataFromFamilyPractice.Bussum,TheNetherlands: Coutinho;1998.
17.InstitutoBrasileirodeGeografiaeEstatística---IBGE.Pesquisa NacionalporAmostradeDomicílios(PNAD).CensoDemográfico. 2011.
18.TravassosC,ViacavaF,LaguardiaJ.OsSuplementosSaúdena PesquisaNacionalporAmostradeDomicílios(PNAD)noBrasil. RevBrasEpidemiol.2008;11:98---112.
19.Fontes Sistema de Informac¸ões de Beneficiários/ANS/MS ---06/2014ePopulac¸ão-IBGE/Datasus/2012.Availablein<http:// www.ans.gov.br/materiais-para-pesquisas/perfil-do-setor/ dados-gerais>.Accessedin:31.11.2014.
20.Boletim PAD-MG, ano 1, n. 3, jun. 2012 --- Belo Horizonte, Fundac¸ãoJoãoPinheiro,CentrodeEstatísticaeInformac¸ões, 2012.
21.Stevens KN, Lang IA, Guralnik JM, Melzer D. Epidemiology of balance and dizziness in a national population: findings from the English Longitudinal Study of Ageing. Age Ageing. 2008;37:300---5.
22.MaarsinghOR, Dros J, Schellevis FG,van WeertHC, Bindels PJ,Horst HE.Dizziness reportedbyelderly patientsin fam-ilypractice:prevalence,incidence,andclinicalcharacteristics. BMCFamPract.2010;11:2.
23.BittarRSM,OiticicaJ,BottinoMA,Gananc¸aFF,DimitrovR. Pop-ulationepidemiologicalstudyontheprevalenceofdizzinessin thecityofSãoPaulo.BrazJOtorhinolaryngol.2013;79:8---11. 24.Moraes SA, Soares WJ, Rodrigues RA, Fett WC, Ferriolli
E, Perracini MR. Dizziness in community-dewelling older adults: a population-based study. Braz J Otorhinolaryngol. 2011;77:691---9.
25.TakanoNA,CavalliSS,Gananc¸aMM,CaovillaHH,SantosMAO, PelusoETP,etal.Qualidadedevidadeidososcomtontura.Braz JOtorhinolaryngol.2010;76:769---75.
26.GámizMJ,Lopez-EscamezJA.Health-RelatedQualityofLifein patientsoversixtyyearsoldwithbenignparoxysmalpositional vertigo.Gerontology.2004;50:82---6.
27.AggarwalNT,BennettDA,BieniasJL,MendesdeLeonCF,Morris MC,EvansDA.Theprevalenceofdizzinessanditsassociation withfunctionaldisabilityinabiracialcommunitypopulation.J GerontolABiolSciMedSci.2000;55:288---92.
28.Lopes AR, Moreira MD, Trelha CS, Marchiori LLM. Asso-ciation between complaints of dizziness and hypertension in non-institutionalized elders. Int Arch Otorhinolaryngol. 2013;17:157---62.
29.TungvachirakulV,LisnichukH,O’LearySJ.Epidemiologyof ves-tibularvertigoinaneuro-otologyclinicpopulationinThailand. JLaryngolOtol.2014;128:31---8.
30.DrosJ,MaarsinghOR, BeemL,vanderHorstHE,terRietG, SchellevisFG,etal.Functionalprognosisofdizzinessinolder primarycarepatients:aprospectivecohortstudy.JAmGeriatr Soc.2012;60:2263---9.
32.TiensoliLO,CoutoER,MitreEI.Fatoresassociadosàvertigem outonturaem Indivíduoscom examevestibular normal.Rev CEFAC.2004;6:94---100.
33.BittarRSM.Labirintopatias hormonais: hormôniosesteroides, estrógeno e progesterona. Int Arch Otorhinolaryngol. 1997;1:32.
34.Gopinath B, McMahon CM, Rochtchina E, Mitchell P. Dizzi-nessand vertigoin anolderpopulation: theBlue Mountains prospective cross-sectional study. Clin Otolaryngol. 2009;34: 552---6.
35.BrohemVMA,CaovillaHH,Gananc¸aMM.Dossintomase acha-dosaudiológicosevestibularesemindivíduoscomhipertensão arterial.ActaAwho.1996;15:4---10.
36.ColledgeNR,Barr-HamiltonRM,LewisSJ,SellarRJ,WilsonJA. Evaluationofinvestigationstodiagnosethecauseofdizziness
inelderly people:a communitybasedcontrolledstudy.BMJ. 1996;313:788---92.
37.Cruz IBM, Barreto DCM, Fronza AB, Jung IVC, Krewer CC, Rocha MIUM, et al. Equilíbrio dinâmico, estilo de vida e estadoemocionaisemadultosjovens.BrazJOtorhinolaryngol. 2010;76:392---8.
38.PereiraCB,StruppM,HolzleitnerT,BrandtT.Smokingand bal-ance:correlationofnicotine-inducednystagmusand postural bodysway.Neuroreport.2001;12:1223---6.
39.MirallasNDR,ContiMHS,VittaA,LaurentiR,SaesSO.Avaliac¸ão ereabilitac¸ãovestibularnoindivíduoidoso.RevBrasGeriatr Gerontol.2011;14:687---98.