ABSTRACT
I N TROD UCTI ON
Over t he past decades, new developm ent s in r esin t echnology and pat ient dem and for t oot h-color ed r est orat ions led t o an incr eased use of resin-bonded iber-reinforced ixed partial dentures ( inlay FPDs) t o r eplace a single m issing t oot h, as report ed in several st udies1,4,13,24,31. The use of ult ra-high molecular weight polyethylene (UHMWP) ibers is based on t he im provem ent of t he com posit e resin m ech an ical pr oper t ies an d beh av iou r6 , 1 9 , 2 4. Th is improvement depends on the iber direction and pre- t reat m ent . I n order t o reinforce t he rest orat ion in multiple directions, woven iber and meshes have been pr oposed, w her e isot r opic pr oper t ies ar e achiev ed17, 24, 30. I ncor porat ed int o com posit e materials, the ibers provide enhanced fracture
I
nformation on the longevity of iber-reinforced composite ixed partial dentures (inlay FPDs) should be consider ed in t he select ion of m at er ials, operat ive t echniques and pat ient inst r uct ions r elat ed t o pr ognosis and long- t er m cost - effect iveness. Obj ect ive: Thisstudy evaluated the long-term survival of iber-reinforced, adhesively-bonded composite
pr ost heses placed in post er ior t eet h. Mat er ials and Met hods: Tw ent y- one pat ient s t hat received adhesively bonded polyet hylene inlay FPDs in post erior t eet h were select ed from a
private practice dental ofice and invited to evaluation. Of the eligible 21 patients, 13 (mean
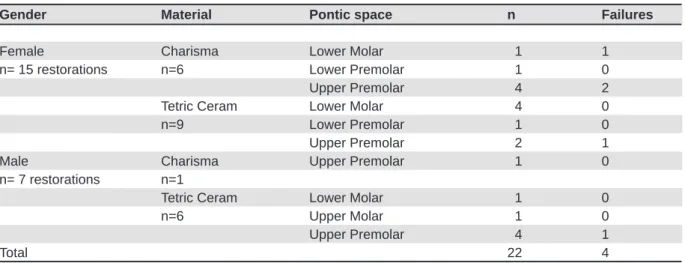
age 50.3 ± 11.5 year s) agr eed t o be enr olled as par t icipant s, pr oviding 22 r est orat ions, as several subj ect s pr esent ed m or e t han one inlay FPD. One dent ist placed all inlay FPDs
using Ribbond as reinforcement and Tetric Ceram/Durail or Charisma/Renamel composite
com bin at ion s, accor din g t o m an u fact u r er ’s in st r u ct ion s. Tw o in depen den t calibr at ed
operators performed the evaluation, using modiied USPHS criteria. Survival functions of
r est orat ions w er e analyzed w it h Kaplan- Meier and Log Rank t est (α = 0.05) . Result s: The m aj or it y of r est orat ions r eceived A or B scor es. Four ( 18.2% ) inlay FPDs fract ur ed am ong t he 22 evaluat ed. The m ean est im at e sur vival rat e was 7 year s ( 95% CI : 5.9 t o 8.1) ,
and the overall percentage of survival was 81.8%. There were no signiicant differences
( p> 0.05) bet w een com posit e com binat ions or t oot h locat ion considering all clinical aspect s
evaluated and survival functions. Conclusion: Posterior iber-reinforced ixed partial dentures
exhibit ed accept able clinical per for m ance aft er a per iod up t o 8 year s.
Ke y w or d s: Sur v ival rat e. Com posit e r esins. Fixed par t ial dent ur e. Fiber - r einfor ced com posit es.
Fixed part ial dent ures in an up t o 8-year follow- up
Maximiliano Sérgio CENCI1, Paulo Antônio da Rosa RODOLPHO2, Tatiana PEREIRA-CENCI1,
Altair Antoninha DEL BEL CURY3, Flávio Fernando DEMARCO4
1-DDS, MSc, PhD, Adjunct Professor, Department of Operative Dentistry, Dental School, Federal University of Pelotas, Pelotas, RS, Brazil. 2- DDS, Private Dental Practitioner, Caxias do Sul, RS, Brazil.
3- DDS, MSc, PhD, Professor, Piracicaba Dental School, State University of Campinas, Piracicaba, SP, Brazil.
4- DDS, PhD, Associate Professor, Department of Operative Dentistry, Dental School, Federal University of Pelotas, Pelotas, RS, Brazil.
Corresponding address: Flávio Fernando Demarco - Faculdade de Odontologia - Rua Gonçalves Chaves, 457 - Pelotas, RS - Brasil - 96015 560 - e-mail:
[email protected] - [email protected]
Received: January 27, 2009 - Accepted: August 25, 2009
r esist ance, indicat ing t heir applicat ion even w hen high st ress is present in t he oral environm ent10,12,25,28. Alt hough t hese const r uct ions w er e or iginally m ade of m et al com bined w it h feldspat hic ceram ic, inlay FPDs ar e cur r ent ly select ed due t o t heir var ious ad v an t ag es w h en com p ar ed t o m et al- cer am ic rest orat ions, as a t oot h- coloured m at erial, presence of an adhesive and t he t issue- saving pr oper t ies of t hese const r uct ions36.
Mor eover, as t he m aj or it y of t he st udies r epor t short- t erm evaluat ion periods11,15,34, t here is lim it ed inform at ion available on perform ance det erm inant s and r easons of failur e of inlay FPDs3,8,14,27,29. I n fact , t her e appear t o be few long- t er m clinical st udies r epor t ing sur vival rat es of post er ior polyet hylene iber-reinforced FPDs showing survival rates from 55 t o 86%2,3,16,20,21,33. Therefore, evidence report ing clinical perform ance of inlay FPDs m ainly from dat a generat ed in clinical pract ice is needed, especially as inform at ion on long- t erm survival is st ill scarce. The aim s of t his st udy w er e t o r epor t t he sur vival rat es of posterior iber-reinforced composite restorations and com par e t he per for m ance of t w o com posit e r esin com binat ions used in inlay FPDs placed in a privat e dent al pract ice. The follow- up period was up t o 8 year s ( ranging fr om 12 t o 96 m ont hs) .
M ATERI ALS AN D M ETH OD S
Th i s st u d y w as a p r osp ect i v e, l on g i t u d i n al evaluat ion, w her e t he case r epor t s of 2 1 adult pat ient s were select ed according t o pre- det erm ined inclusion cr it er ia am ong t he r egist er s of a pr ivat e p r act ice d en t al of f ice. Th ese cr it er ia in clu d ed pat ient s in cont inuous clinical follow- up considering success and failur es in t he last 8 year s t hat had received polyethylene iber-reinforced (Ribbond Co., Seat t le, WA, USA) adhesively bonded com posit e r esin 3- unit pr ost heses in post er ior t eet h. Resins used w er e Char ism a ( Heraeus- Kulzer, Wehr heim , Ger m an y ) t og et h er w it h Ren am el ( Cosm ed en t I nc., Chicago, I L, USA) or Tet r ic Ceram ( I voclar Vivadent I nc., Schaan, Liecht enst ein) t oget her wit h Durail (Heraeus-Kulzer); the resin combination for each inlay FPD was select ed by chance. Pat ient s pr esent ing parafunct ional habit s, loss of occlusal st abilit y or any m edical condit ion t hat im pair ed co r r e ct h y g i e n e p r o ce d u r e s w e r e e x cl u d e d . Ant agonist dent it ion was always in nat ural t eet h.
Po n t i c a r e a s l a r g e r t h a n 7 m m w e r e n o t
consider ed for t his t r eat m ent m odalit y. The pont ic was eit her a 2nd pr em olar or 1st m olar ( 5- 7 m m m esiodist al dist ance) , while t he abut m ent s were t he adj acent t eet h. Thir t een of t he 21 eligible pat ient s ( m ean age 50. 3± 11. 5 y ear s) m et t he inclusion cr it er ia and agr eed t o be enr olled as par t icipant s. All st udy subj ect s signed an infor m ed consent for m prior t o t he beginning of t he clinical evaluat ion. This st udy was appr oved by t he Univer sit y Resear ch Et h ics Com m it t ee. Alt h ou g h 1 3 p at ien t s w er e select ed , 2 2 r est or at ion s w er e con sid er ed , as several pat ient s pr esent ed m or e t han one inlay FPD ( Table 1) .
On e oper at or ( PARR) car r ied ou t all clin ical an d labor at or ial pr ocedu r es. Pr epar at ion s w er e per for m ed using a 245- car bide bur ( KG Sor ensen, São Paulo, SP, Brazil) t o rem ove previous rest orat ions and a 4137 ( KG Sor ensen) diam ond bur t o achieve t h e cav i t y co n ser v a t i v e a n d ex p u l si v e sh a p e sim ilar t o t hose for inlay r est orat ions as com m only descr ibed in lit erat ur e24, w it hout bevels in enam el. All cav it ies w er e r est r ict ed t o en am el m ar gin s. Cavit ies had a m inim um of 4 m m in dept h and widt h in t he occlusal box t o accom m odat e com posit e and ibers and also to prevent ibers’ exposure. The pr oxim al boxes w er e 6 t o 8 m m deep and 4 m m w ide ( Figur e 1) .
I m pr essions w er e t aken w it h a silicon r ubber i m p r e ssi o n m a t e r i a l ( Ex p r e ss, 3 M ESPE, St . Pa u l , MN , USA) u s i n g a 2 - s t e p p u t t y - w a s h impression technique and cavities were illed with a provisional m et hacrylat e m at erial ( Ferm it , I voclar Vivaden t I n c., Sch aan , Liech t en st ein ) , follow ed by color select ion per for m ed using a shade guide system (VITAPAN Classical, VITA Zahnfabrik, Bad Säckingen, Ger m any) .
Casts obtained with type I V dental stone ( Vigodent S.A. I ndúst ria e Com ércio, Rio de Janeiro, RJ, Brazil) w er e coat ed w it h cyanoacr y lat e ( Super Bonder, Loct it e, Brazil) pr ior t o laborat or y pr ocedur es. A 1 m m com posit e r esin incr em ent ( Char ism a or
Gender Material Pontic space n Failures
Female Charisma Lower Molar 1 1
n= 15 restorations n=6 Lower Premolar 1 0
Upper Premolar 4 2
Tetric Ceram Lower Molar 4 0
n=9 Lower Premolar 1 0
Upper Premolar 2 1
Male Charisma Upper Premolar 1 0
n= 7 restorations n=1
Tetric Ceram Lower Molar 1 0
n=6 Upper Molar 1 0
Upper Premolar 4 1
Total 22 4
Tet r ic Ceram ) was posit ioned in each pulpal- axial wall t o r et ain t he pr eviously adhesive m oist ened (Scotch Bond, 3M ESPE) polyethylene iber. The iber was positioned with its extremities within t he cav it ies on t he non- poly m er ized com posit e, follow ing pulpal and axial pr eparat ion cont our s. I n the pontic region, the iber was positioned 2 mm above gingival area. Next, composite and iber were polym erized for 40 seconds wit h a light- curing
unit operat ing at 600 m W cm- 2 ( Dem et r on LC Ker r, Orange CA, USA) ( Figur e 2) . An addit ional 1 m m incr em ent was placed and anot her polyet hy lene iber was positioned in the same way as the previous one. Rest orat ions w er e com plet ed incr em ent ally ( in 2- m m - t hick incr em ent s) and poly m er ized as descr ibed above. Gingival and buccal walls w er e co m p l et ed w i t h a m i cr o f i l l ed co m p o si t e r esi n (Durail or Renamel) to ascertain translucence and sur face sm oot hness32 ( Figur es 3) . A closer view is dem onst rat ing t he r est orat ions com plet ed ( Figur e 4) and being t est ed in t he m odel ( Figur e 5) .
A l l e n a m e l a n d c a v o s u r f a c e m a r g i n s o f p r ep ar at i o n s o n ab u t m en t s w er e aci d - et ch ed and coat ed w it h a bonding agent ( Single Bond, 3M ESPE). Fiber-reinforced ixed partial dentures w er e t r eat ed w it h alum inum oxide ( Micr o- et cher, Danville I nc., Danville, USA) , acid- et ched, coat ed w it h Single Bond and lut ed w it h Rely X ARC cem ent ( 3M ESPE) . Bonding agent s and com posit es w er e placed accor ding t o m anufact ur er ’s inst r uct ions, and FDPs w er e placed under r ubber dam isolat ion and polym er ized for 60 seconds on each aspect ( occlusal, buccal, and lingual) . Occlusal adj ust m ent s w er e car r ied out befor e cem ent at ion pr ocedur es. How ev er, w e r e- check ed occlusal cont act s aft er
Figure 1- Cast obtained after cavity preparation, with
conservative and expulsive shape, restricted to enamel margins, which provided an adequate restorative material thickness
Figure 2- The polyethylene iber was positioned in place
with a layer of composite resin
Figure 3- The ixed partial denture is completed with
additional composite layers
Figure 4- A closer view of the iber-reinforced ixed partial
denture after inishing and polishing procedures
Figure 5- The inished restoration placed in the cast
cem en t at ion , as d eb on d in g m ay b e r elat ed t o im pr oper occlusal adj ust m ent in FPDs34.
Fi n i sh i n g o f t h e r e st o r a t i o n s w a s ca r r i e d out befor e t he lut ing pr ocedur e and com plet ed im m ediat ely aft er placing. Cervical overhangs were r em ov ed w it h a # 1 2 scalpel blade and plast ic inishing strips (3M ESPE). Proximal margins were inished with Sof-Lex XT discs (3M ESPE). The occlusal surfaces were inished with ine diamond inishing burs (KG Sorensen), multibladed carbide bur s ( Jet Bur s) , and polished w it h alum inum oxide point s ( Flexicups, Cosm edent Co., Chicago I L, USA) an d a silicon e br u sh ( Jiffy Com posit e Polish in g Br u sh , Ult r aden t Sou t h Jor dan , UT, USA) , w it h a polish in g past e ( En am elize, Cosm eden t I n c., Chicago, I L, USA) ( Figure 6) . The sam e invest igat or t hat placed t he r est orat ions car r ied out baseline evaluat ions.
Dir ect ev alu at ion w as car r ied ou t w it h t h e
modiied USPHS criteria9,26.I ndir ect evaluat ion by st andard phot ographs ( Sony CyberShot DSC- F717, Sony Elect r onics I nc., Tokyo, Japan) was used t o com plem ent dat a fr om dir ect evaluat ion.
Tw o ca l i b r a t e d e x a m i n e r s ( MSC a n d TPC) w or ked independent ly t o per for m t he evaluat ion, and an int er- exam iner agr eem ent of 80 per cent or m or e was obt ained and consider ed st at ist ically accept able. Evaluat ion was blind in r elat ion t o t he exam iner s. Radiographic exam inat ion was car r ied out w hen necessar y t o com plem ent t he clinical evaluat ion. Addit ionally, all pat ient s had a com plet e annual per iapical radiographic ex am , w hich was exam ined by exam iner s.
Descr ipt ive st at ist ics w er e used t o descr ibe t he fr equency dist r ibut ions of t he evaluat ed cr it er ia. Differ ences bet w een m at er ial com binat ions w er e an aly zed w it h Ch i- sq u ar e t est an d d if f er en ces bet w een baseline and 96- m ont h evaluat ions w er e analyzed w it h McNem ar ’s t est (α= 0.05) . For each FPD evaluat ed, t he t im e t o failur e or longev it y in m ont hs was r ecor ded and t he sur vival of t he r est orat ions or subset s of r est orat ions gr ouped on t he basis of var iables ( m at er ial and t oot h locat ion) w e r e d i sp l a y e d u si n g Ka p l a n - Me i e r su r v i v a l curves7,18. Com parison bet ween survival curves was det er m ined w it h t he Log Rank t est .
RESULTS
Thir t een pat ient s ( 61.54% fem ale and 38.46% m ale, m ean age 50.31± 11.48) agreed t o part icipat e in the study. No statistically signiicant difference was found bet w een fem ale and m ale concer ning failu r e r at es ( Table 1 ) . Of t h e 1 5 Tet r ic Cer am + Durail restorations evaluated, 1 was replaced
Figure 6- Occlusal view of the definitive restoration
demonstrates esthetic integration relecting harmonious integration of form and function
Figure 7- Survival functions of iber-reinforced ixed partial dentures according to composites combinations. Differences
Tooth Location
Estimate Standard Error Lower Bound Upper Bound
Maxilla 82.32 10.35 62.04 102.60
Mandible 76.00 1.63 72.80 79.20
Overall 84.00 6.95 70.37 97.63
95% Conidence Interval
Mean Table 4- Means for survival time in months according to tooth location
Criteria
Baseline Up to 96-month Baseline Up to 96-month
Color Match A 7 4 15 14
B 0 0 0 0
C 0 0 0 0
Marginal Adaptation A 7 3 15 11
B 0 1 0 3
C 0 0 0 0
Anatomic Form A 7 3 15 13
B 0 1 0 1
C 0 0 0 0
Surface Roughness A 7 4 15 14
B 0 0 0 0
C 0 0 0 0
Marginal Staining A 7 2 15 9
B 0 2 0 5
C 0 0 0 0
Occlusal Contacts A 7 3 15 14
B 0 1 0 0
C 0 0 0 0
Sensitivity A 7 4 15 14
B 0 0 0 0
C 0 0 0 0
Secondary Caries A 7 4 15 14
B 0 0 0 0
Inlay FPDs Retention A 7 4 15 14
B 0 0 0 0
Tetric Ceram + Durail
Charisma + Renamel
Restorative Material
Table 2- Results of direct assessment for the iber-reinforced composite ixed partial dentures (FPDs) that remained in
place after the evaluation period
No statistically signiicant differences were found between materials (qui square test) or between baseline and inal evaluation (McNemar test) considering any clinical aspect evaluated (p>0.05). Scores A and B were considered as success (except for secondary caries and inlay FPDs retention) for statistical analysis.
Material
Estimate Standard Error Lower Bound Upper Bound
Charisma / Renamel 81.00 11.78 58.51 104.69
Tetric Ceram / Durail 69.00 6.36 56.53 81.47
Overall 84.00 6.95 70.37 97.63
95% Conidence Interval
du r in g t h e clin ical ser v ice, an d 1 4 r est or at ion s rem ained wit hout any addit ional t reat m ent . Of t he 7 Charism a + Renam el rest orat ions, 3 were replaced, w it h 4 r est orat ions r em aining in loco. All 4 failur es r ecor d ed w er e f r act u r e- r elat ed , an d f r act u r es always occur r ed in t he abut m ent - pont ic j unct ions. Th e m aj or it y of t h e r est or at ion s ev alu at ed exhibit ed scor e A in all of t he evaluat ed cr it er ia ( Table 2) . Neit her m at er ial nor t im e of evaluat ion demonstrated to be signiicant factors regarding any clinical aspect direct ly evaluat ed ( p> 0.05) . No case of secondar y car ies was found for bot h m at er ials ( Table 2) . Kaplan Meier overall sur vival pr obabilit y at 8 year s was 34.2% ( m ean est im at e sur vival of 7 year s) ( Tables 3 and 4) . Ther e w er e no st at ist ically signiicant differences (p>0.05) between survival f u n ct ion s t o com posit es com bin at ion s or t eet h locat ion by t he Log Rank Test ( Figur es 7 and 8) .
D I SCUSSI ON
L o n g i t u d i n a l , p r o s p e c t i v e s t u d i e s a n d r et r ospect ive analy ses of dent al r ecor ds ar e t he only feasible t ools t o use in evaluat ing t he long-t erm perform ance of reslong-t oralong-t ions in vivo. This slong-t udy w as an up t o 8 year s longit udinal r et r ospect ive clinical- follow up evaluat ing t he per for m ance of adhesively bonded iber-reinforced composite ixed par t ial dent ur es.
The success rate of irst-generation, multiphase polymer matrix iber-reinforced composite FDPs i n cl u d i n g su r f ace- i n l ay - an d h y b r i d - r et ai n ed designs and consist ing of 1 t o 3 pont ics was 93% aft er a m axim um of t w o year s follow- up34. Ot her st u d ies h av e also r ep or t ed h ig h su r v iv al r at es ( 100% at 12, 15 and 24 m ont hs) for 3- unit
inlay-retained iber-reinforced composites FDPs with shor t - t er m follow- up2,11,15. Clinical per for m ance of surface-retained adhesive composite ixed partial dent ures reinforced by an UHMWP has also report ed a 9 1 . 3 % su r v ival at t h e en d of t w o y ear s an d 78.3% aft er a m axim um of 3 years33. I n t he present st udy, t he overall est im at e survival m ean was of 84 m ont hs ( 7 years) for t he rest orat ions in t he present st udy, and t he overall per cent age of sur vival was 81. 8% . Pr öbst er and Henr ich23 ( 1997) r epor t ed 61% of overall sur vival rat es and 76% of funct ional survival rates for metal framework ixed partial dent ur es aft er an 11- y ear per iod of evaluat ion, w h ile r ep or t ed sig n if ican t ly h ig h er ov er all an d funct ional sur v ival rat es aft er 6 3 m ont hs, 7 5 % and 93%, respectively in iber-reinforced ones. Alt h ou gh it is n ot possible t o dir ect ly com par e metal-ceramic to iber-reinforced FPDs with regard t o t heir m echanical pr oper t ies, w hen consider ing t heir survival, t hey should be com pared considering t heir cost , less t im e- consum ing procedure, m at erial color, pr esence of an adhesive and t issue- saving pr oper t ies36. The low er sur vival rat es found in t he pr esent st udy can be at t r ibut ed t o t he lar ge range ( 12 t o 96 m ont hs) of clinical ser vice t im e r epor t ed. Yet , su ccess r at es m igh t also be affect ed by a long- t er m assessm ent , i.e., inlay FPDs evaluat ed aft er a deliver y per iod of t w o year s or m or e m ay ex hibit a t w ice- higher failur e r isk8. Addit ionally, f i b e r - r e i n f o r ce d co m p o si t e r e st o r a t i o n s m a y pr esent differ ent m echanical pr oper t ies com par ed t o cast alloys and t he differ ences r elat ed t o t he adhesive properties may inluence the survival rat es. How ever, t he est im at e m ean sur vival was higher t han t he 55.03 m ont hs described by Vallit t u35 ( 2004) , which is associat ed t o t he longer evaluat ion
Figure 8- Survival functions of iber-reinforced ixed partial dentures according to tooth location. Differences among curves
per iod r epor t ed in t he pr esent st udy.
Lo n g e v i t y o f f i x e d p a r t i a l d e n t u r e s f i b e r -r ein fo-r ced com posit e -r est o-r at ion s is depen den t upon m any differ ent fact or s, including m at er ial, m ax i l l ar y or m an d i b u l ar ar ch es, p at i en t - an d dent ist - r elat ed. Mor eover, pat ient fact or s such as oral hygiene, diet ar y habit s, pr event ive m easur es, f l u o r i d e av ai l ab i l i t y, co m p l i an ce i n r ecal l an d cooperat ion during t reat m ent , and oral environm ent are relevant t opics when considering t he rest orat ion durabilit y21. Alt hough t he evidence t hat inlay FPDs placed in t he m andible show a higher failur e r isk t han t hose placed in t he m axilla8, in t he pr esent st udy m axillary and m andibular rest orat ions did not differ in sur vivals, in agr eem ent w it h t he pr evious indings reported by Vallittu3 5 ( 2 0 0 4 ) . How ev er, fur t her clinical invest igat ions ar e st ill needed for im proved long- t erm clinical perform ance, as clinical trials with larger number of inlay FPDs could conirm or decline differ ences bet w een ar ches. The m ain reason for failure in t he present st udy was fract ure, w hilst neit her secondar y car ies nor post operat ive sensit ivit y was r elat ed. I t is im por t ant t o highlight t hat t he clinical envir onm ent w her e t he inlay FPDs were placed has a dent al pract ice focused on healt h pr om ot ion, w it h a pr event ive appr oach and based on t he cont rol of caries disease. I n addit ion, pat ient s included in t his st udy had r egular ly at t ended t he dental ofice with at least one appointment per year.
Fi b e r - r e i n f o r ce d p a r t i a l d e n t u r e s f r a ct u r e st r engt h depends on several fact or s including t he elast ic m odulus of t he suppor t ing subst r uct ur e, t he pr eparat ion design, occlusal load of t he span and t he charact er ist ics of t he m anufact ur ing and lab or at or y p r ocess, an d t h e m at er ials u sed t o fabr icat e t he pr ost hesis24. The failur es r ecor ded in t he pr esent st udy could som ew hat be at t r ibut ed to cavity preparation deiciency and/or excessive occlusal load as r esult of a slight ly lar ger int er-abut m ent dist ance. I n addit ion, clinical t r ials have det erm ined t hat larger prost het ic spaces especially in m andible ar e a pot ent ial r isk fact or for post er ior inlay FPDs8, and t her efore should be avoided. All fract ur ed inlay FPDs w er e r eplaced aft er cav it y r e- cont our ing, and no im m ediat e evidence of new failur es was r ecor ded subsequent ly, em phasizing t he im por t ance of adequat e cavit y pr eparat ion in order t o provide adequat e fract ure st rengt h t o inlay FPDs. Conv er sely, few st udies hav e focused on cavit y preparat ion for inlay FPDs, and t he principles governing st andard cavity preparat ion have not been well est ablished24,27. When m aking box preparat ions for an inlay FPD, if pr e- exist ing r est orat ions ar e p r esen t , t h ey can d et er m in e ab u t m en t sh ap e. Ot her w ise, w hen t eet h ar e int act , m echanical and biological aspect s m ust be consider ed in choosing t he pr eparat ion design: t he occlusal box should be suficiently deep to accommodate the iber and a
pr ot ect ive layer of com posit e; and t he pr ox im al box should be as deep as possible in t he gingival direction to ensure an adequate amount of iber and com posit e, and t o pr ovide m axim al st r engt h in t he connect ion ar ea. Also, t he m ar gins m ust be locat ed w it hin t he enam el for bet t er long- t er m m ar ginal adapt at ion24,27, and t o assur e t he cor r ect dental bioilm control and avoid tissues diseases.
The reduct ion in sound dent al st ruct ure rem oval, t he bonding capacit y - pr event ing m icr oleak age an d r ei n f o r ci n g t h e r em n an t d en t al st r u ct u r e w h en com p ar ed t o ot h er f r am ew or k m at er ials an d t h e est h et ics ar e som e of t h e r eason s f or the increasing use of iber-reinforced composite ixed partial dentures placement. The results of this investigation suggest that iber-reinforced ixed partial dentures may be a feasible choice for a long- t er m pr ovisional t r eat m ent for a single t oot h r eplacem ent . Despit e t he sm all num ber of pat ient s in t his st udy, t he r esult s w er e obt ained follow ing a st andar dized pr ot ocol, w it h a single o p er a t o r p l a ci n g t h e r est o r a t i o n s, a n d u si n g on ly t w o differ en t com bin at ion s of com posit es. Information on clinical survival of iber-reinforced ixed partial dentures lacks in literature22, and hence
the indings of the present study may help bringing int o discussion som e im por t ant aspect s r elat ed t o t h e per f or m an ce of t h ese r est or at ion s, w it h som e int er est ing clinical obser vat ions. How ever, a larger num ber of evaluat ed rest orat ions and longer evaluat ion per iods in m ult icent er st udies could be m or e appr opr iat e in or der t o generat e st r onger scientiic evidence.
CON CLUSI ON
The r esult s of t his st udy suggest t hat clinical performance of posterior iber-reinforced ixed par t ial dent ur es evaluat ed was accept able aft er a per iod of up t o 8 year s, and t hat inlay FPDs m ay be a feasible alt er nat ive for t he r eplacem ent of a single m issing t oot h.
REFEREN CES
1- Aj louni R, Aj louni K, Oonsom bat C, Ruder G. Conser vat ive inlay ixed partial denture: a clinical and laboratory technique. Gen Dent . 2005; 53: 266- 9.
2- Ayna E, Celenk S. Polyethylene iber-reinforced composite inlay ixed partial dentures: two-year preliminary results. J Adhes Dent. 2005; 7: 337- 42.
3- Behr M, Rosent r it t M, Handel G. Fiber- r einfor ced com posit e crowns and FPDs: a clinical report . I nt J Prost hodont . 2003; 16: 239-43.
4- Belvedere PC. Single-sitting, iber-reinforced ixed bridges for t he m issing lat eral or cent ral incisor s in adolescent pat ient s. Dent Clin Nor t h Am . 1998; 42: 665- 82.
6- Colán Guzm án P, Fr eit as FF, Fer r eira PM, Fr eit as CA, Reis KR. Inluence of different cantilever extensions and glass or polyaramide reinforcement ibers on fracture strength of implant-suppor t ed t em porar y. J Appl Oral Sci. 2008; 16: 111- 5.
7- Collet D. Modelling sur vival dat a in m edical r esear ch. London: Chapm an & Hall; 1994.
8- Cr euger s NH, Van't Hof MA. An analysis of clinical st udies on r esin- bonded br idges. J Dent Res. 1991; 70: 146- 9.
9 - Rosa Rod olp h o PA, Cen ci MS, Don assollo TA, Log u ér cio AD, Dem ar co FF. A clinical evaluat ion of post er ior com posit e restorations: 17-year indings. J Dent. 2006;34:427-35. 1 0 - Dy er SR, Sor en sen JA, Lassila LV, Vallit t u PK. Dam ag e mechanics and load failure of iber-reinforced composite ixed par t ial dent ur es. Dent Mat er. 2005; 21: 1104- 10.
11- Edelhoff D, Spiek er m ann H, Yildir im M. Met al- fr ee inlay-retained ixed partial dentures. Quintessence Int. 2001;32:269-81. 12- Ellakwa AE, Shortall AC, Marquis PM. Inluence of different t echniques of laborat or y const r uct ion on t he fract ur e r esist ance of iber-reinforced composite (FRC) Bridges. J Contemp Dent Pract . 2004; 15: 1- 13.
13- Ferreira ZA, Carvalho EK, Mitsudo RS, Bergamo PM. Bondable r einfor cem ent r ibbon: clinical applicat ions. Quint essence I nt . 2000; 31: 547- 52.
14- Fr eilich MA, Meier s JC, Duncan JP, Eckr ot e KA, Goldber g AJ. Clinical evaluation of iber-reinforced ixed bridges. J Am Dent Assoc. 2002; 133: 1524- 34.
15- Göhr ing TN, Mor m ann WH, Lut z F. Clinical and scanning electron microscopic evaluation of iber-reinforced inlay ixed par t ial dent ur es: pr elim inar y r esult s aft er one year. J Pr ost het Dent . 1999; 82: 662- 8.
16- Göhring TN, Roos M. Inlay-ixed partial dentures adhesively retained and reinforced by glass ibers: clinical and scanning electron microscopy analysis after ive years. Eur J Oral Sci. 2005; 113: 60- 9.
17- Kanie T, Fuj ii K, Ar ikawa H, I noue K. Flexural pr oper t ies and im pact st r engt h of dent ur e base polym er r einfor ced w it h w oven glass ibers. Dent Mater. 2000;16:150-8.
18- Kaplan EL, Meier P. Nonparam et ric est im at ion from incom plet e obser vat ions. J Am St at ist Assoc. 1958; 53: 457- 81.
19- Kau K, Rudo DN. A t echnique for fabr icat ing a r einfor ced com posit e splint . Tr ends Tech Cont em p Dent Lab. 1992; 9: 31- 3. 20- Monaco C, Fer rar i M, Miceli GP, Scot t i R. Clinical evaluat ion of iber-reinforced composite inlay FPDs. Int J Prosthodont. 2003; 16: 319- 25.
21- Piovesan EM, Demarco FF, Piva E. Fiber-reinforced ixed-partial dent ur es: a pr elim inar y r et r ospect ive clinical st udy. J Appl Oral Sci. 2006; 14: 100- 4.
22- Pjetursson BE, Tan WC, Tan K, Brägger U, Zwahlen M, Lang NP. A syst em at ic r eview of t he sur vival and com plicat ion rat es of r esin- bonded br idges aft er an obser vat ion per iod of at least 5 year s. Clin Oral I m plant s Res. 2008; 19: 131- 41.
23- Pr öbst er B, Henr ich GM. 11- year follow- up st udy of r esin-bonded ixed partial dentures. Int J Prosthodont. 1997;10:259-68. 24- Rappelli G, Coccia E. Fiber-reinforced composite ixed partial den t u r e t o r est or e m issin g post er ior t eet h : a case r epor t . J Cont em p Dent Pract . 2005; 6: 168- 77.
2 5 - Ru d o D N , Ka r b h a r i VM. Ph y s i c a l b e h a v i o r s o f f i b e r r einfor cem ent as applied t o t oot h st abilizat ion. Dent Clin Nor t h Am . 1999; 43: 7- 35.
26- Schm alz G, Ryge G. Reprint of crit eria for t he clinical evaluat ion of dent al rest orat ive m at erials. Clin Oral I nvest ig. 2005; 9: 215- 32. 27- Song HY, Yi YJ, Cho LR, Par k DY. Effect s of t w o pr eparat ion designs and pont ic dist ance on bending and fract ur e st r engt h of iber-reinforced composite inlay ixed partial dentures. J Prosthet Dent . 2003; 90: 347- 53.
28- St iesch- Scholz M, Schulz K, Bor cher s L. I n v it r o fract ur e resistance of four-unit iber-reinforced composite ixed partial dent ur es. Dent Mat er. 2005; 22: 374- 81.
29- Strassler HE, Serio CL. Single-visit natural tooth pontic ixed partial denture with iber reinforcement ribbon. Compend Contin Educ Dent . 2004; 25: 224- 30.
30- Tezvergil A, Lassila LV, Vallittu PK. The effect of iber orientation on the thermal expansion coefficients of iber-reinforced com posit es. Dent Mat er. 2003; 19: 471- 7.
3 1 - Tr u sh k ow sk y R. Fib er - r ein f or ced com p osit e b r id g e an d splint . Replacing congenit ally m issing t eet h. N Y St at e Dent J. 2004; 70: 34- 8.
3 2 - Tr u sh k ow sk y R. Ver sat ilit y of r esin com p osit e: est h et ic considerat ions. Com pend Cont in Educ Dent . 2001; 22: 352- 61. 33- Unlu N, Belli S. Three-year clinical evaluation of iber-reinforced composite ixed partial dentures using prefabricated pont ics. J Adhes Dent . 2006; 8: 183- 8.
34- Vallittu PK, Sevelius C. Resin-bonded, glass iber-reinforced composite ixed partial dentures: a clinical study. J Prosthet Dent. 2000; 84: 413- 8.