ISSN 2321-4287
Review Article
ON THE VARIATIONS OF CERVICAL DERM ATOM ES
Henrietta Redebrandt Nittby, M D, PhD *
1,2, Tom Bendix, M D, Dr M ed Sci
1.
ABSTRACT
Address for Correspondence: Henrietta Nitt by, M D,Depart ment of Neurosurgery, Skåne Univer-sit y Hospital, Lund UniverUniver-sit y, Sw eden, BM C D10 SE-221 85 Sw eden.
E-M ail : henrietta.nitt [email protected]
Access this Article online
Quick Response code Web site:
* 1 Center for Rheumat ology and Spinal Diseases, Glost rup Hospital, Universit y of Copenhagen,
Glost rup, Denmark.
2 Depart ment of Neurosurgery, Skåne Universit y Hospital, Lund Universit y, Sw eden.
Background: Ner ve-root relat ed der m at om es have been considered t o have quit e solid anat om ical f ram ings.
How ever, especially in t he lum bar region, st udies have quest ioned such firm anat omy. Regarding t he cervical ner ve root s, m any st udies have show n an overlap bet w een different derm at om es, w hich of course affect s decisions taken in t he clinical w ork. All t he sam e, derm at om e draw ings w it h clear borders are st ill w idely used.
Context and purpose of the study:We conduct ed a lit erat ure review in order t o find t oday’s stat e of t he art ,
including t he m et hods on w hich t he anat om ical at lases have been based. The overall pragm at ic t hought s w ere t o creat e sum m arized guide for clinicians w hen t rying to correlat e an M RI-dem onst rated prolapse/ recess st enosis t o pain and neurologic findings, part icularly if t he nerve root ’s peripheral neurology does not follow convent ional anat omy.
Results: We isolat ed 24 st udies t hat suff icient ly dealt w it h t he issue of cervical derm at om es. Pain and sensory
dist urbance caused by cervical root affect ion could deviat e from t he derm at om al patt erns. We found indicat ions t hat som et im es no paralysis or anaest hesia w ould be seen aft er sect ion of a single root . Because t he fract ion of cases w it hout classical fit bet w een nerve root and anat om ical level cannot be given, st udies should go int o t his issue.
Conclusion: There are many st udies showing t hat derm at om al dist ributions are varying, and not only overlapping.
We t herefore m ean t hat new st udies, w it h m oder n im aging and surgical t echniques, are m uch needed.
KEYW ORDS: Cervical nerve root , derm at om e, radicular pain, radiculopat hy.
INTRODUCTION
Int ernat ional Journal of Anatomy and Research,
Int J Anat Res 2014, Vol 2(3):462-69. ISSN 2321- 4287
Received: 17 June 2014
Peer Review : 17 June 2014 Published (O):31 July 2014 Accepted: 07 July 2014 Published (P):30 Sep 2014 Internat ional Journal of Anat omy and Research
ISSN 2321-4287 w w w.ijmhr.org/ ijar.ht m
Acco r d in g t o t he Oxf o r d d i ct i o n ar i es, a dermat ome is “ an area of t he skin supplied by nerves from a single spinal root ”. During t he 19th and 20t h cen t u r i es, t h e est ab l i shm en t o f dermat omes and anat omical st udies att racted focus. Int erest ingly, in som e st udies, it w as present ed t hat t here w as an overlap of t he dermat omal patterns as w ell. In t he latter part s of t he 20t h cent ury, t his was furt her invest igated t hrough root stimulations, eit her w it h blockades or pain provocat ion, w hen t rying t o define t he
years, but also from t he beginning of t he last cent u r y, t he o ver l ap b et w een d if f eren t dermat omal levels has been described repeat-edly. Nevert heless, st andardised derm at om al maps w it h linear borders are st ill used in text books Therefore, t he aim was t o perform e a review on avai lable st udies o f anat o m ical locat ions of cervical derm a- and myot om es’ overlap, and cervical-level variat ions from t hose t radit ionally believed.
M ATERIALS AND M ETHODS
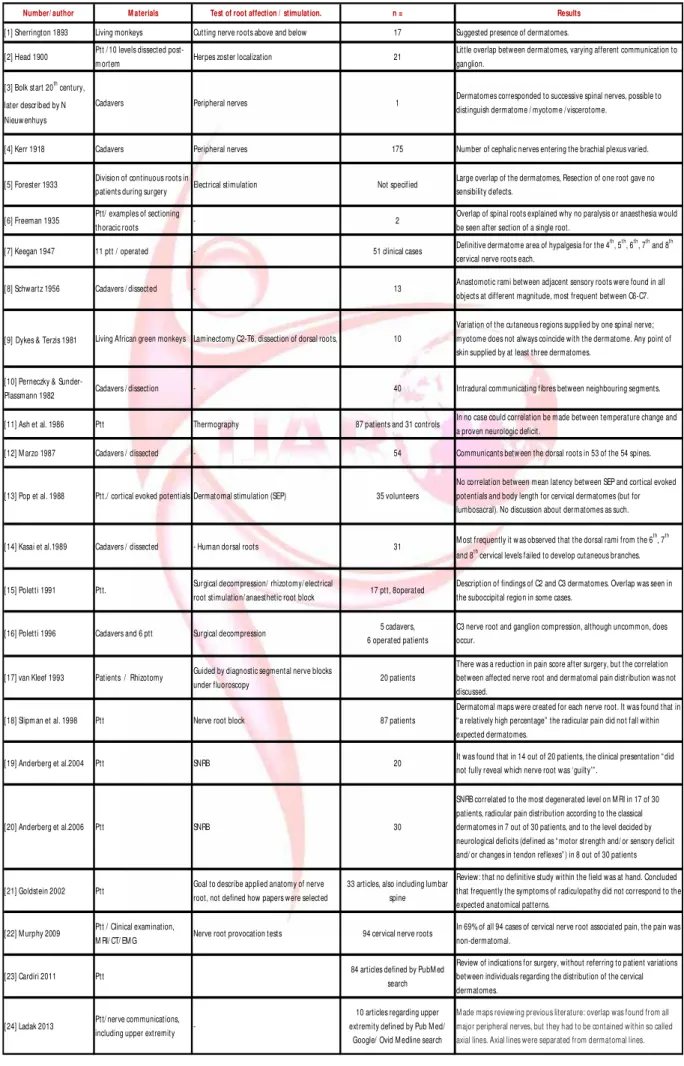
We designed our st udy in order t o ident ify current art icles covering t he issue of cervical dermat ome locat ions. A PubM ed search was per for m ed, w it h t h e w o rds “ cer vical” and “ derm at om e”. From t he art icles found, t he relevant ones w ere sort ed out by review ing eit her t it le or, w hen in doubt , also abst ract s. In order t o be able t o cover in a larger number of art icles t han t hose found in a PubM ed search, and above all t hose original w orks from t he beginning of t he 19t h cent ury and start of t he 20t h cent ury, also references from t hose art icles selected in the PubM ed search w ere considered.
RESULTS
PubM ed search
A PubM ed search including t he w ords “ cervical dermat ome” gave 183 hit s (2014 M arch 20t h), ten of t hem (Ladak et al. 2013; M urphy et al. 2009; Anderberg et al. 2006; Polett i 1991 and 1996; Kasai et al. 1989; van Kleef et al. 1993; Keegan 1947, Pop et al. 1989 and Ash et al.1986) w er e fo cu si n g m o r e d i rect ly u po n t h e dermat omes and t heir anat omical dist ributions, as selected by t it le and abst ract (see Figure 1). The r ef er en ce l i st s o f t h e ar t i cl es w er e considered, and as selected by t it le and abst ract anot her 14 relevant papers w ere defined. For a summary, see Table 1.
Results presented in chronological order
t hen determined t he area w here pain sensat ion r em ain ed , an d su ggest ed t hat t h is w o ul d correspond t o dermat omes.
[2] Sir Henry Head and Campbell (1900) st udied 21 p at i en t s w it h her p es zost er, w hi ch i s supposed t o affect t he dorsal spinal ganglia and give rise t o erupt ions in t he skin. His dermatomal patterns based upon t his show ed litt le overlap. Bot hcervical, t horacic and lumbar dermat omes w ere examined. Ten levels w ere examined post-mortem and found t o be correct ly numbered, but regarding t he cervical levels only t he 3rd and 4t h w ere examined in t his way. Interest ingly, t he aut hors w rot e: “ We are also confront ed w it h anot her difficult y w hich must always make such a combined diagram incomplete; for t he supply of t he afferent ganglionic fibers is subject t o variat ion, and any one port ion of skin may be supplied in t he one pat ient by t he fibers t hat enter one ganglion, in anot her by t hose t hat enter t he ganglion above or below.”
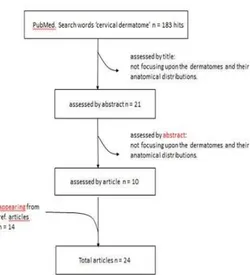
[3] Bolk at t he start of t he 20t h cent ury (cited in Nieuw enhuys 1975) carried out dissect ions of peripheral nerves, t hrough t heir plexus and t o t he spinal root s. He meant t hat the spinal nerves represented t heir original spinal segment s. He p r esen t ed dr aw in gs sh o w in g t h at t h e dermat omes corresponded t o successive spinal ner ves and m eant t hat : “ in principle, each segm ent enco m p asses a par t of al l o rgan systems: it is t herefore possible t o dist inguish a d er m at o m e, a m yo t o m e, a scl ero t om e, a neurot ome, a vasot ome and a viscerot ome or splanchnot ome.”
[4] Albert Kerr in 1918 presented a summary of cadaver dissect ions, w here peripheral nerves had been dissect ed and follow ed, result ing in 400-500 diagrams, from which 175 w ere chosen. These 175 diagram s w ere evaluat ed by t he author as scient ifically correct. The anterior rami entering t he brachial plexus w ere recorded. It was found t hat t he number of cephalic nerves entering t he plexus varied. This meant t hat in some cases t he 4th cervical root joined t he plexus (63%), in some cases t he cephalic limitat ion was t he 5th cervical root (30%) and finally, somet imes only a part of t he 5t h cervical root was included (7%).
[5] In 1933, Foerster made a t horough summary Older st udies from t he end of t he 19t h and start
of t he 20t h cent ur ies – including dissect ion st udies
ISSN 2321-4287
Number/ author M aterials Test of root affection / stimulation. n = Results
[1] Sherrington 1893 Living monkeys Cutting nerve roots above and below 17 Suggested presence of dermatomes.
[2] Head 1900 Ptt / 10 levels dissected
post-m ortepost-m Herpes zoster localization 21
Little overlap between dermatomes, varying afferent communication to ganglion.
[3] Bolk start 20th century,
later described by N Nieuw enhuys
Cadavers Peripheral nerves 1 Dermatomes corresponded to successive spinal nerves, possible to distinguish dermatome / myotom e / viscerotome.
[4] Kerr 1918 Cadavers Peripheral nerves 175 Number of cephalic nerves entering the brachial plexus varied.
[5] Forester 1933 Division of continuous roots in
patients during surgery Electrical stimulation Not specified
Large overlap of the dermatomes, Resection of one root gave no sensibility defects.
[6] Freeman 1935 Ptt/ examples of sectioning
thoracic roots - 2
Overlap of spinal roots explained why no paralysis or anaesthesia would be seen after section of a single root.
[7] Keegan 1947 11 ptt / operated - 51 clinical cases Definitive dermatome area of hypalgesia for the 4
th
, 5th, 6th, 7th and 8th cervical nerve roots each.
[8] Schwartz 1956 Cadavers / dissected - 13 Anastomotic rami between adjacent sensory roots were found in all objects at different magnitude, most frequent between C6-C7.
[9]Dykes & Terzis 1981 Living African green monkeys Laminectomy C2-T6, dissection of dorsal roots, 10
Variation of the cutaneous regions supplied by one spinal nerve; myotome does not always coincide with the dermatome. Any point of skin supplied by at least three dermatomes.
[10] Perneczky &
Sunder-Plassmann 1982 Cadavers / dissection - 40 Intradural communicating fibres between neighbouring segments.
[11] Ash et al. 1986 Ptt Thermography 87 patients and 31 controls In no case could correlation be made between temperature change and a proven neurologic deficit.
[12] M arzo 1987 Cadavers / dissected - 54 Communicants betw een the dorsal roots in 53 of the 54 spines.
[13] Pop et al. 1988 Ptt./ cortical evoked potentials Dermatomal stimulation (SEP) 35 volunteers
No correlation between mean latency between SEP and cortical evoked potentials and body length for cervical dermatomes (but for lumbosacral). No discussion about dermatomes as such.
[14] Kasai et al.1989 Cadavers / dissected - Human dorsal roots 31 M ost frequently it w as observed that the dorsal rami from the 6
th
, 7th and 8th cervical levels failed to develop cutaneous branches.
[15] Poletti 1991 Ptt. Surgical decompression/ rhizotomy/ electrical
root stimulation/ anaesthetic root block 17 ptt, 8operated
Description of findings of C2 and C3 dermatomes. Overlap was seen in the suboccipital region in some cases.
[17] van Kleef 1993 Patients / Rhizotomy Guided by diagnostic segmental nerve blocks
under fluoroscopy 20 patients
There was a reduction in pain score after surgery, but the correlation between affected nerve root and dermatomal pain distribution was not discussed.
[18] Slipm an et al. 1998 Ptt Nerve root block 87 patients
Dermatomal maps were created for each nerve root. It was found that in “ a relatively high percentage” the radicular pain did not fall within expected dermatomes.
[19] Anderberg et al.2004 Ptt SNRB 20 It was found that in 14 out of 20 patients, the clinical presentation “ did not fully reveal which nerve root was ‘guilty’” .
[20] Anderberg et al.2006 Ptt SNRB 30
SNRB correlated to the most degenerated level on M RI in 17 of 30 patients, radicular pain distribution according to the classical dermatomes in 7 out of 30 patients, and to the level decided by neurological deficits (defined as “ motor strength and/ or sensory deficit and/ or changes in tendon reflexes” ) in 8 out of 30 patients
[21] Goldstein 2002 Ptt Goal to describe applied anatomy of nerve root, not defined how papers were selected
33 articles, also including lum bar spine
Review: that no definitive study within the field was at hand. Concluded that frequently the symptoms of radiculopathy did not correspond to the expected anatomical patterns.
[22] M urphy 2009 Ptt / Clinical examination,
M RI/ CT/ EM G Nerve root provocation tests 94 cervical nerve roots
In 69% of all 94 cases of cervical nerve root associated pain, the pain was non-dermatomal.
[23] Cardiri 2011 Ptt 84 articles defined by PubM ed search
Review of indications for surgery, without referring to patient variations between individuals regarding the distribution of the cervical dermatomes.
[24] Ladak 2013 Ptt/ nerve communications, including upper extremity
-10 articles regarding upper extremity defined by Pub M ed/
Google/ Ovid M edline search
M ade maps review ing previous literature: overlap was found from all major peripheral nerves, but they had to be contained within so called axial lines. Axial lines were separated from dermatomal lines. [16] Poletti 1996 Cadavers and 6 ptt Surgical decompression C3 nerve root and ganglion compression, although uncomm on, does
of der m at om al research up t o t hat dat e. A dermat om e was defines as “ t he area of skin w hich is supplied by t he fibres of a certain spinal root ”. It could be defined t hrough anat omy or physiology. A draw back w it h t he anat om ical m et h o d w as m ean t t o b e t h at t he l ast ramificat ions of t he distal nerve fibres could not b e f o ll o w ed . As p hy si ol o gical m et ho d s strychnine intoxication of the posterior root s was ment ioned, and t he aut hor referred t o a st udy by Dusser de Barenne, w here hyperaest het ic areas w ere defined and a large degree of overlap of derm at om es adjacent t o each ot her w as observed. It was also referred back t o w ork by Sir Henry Head, w ho made dermat omal st udies based upon herpet ic lesions and found out t hat t here was almost no overlap of the dermat omes. Thus, already at t hat t ime, t here was a discussion about dermat omal overlap and correlat ion t o t he nerve root s. Foerst er him self cont ribut ed w it h know ledge w it hin t he area by present ing cases w here cont iguous root s w ere divided and a single root in t he middle was left intact , during w hich t he border of sensibilit y was defined. This was t he case for all lumbar root s and for t he 6t h and 2ndcervical root s. Ot her cervical root s w ere elect rically st im ulat ed and vasodilatat ion w as obser ved. Pict ures of t he pat ient s and t he derm at omal patterns pict ured on t hem w ere presented. Problems w ere t hat neit her was t he variat ion bet w een subject s fully described, nor exact ly how many pat ient s w ho w ere act ually included in t he st udy. Foerst er cam e t o t he conclusion t hat t here was a large overlap of t he dermat omes, and that resection of one root gave no sensibilit y defect s.
[6] In 1935, Freeman debated t hat overlap of spinal root s explained w hy no paralysis or anaest hesia w ould be seen after sect ion of a single root . He w rote t hat : “ It has been know n for a long t ime t hat sect ion of a single spinal root is follow ed by neit her paralysis nor sensory loss of any im port ance, but t hat cut t ing of t w o adjacent root s is follow ed by such loss.” He f u r t h er m ean t t h at t h e di v i si o n b et w een adjacent segment s should be made betw een the upper and low er point s of each t w o adjacent root s at each level. He concluded t hat t his was t he reason that t here was neit her t otal paralysis nor sensory loss from damaging just one single
root . Regarding dorsal ner ve root s, he also commented upon t he fact t hat t he anaest hesia result ing from cutt ing t w o adjacent nerve root s w ould show substant ial variat ion, possibly due t o even m ore nerve root s cont ri but ing t he innervat ion. As an example, it was ment ioned t hat cut t ing t he 10t h and 11t h t horacic dorsal root s resulted in an irregular anaest het ic band. As compared t o t he varying segmentat ion of t he dorsal root s, t he segmentat ion of t he spinal cord it self was concluded t o be m uch more stable over subject s.
[7] Keegan and Garret t report ed in 1947 51 clinical cases w it h, w hat t hey considered a definit ive dermat ome area of hypalgesia for t he 4t h, 5t h, 6t h, 7t h and 8t h cervical nerve root s each, w here t he anam nesis indicat ed cervical disc herniat ion. They meant that unilateral herniation of a cervical disc resulted in affect ion of only one nerve root and t herefore sensory and mot or loss w ould be seen only in t he dist ribut ion of t hat nerve root . How ever, only 11 of t he 51 cervical cases w er e o p erat ed, and t her efo r e t h e remaining cases could not be considered t o be definitely confirmed.
[8] In 1956, Schwart z could explain t hat pain and sensory dist urbance caused by cervical root affect ion could deviate from t he derm at om al patterns. Thirteen human bodies w ere dissected and anast omot ic rami bet ween adjacent sensory root s w ere found in all obj ect s at dif ferent magnit ude. Approximate bilateral symmet ry of t he anast omoses was noted in only one of t he cases. The most frequent communicat ions w ere found t o be bet w een C6 and C7 root s. M ost anast om oses cam e from t he ganglion of t he nerve below, and joined t he fibres from t he segment one level above. Interest ingly, Schwart z also referred back t o st udies made already at t he beginning of t he 20t h cent ury by Kazzander and Weigner, w here sim i lar anast om oses at t he cervical level w ere observed.
St udies from t he later part of t he 20t h cent ury – including m onkey st udies and m ore recent dissect ion st udies
ISSN 2321-4287 regions supplied by one spinal nerve and t he myot ome did not necessarily coincide w it h t he dermat ome from t he same level.
[10] Perneczky and Sunder-Plassmann reported in 1980 t he examinat ions of 40 post-mort em specimens of t he cervical posterior root s under surgical microscope. Int radural communicat ing fibres bet w een neighbouring segment s w ere demonst rated. It was concluded t hat t he exact l ocal izat io n of n er v e r o o t co m p r essi o n i s ham pered by variat ions, and t hat t here are im plicat ions of t he frequent variant s for t he diagnosis of prolapsed cervical discs. “ In all of t he 40 specimens at least one int radural variant of t he cervical posterior root s was found t o be present . Tw o and morevariant s of sensory root s w ere demonst rable in 33 specim ens.” It was predominant ly t he posterior root s of C4 and C7 w hich w ere involved in t hese variant s.
[11] Ash et al. (1986) concluded t hat t hermo-graphic imaging of t he sensory dermat ome was not plausible, but dw elled no furt her upon t he sensory dermat omes more specifically.
[12] M arzo et al. (1987) dissected 54 human cer vi cal sp in es, and fo u nd co m m un i cant s bet w een t he dorsal root s in 53 of t he 54 spines. It w as suggest ed t hat t his m ight provide an overlap bet w een t he sensory dermat omes.
[13] Pop et al. (1988) investigated cortical evoked potent ials after dermat omal st imulat ion (SEP). Cervical recordings w ere made in 35 volunteers. Latency t ime bet w een peripheral st imulat ion and cort ical evoked response w ere measured. How ever, t hey did not discuss derm at om al dist ribut ion as such, but instead it was presumed t hat t his did not vary across t he subject s.
[ 14] Kasai et al . (1989) inv est i gat ed t h e cutaneous branches from t he cervical dorsal root s in 31 human cadavers, dissected on bot h sides expect for one case. In 60 out of 61 cases i t w as f o u nd t hat t h er e w as ab sen ce o f cut an eous branches f rom t he dorsal ram i, regarding t he low er cervical nerves. In 87% of t he cases t he cutaneous branches w ere absent in successive segment s. M ost frequent ly it was observed t hat t he dorsal rami from t he 6t h, 7t h and 8t h cer v i cal l ev el s f ai l ed t o d ev el o p cutaneous branches. They meant t hat only in 2% of all cases, dermat omal maps such as t hat
presented by Keegan and Garret in 1948, w ere relevant . In t he m ajorit y of t he cases, som e segments of the lower cervical dorsal rami lacked cutaneous branches.
[15] Polett i (1991) and [16] (1996) focused upon C2 and C3 dermat omes and t heir dist ribut ions. In t h e st ud y f r o m 1991, six p at i ent s microsurgically t reated w it h decompression of C2 or C3 nerve root s w ere included. The aut hors presented a descript ion of t heir findings of C2 and C3 dermat omes. Overlap was seen in t he suboccipital region in some cases. In t he st udy from 1996, Polett i et al described C3 nerve root compression, and meant t hat t his might lead t o radiat ing pain, dyeset hesia, numbness and C3 dermat ome sensory deficit, which resolved after facetect omy.
[17] van Kleef et al. (1993) st udied 20 pat ient s w it h cer v ical p ai n r adi at in g t o t he h ead / shoulder/ ar m for at least 1 year. Diagnost ic segmental nerve blocks under fluoroscopy w ere performed at all levels w hich w ere est imated t o be relevant eit her t hrough localisat ion of t he pain or findings on physical examinat ion. The level w it h t he best analget ic response w as chosen for RF rhizot omy. There was a reduct ion in pain score af t er t he procedure, but t he correlat ion bet w een affect ed nerve root and dermat omal pain distribution was not discussed.
M ost recent st u d i es i ncl u di n g n er ve-r oo t st imulat ion
not presented. It was said t hat all subject s had a cervical M RI performed before test ing, but t he correlat ions bet w een t he M RI findings and t he pain provocat ions by diagnost ic SNRB (select ive diagnostic nerve root blocks) w ere not presented furt her.
[19] Anderberg et al. (2004) invest igated t he effect s of SNRB, in 20 pat ient s w it h cervical radiculopat hy and single level M RI pat hological findings (soft discs and/ or spondylosis at t he same side as t he radicular pain). It was found t h at i n 14 o ut o f 20 pat i en t s, t h e cl in ical presentat ion “ did not fully reveal w hich nerve root w as ‘guilt y ’”, but t he analyses are not stat ist ically explored in more detail and the exact way of t he clinical examinations performed w ere not presented. They concluded from t he st udy t hat SNRB could be a useful t ool in ident ifying t he clinically significant root .
[20] A few years later, Anderberg et al (2006) present ed a prosp ect ive st udy i n order t o cor r elat e t r ansf o ram i nal SNRB t o cl i n ical sympt oms and M RI findings in 30 pat ient s w it h degenerat ive disease in t he cervical spine at tw o levels, and outcome depending on nerve block t reat m ent w it h steroid inject ions, surgery or conservat ive t reat ment . Degenerat ion on M RI findings was graded by t he reduct ion of t he area of the neuroforamen; the cause of reduction was not specified. It was described t hat t he pat ient s w ere exam ined by neurosurgeon aft er M RI, w hich seems t o imply t hat t he neurosurgeon already had a M RI answ er w hen m aking t he clinical exam inat ion. The primary finding w as t hat 18 pat ient s had effect of SNRB on a single level, and 11 had effect s of SNRB on t w o levels. Int erest ingly, it w as also foun d t h at SNRB correlated t o t he most degenerated level on M RI in 17 of 30 pat ient s, radicular pain dist ribut ion according t o t he classical dermat omes in 7 out of 30 pat ient s, and t o t he level decided by neurological deficit s (defined as “ mot or strengt h and/ or sensory deficit and/ or changes in tendon reflexes” ) in 8 out of 30 pat ient s. The possible/ li kely (?) bias w as not discussed. The level decided by neurological deficit s correlat ed t o M RI findings in 15 out of 30 pat ient s, and of t hese 15 only 6 correlated t o t he SNRB.
[21] Goldstein (2002) described in a review how dermat omes are not separated sharply, based
upon animal st udies, but also anat omical st udies and different st udies based upon neurological lesions. How ever, he meant t hat no definit ive st udy w it hin t he field w as at hand. He also referred t o previous st udies, w here int radural communicant s betw een adjacent cervical spinal root s have been shown (Freeman et al. 1935 and M arzo et al. 1987). Goldst ein concluded t hat frequent ly t he sympt oms of radiculopat hy did not cor respond t o t he expect ed anat om ical patterns, w hich is due t o t he common variations of nerve root s and spinal nerves, w hich were not least differing much bet w een individuals.
[22] M urphy et al. (2009) quest ioned w het her radicular pain necessarily follow ed a specific dermat om e. Pat ient s w ere chosen at a spine cent re, and considered t o fulfil t he criteria of radicular pain. They assessed 94 M R/ CT defined cervical nerve roots, affected by disk protrusions and/ o r lat eral canal st enosis or w it h EM G do cu m ent at io n of n er v e ro ot d ysf u nct i on t oget her w ith nerve root provocation test s. “ For a pain pattern t o be deemed dermat omal, t he p ain m ust be con t ain ed w i t hi n t h e ar ea designated in t he reference sources as arising from t he nerve root involved. If all or part of t he pain pattern fell out side t he area designated by bot h reference sources for t he involved nerve roo t , it w as d esignat ed no n-der m at om al.” Regarding specific nerve root levels, t he majorit y of affected root s follow ed a non-dermat om al pattern of radiculopat hy for t he levels C5, C6, C7. For t he C4 level, t he majorit y of t he affected r oo t s l ed t o a d er m at om al p at t er n o f radiculopat hy. This meant t hat in 69% of all 94 cases of cervical nerve-root associated pain, t he pain was non-dermat omal. It was suggested t hat overlap bet w een dermatomes could explain this finding, but anot her hypot hesis presented was t hat t here might be ot her sources of pain, such as intervertebral discs or t he dura mater.
ISSN 2321-4287 dist ribut ion of t he cervical derm at om es, and act ually was underlining t he general percept ion t hat specific peripheral sympt oms direct ly refer t o a specific cervical root .
[24] Ladak et al. (2013) described in a review t he know ledge of peripheral nerve overlap. In t he head and neck region, t he overlap was found from all major peripheral nerves, but t hey had t o be contained w it hin so called axial lines - i.e: “ lines form ed w here non-cont iguous spinal ner v es m eet , acro ss w h ich m ini m al t o no sensory overlap occurs”. That is, t he axial lines should be separated from dermat omal lines, and bet w een different axial lines no sensory overlap existed. In t he upper ext remit y, axial lines w ere present on t he anterior and posterior surfaces of t he ar m separat ing t he C5-C6 and T1-2 derm at om es, only t he proxim al part of t he armwas considered t o have axial lines, and t hus t here was no axial line separat ing for example C7 der m at om e f rom C6 d er m at om e or C8 dermat ome . The conclusion was t hat “ w it hin axial li n e t er r i t o r i es, i n ar eas o f sen so r y derm at om e over lap, t here of t en also exist physical com m un icat i ons bet w een ner v es derived from cont iguous spinal nerves”. Based upon t his, a map show ing t hese overlaps was suggest ed. It w as suggest ed t o be contained w it h i n an axi al l in e t h eo r y, bu t al so em b r yol ogical ly exp l ai nabl e: “ der m at om e dist ribut ion is affected by longit udinal growt h of t he lim bs as t he cut aneous sensory ner ves elongate t oward t heir target s”.
Fig. 1:Result of pub m ed search for cervical derm at om e.
Fig. 2: From Nieuw enhuys (1975), original draw ing by Bo lk, sho w i ng hi s p ict u res o f t he ar rangem ent s of derm at om es in t he upper ext remit y, as suggest ed by Bolk from his dissect ion st udies.
DISCUSSION AND CONCLUSION
The anat omy of cervical spinal nerves is w ell established. Know ledge of t he norm al supply and draining areas of t hese nerve root s, and t he pat hology associat ed w it h im pingem ent , is helpful w hen t rying t o diagnose radiculopat hy i n m any cases. Ho w ev er, f r eq u ent l y t h e sym pt om s and clinical obser vat ions do not correlat e w it h expected anat om ical pat terns. Commonly, variat ions of nerve root s and t heir connect ions w it h each ot her, lead t o anot her picture. Dermat ome maps used t oday are based upon st udies w it h different met hods, and many st udies also lack a detailed presentat ion of t he material and met hods used as a basis for t heir conclusions. As w it h so m any ot her part s of anat om y an d p hysi ol o gy, t h ere ar e in t er -individual variat ions t hat need t o be taken int o account during daily clinical decisions.
Th ou gh a vast am ou nt o f an at om ical and p hysi o lo gi cal resear ch has been d o n e o n pat ient s, cadavers and animals, t here seems t o be lack of know ledge of how often an affect ion of a specific root should give rise t o sympt oms w it hin it s specific dermat ome, and how often t his dermat ome fit s or does not fit int o classical anatomy.
possi ble, also use t he know ledge found by surgical intervent ions. M oreover, w e t hink t hat it is important t o keep in mind t hat t here, during t he years, has been increasing evidence of a vast variat ion bet w een individuals, indicat ing t hat pre-designed der m at om al m aps should be handled carefully.
Conflicts of Interests: None
ACKNOW LEDGEM ENTS
We are t hankful t o Anders Føhrby Overgaard for init ial cont ribut ion w it h concept ion of t he st udy.
REFERENCES
[ 13] .Po p PH, Oep kes CT, Not er m an s SL, Vl ek NM , St egem anDF.Derm at om al som at osensory evoked potent ials of t he lumbar and cervical root s. M ethod and norm al values. Eur Arch Psychiat r y Neurol Sci. 1988; 238(1):22-7.
[ 14] .Kasai T, Chi ba S, Suzuki T, Okuno Y. Cut aneous branches f rom t he dorsal ram i of t he cervical ner ves, w it h em phasis on t heir posit ional relat ions t o t he sem ispinalis cervicis. Okajim asFoliaAnat Jpn. 1989; 66(4):153-9.
[15]. Polett i CE. Third cervical nerve root and ganglion com pression: clinical syndrom e, surgical anat omy, and pat hological f indings. Neurosurger y. 1996; 39(5):941-8.
[16]. Polett i CE. C2 and C3 pain derm at om es in m an. Cephalalgia. 1991; 11(3):155-9.
[17]. VanKleef M , Spaans F, Dingem ans W, Barendse GA, Floor E, Sluijt er M E. Effect s and side effect s of a percutaneous t her m al lesion of t he dorsal root ganglion in pat ient s w it h cervical pain syndrom e. Pain. 1993; 52(1):49-53.
[18]. Slipm an CW, Plastaras CT, Palm it ier RA, Hust on CW, St e r e n f e l d EB. Sym p t o m p r o vo cat i o n o f f l u o r o sco p i cal l y gu i d ed ce r v i cal n e r ve r o o t st im ul at io n. A redynat o m al m ap s id en t i cal t o der m at om al m aps? Spine. 1998; 1523:2235–2242 [ 19]. Anderberg L, Annert z M , Brandt L, Saveland H. Select ive diagnost ic cer vical nerve root block – co r r el at i o n w i t h cl i ni cal sym pt o m s an d M RI-pat hology.Act aNeurochir (W ien) 2004; 146: 559– 565.
[ 20]. Ander berg L, Annert z M , Ryd holm U, Brandt L, Säveland H. Select ive diagnost ic nerve root block for the evaluat ion of radicular pain in t he m ult ilevel degenerat ed cer vical sp ine. Eur Spine J. 2006; 15:794-801.
[21]. Goldst ein B. Anat om ic issues relat ed t o cervical an d l u m b o sacr al r ad i cu l o p at h y. Phy s M ed RehabilClin N Am 13 2002; 423–437.
[22]. M urphy DR, Hurw it z EL, Ger rard JK, Clary R. Pain patt erns and descript ions in pat ient s w it h radicular pain: does t he pain necessari ly follow a specif ic der m at om e? Chiropr Ost eopat (2009) 17:1-9. [ 23]. Car idi JM , Pum berger M , Hughes AP. Cer vical
Radiculopat hy: A Review. HSSJ 2011; 7:265–272. [24]. Ladak A, Tubbs RS, Spinner RJ. M apping Sensory
Nerve Com m unicat ions Bet w een Peripheral Nerve Ter rit or ies (2013). Clinical Anat omy e-pub ahead of print .
[1] . Sheringt on CS. Experim ent s in exam inat ion of t he peripheral dist ribut ion of t he fibres of t he post erior root s of som e spinal ner ves. Phi l Trans Roy Soc London, series B 1893; 184: 641-763.
[2] . Head H and Cam pbell AW.The pat hology of her pes zost er and it s bearing on sensory localizat ion. Brain 1900; 23:353.
[ 3] . Ni e u w e n h u y s. Bo l k’s st u d i es o n se gm e n t al anat omy.ActaM orpholNeerl.-Cand. 1975; 13: 7-33. [4] . Kerr A. The brachial plexus of nerves in m an, t he var i at ions i n it s f or m at ion s and b ranches. The Am erican journal of anat om y 1918; 23(2) 285-395. [5] . Foerst er O. The derm at om es in m an. Brain 1933;
1(56): 1-36.
[6] . Freem an W. M ot or and sensor y overlap in t he spinal root s. AnnSurg 1935; 101:133–7.
[ 7] . Ke e gan JK. De r m at o m e hy p al gesi a w i t h p o st e r o l at e r al h e r n i at i o n o f l o w e r cer v i cal int ervert ebral disc. J Neurosurg 1947; 4(2):115-39. [8]. Schw art z HG. Anast om oses bet w een cervical nerve
root s.Neurosurger y 1956; 13:190-4.
[9] . Dykes RW and Terzis JK. Spinal nerve dist ri but ions i n t h e u p p e r l i m b : t h e o r gan i zat i o n o f t h e der m at om e and afferent myot om e. Philos Trans R SocLond B BiolSci 1981; 293(1070): 509-54. [10]. Perneczky A and Sunder-Plassm ann M . Int radural
variant of cervical nerve root fibres pot ent ial cause o f m i si nt er pr et i ng t h e segm en t al l o cat i o n o f cer vical disc prolapses from clinical evidence. Acta Neurochir 1980; 52(1-2): 79-83.
[ 11] .Ash CJ, Shealy CN, Young PA, Van Beaum ont W. Th e r m o gr ap hy an d t h e sen so r y d er m at o m e. Skeletal Radiol. 1986; 15(1):40-6.
[ 12 ] .M ar zo JM , Si m m o n s EH, Kal l e n F. I n t r ad u r al connect ions bet w een adjacent cervical spinal roots. Spine 1987; 12(10):964–68.