w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
Higher
body
mass
index
and
anti-drug
antibodies
predict
the
discontinuation
of
anti-TNF
agents
in
Korean
patients
with
axial
spondyloarthritis
Jiwon
Hwang
a,
Hye-Mi
Kim
b,
Hyemin
Jeong
c,
Jaejoon
Lee
c,
Joong
Kyong
Ahn
d,
Eun-Mi
Koh
c,
Eun-Suk
Kang
e,∗,
Hoon-Suk
Cha
c,∗aNationalPoliceHospital,DepartmentofInternalMedicine,Seoul,SouthKorea bSamsungBiomedicalResearchInstitute,Seoul,SouthKorea
cSungkyunkwanUniversitySchoolofMedicine,SamsungMedicalCenter,DepartmentofMedicine,Seoul,SouthKorea
dSungkyunkwanUniversitySchoolofMedicine,KangbukSamsungHospital,DepartmentofInternalMedicine,Seoul,SouthKorea eSungkyunkwanUniversitySchoolofMedicine,SamsungMedicalCenter,DepartmentofLaboratoryMedicineandGenetics,Seoul,
SouthKorea
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received10May2016 Accepted8October2016
Availableonline23December2016
Keywords:
Adalimumab Anti-drugantibody Axialspondyloarthritis Infliximab
Tumornecrosisinhibitors
a
b
s
t
r
a
c
t
Objective:Thedevelopmentofanti-drugantibodiesagainsttumornecrosisfactorinhibitors isalikelyexplanationforthefailureofTNF-inhibitorsinpatientswithspondyloarthritis.Our studydeterminedtheexistenceandclinicalimplicationsofADAbsinaxialspondyloarthritis patients.
Methods:AccordingtotheAssessmentofSpondyloArthritisInternationalSociety classifica-tioncriteriaforaxialspondyloarthritis,patientstreatedwithadalimumaborinfliximabwere recruitedconsecutively.Serumsampleswerecollectedatenrollmenttomeasureanti-drug antibodiesanddruglevels.
Results:Of100patients,themeandurationofcurrentTNFinhibitorusewas22.3±17.9 months.Anti-drugantibodiesweredetected in5of72 adalimumabusers comparedto 5 of28 infliximab users (6.9% vs. 17.9%).Anti-drug antibodies-positive patients hada significantlyhigherbodymassindexthananti-drugantibodies-negativepatientsamong bothadalimumab(28.4±5.9kg/m2vs.24.3±2.9kg/m2,respectively,p=0.01)andinfliximab users (25.9±2.8kg/m2 vs. 22.6±2.8kg/m2,respectively,p=0.02). Duringthe median 15-monthfollow-upperiod,drugdiscontinuationoccurredmorefrequentlyintheanti-drug antibodies-positive groupthantheanti-drugantibodies-negativegroup(30.0%vs.6.5%, respectively,p=0.04).Inlogisticregression,anti-drugantibodiespositivity(OR=5.85,95% CI1.19–28.61,p=0.029)andbodymassindex(OR=4.35,95%CI1.01–18.69,p=0.048)were associatedwithagreaterriskofstoppingTNFinhibitortreatment.
Conclusions: Ourresultsuggeststhatthepresence ofanti-drugantibodiesagainst adali-mumabandinfliximabaswellasahigherbodymassindexcanpredictsubsequentdrug discontinuationinaxialspondyloarthritispatients.
©2016PublishedbyElsevierEditoraLtda.ThisisanopenaccessarticleundertheCC BY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/4.0/).
∗ Correspondingauthors.
E-mails:[email protected](E.Kang),[email protected](H.Cha).
http://dx.doi.org/10.1016/j.rbre.2016.11.009
O
maior
índice
de
massa
corporal
e
a
presenc¸a
de
anticorpos
antifármacos
predizem
a
interrupc¸ão
no
uso
de
agentes
anti-TNF
em
pacientes
sul-coreanos
com
espondiloartrite
axial
Palavras-chave:
Adalimumabe
Anticorposantifármacos Espondiloartriteaxial Infliximabe
Inibidoresdanecrosetumoral
r
e
s
u
m
o
Objetivo: Odesenvolvimentodeanticorposantifármacos(ADAb)contraofatordenecrose tumoral(TNF)éumaexplicac¸ãoprovável paraa falhadosanti-TNFem pacientescom espondiloartrites(EspA).Opresenteestudodeterminouapresenc¸aeasimplicac¸õesclínicas dosADAbempacientescomEspAaxiais.
Métodos: Deacordo comos critériosde classificac¸ãoparaEspA axialda Assessmentof SpondyloArthritisInternationalSociety,recrutaram-seconsecutivamentepacientestratados comadalimumabeouinfliximabe.Coletaram-seamostrasdesoronomomentodaentrada noestudoparamedirosníveisdeADAbedefármaco.
Resultados: Dos100pacientes,adurac¸ãomédiadeusodosanti-TNFatuaisfoide22,3±17,9 meses.OsADAbforamdetectadosemcincode72pacientesemusodeadalimumabe,em comparac¸ãocomcincode28usuáriosdeinfliximabe(6,9%vs.17,9%).Ospacientes ADAb-positivostinhamumíndicedemassacorporalmaiordoqueaquelesADAb-negativos,tanto entreindivíduosemusodeadalimumabe(28,4±5,9kg/m2vs.24,3±2,9kg/m2, respectiva-mente,p=0,01)quantodeinfliximabe(25,9±2,8kg/m2vs.22,6±2,8kg/m2respectivamente, p=0,02).Duranteoperíodomédiodeseguimentode15meses,asuspensãodofármaco ocor-reucommaiorfrequêncianogrupoADAb-positivodoquenogrupoADAb-negativo(30,0%
vs.6,5%,respectivamente,p=0,04).Naregressãologística,apositividadenoADAb(OR=5,85, IC95%1,19a28,61,p=0,029)eoIMC(OR=4,35,IC95%1,01a18,69,p=0,048)esteveassociada aummaiorriscodeinterromperotratamentocomanti-TNF.
Conclusões: Osresultadosdopresenteestudosugeremqueapresenc¸adeADAbcontrao adalimumabeeoinfliximabe,bemcomoumIMCmaisalto,podepredizerasubsequente interrupc¸ãodofármacoempacientescomEspAaxial.
©2016PublicadoporElsevierEditoraLtda.Este ´eumartigoOpenAccesssobuma licenc¸aCCBY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
The advent of tumor necrosis factor (TNF) inhibitors rep-resented a breakthrough in the management of chronic inflammatory diseases such as rheumatoid arthritis (RA), spondyloarthritis (SpA), psoriasis, and inflammatory bowel disease(IBD).Notonlyankylosingspondylitis(AS),but also thenon-radiographicformofaxialSpAhavebenefittedfrom thesedrugswithresponseratesof60–70%.1–3 Regardless,a considerableproportionofSpApatientsfailtorespondab ini-tio(primaryfailure),ortheinhibitorslosetheirefficacyover timedespiteaninitialgoodresponse(secondaryfailure).4,5 Somepatients mayalso needtodiscontinue TNFinhibitor treatmentduetosignificantadverseevents.6
Recently,immunogenicityhas beenimplicated asa pri-marycauseofresponsefailure,becauseallbiologics,including TNF inhibitors, have immunogenic potential. The devel-opment of anti-drug antibodies (ADAbs) leads to low or undetectabledruglevels,resultinginthefailureorlossof effi-cacyofthedrugandadverseevents;thisphenomenonhas beenwelldocumentedinpatientswithRAandCrohn’sdisease (CD).7,8 To date, ADAbs have been detected against inflix-imab(IFX),adalimumab(ADL),andgolimumab(GLM)inSpA patientsandthereareseveralreportsabouttheassociations oftheseADAbswithclinicalresponse.9InadditiontoADAbs, thereare other factors thataffect the pharmacokineticsof
TNFinhibitors,suchasconcomitantuseofdisease-modifying antirheumaticdrugs(DMARDs),especiallymethotrexate,the degree of systemic inflammation (e.g., serum albumin, C-reactiveprotein,andTNFburden),bodyweight,andgender.10 Historically,inthemeantime,ADAbsagainstIFXweremore oftenobservedinRApatientscomparedtoASpatients.Itwas thoughttobehigherdosesofIFXusedinaxialSpApatients.11 Established combination therapy with biologic agent and immunomodulators hasalsobeen describedtopreventthe developmentofADAbsinpatientswithRAandCDaswell.12,13 WithrespecttoDMARDs,thereisnosolidevidencetosupport theiruseinaxialSpA.
PreviousstudiesofADAbs inSpA patientshavefocused mostlyontheincidenceofADAbsandtheireffectsinwestern populations. Weundertookthepresentstudytoinvestigate whetherADAbsexistinKoreanpatientswithaxialSpAand theclinicalsignificanceofthis.Additionally,weinvestigated whether factorssuchasbodyweightandsmoking affected ADAblevelsinKoreanSpApatients.
Methods
Studydesignandpatients
SpApatientswererecruitedconsecutivelyfromasingle ter-tiaryhospital.BothADAbanddruglevelsweremeasuredin 89ASpatients, nine SpA-associated-with-IBDpatients, one psoriatic SpA patient, and one undifferentiated axial SpA case.AllpatientsfulfilledtheAssessmentof SpondyloArthri-tisInternationalSociety(ASAS)classificationcriteriaforaxial SpA.14ASpatientsalsosatisfiedthe1984modifiedNewYork Criteria.15Atenrollment,theyweretreatedwitheitherADL orIFXafterfailingtorespondtoatleasttwonon-steroid anti-inflammatorydrugs(NSAIDs)orotherkindsofTNFinhibitors. ADLwasadministeredsubcutaneouslyat40mgbiweekly.IFX wasgivenintravenouslyat5mg/kgatweeks0,2,6,andevery8 weeksthereafter.Dosingintervalsforeachdrugwereadjusted accordingtodiseaseactivityandthetreatingphysician’s deci-sion. Disease activity was scored by the Bath Ankylosing SpondylitisDiseaseActivityIndex (BASDAI),and the differ-ence in score between baseline and the time of sampling orlastobservationwascalculated.Datawere reviewed ret-rospectively via medical records or obtained prospectively toassess the followingvariables: demographics,laboratory findingsincludingerythrocytesedimentationrate(ESR)and C-reactiveprotein(CRP)level,BASDAIscore,concomitantuse ofNSAIDsorDMARDs,presenceofinfections,includinglatent or reactivated tuberculosisinfection, side-effects including infusionreactionorinjectedsitereaction,andthecausefor switchingordiscontinuationofTNFinhibitors.Smoking sta-tuswas notavailableinall participantsand theaccessible numbers were shown in brackets for each item in tables. Latenttuberculosisinfection wasdiagnosedbyexperienced pulmonologists based on a positive QuantiFERON-TB Gold In-tubetestresult(CellestisLimited,Carnegie,Victoria, Aus-tralia)andchestradiographfindings.Bodymassindex(BMI) atenrollmentwascalculatedandpatientsweredividedinto threeclassesaccordingtoBMIbasedonthe National Insti-tute ofHealth classification16: BMI<25kg/m2, normal; BMI 25–30kg/m2,overweight;BMI>30kg/m2,obese.Patientswith afollow-upperiodof6monthsorgreateraftersamplingwere includedinpost-samplingstatisticalanalyses.Studyprotocol wasapprovedbytheinstitutionalreviewboardofSamsung Medical Center and all participants gave written informed consent.
MeasurementofdrugandADAbconcentrations
Bloodsampleswerecollectedatthetimeofenrollmentbefore thenext ADLinjectionorIFX infusion.Trough serumlevel ofdrugs(ADL orIFX) andthe amount ofADAbs(anti-ADA or anti-IFX)were measured by enzyme-linked immunosor-bentassay(TNF␣-Blocker-MonitoringandTNF␣-BlockerADA, Immundiagnostik AG, Bensheim, Germany). Weperformed ELISAaccordingtothemanufacturer’sinstructions.To deter-mine the quantity of free therapeutic TNF inhibitors, six calibrators were used to generate a standard curve, and positiveand negative controlswere included on all plates. The lower limit of detection was 0.4g/mL. The presence orabsenceofADAbwas determinedusingthe cut-off con-trol included in the kit, which had a concentration of 10AU/mL.
Statisticalanalysis
Statistical analyses were performed using the Statistical PackagefortheSocialSciences,version18.0(SPSS,Chicago, IL, USA).Descriptive dataare reported asmeans, standard deviations(SD),orpercentages.Differencesbetweengroups were testedwithStudent’st-test,Pearson’schi-square test, ortheMann–WhitneyUtestasappropriate.Oddsratios(OR) were calculated bylogistic regression to determine factors predictiveofdrugdiscontinuation.Lastobservationalcarried forward(LOCF)analysiswasperformedduringthefollow-up. Whenpatientswerecategorizedintofourgroupsaccordingto theirdruglevelsandpresenceofADAbs,thecut-offof ade-quatedruglevelswassetto5g/mLforADLand0.8g/mL for IFX based on the suggested levels of adequacy in IBD patients.17,18Thresholdforsignificancewassettop<0.05.
Results
Patientcharacteristics
Mean age of the patients was 34.8±10.1 years and mean disease duration from symptomonsetwas 11.1±7.8years. DemographicdataandbaselinecharacteristicsofADLusers andIFXusersarecomparedinTable1.ADLwasprescribed mostlyinpatientswithAS(95.8%),whileIFXwasprescribed to 25% of patients with SpA-associated IBD. Concomitant DMARDusewasmorefrequentwithIFXthanADL(p=0.015). History of ever-smoking was more frequently observed in ADLusers thannon-ADL users(p=0.02,n=75).Other clini-calcharacteristicswerecomparablebetweenADLusersand IFXusers.Eighty-twopatientswerefirst-timeusersof TNF-inhibitors (anti-TNF naïve).Among 18switchers previously treated with other kinds ofTNF-inhibitors, the most com-monly used agent was ETN (n=12), followed byIFX (n=3) andADL(n=1).Othertwoswitchershadbeenprescribedtwo agentspreviously.Secondaryfailurewasthemajorreasonfor switching(83.3%).Comparedwithswitchers,first-timeusers had dosing intervals significantly extended relative to the schedulingsuggestedbythemanufacturer(1.27timesvs.1.64 times;equivalentto2.54weeksvs.3.28weeks,respectively,
p=0.02).
Anti-drugantibodiesagainstcurrentTNF-inhibitors
At the time of sampling, mean duration of use of cur-rent TNFinhibitors was22.3±17.9 months.Five of74ADL users (6.9%) had detectable ADAbs, while five of 28 IFX users (17.9%) had detectable ADAbs; this difference was not statistically significant (p=0.13). Immunogenicity and clinical variables are shown in Tables 2 and 3. Baseline ESR, CRP level, and BASDAI were significantly different between ADAb-negative and ADAb-positive groups, as was the improvement in BASDAI from baseline in ADL and IFX users. Mean BMI of patients with ADAbs was signifi-cantly higher than that ofADAb-negative patients; among ADLusers,28.4±5.9kg/m2 vs.24.3±2.9kg/m2, respectively,
Table1–Patientdemographicsandbaselineclinicalcharacteristics(N=100).
Variables Adalimumab(n=72) Infliximab(n=28) p-Value
Ageatsampling,yrs(mean±SD) 34.9±9.6 34.8±11.7 0.97
Male(%) 91.7 23(82.1) 0.28
BMI,kg/m2(mean±SD) 24.5±3.33 23.2±3.10 0.07
Normal(%) 63.9 67.9
Overweight(%) 30.6 32.1
Obese(%) 5.6 0
Eversmokera(%) 68.5(n=54) 38.1(n=21) 0.02
Diseaseduration,yrs(mean ± SD) 11.8 ± 7.7 9.5 ± 8.0 0.17
HLA-B27positive(%) 87.5(n=56) 84.2(n=19) 0.71
Historyofperipheralarthritis(%) 70.8 22(78.6) 0.43
Historyofenthesitis(%) 29.2 6(21.4) 0.43
Historyofuveitis(%) 29.2 5(17.9) 0.25
RadiographicSIjointinvolvement(%) 88.9 27(96.4) 0.44
DiagnosisofaxialSpA 0.001
AS(%) 95.8 71.4
SpA-associatedIBD(%) 2.8 25.0
PsoriaticSpA(%) 1.4 0
UndifferentiatedaxialSpA(%) 0 3.6
ConcomitantDMARDsb 0.015
Sulfasalazine(%) 1.4 10.7
Methotrexate(%) 2.8 3.6
Otherimmunosuppressant(%) 0 10.7
ConcomitantNSAIDsc(%) 52.8 42.9 0.37
BaselineESR,dmm/h(mean± SD) 42.8 ± 32.6 54.4± 38.3 0.14
BaselineCRP,dmg/dL(mean± SD) 2.17 ± 2.30 3.08± 3.20 0.13
BaselineBASDAId(mean± SD) 9.34 ± 1.36 8.92± 2.11 0.25
SwitcherfromotherkindsofTNF-inhibitors(%) 20.8 10.7 0.24
LTBIpositive(%) 23.6 17.9 0.53
BMI,bodymassindex;SI,sacroiliac;SpA,spondyloarthritis;AS,ankylosingspondylitis;IBD,inflammatoryboweldisease;DMARDs, disease-modifyingantirheumaticdrugs;NSAIDs,non-steroidanti-inflammatorydrugs;ESR,erythrocytesedimentationrate;CRP,C-reactiveprotein; BASDAI,BathAnkylosingSpondylitisDiseaseActivityIndex;LTBI,latenttuberculosisinfection.
a Ever-smokerpercentagewascalculatedonthebasisofthenumberinbrackets,ofwhichpatientswereavailableforsmokingstatus.
b ConcomitantDMARDsmeanttheuseatinitiationofcurrentTNF-inhibitorsforatleast3months.
c ConcomitantNSAIDswereusedondemand,notonaregularbasis. dValuesarebaselinevaluesofcurrentTNFinhibitors.
Table2–Adalimumabimmunogenicityandclinicalvariablesatthetimeofsampling(N=72).
Variables ADAb(−)(n=67) ADAb(+)(n=5) p-Value
Male(%) 61(91.0) 5(100) 1.00
Diseaseduration,yrs(mean±SD) 12.0±7.7 10.2±8.0 0.62
BaselineESR,mm/h(mean±SD) 41.5±30.5 60.0±55.0 0.21
BaselineCRP,mg/dL(mean±SD) 2.07±2.18 3.40±3.72 0.22
BaselineBASDAI(mean±SD) 9.29±1.40 9.96±0.06 0.29
BASDAIa(mean± SD) 7.26± 2.24 7.12± 3.96 0.89
BMI,kg/m2(mean± SD) 24.3± 2.9 28.4± 5.9 0.01
Eversmokerb(%) 68.0(n=50) 75.0(n=4) 1.00
Serumalbumin,g/dL(mean ± SD) 4.50± 0.33 4.38± 0.27 0.45
ConcomitantDMARDs(%) 10.5 20.0 0.45
SwitcherfromotherkindsofTNF-inhibitors(%) 22.4 0 0.57
DurationofcurrentTNFinhibitoruse,months(mean± SD) 23.6± 19.1 16.4± 12.0 0.26
Dosingintervalc(mean ± SD) 0.19
n× times 1.7 ± 0.9 3.1 ± 2.0
Correspondingperiod(weeks) 3.4 ± 1.8 6.2 ± 4.0
Druglevel,g/mL(mean± SD) 5.64± 4.12 0.45± 0.68 <0.001
ADAb,anti-drugantibodies;BASDAI,BathAnkylosingSpondylitisDiseaseActivityIndex;BMI,bodymassindex;DMARDs,disease-modifying antirheumaticdrugs.
Cut-offforADAbpositivitywas10AU/mL.
a DifferenceinBASDAIbetweenbaselineandtimeofsampling.
b Ever-smokerpercentagewascalculatedonthebasisofthenumberinbrackets,ofwhichpatientswereavailableforsmokingstatus.
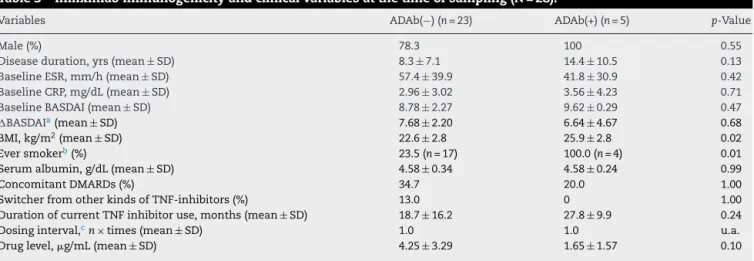
Table3–Infliximabimmunogenicityandclinicalvariablesatthetimeofsampling(N=28).
Variables ADAb(−)(n=23) ADAb(+)(n=5) p-Value
Male(%) 78.3 100 0.55
Diseaseduration,yrs(mean±SD) 8.3±7.1 14.4±10.5 0.13
BaselineESR,mm/h(mean±SD) 57.4±39.9 41.8±30.9 0.42
BaselineCRP,mg/dL(mean±SD) 2.96±3.02 3.56±4.23 0.71
BaselineBASDAI(mean±SD) 8.78±2.27 9.62±0.29 0.47
BASDAIa(mean± SD) 7.68 ± 2.20 6.64± 4.67 0.68
BMI,kg/m2(mean± SD) 22.6 ± 2.8 25.9± 2.8 0.02
Eversmokerb(%) 23.5(n=17) 100.0(n=4) 0.01
Serumalbumin,g/dL(mean ± SD) 4.58 ± 0.34 4.58± 0.24 0.99
ConcomitantDMARDs(%) 34.7 20.0 1.00
SwitcherfromotherkindsofTNF-inhibitors(%) 13.0 0 1.00
DurationofcurrentTNFinhibitoruse,months(mean± SD) 18.7 ± 16.2 27.8± 9.9 0.24
Dosinginterval,cn× times(mean± SD) 1.0 1.0 u.a.
Druglevel,g/mL(mean ± SD) 4.25 ± 3.29 1.65± 1.57 0.10
ADAb,anti-drugantibodies;BASDAI,BathAnkylosingSpondylitisDiseaseActivityIndex;BMI,bodymassindex;DMARDs,disease-modifying antirheumaticdrugs;u.a.,unavailable.
Cut-offforADAbpositivitywas10AU/mL.
a DifferenceinBASDAIbetweenbaselineandtimeofsampling.
b Ever-smokerpercentagewascalculatedonthebasisofthenumberinbrackets,ofwhichpatientswereavailableforsmokingstatus.
c Concomitant.
respectively, p=0.02. Among IFX users, current and ex-smokers were overrepresented in the ADAb-positive group relative to the ADAb-negative group (100.0% vs. 23.5%, respectively, p=0.01), whereas there was no difference in theproportionsofcurrent andex-smokers between ADAb-positive and ADAb-negative ADL users (75.0% vs. 68.0%, respectively,p=1.00).NoswitchershadADAbsagainsttheir current TNF-inhibitors. In ADL users, the dosing inter-vals tended to be prolonged in the ADAb-positive group (3.1±2.0 times vs. 1.7±0.9 times; equivalent to 6.2±4.0 weeks vs. 3.4±1.8 weeks, p=0.19), whereas it was not adjusted in IFX users. Druglevel of ADLwas significantly lowerinADAb-positivepatientsthanADAb-negativepatients (0.45±0.68g/mLvs.5.64±4.12g/mL,respectively,p<0.001). InIFXusers,theADAb-positivegrouptendedtohavealower drug level than the ADAb-negativegroup but without sta-tistical significance (1.65±1.57g/mL vs. 4.25±3.29g/mL, respectively,p=0.10).Concomitant useofDMARDswasnot differentbetweenADAb-negativeandADAb-positiveADLor IFXusers.BMI≥25kg/m2wastheonlyriskfactorassociated withADAbpresence[OR=9.33(95%confidenceinterval (CI) 1.85–46.86),p=0.007];inversely,normalweightprotectedfrom thepresenceofADAbs[OR=0.10(95%CI0.02–0.52),p=0.006]. NoothervariablesshowedacorrelationwithADAbpositivity, includingconcomitantDMARDs.
Associationsamongdiscontinuationoftreatment,adverse events,andADAbstatus
Follow-updatafor98patientswhohadbeenobservedforat least6monthsormore(71ADLpatientsand27IFXpatients) wereanalyzed.Onepatientwaslosttofollow-upat1month (oneIFXuser)andanotherat4months(oneADLuser)and were therefore excluded from the post-sampling analysis. TwofemalepatientsstoppedtakingTNFinhibitorsbecause ofpregnancy(oneIFXuserat7monthsandoneADLuserat
14monthsand)andtheirmissingvalueswerereplacedbythe LOCFmethod.
Medianfollow-upduration wassimilarbetweenthetwo groups (15.0 months in the ADAb-negative group vs. 13.5 monthsin the ADAb-positivegroup, p=0.15).Regardless of the typeofcurrent TNF inhibitor,discontinuationof treat-ment occurredmorefrequentlyintheADAb-positivegroup than the ADAb-negativegroup (30.0%vs. 6.5%respectively,
p=0.04).OfthepatientswhodiscontinuedADLduring follow-up,druglevelswassignificantlyloweratthetimeofsampling comparedtobaselinethanthatofpatientswhomaintained ADLduringfollow-up(2.18±1.49g/mLvs.5.55±4.26g/mL, respectively,p=0.04).ForIFXusers,therewasnosignificant difference indrug level atbaselineand follow-up between those patientswho discontinuedtreatmentand thosewho didnot(1.79±2.06g/mLvs. 3.95±3.22g/mL,respectively,
p=0.21).ReasonsfordiscontinuingTNFinhibitorusebetween groupsweresovariablethatstatisticalanalysiswasnot pos-sible.Therewereseveraladverseeventsduringfollow-up,but noneoftheserequireddiscontinuationoftreatment(Table4). IrrespectiveofthetypeofTNFinhibitor,patientscouldbe dividedintofourcategoriesbasedondruglevelandthe pres-enceofADAbs:53(54.1%)patientshadanadequatedruglevel andnoADAbs(group1);35(35.7%)patientshadalowdrug levelandnoADAbs(group2);three(3.1%)patientshadan ade-quatedruglevelanddetectableADAbs(group3);seven(7.1%) patientshadanundetectabledruglevelandwereADAb pos-itive(group4).Inthe71ADLpatientswhowerefollowed-up, fourpatientsingroup2andonepatientingroup4 discontin-uedtakingdrugs,whileamongthe27IFXpatientswhowere followed-up,twopatientsingroup1andtwopatientsingroup 4discontinueddruguse.
Table4–Clinicalresponseduringthefollow-upperiodofpatientswithADAbsandthosewithoutADAbs(N=98).
ADAb(−)(n=88) ADAb(+)(n=10) p-Value
Follow-upduration,monthsmedian(range) 15.0(6–17) 13.5(6–17) 0.15a
DiscontinuationofcurrentTNF-inhibitors(%) 6.8 30.0 0.04
Adverseevents
AbnormalLFT(%) 1.1 0 1.00
Injection/infusionsitereaction(%) 3.4 10.0 0.35
New-onsetpsoriasisordermatitis(%) 10.2 0 0.59
TBreactivation(%) 0 0 u.a.
Tableshowstheresultsof98patientswhosedatawereavailableduringfollow-up. ADAbs,anti-drugantibodies;LFT,liverfunctiontests;TB,tuberculosis;u.a.,unavailable. a Mann–Whitney.
significantvariablesfromunivariateanalysis.ADAbpositivity hadnoimpactonadverseevents.
Discussion
Ourgoalsinthis studywere assessthe presenceofADAbs againstADLandIFXinKoreanaxialSpApatients,todetermine theclinicalimportanceofthis,andtoinvestigatefactors asso-ciatedwiththedevelopmentofADAbs.WedetectedADAbs inpatientsreceivingeitherADLorIFXtreatment,andthese ADAb-positivepatientswereatriskofsubsequentdrug dis-continuation.AhigherBMIwasalsorelatedtoahigherriskof ADAbpositivity,andpredictedsubsequentdrug discontinua-tion.
DetectableADAbs toADL and IFXhave previouslybeen reportedtodecreasetreatmentresponse.19TheseADAbsmay reducedrug levels in severalways. First, ADAbs may neu-tralizetherapeuticdrugsbyblockingbindingsitesforTNFs. Another possibilityisthat ADAbsmay formimmune com-plexeswiththerapeuticdrugs, enhancingdrug clearance.10 IFXasachimericmonoclonalantibodyisconsideredtohave moreimmunogenicpotentialthanADL,andADAbsagainst IFX were investigated as human anti-chimeric antibodies (HACAs).HACAsreduceorshortenIFXefficacyinpatientswith RAandCD.7,8Recently,theepitopeofIFXimmunogenictothe paratopeofHACAwaslocalizedtoF(ab′)
2.20Incontrast,ADL isahumanizedmonoclonalantibodythatwasengineeredto havegoodinvivo tolerabilityandweakened immunogenic-ity.Unfortunately,however,ADAbshavealsobeenfoundin ADL-treatedpatients,andtheseADAbshavebeenshownto hampertheclinicalresponsetoADL,aswasobservedin IFX-treatedpatients.21 ImmuneresponseagainstADLhasbeen suggestedto be highly restricted tothe idiotype, resulting inanti-idiotypicantibodiesthatfunctionallyneutralizeADL, despitetheexistenceofsmallimmunecomplexes.10 Inour study,amongninepatientswho discontinueddrugsduring follow-up,sevenhadlowdruglevels,includingfourpatients withoutdetectableADAbs.Theothertwopatientsbelonged to group 1 ofIFX, indicating adequate drug levels and no ADAbsatsampling.Ofthesetwopatients,onehadaslightly lowerdruglevel(2.49g/mL)thanthemeaninADAbnegative patients(4.25g/mL),butthislevelwassomewhathigherthan themeanofADAb-positivepatients(1.65g/mL).Thesecond
patienthadsufficientdruglevels(4.40g/mL)butdeveloped pleural effusion resembling serositis at the 13 month of follow-up.Thispatientreceivedathoroughwork-upfor etiol-ogy,includingthoracentesis,andbasedonthis,weconcluded thatpleuraleffusionwasalupus-likemanifestationbasedon the high titerof positiveanti-nuclear antibodies and anti-double strand DNA antibodies. Autoimmune-like diseases such as psoriasis and systemic lupus erythematosus (SLE) aredocumentedadverseeventsofTNF-inhibitors,andADAbs may underlie these adverse events. Despite undetectable ADAbsatcertaintimepoints,long-lastingsmallimmune com-plexesmayinducetypeIIIhypersensitivityreactionssuchas serumsicknessandSLE.10
yielddifferentialimmunitytoinfectiousdiseases.23For exam-ple,individualswiththeG1m3phenotypewereshowntohave ADLADAbslessoftenthanthosewiththeG1m1,17-allotype.24 ThetypesofimmunoglobulinGMandKMallotypespresentin theKoreanpopulationcouldhaveaffectedourresults,butthis wasbeyondthescopeofourstudy.
Among100axialSpApatients,concomitantDMARDswere used in only 10 patients. Because our practice complies withtherecommendationsforthemanagementofaxial dis-ease,mostpatientsweretreatedwithTNFinhibitorsand/or NSAIDsunlesstheyhadotherrequirements.25DMARDswere more often prescribed together with IFX than ADL. This is likely because more patients with SpA-associated IBD weretreatedwithIFXthanADLandthesepatientsrequired mesalazine,sulfasalazine,orazathioprine.Duringthe post-samplingperiod,concomitantDMARDswerestoppedinhalf ofthepatientswhiletheyweremaintainedintheother50%of patientsbecauseofIBDandperipheralarthritis.Nevertheless, logisticregressionrevealedthattheuseofDMARDswasnot associatedwithADAbpositivity,althoughlargersamplesizes arerequiredtotestthis hypothesisinarigorousstatistical manner.
UnlikeIFXuserswhohadfixed,regulardosingintervals, ADLusershadvariabledosingintervals.Comparedtopatients without ADAbstoADL, ADAb-positivepatients had signifi-cantlyprolongeddosingintervals.ScheduledIFXtreatment strategiesare knowntobeless immunogenicthan variable IFXtreatmentstrategies,26butthishasnotbeeninvestigated forADL.Itisalsonotclearwhetherascheduledregimenhelps diminishimmunogenicityorwhetherlabiledosingintervals aredirectlyrelatedtoeventualtreatmentfailure.
Intriguingly, ADAb-positive patients were significantly overweightorobesecomparedtoADAb-negativepatientsin both ADLand IFX groups. BMIwas the only variable that increasedtheriskofADAbdevelopmentorprotectedagainstit inlogisticregressionanalysis.Obesityisastrongdeterminant ofinflammationinthegeneralpopulation.27Inrecent stud-ies,BMIhasbeenshowntostronglyinfluencetheresponseto TNFinhibitorsinRAandSpApatients;ahigherBMIis asso-ciatedwithadecreasedchanceofachievingremission.28,29In particular,responsetoIFXwas reducedtoagreater extent than that to ADL or ETN in obese axial SpA patients, but thereasonforthishasnotbeenelucidated.29Adiposetissue canmodulatetheinflammatoryresponsebyproducing sev-eralinflammatorycytokines,includingTNF-␣,andexpressing Fcreceptors.30DecreasedefficacyofTNFinhibitorsinobese patientscouldbecausedbyinteractionsbetweenFcreceptors expressedonadipocytesandtheFcportionofdrugsas lig-ands.WhileTNFinhibitorscouldpotentiallyinteractwithFc receptorsonadipocytes,variableregionsofthe drugs,such as the Fab′ or F(ab′)
2 fragments, may be exposed, thereby servinganimmunogenicfunction.Inourstudy,BMIwasnot significantlyrelatedtoADAbpositivitywhen patientswere stratifiedbasedonthetypeofTNFinhibitortheyused.This maybeduetothesmallnumbersofpatientsevaluatedinthis study;theseresultsneedtobeconfirmedinalargercohortof patients.
Another notable finding was that among ADL users, a history of smoking was more frequent in ADAb-positive
patients than ADAb-negative patients. This indicates that smoking may be a risk factor for ADAb development in patientstreatedwithTNFinhibitors.Smokinghasalsobeen shown to beassociatedwith RApathogenesisand disease activity.31 Recent studies showedthat smoking was a neg-ative prognosticfactor for responseto bothMTX and TNF inhibitors inRA.32,33 A possible mechanism linking smok-ing to a poor TNF inhibitor response may be significantly higherserumsolubleIL-2receptor(sIL-2R)levelsinsmokers.34 Meanwhile,humanleptinhasbeenreportedtoenhance pro-liferation and activation of circulating T lymphocytes in a dose-dependentmannerbystimulatingthesynthesisofIL-2. Inlightofthis,increasedleptinlevelsinobesepatientscould activatecirculatingTcellsvia IL-2,resultinginadecreased responsetoTNFinhibitors.35Smokingandobesitymighthave a synergistic effect on a poor response to TNF inhibitors; however, the underlying mechanisms still have to be determined.
Thisstudyhadseverallimitations.First,thesamplesize wassmallandmissingdatawerepresent.Second,ADAband druglevelswereassayedonlyonceinacross-sectional man-ner,notinaserialmanner,preventingmorecomprehensive deductions aboutthe relationshipbetweendrugresponses, sideeffects,andADAbstatus.Therearestillargumentsabout the utilityofADAband druglevel measurementinclinical practice fordecision-making purposes.Lastly, it requires a more cautious approach to generalizing our data to other populationsorracesduetothegeneticdifferences. Neverthe-less,weconcludedthatthedevelopmentofADAbstoADLand IFXcouldbeassociatedwithareductioninserumlevelsof ADLandIFX,leadingtosubsequentdiscontinuationof treat-ment,andthatoverweightandobesepatientsmaybemore pronethantheircounterpartstodevelopimmunogenicityto TNFinhibitors.Thesedataneedtobeconfirmedinalarger cohortofaxialSpApatientsinalong-termprospectivestudy. Theunderlyingmechanismsbywhichobesityandsmoking contributetotheimmunogenicityofTNFinhibitorsinaxial SpApatientsalsorequireelucidation.
Funding
This work was supported by a grant of the Korea Health Technology R&D Projectthrough theKoreaHealth Indus-try Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (grant number: HI14C2285).
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
placebo-controlledtrial(ASSERT).ArthritisRheum. 2005;52:582–91.
2. vanderHeijdeD,KivitzA,SchiffMH,SieperJ,DijkmansBA, BraunJ,etal.Efficacyandsafetyofadalimumabinpatients withankylosingspondylitis:resultsofamulticenter, randomized,double-blind,placebo-controlledtrial.Arthritis Rheum.2006;54:2136–46.
3. SieperJ,vanderHeijdeD,DougadosM,MeasePJ, MaksymowychWP,BrownMA,etal.Efficacyandsafetyof adalimumabinpatientswithnon-radiographicaxial spondyloarthritis:resultsofarandomisedplacebo-controlled trial(ABILITY-1).AnnRheumDis.2013;72:815–22.
4. deVriesMK,WolbinkGJ,StapelSO,deGrootER,DijkmansBA, AardenLA,etal.Inefficacyofinfliximabinankylosing spondylitisiscorrelatedwithantibodyformation.Ann RheumDis.2007;66:133–4.
5. deVriesMK,BrouwerE,vanderHorst-BruinsmaIE, SpoorenbergA,vanDenderenJC,JamnitskiA,etal. Decreasedclinicalresponsetoadalimumabinankylosing spondylitisisassociatedwithantibodyformation.Ann RheumDis.2009;68:1787–8.
6. MatsumotoY,MaedaT,TsuboiR,OkuboY.Anti-adalimumab andanti-infliximabantibodiesdevelopedinpsoriasisvulgaris patientsreducedtheefficacyofbiologics:reportoftwocases. JDermatol.2013;40:389–92.
7. BaertF,NomanM,VermeireS,VanAsscheG,D’HaensG, CarbonezA,etal.Influenceofimmunogenicityonthe long-termefficacyofinfliximabinCrohn’sdisease.NEnglJ Med.2003;348:601–8.
8. WolbinkGJ,VisM,LemsW,VoskuylAE,deGrootE, NurmohamedMT,etal.Developmentofantiinfliximab antibodiesandrelationshiptoclinicalresponseinpatients withrheumatoidarthritis.ArthritisRheum.2006;54:711–5.
9. VincentFB,MorandEF,MurphyK,MackayF,MarietteX, MarcelliC.Antidrugantibodies(ADAb)totumournecrosis factor(TNF)-specificneutralisingagentsinchronic inflammatorydiseases:arealissue,aclinicalperspective. AnnRheumDis.2013;72:165–78.
10.OrdasI,MouldDR,FeaganBG,SandbornWJ.Anti-TNF monoclonalantibodiesininflammatoryboweldisease: pharmacokinetics-baseddosingparadigms.ClinPharmacol Ther.2012;91:635–46.
11.ArstikyteI,KapleryteG,ButrimieneI,VenalisA.Influenceof immunogenicityontheefficacyoflong-termtreatmentwith TNF␣blockersinrheumatoidarthritisandspondyloarthritis
patients.BiomedResInt.2015;2015:604872.
12.vanderLakenCJ,VoskuylAE,RoosJC,StigtervanWalsumM, deGrootER,WolbinkG,etal.Imagingandserumanalysisof immunecomplexformationofradiolabelledinfliximaband anti-infliximabinrespondersandnon-responderstotherapy forrheumatoidarthritis.AnnRheumDis.2007;66:253–6.
13.WeinblattME,KremerJM,BankhurstAD,BulpittKJ, FleischmannRM,FoxRI,etal.Atrialofetanercept,a recombinanttumornecrosisfactorreceptor:Fcfusionprotein, inpatientswithrheumatoidarthritisreceivingmethotrexate. NEnglJMed.1998;340:253–9.
14.RudwaleitM,vanderHeijdeD,LandeweR,ListingJ,AkkocN, BrandtJ,etal.Thedevelopmentofassessmentof
spondyloarthritisinternationalsocietyclassificationcriteria foraxialspondyloarthritis(partII):validationandfinal selection.AnnRheumDis.2009;68:777–83.
15.vanderLindenS,ValkenburgHA,CatsA.Evaluationof diagnosticcriteriaforankylosingspondylitis.Aproposalfor modificationoftheNewYorkcriteria.ArthritisRheum. 1984;27:361–8.
16.NationalInstitutesofHealth.Clinicalguidelinesonthe identification,evaluation,andtreatmentofoverweightand
obesityinadults–theevidencereport.ObesRes.1998;6 Suppl.2:51s–209s.
17.SteenholdtC,BendtzenK,BrynskovJ,ThomsenOO, AinsworthMA.Cut-offlevelsanddiagnosticaccuracyof infliximabtroughlevelsandanti-infliximabantibodiesin Crohn’sdisease.ScandJGastroenterol.2011;46:310–8.
18.VelayosFS,SheibaniS,LocktonS,HauensteinS,SinghS, TerdimanJP,etal.Prevalenceofantibodiestoadalimumab (ATA)andcorrelationbetweenATAandlowserumdrug concentrationonCRPandclinicalsymptomsinaprospective sampleofIBDpatients.GastroenterolHepatol.2013;9Suppl. 4:4–5,8.
19.ArendsS,LebbinkHR,SpoorenbergA,BungenerLB, RoozendaalC,vanderVeerE,etal.Theformationof autoantibodiesandantibodiestoTNF-alphablockingagents inrelationtoclinicalresponseinpatientswithankylosing spondylitis.ClinExpRheumatol.2010;28:661–8.
20.Ben-HorinS,YavzoriM,KatzL,KopylovU,PicardO,FudimE, etal.TheimmunogenicpartofinfliximabistheF(ab′)2,but measuringantibodiestotheintactinfliximabmoleculeis moreclinicallyuseful.Gut.2011;60:41–8.
21.KneepkensEL,WeiJC,NurmohamedMT,YeoKJ,ChenCY,van derHorst-BruinsmaIE,etal.Immunogenicity,adalimumab levelsandclinicalresponseinankylosingspondylitispatients during24weeksoffollow-up.AnnRheumDis.
2015;74:396–401.
22.vanSchouwenburgPA,KrieckaertCL,RispensT,AardenL, WolbinkGJ,WoutersD.Long-termmeasurementof anti-adalimumabusingpH-shift-anti-idiotypeantigen bindingtestshowspredictivevalueandtransientantibody formation.AnnRheumDis.2013;72:1680–6.
23.PandeyJP.ImmunoglobulinGMandKMallotypesandvaccine immunity.Vaccine.2000;19:613–7.
24.BarteldsGM,deGrootE,NurmohamedMT,HartMH,vanEede PH,WijbrandtsCA,etal.Surprisingnegativeassociation betweenIgG1allotypedisparityandanti-adalimumab formation:acohortstudy.ArthritisResTher.2010;12:R221.
25.BraunJ,vandenBergR,BaraliakosX,BoehmH,
Burgos-VargasR,Collantes-EstevezE,etal.2010updateofthe
ASAS/EULARrecommendationsforthemanagementof
ankylosingspondylitis.AnnRheumDis.2011;70:896–904.
26.RutgeertsP,FeaganBG,LichtensteinGR,MayerLF,Schreiber S,ColombelJF,etal.Comparisonofscheduledandepisodic treatmentstrategiesofinfliximabinCrohn’sdisease. Gastroenterology.2004;126:402–13.
27.KheraA,McGuireDK,MurphySA,StanekHG,DasSR, VongpatanasinW,etal.Raceandgenderdifferencesin C-reactiveproteinlevels.JAmCollCardiol.2005;46:464–9.
28.GremeseE,CarlettoA,PadovanM,AtzeniF,RaffeinerB, GiardinaAR,etal.Obesityandreductionoftheresponserate toanti-tumornecrosisfactoralphainrheumatoidarthritis: anapproachtoapersonalizedmedicine.ArthritisCareRes (Hoboken).2013;65:94–100.
29.GremeseE,BernardiS,BonazzaS,NowikM,PelusoG, MassaraA,etal.Bodyweight,genderandresponseto TNF-alphablockersinaxialspondyloarthritis.Rheumatology (Oxford).2014;53:875–81.
30.PalmingJ,GabrielssonBG,JennischeE,SmithU,CarlssonB, CarlssonLM,etal.PlasmacellsandFcreceptorsinhuman adiposetissue–lipogenicandanti-inflammatoryeffectsof immunoglobulinsonadipocytes.BiochemBiophysRes Commun.2006;343:43–8.
32.SaevarsdottirS,WedrenS,SeddighzadehM,BengtssonC, WesleyA,LindbladS,etal.Patientswithearlyrheumatoid arthritiswhosmokearelesslikelytorespondtotreatment withmethotrexateandtumornecrosisfactorinhibitors: observationsfromtheEpidemiologicalInvestigationof RheumatoidArthritisandtheSwedishRheumatology Registercohorts.ArthritisRheum.2011;63:26–36.
33.AbhishekA,ButtS,GadsbyK,ZhangW,DeightonCM. Anti-TNF-alphaagentsarelesseffectiveforthetreatmentof rheumatoidarthritisincurrentsmokers.JClinRheumatol. 2010;16:15–8.
34.ParkSJ,ShinJI.Theeffectofsmokingonresponseanddrug survivalinrheumatoidarthritispatientstreatedwiththeir firstanti-TNFdrug:commentsonthearticlebySoderlinetal. ScandJRheumatol.2012;41:411–2.