Rev. Bras. Reumatol. vol.56 número6
Texto
Imagem
Documentos relacionados
We report a case of Aspergillus meningitis in an immunocompetent patient successfully treated with fluconazole..
We report the case of a female patient with native valve, who had Eikenella corrodens infective endocarditis..
Mylodontidae tem registro nos estados brasileiros: Acre (SIMPSON & PAULA COUTO 1981), São Paulo (CARVALHO 1952), Minas Gerais, Rio Grande do Sul (PAULA COUTO 1979), Mato
Este excerto faz parte do l'vianífesto Separatista, documento distribuído durante a solenidade de criação da República Federativa do Pampa, na cidade de Santa Cruz do Sul,
In the case report “Influenza A H1N1 pneumonia in an immunosuppressed patient after heart transplantation”, we presented a report on a heart transplant patient with a
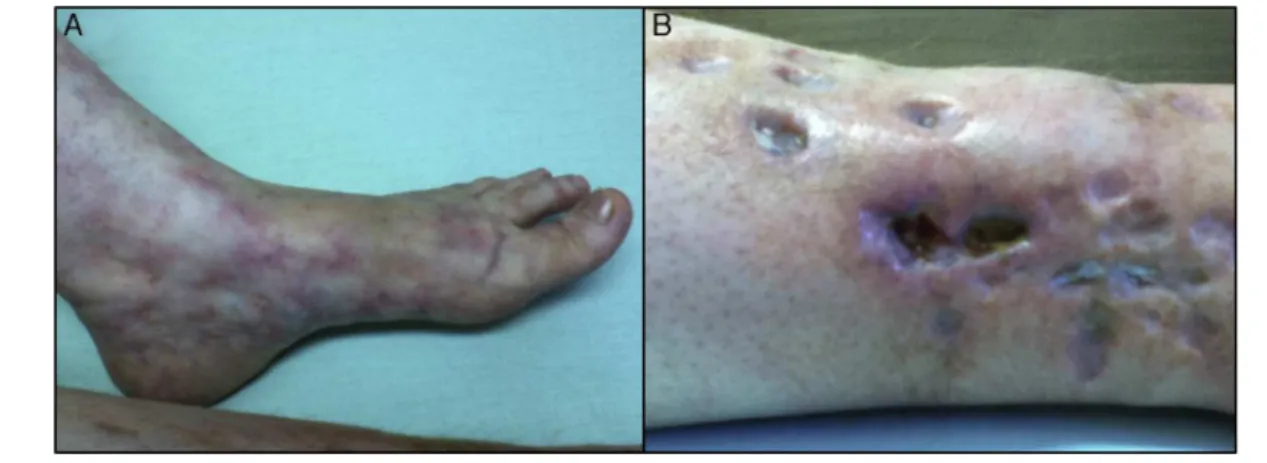
We report the case of a young female patient diagnosed with systemic lupus erythematosus (SLE) associated with the presence of antiphospholipid antibodies for a long time,
We report on a case of lower limb critical ischemia treated using a combination of surgery and endovascular techniques, in an application of the hybrid technique in a
We report an atypical case of treatment of a dialysis patient with multiple comorbidities, severe swelling and pain in the right upper limb (RUL), few alternative sites for
