CEREBRAL ANEURYSMS
A S S E S S M E N T O F 377 C A S E S (1956-1982)
O. HEY * — K. DEI-ANANG * — G. BORGES * — K. SCHÜRMANN * W. MÜLLER **
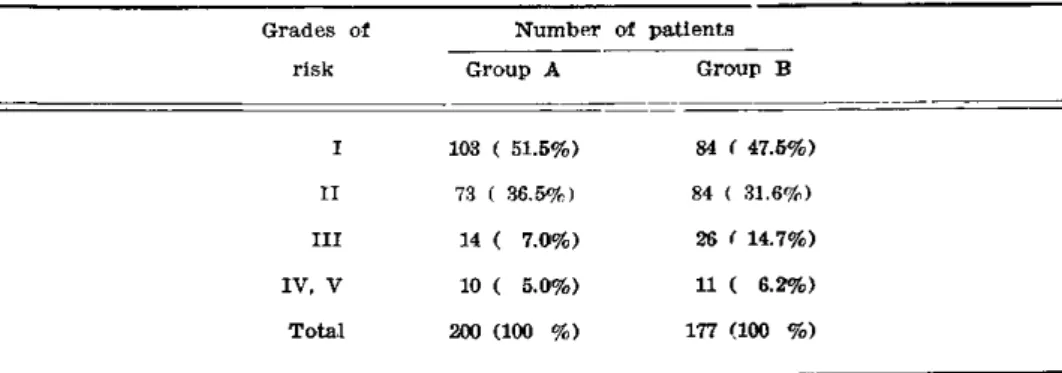
S U M M A R Y — A review of 177 patients with cerebral aneurysms is made, out of whom 106 with ruptured aneurysms w e r e examined, whose operational timing and prognostic chances were well documented ( g r o u p B , 1979-1982) and in part updated to 1984. Furthermore, relevant data of a previous series of 200 cases of cerebral aneurysm, treated between 1956-1978 were used ( g r o u p A ) . The patients w e r e g r a d e d according to H u n t and Hess, assessing the risks involved. The percentages of recurrent bleeding w e r e in g r o u p A 36.5% and 28% in g r o u p B . The incidence of vasospasm (as seen in a n g i o g r a p h y ) w a s in group B 39.6% (42/106 patients). T h e highest rate of vasospasm in the spasm g r o u p division B w a s found to occur in the second and third week after subarachnoid haemorrhage and amounted to 64.7% and 62.5%. A pre-operatively present vasospasm had no negative effects on the mor-tality rate, but influenced the outcome for the survivors effectively. T h e total mormor-tality in g r o u p A was 22.5% and in g r o u p B 11.7%. T i m i n g of the operation among patients in H u n t and Hess-grades I and I I needs to discussion. T h e surgical position of patients in grade V is also certain. W h a t remains to be discussed and needs attention is grade I I I and patients in grade I V a . H e r e the time of operative intervention must be planned indivi-dually depending on the course of the neurological status.
Aneurismas cerebrais: conduta em 377 casos (1956-1982).
R E S U M O — Os autores apresentam revisão de 177 pacientes com aneurisma observados durante o período de 1979 a 1982 ( G r u p o B ) e dos quais 106 sofreram r u p t u r a aneurismática. É feita comparação com série prévia tratada de 1956 a 1978 ( G r u p o A ) , com 20G pacientes. Observou-se a classificação de H u n t e Hess. N o G r u p o A , 36,5% sofreram ressangramento; no Grupo B, 28%. Vasoespasmo foi observado (angiograficamente) em 42 de 106 pacientes do Grupo B (39,6%). Observou-se ainda que o vasoespasmo ocorreu preponderantemente na segunda e na terceira semanas após o sangramento inicial (64.7% — 62,5%). A presença de vasoespasmo pré-operatório não mostrou efeito negativo quando relacionada ao índice de mortalidade, embora tenha influenciado no prognóstico e na recuperação do paciente. A mortalidade do g r u p o A foi 22,5% e no grupo B , 11,7%. O « t i m i n g » cirúrgico para os pacien-tes classificados em g r a u I e g r a u I I ( H u n t e H e s s ) merece ainda discussão. Pacienpacien-tes em grau I I I e grau I V merecem atenção especial: a indicação cirúrgica deve ser planejada individualmente, dependendo da evolução do quadro clínico-neurológico.
*Department of N e u r o s u r g e r y ( H e a d : Prof. D r . h.c. K . S c h ü r m a n n ) ; ** Department of N e u r o r a d i o l o g y H e a d : Prof. D r . S. W e n d e ) , University Hospital, Mainz (Langenbeckstrasse 1, 6500 Mainz 1, D B R ) .
Cerebral aneurysm as a disease poses a challenge to the patient and the neuro-surgeon alike. For the patient the course of the disease is fateful. Subarachnoid haemorrhage ( S A H ) from a ruptured aneurysm is an even more serious variation of this disease. T h e time involved from rupture and onset of bleeding until its closure is of absolute importance to the patient as far as prognosis is concerned. T h e w o r d « t i m i n g » in relationship to surgery of aneurysms w a s coined in order to strategically determine the best appropiate time for surgery in which the least possible damage and complications w o u l d occur and not add to already existing ones. During the course of finding suitable protective measures, Norlen and O l i v e c r o n a S in 1953 showed that excellent results could be expected in g r a d e I and II patients if operations w e r e performed 2-3 w e e k s after S A H . W h e n Hunt and H e s s1
provided grading consisting of neurological deficits, meningeal irritation and state of corciousness a useful para-meter of grading w a s established for clinical use ( T a b l e 1 ) . Recently Y a s a r g i l n has presented a modification of this grading to add aneurysms which have not yet bled as grade 0 and further added r.ubgrading of « a » and « b » for the sake of better diffe-rentiation.
Table 1 — Hunt and Hess grading.
M A T E R I A L . A N D M E T H O D S
Preoperative) management — T h e diagnosis of S A H w a s based on a lumbar puncture and computer tomography ( C T ) . T h e evidence of aneurysm w a s eventually proved b y angiography.
Pre-operative vasospasm — The rate of the pre-operative vasospasm of group A accounted for 32.5% and in group B to 39.6% ( T a b l e 3). T h e vasospasm rate within three days after S A H w a s registered in 27.3%, within, the fourth week 20% and after the fourth week 20%. The highest rate of vasospasm occurs in the second and third week with 76% and 72.7% respectively.
R E S U L T S
The review of the survivors revealed that a total of 74.8% patients fulfilled the criteria for being classified «capable to w o r k » . Grade I and I I patients present with 88.5% a significantly better prognosis than those graded in I I I , I V and V ( T a b l e 4 ) ; 55% of grade I I I patients had serious neurological deficits; 88.8% of grade I V - V patients w e n;
classified to be vegetative-like survivors. Table 5 illustrates the results of the relationship between timing of operation and mortality in relation to risk grading among 166 patients with ruptured aneurysms in group B (1978-1984).
C O M M E N T S
It is generally known and supported by the literature that the general morta-lity rate of cerebral aneurysms could be estimated to 50-60% and morbidity of 20-30% 7
. If untreated, ruptured aneurysms could have a total mortality of as high as 80-90%. Fact is that the highest rate of rebleed occurs or w o u l d occur between the end of the first w e e k and the beginning of the second ( F i g . 1)7,8,11. W h e n a rebleed occurs, the mortality is rated at 8 0 % . Jane et a l .2
and Kassel and T o r n e r4 reported rebleed that occurs within this period to be 2 0 % and 19% respectively. Within the first 24 hours Kassel and T o r n e r 4 reported that the rate of the second S A H could be as high as 4 . 1 % . T h i s finding provided a strong argument for an early surgical intervention among certain groups of neurosurgeons, even though other authors have found this incident to be relatively l o w : 0.8% 7
unlikely that factors which increase the risk of operation also significantly protect the patient from the rerupture during the w a i t i n g p e r i o d » . T h i s implies that the quickest possible period must be found to operate in order to reduce the risk of rerupture to an absolute minimum. It provides a strong argument for an early o p e -ration.
Which risks and complications should be considered? Grading however v i e w e d , provides general guidelines reflecting only a rough estimation of the extention of brain damage after aneurysm rupture. A n y g r a d i n g system presents certain difficulties of a kind. Refering Y a s a r g i l n « e a c h proposed grade includes a spectrum of patients grouped together regardless of ( 1 ) a g e , ( 2 ) general medical state and basic physical condition, ( 3 ) vasospasm, ( 4 ) state of intracranial pressure ( I C P ) , ( 5 ) alteration of the cerebral perfusion ( C B F ) , and ( 6 ) S A H and intracerebral haematomas»:
I. A g e — Y o u n g e r patients in general have better chances of survival than older ones of the same grading.
II. Medical condition — A n alert patient without neurological deficit must be in a medically and physically g o o d condition to reduce the risk of morbidity after operation.
after a certain period of time must be interpreted carefully. T h e y could be anything else but not reactive vasospasm, for example: ( a ) arteritis, ( b ) intima proliferation of the vessel, ( c ) intravasal oedema, ( d ) calcification ( p l a q u e s ) » . ^
I V . 1CP — "Whereas increase of I C P in general should be considered to be a factor which w o u l d not favour surgery, there seems to be a difference in perspective in the literature concerning I C P . Nornes 6 thinks an increased I C P provides a support for the aneurysm w a l l and therefore lowers the incidence of rebleeding, whereas Suzuki prefers cerebrospinal fluid ( C S F ) drainage which he is convinced benefits a decrease of I C P 8.11.
V . S A H and intracerebral haematomas — A c c o r d i n g to Jellinger 3, aneurysms account for 2 2 % of all hemispheric intracerebral bleedings. T h e localisation of such bleeding would give rise to suspicion when they are typical and close to areas of the cerebral vessels where aneurysms could be expected, for example in the temporal lobe in the vicinity of the sylvian fissure typical for median trifurcation aneurysms or frontal region, typical for the anterior communicating aneurysm. A n g i o g r a p h y must be per-formed to rule out the existence of a malformation.
Our general concept of management — In general w e base the concept of management along the guidelines of the Hunt and Hess-grading. Our Neurosurgical Department in Mainz maintains an interdisciplinary 24-hour-service in cooperation with the Departments of N e u r o r a d i o l o g y and Anaesthesiology.
Patients admitted in Hunt and Hess I, when they meet medical conditions suitable for operation, undergo a C T examination and angiography immediately. W h e n the diag-nosis of an aneurysm is made, a basic X e n o n - C B F measurement is quickly performed which is manned also 24 hours in service, either with the standard C B F installation or a smaller mobile unit which is available in the intensive care unit. After that the operation is planned. Generally lumbal C S F drainage is made before and during the operation. Patients in Hunt and Hess II are treated along similar lines.
T h e problem of decision making as to when to operate arises according to our expe-rience with patients in Grade 111. Generally, w e prefer « a wait and see attitude» of about 24 hours. In this stage w e do not operate in the acute situation. If after 24 hours the patient's condition becomes better under observation and treatment with calcium antagonists, and be graded as I I , the operation is performed. It becomes evident that patients w h o s e conditions worsen most likely develop vasospasm. Although there are sometimes discrepancies in the proof of vasospasm by means of C B F measu-rement, it still gives us enough evidence and indication of the state of the cerebral perfusion. Recently w e have added into our supplementary predictive diagnostic methods transcranial Doppler examinations as an additional means of obtaining information about the state of intracerebral blood flow.
Patients in Hunt and Hess-grading I V and V are never operated on acutely with the exception of patients in grades I V and V with massive intra- or extracerebral haematomas. Haematomas with space occupying effect must be evacuated. Depending on the general condition of the patient and neurological status one must make a choice between acute removal of the clot alone or perform angiogram with the intention of closing the aneurysm. In many cases it is possible to clip the aneurysm in the same sitting. In general, according to our experience most of such patients are in the group of a high Hunt- and Hess-grading of I V - V . T h e prognosis is gene-rally bad with a high rate of morbidity, and neurological deficit.
Smaller haematomas without midline shifting must be treated along the lines for management of the aneurysm in the Hunt- and Hess-grading.
R E F E R E N C E S
1. H u n t W E , Hess R M — Surgical risk as related to time of intervention in the repair of intracranial aneurysms. J N e u r o s u r g 28:14, 1968.
2. Jane J A , W i n n H R , Richhardson AE — T h e natural history of intracranial aneurysms: rebleeding rates during the acute and long term period and implication for surgical management. Clin N e u r o s u r g 24:176, 1977.
4. Kassel N F , T o m e r JC — Aneurysmal rebleeding: a preliminary report from the Coopera-tive A n e u r y s m Study. N e u r o s u r g e r y 13:479, 1983.
5. Norlen G, Olivecrona H — The treatment of aneurysms of the circle of W i l l i s . J N e u r o s u r g 10:404, 1953.
6. Nornes H — T h e role of intracranial pressure in the arrest of hemorrhage in patients with ruptured intracranial aneurysms. J N e u r o s u r g 39:226, 1973.
7. Rosenorn J, Eskesen V , Schmidt K , Ronde F — T h e risk of rebleeding from ruptured intracranial aneurysms. J N e u r o s u r g 67:329, 1987.
8. Suzuki J. K o d a m a N , F u i i w a r a S — Surgical treatment of internal carotid-posterior communicating aneurysms: from the experience of 213 case3. In Suzuki J — Cerebral Aneurysms. N e u r o n , Tokyo, 1979, p g 256.
9 WiLkins RH — Attempted prevention of treatment of intracranial arterial spasm: a survey. N e u r o s u r g e r y 6:198, 1980.