REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
OfficialPublicationoftheBrazilianSocietyofAnesthesiologywww.sba.com.br
SCIENTIFIC
ARTICLE
Adverse
respiratory
events
after
general
anesthesia
in
patients
at
high
risk
of
obstructive
sleep
apnea
syndrome
Daniela
Xará
a,
Júlia
Mendonc
¸a
a,
Helder
Pereira
a,
Alice
Santos
a,
Fernando
José
Abelha
a,b,c,∗aDepartmentofAnaesthesiology,CentroHospitalardeSãoJoão,Porto,Portugal
bAnaesthesiologyandPerioperativeCareUnit,FaculdadedeMedicina,UniversidadedoPorto,Porto,Portugal cSurgicalDepartmentofFacultyofMedicine,UniversityofPorto,Portugal
Received23December2013;accepted5February2014 Availableonline12March2014
KEYWORDS
Obstructivesleep apnea;
Respiratoryevents; Postoperative outcome
Abstract
Introduction:PatientswithSTOP-BANGscore>3haveahighriskofObstructivesleepapnea. Theaimofthisstudywastoevaluateearlypostoperativerespiratorycomplicationsinadults withSTOP-BANGscore>3aftergeneralanesthesia.
Methods:Thisisaprospectivedoublecohortstudymatching 59pairsofadultpatientswith STOP-BANGscore>3(highriskofobstructivesleepapnea)andpatientswithSTOP-BANGscore <3(lowriskofobstructivesleepapnea),similarwithrespecttogender,ageandtypeofsurgery, admittedafterelectivesurgeryinthePost-AnaesthesiaCareUnitinMay2011.Primaryoutcome wasthedevelopmentofadverserespiratoryevents.Demographicsdata,perioperative varia-bles,andpostoperativelengthofstayinthePost-AnesthesiaCareUnitandinhospitalwere recorded.TheMann---Whitneytest,thechi-squaretestandtheFisherexacttestwereusedfor comparisons.
Results:Subjectsinbothpairsofstudysubjectshadamedianageof56years,including25% males,and59%weresubmittedtointra-abdominalsurgery.Highriskofobstructivesleepapnea patients hadahighermedianbodymassindex(31versus24kg/m2,p<0.001)andhadmore frequentlyco-morbidities,includinghypertension(58%versus24%,p<0.001),dyslipidemia(46% versus17%,p<0.001)andinsulin-treateddiabetesmellitus(17%versus2%,p=0.004).These patientsweresubmittedmorefrequentlytobariatricsurgery(20%versus2%,p=0.002).Patients withhighriskofobstructivesleepapneahadmorefrequentlyadverserespiratoryevents(39% versus10%,p<0.001),mildtomoderatedesaturation(15%versus0%,p=0.001)andinability tobreathedeeply(34%versus9%,p=0.001).
Conclusion: After general anesthesia high risk of obstructive sleep apnea patients had an increasedincidenceofpostoperativerespiratorycomplications.
© 2014SociedadeBrasileirade Anestesiologia.Publishedby ElsevierEditoraLtda.Allrights reserved.
∗Correspondingauthor.
E-mails:[email protected],[email protected](F.J.Abelha).
0104-0014/$–seefrontmatter©2014SociedadeBrasileiradeAnestesiologia.PublishedbyElsevierEditoraLtda.Allrightsreserved.
PALAVRAS-CHAVE
Apneiaobstrutivado sono;
Eventosrespiratórios; Desfechono
pós-operatório
Eventosrespiratóriosadversosapósanestesiageralempacientescomaltoriscode síndromedaapneiaobstrutivadosono
Resumo
Justificativaeobjetivo:OspacientescomescoreSTOP-BANG>3possuemaltoriscode desen-volver apneia obstrutiva do sono. O objetivo deste estudo foi avaliar as complicac¸ões respiratóriasnopós-operatórioimediatoemadultoscomescoreSTOP-BANG>3apósanestesia geral.
Métodos: Estudoprospectivodedupla-coorte,comparando59paresdepacientesadultoscom escoreSTOP-BANG>3(altoriscodeapneiaobstrutivadosono)epacientescomescore STOP-BANG<3(baixoriscodeapneiaobstrutivadosono),similaresnoquedizrespeitoaogênero, idadeetipodecirurgia,admitidosapósacirurgiaeletivaemsaladerecuperac¸ãopós-anestésica (SRPA)emmaiode2011.Odesfechoprimáriofoiodesenvolvimentodeeventosrespiratórios adversos.Dadosdemográficos,variáveisnoperioperatórioetemposdepermanêncianaSRPAe nohospitalapósacirurgiaforamregistrados.OstestesdeMann-Whitney,qui-quadradoeexato deFisherforamusadosparacomparac¸ão.
Resultados: Osindivíduosdeambososgruposdepacientesdoestudotinhamumamédiade idade de 56 anos, 25% eram do sexo masculino e 59% foram submetidos à cirurgia intra-abdominal.Ospacientescomaltoriscodeapneiaobstrutivadosonoapresentavamumamediana maiordoíndicedemassacorporal (31versus24kg/m2,p<0,001)ecomorbidadesmais fre-quentes,como hipertensão (58%vs. 24%,p<0,001), dislipidemia(46%vs. 17%,p<0,001) e diabetesmelitodependentedeinsulina(17%vs.2%,p=0,004).Essespacientesforam submeti-doscommaisfrequênciaàcirurgiabariátrica(20%vs.2%,p=0,002).Ospacientescomaltorisco deapneiaobstrutivadosonoapresentarammaiseventosrespiratóriosadversos(39%vs.10%,
p<0,001),dessaturac¸ãodeleveamoderada(15%vs.0%,p=0,001)eincapacidadederespirar profundamente(34%vs.9%,p=0,001).
Conclusões:Após a anestesia geral, os pacientes com alto risco de apneia obstrutiva do sonoapresentaram umaumentodaincidênciadecomplicac¸õesrespiratóriasnoperíodo pós-operatório.
©2014SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Todosos direitosreservados.
Introduction
Obstructivesleepapnea(OSA)canoccurinallagegroups1
andis acommon formofsleep-disorder breathing affect-ing2---26%of thegeneral population.2 Studieshave shown
thatpatientswithOSAhaveanassociatedincreasein mor-bidity and mortality.3,4 These patients also have higher
ratesofpostoperativecomplications.5---9Sincemanypatients
with OSA have not been formally diagnosed at the time of surgery,10 preoperative management and the adoption
of measures to reduce postoperative risk are difficult to apply. It is estimated that a great number of men or womenwithmoderate-to-severesleepapneahavenotbeen diagnosed.11 Overnightpolysomnography (PSG)is stillthe
‘‘goldstandard’’fordiagnosisofOSA,butitmaybe unfea-sibletoperformduringthepreoperativeevaluation.
The routine performance of preoperative screening instrumentsis important toidentifypatientswith undiag-nosedOSA.12---14 Many tools for screening patients for OSA
havebeenproposed---suchastheBerlinquestionnaire,the STOPquestionnaireandtheAmericanSocietyof Anesthesiol-ogists(ASA)checklist---andtheiruseimprovesthelikelihood of identifying OSA preoperatively.1,9,13,15 The STOP-BANG
questionnaire (Table 1), which wasvalidated for surgical
population by F. Chunget al.,is a scoring model consist-ing of eighteasily administered questions,referred to by theacronymSTOP-BANG(Snoring,Tirednessduringdaytime, Observedapnea,highbloodpressure,bodymassindex,age, neck circumference,gender). Thisquestionnaire isscored basedonYes/Noanswers(score:1/0),andscoresrangefrom avalueof0to8.Ascoreof≥3hasshownahighsensitivity
for detectingOSA: 93%and100%formoderate andsevere OSA,respectively.12Owingtoitshighsensitivityandbeingan
easy-to-useandascreeningtool,theSTOP-BANG question-naireis considered veryuseful toidentifypatients having moderateandsevereOSA.12
InsurgicalpatientstheprevalenceofOSAisevenhigher than in the general population and it can vary broadly according to the presence of medical comorbidities.16 In
particular,asmanyas70%ofpatientsundergoingbariatric surgery were found to have OSA.17 OSA has been
recog-nized as a potential independent risk factor for adverse perioperative outcome.18 OSA patients undergoing
surgi-cal procedures are vulnerable to postoperative airway obstruction,18 myocardial ischemia, congestive heart
fail-ure,strokeandoxygendesaturation.18---20PatientswithOSA
Table1 STOP-BANGquestionnaire.HighriskofOSA:Yesto≥3questions.LowriskofOSA:Yesto<3questions.
SNORING:doyousnoreloudly(loudenoughtobeheardthroughcloseddoors)? YES NO TIRED:doyouoftenfeeltired,fatigued,orsleepyduringdaytime? YES NO OBSERVED:hasanyoneobservedyoustopbreathingduringyoursleep? YES NO BLOODPRESSURE:doyouhaveorareyoubeingtreatedforhighbloodpressure? YES NO
BMI:BMImorethan35kgm−2? YES NO
AGE:ageover50yearsold? YES NO
NECKcircumference:neckcircumference>40cm? YES NO
GENDER:male? YES NO
anesthesiamay increasethe risk for prolonged periodsof apnea.14
The objective of this study was to evaluate the early postoperative respiratory complications in patients with STOP-BANGscore≥3,aftergeneralanesthesia.
Methods
TheCentroHospitalarSãoJoãoEthicsCommitteeapproved thisstudyandwritteninformedconsentwasobtainedfrom all participants. Centro Hospitalar São João, in Porto, is an 1124-bedtertiary hospitalinametropolitanarea serv-ing3,000,000people.Thisprospectivedouble-cohortstudy wasconductedina13-bedPost-AnesthesiaCareUnit(PACU) over a three-week period(from May 9 to May 27, 2011). Everypatientabletoprovidewritteninformedconsentand admittedtothePACUaftergeneralanesthesiawasincluded inthe study.Exclusioncriteriawerepatientrefusal, inca-pacity of providing informed consent, a score of <25 in the Mini-Mental StateExamination (MMSE), age below 18 years, foreign nationality, known neuromuscular disease, urgent/emergentsurgeryandcardiacsurgery,neurosurgery orotherproceduresthatrequiredtherapeutichypothermia. All patients were interviewedeither in theeve of the surgeryor onthe day ofthe surgery,at least threehours beforesurgery,in thesurgical ward.Duringthisinterview the consentwasobtained, MMSEtest and theSTOP-BANG questionnairewerecompletedandthemedicalhistorywas collected.
Anesthesiologistswereblindedtopatientinvolvementin thestudy.Anesthesia wasprovidedandmonitored accord-ing to the criteria of the anesthesiologist in charge, but thisconductfollowedminimumdepartmentalstandards.In accordancetoourstandardprocedures,generalanesthesia wasinducedwithanintravenousanestheticincombination with an opioid, followed when needed by neuromuscular blockade(NMB).Anesthesiawasmaintainedbytotal intra-venousanesthesia(TIVA)orwithinhalationanesthetics.The anesthesiologist was free to choose to use nitrous oxide. Fluidmanagementwascompletelyguidedbythe anesthesi-ologist.
Neuromuscularblockingdrugs(NMBD)wereusedfor tra-cheal intubation, and additional boluses were provided, if needed. Nowritten policyexists concerning theuse of neuromuscular monitoring, so this was performed at the discretionoftheanesthesiologist.
To ensure that the anesthesiologist remained blinded to the patients’ participation in the study, we did not
attempt to observe the intraoperative use or interpreta-tionof Train-of-Four(TOF). The anesthesiologist wasfree to decide whether to reverse the NMB with neostigmine at the conclusion of the surgical procedure. Usually, the patientwasextubatedintheoperatingroomandtransferred tothePACU.All subjectswere administered100% oxygen byafacemaskaftertrachealextubation.The anesthesiolo-gistinchargedecidedwhethertoadministeroxygenduring thetimebetweentransfertothecartandadmissiontothe PACU.
UponarrivalatthePACUoxygenwasprovidedtoall sub-jectsby a nasal cannulaor face mask, with the decision ofthe type andoxygen concentrationbeing takenby the anesthesiologistscheduledtothePACU.
Residualneuromuscularblockade(RNMB)wasdefinedas TOF<0.9 and it was quantified at admission tothe PACU using acceleromyography of the adductor pollicis muscle (TOF-Watch®).ThreeTOFmeasurements(separatedby15s)
were obtained, and the average of the three values was recorded.Ifavaluedifferedfromtheothersbymorethan 10%,anadditionalTOFmeasurementwasobtainedandthe closest three ratios were averaged. Neuromuscular block wasre-assessedhourlywhilepatientsmaintainedTOF<0.9. When patients had a TOF below 0.9, then the attending anesthesiologistwascontactedandinformed.
PatientswereclassifiedasbeingathighriskforOSA (HR-OSA) if their STOP-BANG score was 3 or more and were classifiedasbeingatlowriskofOSA(LR-OSA)iftheirscore waslessthan3.
Adouble-cohortstudydesignwithprospectivelydefined caseswasperformed.Allcasesduringthestudyperiodwith HR-OSA were identified and then matched with selected controlpatients for comparison. Cases and controls were identified by collecting data on all consecutive patients arriving in the PACU during the study period. The cases consisted of all HR-OSA patients and were matched with similarinrespecttogender,ageandtypeofdefinedas intra-abdominal,musculoskeletalorheadandneck,admittedin thePACUaftergeneralanesthesiaforelectivesurgery.
TheLR-OSApatients wereclassifiedbasedona one-to-onematchwiththeHR-OSApatientsandwereselectedfrom theconsecutivepatientswithoutSTOP-BANG≥3according
tothematchingcharacteristics.
for each patient, signaling a point for each of the fol-lowing risk factors: high risk surgery, history of ischemic heart disease, history of congestive heart failure, history of cerebrovascular disease, pre-operative treatment with insulinfordiabetesmellitusandpre-operativeserum creati-nine>2.0mg/dl.21Surgicalriskswereevaluatedaccordingto
theCardiacRiskStratificationforNoncardiacSurgical Proce-duresofthe2007guidelinesofPerioperativeCardiovascular EvaluationandCare for NoncardiacSurgery ofthe Ameri-canCollegeofCardiology/AmericanHeartAssociationTask ForceonPracticeGuidelines.22
Premedicationwithbenzodiazepinesanditschronicuse wererecorded. Intraoperative details were alsorecorded andincluded typeanddurationofanesthesia, andtheuse ofNMBDandneostigmine.
Patients’tympanictemperatureandmeantrain-of-four ratiowererecordedonadmissiontothePACU.Allpatients hadcontinuous monitoringof blood pressure,cardiac fre-quency, electrocardiogram (ECG) and peripheral oxygen saturation,andmeantrain-of-fourratiorecordedon admis-siontothePACU.
Thepostoperativedataregisteredincludedmortalityand lengthofhospitalandPACUstay.
Earlypostoperativeadverserespiratoryevents
Eachpostoperative adverse respiratoryevents (ARE)were defined on the data collection sheet using the following criteriausingaclassificationdescribedbyMurphyetal.23:
1. Upperairwayobstructionrequiringanintervention(jaw thrust,oralairway,ornasalairway);
2. Mild-moderate hypoxemia (O2 saturations (SpO2) of
93%---90%) on 3L nasal cannula O2 that was not
improvedafteractiveinterventions(increasingO2flows
to>3L/min,applicationofhigh-flowfacemaskO2,verbal
requeststobreathedeeply,tactilestimulation); 3. Severe hypoxemia (SpO2 <90%) on 3L nasal cannula
O2 that was not improved after active interventions
(increasingO2flowsto>3L/min,applicationofhigh-flow
facemaskO2,verbalrequeststobreathedeeply,tactile
stimulation);
4. Signs of respiratory distress or impending ventilatory failure(respiratoryrate>20breathsperminute, acces-sorymuscleuse,trachealtug);
5. Inability to breathe deeply when requested to by the PACUnurse;
6. Patientcomplainingofsymptomsofrespiratoryorupper airwaymuscle weakness(difficulty breathing, swallow-ing,orspeaking);
7. PatientrequiringreintubationinthePACU;
8. Clinical evidence or suspicion of pulmonary aspiration
after trachealextubation(gastriccontents observedin theoropharynxandhypoxemia).
During PACU stay the patients were observed continu-ouslybythePACUnurseswhocontactedastudyinvestigator without delay if an ARE was observed. The inability to breathedeeplyandassessmentofsymptomsofrespiratory orupperairwaymuscleweaknessweredoneatintervalsof 10min.Oneother investigator ofthestudy thenobserved
the patienttoverifythatthe patientmetat leastone of thecriteriaforanARE.
Statisticalanalysis
Variabledescriptiveanalysiswasusedtosummarizethedata andMann---WhitneyUtestwasusedforcomparisonof con-tinuousvariablesbetweengroupsofindividuals;Chisquare testandFisher’sexacttestwereusedforcomparisonof pro-portions betweengroups ofindividuals. Allvariableswere consideredsignificantwhenp<0.05.
Thestatistical softwarepackageSPSSfor Windows ver-sion19.0(SPSS,Chicago,IL)wasusedtoanalyzethedata.
Results
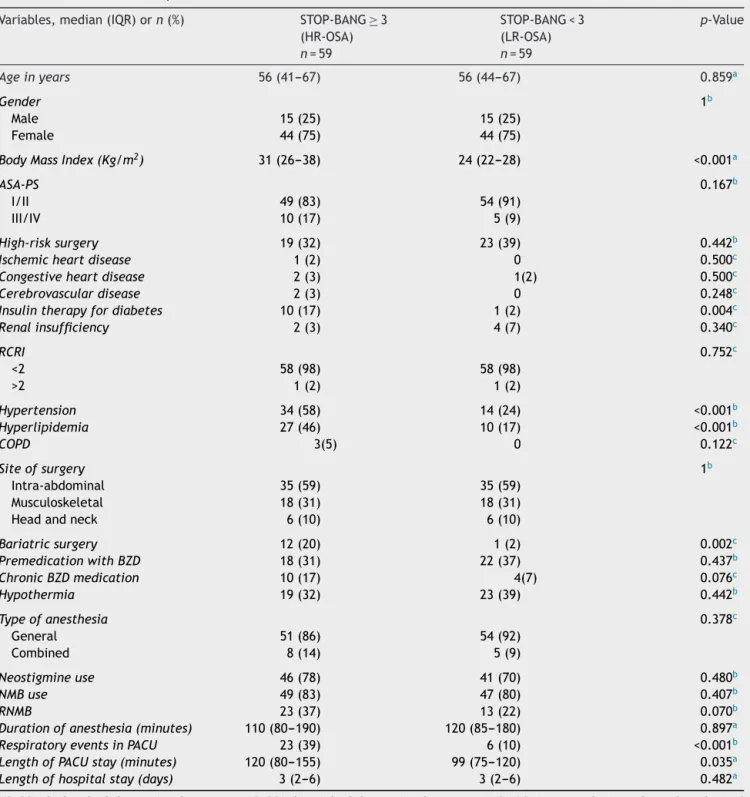
Atotalof59pairsofstudysubjectswereadmittedinPACU duringtheperiodofthestudy.Table2presentsthe charac-teristicsofpatientsadmittedinthePACU,thesurgicaldata, anestheticmanagement,thepostoperativedataanda com-parisonbetweenthepatientswithHR-OSAandpatientswith LR-OSA.Bothpairsofstudysubjectshadamedianageof56 years,included25%males,and59%weresubmittedto intra-abdominalsurgery.Combinedanesthesiawasusedin13of the118patientsstudied.
Patients with HR-OSA had a higher body mass index (median 31 versus 24kg/m2, p<0.001) andhad more
fre-quentlyco-morbidities,includinghypertension(58%versus 24%,p<0.001),dyslipidemia(46%versus17%,p<0.001)and insulin-treateddiabetesmellitus(17%versus2%,p=0.004). Thesepatientsweresubmittedmorefrequentlytobariatric surgery(20%versus2%,p=0.002).
Twenty-ninepatientsoftheentirepopulationpresented ARE(24.6%;95%confidenceinterval:16.7,32.5)(Table3); 25wereunabletobreathedeeplywhenrequested(21.2%; 95% confidence interval: 13.7, 28.7), 9 had symptoms of respiratory or upper airway muscle weakness (7.6%; 95% confidenceinterval:2.8,12.5),9developedmild-moderate hypoxemia(7.6%;95%confidenceinterval:2.8,12.5),6had upper airway obstruction (5.1%; 95% confidence interval: 1.1, 9.1), 5 had severe hypoxemia(4.2%; 95% confidence interval:0.1,7.9)and5presentedsignsofrespiratory dis-tress(4.2%;95% confidenceinterval:0.1,7.9).Nopatient requiredre-intubationorhadclinicalevidenceorsuspicion ofpulmonaryaspiration.
Patients with HR-OSA developed more respiratory complicationsinthePACU(39%versus10%,p<0.001).Only HR-OSA patients hadmild-moderatehypoxemia andthese patientsalsoshowedhighinabilitytobreathedeeply(34% versus9%,p=0.001).
HR-OSApatients hadamedian longerstay in thePACU (120minversus99min,p=0.035).Lengthofstayinthe hos-pitalwassimilarinbothgroupsofpatients.
Discussion
The majorityof OSApatients scheduledtosurgeryremain withoutaformaldiagnosis.Thisentitymaybeconsidereda prevalentconditionamongsurgicalpatientsandmaycause significant adverse effects in the perioperative period.10
Table2 Characteristicsofpatients.
Variables,median(IQR)orn(%) STOP-BANG≥3
(HR-OSA)
n=59
STOP-BANG<3 (LR-OSA)
n=59
p-Value
Ageinyears 56(41---67) 56(44---67) 0.859a
Gender 1b
Male 15(25) 15(25)
Female 44(75) 44(75)
BodyMassIndex(Kg/m2) 31(26---38) 24(22---28) <0.001a
ASA-PS 0.167b
I/II 49(83) 54(91)
III/IV 10(17) 5(9)
High-risksurgery 19(32) 23(39) 0.442b
Ischemicheartdisease 1(2) 0 0.500c
Congestiveheartdisease 2(3) 1(2) 0.500c
Cerebrovasculardisease 2(3) 0 0.248c
Insulintherapyfordiabetes 10(17) 1(2) 0.004c
Renalinsufficiency 2(3) 4(7) 0.340c
RCRI 0.752c
<2 58(98) 58(98)
>2 1(2) 1(2)
Hypertension 34(58) 14(24) <0.001b
Hyperlipidemia 27(46) 10(17) <0.001b
COPD 3(5) 0 0.122c
Siteofsurgery 1b
Intra-abdominal 35(59) 35(59)
Musculoskeletal 18(31) 18(31)
Headandneck 6(10) 6(10)
Bariatricsurgery 12(20) 1(2) 0.002c
PremedicationwithBZD 18(31) 22(37) 0.437b
ChronicBZDmedication 10(17) 4(7) 0.076c
Hypothermia 19(32) 23(39) 0.442b
Typeofanesthesia 0.378c
General 51(86) 54(92)
Combined 8(14) 5(9)
Neostigmineuse 46(78) 41(70) 0.480b
NMBuse 49(83) 47(80) 0.407b
RNMB 23(37) 13(22) 0.070b
Durationofanesthesia(minutes) 110(80---190) 120(85---180) 0.897a
RespiratoryeventsinPACU 23(39) 6(10) <0.001b
LengthofPACUstay(minutes) 120(80---155) 99(75---120) 0.035a
Lengthofhospitalstay(days) 3(2---6) 3(2---6) 0.482a
HR-OSA,high-riskofobstructivesleepapnea;LR-OSA,low-riskofobstructivesleepapnea;ASA-PS,AmericanSocietyofanesthesiologists’ physicalstatus;RCRI,revisedcardiacriskindex;COPD,chronicobstructivepulmonarydisease;BZD,benzodiazepine;NMB,neuromuscular blockade;RNMB,residualneuromuscularblockade;PACU,Post-AnesthesiaCareUnit.
a Mann---WhitneyUtest. b Pearson’schi-squaredtest. c Fisher’sexacttest.
OSA topromotetheimplementationof strategiesto mini-mizetheperioperativeriskofadverseevents.Astheclinical historyisanunreliableindicatorofthepresenceofOSA,and PSGisnotavailableforallsurgicalpatients,itisnecessarily aneffectivescreeningmodality.24
TheSTOPquestionnairewasvalidatedinsurgicalpatients at preoperative clinics as a screening tool and it has
demonstrated a high sensitivity and Negative Predictive Value, especially for patients with moderate to severe OSA.12,15
Thereportedincidenceofadverserespiratoryeventsin thePACUvarieswidely,withobservationalstudiesdescribing anincidenceof1.3%---34%25---27dependingonAREstudiedand
Table3 Postoperativecomplications.
All(n=118) HR-OSA (LR-OSA)p
Respiratorycomplications 29(25) 23(39) 6(10) <0.001
Obstructionairway 6(5) 4(7) 2(3) 0.340
Mild-moderatehypoxemia 9(8) 9(15) 0 0.001
Severehypoxemia 5(4) 3(5) 2(3) 0.500
Respiratoryfailure 5(4) 3(5) 2(3) 0.500
Inabilitytobreathedeeply 25(21) 20(34) 5(9) 0.001
Muscleweakness 9(8) 7(12) 2(3) 0.081
HR-OSA,high-riskofobstructivesleepapneasyndrome;LR-OSA,low-riskofobstructivesleepapneasyndrome.
Differentstudies had alreadydocumented the associa-tionofOSAwithcomorbidities8,28,29andinourstudyHR-OSA
patients had more frequently hypertension, dyslipidemia and renal failure,but we could not show the association betweenOSAandischemicorcongestiveheartdiseasethat wasestablishedbyothers.28,29Onereasonforthismightbe
relatedtotherelativelowmedianageofourpopulation. OSA hasbeen described asan independentrisk factor forperioperativepulmonarycomplications,30,31butthereis
littleevidencedescribingrespiratorycomplicationsofOSA patientsatPACU.Liaoetal.8documentedthatthemajority
ofthepostoperativecomplicationsoccurredafterpatients weretransferredtothewardand thatthemajor contrib-utortothehighoccurrenceofpostoperativecomplications inOSApatientswastheincreasedincidenceofrespiratory complications.
Our study shows that after surgery HR-OSA patients mayhave ahigh risk of AREandthey hada nearly4-fold increaseindevelopingAREinthePACUcomparedwith LR-OSApatients.ThisisaccordingtothestudyofLiaoetal.that hasshownahigherincidenceofpulmonarycomplicationsin patientswithOSA(33%versus22%).
Respiratory complications in theimmediate postopera-tiveperiodcanleadtoincreasedmorbidityandmortality.32
Pulmonary andpharyngeal physiologymay beaffected by perioperativefactorsthatmayhavedetrimentaleffectsin patientswithOSA.33,34Impairmentoftheactivityof
pharyn-geal muscles promoted by pharmacologic and mechanical related factors may be viewed as aggravating factors increasingthe risk for ARE in the postoperative periodin patientswithOSA.23Thestudyofimpactoftheanesthetic
managementwasnottheaimofthepresent study,sothe authors decidedto perform an observational work allow-ing different anesthetic protocols. Actually, only 11% of thepatientsweresubmittedtocombinedanesthesia,soits impactontheoccurrenceofAREcouldnotbestudied.
Patients withHR-OSA presented more RNMB and were morefrequently submitted tobariatric surgery andthese twofactorsmayberesponsibleforthehigherratesofARE. The most common AREoccurring in HR-OSA group was theinabilitytobreathedeeply,recordedin34%ofpatients. Mild-moderate hypoxemia was the second most common AREintheHR-OSAgroupandoccurredin15%.Other stud-ieshavedemonstratedsimilarresultsregardinghigherrisk of hypoxia,13,35,36 but a recent study in morbidly obese
patientsdidnotfindadifferencebetweenOSAandnon-OSA patientsinthenumberofhypoxemicepisodesafterbariatric surgery.37
The consequences of the ARE delaying PACU discharge aredifficulttocalculateanddivergebasedonsingular insti-tutional factors including staffing models, PACU size and readinessforwardbeds.Inthisstudy,HR-OSApatientshad alongerlengthofPACUstay,whichisinconcordancewith themajorityofthestudies.8
Our study has a number of limitations that must be acknowledged.First,thesampleissmallandwascompleted at asinglecenter, makingitdifficult togeneralizeresults beyondourstudysite.Second,werelyonlyonSTOP-BANG score to make the OSA diagnosis because there were no polysomnographicdataavailableforallthepatients;thus, we couldnot quantify the severity of considered HR-OSA patients. Third, the definitions of ARE had some subjec-tivecriteriawhichmayhaveinfluencedthediagnosis.Forth, therespiratoryeventswereonlyregisteredinthePACUand complicationsthatcouldhaveoccurredafterPACUdischarge arenotconsidered.
Andlastly,althoughtheauthorsattemptedtohave simi-larityconcerningthetypeofsurgerythatwasperformedin thetwogroupsstudied,HR-OSA patientsweremoreoften submittedtobariatricsurgeryandthiscouldhaveaffected theincidenceofAREamongthesepatients.
The principal findings of this study were that patients withSTOP-BANGscore≥3hadahigherbodymassindexand
were submittedmore frequentlytobariatric surgery; HR-OSApatientshadmorefrequentlyco-morbidities,including hypertension, dyslipidemia and insulin-treated diabetes mellitus; patients with STOP-BANG score≥3 had a higher
incidenceofpostoperativerespiratorycomplications; inabil-itytobreathedeeplyandmild/moderatehypoxiawerethe most frequent adverse respiratory events in the immedi-atepostoperative periodand theyweremore frequent in patientswithhighriskofOSA.
Conclusion
InconclusionAREwasacommonoccurrenceinthePACUand weremorefrequentlyobservedinHR-OSApatients.
Authorship
beforeits submissionfor publication andare preparedto signastatementstatingtheyhadreadthemanuscriptand agreetoitspublication.
FernandoAbelhamadeallcoordinationofthestudy, per-formed statistical analyses and wrote the draft and the manuscript.DanielaXaráparticipatedinthedesignof the studyandmadethecriticalrevisionofthefinalmanuscript. JuliaMendonc¸aparticipatedinthedesignofthestudyand coordinated the dataacquisition andhelped in databases construction. HelderPereira participated in the designof thestudy,coordinateddatabasesconstructionandhad sub-stantial contribution in acquisition of data. Alice Santos made substantial contributions in the analyses and inter-pretationofdata,wrotethedraftandthemanuscriptand coordinatedrevisionofthefinalmanuscript.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.LettieriCJ, Eliasson AH,Andrada T, etal. Obstructive sleep apneasyndrome:arewemissinganat-riskpopulation?JClin SleepMed.2005;1:381---5.
2.YoungT,HuttonR,FinnL,etal.Thegenderbiasinsleepapnea diagnosis.Arewomenmissedbecausetheyhavedifferent symp-toms?ArchInternMed.1996;156:2445---51.
3.MarshallNS,WongKK,LiuPY,etal.Sleepapneaasan indepen-dentriskfactorfor all-causemortality:theBusseltonHealth Study.Sleep.2008;31:1079---85.
4.YoungT,FinnL,PeppardPE,etal.Sleepdisorderedbreathing andmortality:eighteen-yearfollow-upoftheWisconsinsleep cohort.Sleep.2008;31:1071---8.
5.Gallagher SF, Haines KL, Osterlund LG, et al. Postopera-tivehypoxemia:common,undetected,andunsuspectedafter bariatricsurgery.JSurgRes.2010;159:622---6.
6.Gupta RM, Parvizi J, Hanssen AD, et al. Postoperative complications in patients with obstructive sleep apnea syn-drome undergoing hip or knee replacement: a case-control study.MayoClinProc.2001;76:897---905.
7.KawR,MichotaF,JafferA,etal.Unrecognizedsleepapneain thesurgicalpatient:implicationsfortheperioperativesetting. Chest.2006;129:198---205.
8.LiaoP,YegneswaranB,VairavanathanS,et al.Postoperative complicationsinpatientswithobstructivesleepapnea:a retro-spectivematchedcohortstudy.CanJAnaesth.2009;56:819---28.
9.MemtsoudisS,LiuSS,MaY,etal.Perioperativepulmonary out-comesinpatientswithsleepapneaafternoncardiacsurgery. AnesthAnalg.2011;112:113---21.
10.YoungT,EvansL,FinnL,etal.Estimationoftheclinically diag-nosedproportionofsleepapneasyndromeinmiddle-agedmen andwomen.Sleep.1997;20:705---6.
11.Ancoli-Israel S, Kripke DF, Klauber MR, et al. Sleep-disordered breathing in community-dwelling elderly. Sleep. 1991;14:486---95.
12.ChungF,YegneswaranB,LiaoP,etal.STOPquestionnaire:atool toscreenpatientsforobstructivesleepapnea.Anesthesiology. 2008;108:812---21.
13.ChungF,YegneswaranB,LiaoP,etal.ValidationoftheBerlin questionnaireandAmericanSocietyofAnesthesiologists check-listasscreeningtoolsfor obstructivesleepapneainsurgical patients.Anesthesiology.2008;108:822---30.
14.Finkel KJ, Searleman AC, Tymkew H, et al. Prevalence of undiagnosed obstructive sleep apnea among adult surgical
patientsinanacademicmedicalcenter.SleepMed.2009;10: 753---8.
15.ChungSA,YuanH,ChungF.Asystemicreviewofobstructive sleepapneaanditsimplicationsforanesthesiologists.Anesth Analg.2008;107:1543---63.
16.Shafazand S.Perioperative managementofobstructive sleep apnea:readyforprimetime?CleveClinJMed.2009;76Suppl. 4:S98---103.
17.Romero-CorralA, CaplesSM,Lopez-JimenezF,etal. Interac-tionsbetweenobesityandobstructivesleepapnea:implications fortreatment.Chest.2010;137:711---9.
18.Stierer TL, Wright C, George A, et al. Risk assessment of obstructivesleepapneainapopulationofpatientsundergoing ambulatorysurgery.JClinSleepMed.2010;6:467---72.
19.MarinJM,CarrizoSJ,VicenteE,etal.Long-termcardiovascular outcomesinmenwithobstructivesleepapnoea-hypopnoeawith orwithouttreatmentwithcontinuouspositiveairwaypressure: anobservationalstudy.Lancet.2005;365:1046---53.
20.IsonoS.Obstructivesleepapneaofobeseadults: pathophysi-ology andperioperative airwaymanagement.Anesthesiology. 2009;110:908---21.
21.Lee TH, Marcantonio ER, Mangione CM, et al. Derivation and prospective validation of a simple index for predic-tionofcardiac riskofmajornoncardiacsurgery.Circulation. 1999;100:1043---9.
22.FleisherLA,BeckmanJA,BrownKA,etal.ACC/AHA2007 Guide-linesonPerioperativeCardiovascularEvaluationandCarefor NoncardiacSurgery:ExecutiveSummary:AReportofthe Amer-ican College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines on PerioperativeCardiovascular Evalua-tionforNoncardiacSurgery)DevelopedinCollaborationWith the American Society of Echocardiography, American Soci-ety of Nuclear Cardiology, Heart RhythmSociety, Societyof Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography andInterventions, SocietyforVascular Medicine andBiology,andSocietyforVascularSurgery.JAmCollCardiol. 2007;50:1707---32.
23.Murphy GS, Szokol JW, Marymont JH, et al. Residual neuromuscular blockade and critical respiratory events in the postanesthesia care unit. Anesth Analg. 2008;107: 130---7.
24.Hoffstein V, Szalai JP. Predictive value of clinical fea-tures indiagnosing obstructive sleep apnea.Sleep. 1993;16: 118---22.
25.LiuSS,ChisholmMF,JohnRS,etal.Riskofpostoperative hypox-emiainambulatoryorthopedicsurgerypatientswithdiagnosis ofobstructivesleepapnea:aretrospectiveobservationalstudy. PatientSafSurg.2010;4:9.
26.Murphy GS, Szokol JW, Marymont JH, et al. Intraoperative acceleromyographic monitoring reduces the risk of resid-ual neuromuscular blockade and adverse respiratory events in the postanesthesia care unit. Anesthesiology. 2008;109: 389---98.
27.PedersenT,Viby-MogensenJ,RingstedC.Anaestheticpractice andpostoperativepulmonarycomplications.ActaAnaesthesiol Scand.1992;36:812---8.
28.PatidarAB,AndrewsGR,SethS.Prevalenceofobstructivesleep apnea,associatedriskfactors,andqualityoflifeamongIndian congestiveheart failure patients: a cross-sectional survey.J CardiovascNurs.2011;26:452---9.
29.SinDD,FitzgeraldF,ParkerJD,etal.Riskfactorsforcentral andobstructivesleepapneain450menandwomenwith con-gestive heartfailure. Am JRespirCrit Care Med. 1999;160: 1101---6.
31.Hendolin H, Kansanen M, Koski E, et al. Propofol-nitrous oxideversusthiopentone-isoflurane-nitrous oxideanaesthesia for uvulopalatopharyngoplastyin patients with sleep apnea. ActaAnaesthesiolScand.1994;38:694---8.
32.Gali B, Whalen FX, Schroeder DR, et al. Identification of patients at risk for postoperative respiratory complications using a preoperative obstructive sleep apnea screening tool and postanesthesia care assessment. Anesthesiology. 2009;110:869---77.
33.McNicholas WT, Ryan S. Obstructive sleep apnoea syn-drome: translating science to clinical practice. Respirology. 2006;11:136---44.
34.CiscarMA,JuanG,MartinezV,etal.Magneticresonance imag-ingofthepharynxinOSApatientsandhealthysubjects.Eur RespirJ.2001;17:79---86.
35.FleissJL,WilliamsJB,DubroAF.Thelogisticregressionanalysis ofpsychiatricdata.JPsychiatrRes.1986;20:195---209.
36.Hwang D, Shakir N, Limann B, et al. Association of sleep-disorderedbreathingwithpostoperativecomplications.Chest. 2008;133:1128---34.