REVISTA
BRASILEIRA
DE
REUMATOLOGIA
ww w . r e u m a t o l o g i a . c o m . b r
Original
article
Gait
characteristics
of
women
with
fibromyalgia:
a
premature
aging
pattern
Suelen
M.
Góes
a,∗,
Neiva
Leite
b,
Ricardo
M.
de
Souza
a,
Diogo
Homann
a,
Ana
C.V.
Osiecki
a,
Joice
M.F.
Stefanello
a,
André
L.F.
Rodacki
aaSectorofBiologicalSciences,CenterforMotorBehaviourStudies,UniversidadeFederaldoParaná,Curitiba,PR,Brazil bSectorofBiologicalSciences,CenterofQualityoflife,UniversidadeFederaldoParaná,Curitiba,PR,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received1August2013 Accepted12November2013 Availableonline20August2014
Keywords:
Chronicpain Elderly Gait
a
b
s
t
r
a
c
t
Background:Fibromyalgiaisaconditionwhichinvolveschronicpain.Middle-aged individ-ualswithfibromyalgiaseemtoexhibitchangesingaitpattern,whichmayprematurely exposethemtoagaitpatternwhichresemblesthatfoundintheelderlypopulation.
Objective:Todeterminethe3Dspatial(linearandangular)gaitparametersofmiddle-aged womenwithfibromyalgiaandcomparetoelderlywomenwithoutthiscondition.
Methods:25women(10inthefibromyalgiagroupand15intheelderlygroup)volunteered toparticipateinthestudy.Kinematicswasperformedusinganoptoelectronicsystem,and linearandangularkinematicvariablesweredetermined.
Results:Therewasnodifferenceinwalkingspeed,stridelength,cadence,hip,kneeand ankle joints rangeofmotion betweengroups,exceptthe pelvicrotation,in whichthe fibromyalgiagroupshowedgreaterrotation(P<0.05)comparedtotheelderlygroup.Also, therewasanegativecorrelationwithpelvicrotationandgluteuspain(r=-0.69;P<0.05),and betweenpelvicobliquityandgreatertrochanterpain(r=-0.69;P<0.05)inthefibromyalgia group.
Conclusion: Middle-agedwomenwith fibromyalgiashowedgaitpatternresemblancesto elderly,women,whichischaracterizedbyreducedlowerlimbROM,stridelengthand walk-ingspeed.
©2014ElsevierEditoraLtda.Allrightsreserved.
Características
da
marcha
de
mulheres
com
fibromialgia:
um
padrão
prematuro
de
envelhecimento
Palavras-chave:
Dorcrônica Envelhecimento Marcha
r
e
s
u
m
o
Introduc¸ão: Fibromialgiaéumacondic¸ãoqueenvolvedorcrônicageneralizada.Alémdisso, mulheres de meia idade com fibromialgia apresentam alterac¸ões no padrão de mar-cha,expondo-seprematuramenteaumpadrãodemarchasemelhanteaoencontradona populac¸ãoidosa.
DOIoforiginalarticle:http://dx.doi.org/10.1016/j.rbr.2013.11.003. ∗ Correspondingauthor.
E-mail:[email protected](S.M.Góes). http://dx.doi.org/10.1016/j.rbre.2014.07.001
Objetivo:Determinarosparâmetrosespaciais(lineareangular)damarchademulherescom fibromialgiaecompará-loscomidosassemessacondic¸ão.
Métodos:25mulheres(10nogrupocomfibromialgiae15nogrupodeidosas)sequalificaram comovoluntáriasparaparticipardoestudo.Aanálisecinemáticafoirealizadapormeiode umsistemaoptoeletrônico,easvariáveislineareseangularesforamdeterminadas.
Resultados: Ambos os grupos apresentaram similaridades na velocidade da marcha, tamanhodapassada,cadênciaeamplitudedemovimentodoquadril,joelhoetornozelo (p>0,05),excetoparaarotac¸ãodapelve,naqualogrupocomfibromialgiaapresentoumaior rotac¸ãodequadril(p<0,05)quandocomparadoaogrupodeidosas.Alémdisso,houve correlac¸ãonegativanogrupocomfibromialgiaentrerotac¸ãodoquadriledornoglúteo(r= -0,69;p<0,05),eentreobliquidadedapelveedornaregiãodotrocantermaior(r=-0,69; p<0,05).
Conclusão: Mulheresdemeiaidadecomfibromialgiaapresentaramumpadrão de mar-chasimilaraodeidosas,oqualécaracterizadoporamplitudedemovimento,tamanhoda passadaevelocidadedamarchareduzidos.
©2014ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Fibromyalgia(FM)isanimpairmentdiseasethatinvolves sys-temicchronicpainanditspathogenesisandetiologyarestill notfullyunderstood.1,2 Functionally,FMisacondition
fre-quentlyaccompaniedbydiminishedphysicalworkcapacity3,4
andmuscularfatigue.5Difficultieswithmaintaining
concen-trationduringcognitivetasks,neurologicalcomplaints(e.g. morning stiffness,muscle painand spasms) and mechani-calimpairments(e.g.,fatigueandweakness)havealsobeen reportedinpatientswithFM.5–6Thesesymptomsmayaffect
theirabilitytoperformsimpledailytasksandcauseanegative impactontheirqualityoflife.7
Gaitproblemshavebeen listedasacommon complaint among patients with FM.8 Indeed, when compared to a
matchedcontrolgroup,subjectswithFMshowalteredgait parameters, characterizedby reduced walking speed,cycle frequency,andstridelength9–11 whichare alsoobservedin
theelderly.12,13
Muscle discomfort, as it is seen inFM, is accompanied by reduced range ofmotion and muscle weakness and is positivelycorrelatedwithchangesingait.12–14 Forinstance,
Paschalis et al.15 showed that subjects with ongoing pain
(inducedbydelayedmuscle sorenessinresponsetosevere eccentric exercises bouts) alter a number of gait parame-terstopreventfurthermuscledamageand/ordiscomfort.In general,musclediscomfortandpainareaccompaniedbya reducedrangeofmotionandmuscleweakness,whichare pos-itivelycorrelatedwithgaitchangesandmayberelatedtofall incidence.12,16–18
Thus, middle-aged FM subjects who are chronically exposedtopainalsoshowreducedjointrangeofmotionand maypresentchangesongaitpatternlikelysimilartoelderly persons.Researchers foundthatwomen withFM(between 40and50yearsold)exhibitaslowwalkingspeed,9–11 thatis
describedasthebestfallpredictorinelderlypopulation.19,20
Inaddition,studies havedemonstratedahighincidenceof reportedfallsperyearamongmiddle-agedwomenwithFM (40%-50%),17,21,22whichisevenhigherwhencomparedtothe
elderly.23,24 Furthermore, middle-aged individuals with FM
maybeprematurelyexposedtoagaitpatternwhichresembles theonefoundintheelderly.
Therefore,theaimofthepresentstudywastodetermine spatial (linearandangular)gaitparameters ofmiddle-aged womenwithFMand comparetoagroupofelderlywomen withoutFM.ItwashypothesizedthatsubjectswithFMpresent a gait pattern that resemblesthe pattern exhibited by the elderly, irrespectiveofagedifferencesbetweengroups.The gaitpatternofmiddle-agedwomenwithFMwascomparedto agroupofolderwomenwithoutFM,astheyaredescribedas tohaveanalteredgaitpatternand,thus,aremoreproneto fallsthanyoungandadults.
Methods
Participants
Twenty-one sedentarymiddle-aged womendiagnosedwith FM,accordingtotheAmericanCollegeofRheumatology1990’s criteria2 fromaRheumatologyWard,volunteeredto
partici-pateinthestudy.Twenty-fiveelderlywomen(over65years old)withasedentarylife-stylewithoutFMsymptomswere invitedfromthelocalcommunityandwereallocatedinthe controlgroups.
Anumberofexclusioncriteriawereappliedforbothgroups andincluded:(a)thepresenceofarthritis,(b)arthritis rheuma-toid,(c)uncontrolledchangesinthyroid,(d)BMIgreaterthan 39kg•m–2 and(e)historyoffractures,(f)jointsurgeryor(g)
anyothermedicalproblemsinthesixmonthsbeforethestart ofthisstudy whichcouldinterfereongaitperformance.In addition,theelderlygroupdidnotreportpainsymptomsthat couldinterfereintheirdailylifeactivitiesorwalkingduring datacollection.
and␣ =0.05.Thestandarddeviationoftenunitswasusedfor
theoldergroupandeightunitsfortheFMgroup.Therefore, 15womenfortheoldergroupand10womenfortheFMgroup wereconsideredavalidsamplesizeforeachone.Allsubjects whoagreedtoparticipateinthestudysignedaninformed con-sentform,whichwaspreviouslyapprovedbytheUniversity’s EthicsCommittee.
TheInternational Physical Activity Questionnaire25 was
appliedtoassessthephysicalactivitylevel,andtheAmerican CollegeofSportsMedicinecriteria26wasappliedtodetermine
asedentarylife-style(<150minutesperweek).
Painassessment
TocharacterizetheFMgroup,participantsanswered apain enquiryabout theirglobalpainand forthreespecificareas (tender point region), through a 10cm visual analog scale (VAS),inwhichtheyratedthecurrentlevelofpain,ranging from0cm(nopain)to10cm(worstimaginablepain). Also, thethreespecificpainareas(knee,greattrochanterand glu-teusmaximus)wereassessedwithaVAS,astheymayimpact ongaitperformance.Thesespecificareaswerenamedasknee pain,greattrochanterpainandgluteuspain.
Gaitanalysis
Gaitanalysiswasassessedinasixmeterswalkwaybya3D kinematicssystems(ViconMX13+,ViconMotionSystemInc, USA)at100Hz. Participantswere allowed towalk barefoot alongthewalkway(threetofivetrials)inanattemptto warm-up andto getfamiliarized withthe experimentalprotocol. Afterthewarm-up,eachparticipantwalkedtentrials unas-sistedattheircomfortablespeedalongthewalkway.
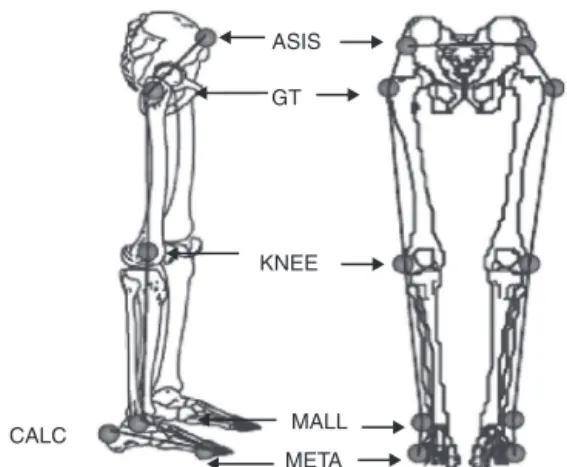
Twelvereflectivemarkerswereattachedtotherightand leftlowerlimb,placedontheanteriorsuperioriliacspine,the mostprominentprotuberanceofthegreatertrochanter, lat-eralfemoralepicondyle,lateralmalleolus,thefifthmetatarsal jointandheels.Fig.1depictsthemarkplacementsites.The markerswereplacedonbothsidesofthebody,however,only therightsidewasusedforanalysis.AsuitofLycrawasworn duringthedatacollectioninanattempttominimize move-mentartifactsduetomovements ofthemarkers.Basedon theselandmarks,athreedimensionalmovement reconstruc-tion was performed. These procedures have been used in otherstudies.13,27Thegaitcyclewasdeterminedasan
inter-valbetweentwoconsecutiveheelstrikes.Heel contactwas definedvisually bytheinstantwherethe heelmarkerwas firstsetontheground.Theensembleaverageofthreeclear gaitcyclesperparticipantwascalculatedtorepresent indi-vidualpatterns.Acleargaitcyclewasthe oneinwhichall markerswere visibleduringthe gaitcycleandsubjects did notperformanystrangemovements(e.g.,scratching).Then, kinematicsdatawereprocessedtoprovideestimatesof lin-ear(walkingspeed,stridelength,cadence)andangular(hip, kneeandanklejointsrangeofmotionandtheirmaximum andminimumvalues)variables.
Inaddition,thekneerangeofmovementwasdividedinto twophasestorepresenttheactionsfromimpacttosupport (ROM1)andfromsupporttopush-off(ROM2).15Thefirstphase
wasdefinedastheperiodbetweenheelstrikeandtheinstant
ASIS
GT
KNEE
MALL
META CALC
Figure1–Bodylandmarksandangulardisplacement
conventions.Representationoftheanatomicallandmarks,
bodysegments,jointsandmovementconvention:ASIS
-anteriorsuperioriliaccrest,GT-themostprominent
protuberanceofthegreatertrochanter,KNEE-lateral
femoralepicondyle,MALL-lateralmalleolus,andMETA
-thefifthmetatarsaljoint,CALC–calcaneus.
the shanksegment isvertical,whilethesecond phasewas definedastheperiodtheshanksegmentisverticaluntil toe-offinstant.TheROM1andROM2allowtodeterminingwhether different strategies were applied in the load response (to absorbimpactforces)andthepush-offphaseofthemovement (togeneratepropulsiveforces).Thejointrangeofmotionwas definedasthedifferencebetweenmaximumextensionand flexiondisplacements.Pelvicrotationwasdefinedaspelvis movementsinthetransversalplanearoundaverticalrotation axisfixedatthehipjointcenter.Pelvicobliquitywasdefinedas therisingandloweringofthepelvisthatoccursinthefrontal planeandaroundahorizontalrotationaxis.
Statistics
Descriptive statistics (mean and standard deviation) were calculated.TheShapiro-Wilktestconfirmeddatanormality, whileLevene’stestconfirmeddatahomogeneity.Differences in spatial gait variables were compared bymean one-way ANOVA,withgroups asfixedfactors.TheSpearman corre-lationcoefficientwasperformedtoidentifytherelationship betweengaitparametersandpainlevelintheFM.The statisti-calprocedureswereperformedusingthesoftwareSTATISTICA 7.0®andthelevelofsignificancewassetatp<0.05.
Results
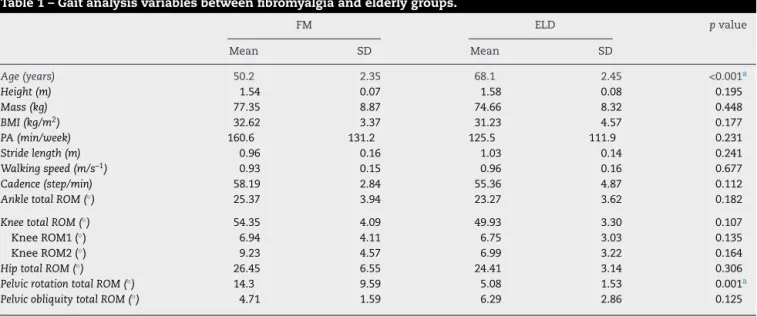
Table1–Gaitanalysisvariablesbetweenfibromyalgiaandelderlygroups.
FM ELD pvalue
Mean SD Mean SD
Age(years) 50.2 2.35 68.1 2.45 <0.001a
Height(m) 1.54 0.07 1.58 0.08 0.195
Mass(kg) 77.35 8.87 74.66 8.32 0.448
BMI(kg/m2) 32.62 3.37 31.23 4.57 0.177
PA(min/week) 160.6 131.2 125.5 111.9 0.231
Stridelength(m) 0.96 0.16 1.03 0.14 0.241
Walkingspeed(m/s–1) 0.93 0.15 0.96 0.16 0.677
Cadence(step/min) 58.19 2.84 55.36 4.87 0.112
AnkletotalROM(◦) 25.37 3.94 23.27 3.62 0.182
KneetotalROM(◦) 54.35 4.09 49.93 3.30 0.107
KneeROM1(◦) 6.94 4.11 6.75 3.03 0.135
KneeROM2(◦) 9.23 4.57 6.99 3.22 0.164
HiptotalROM(◦) 26.45 6.55 24.41 3.14 0.306
PelvicrotationtotalROM(◦) 14.3 9.59 5.08 1.53 0.001a
PelvicobliquitytotalROM(◦) 4.71 1.59 6.29 2.86 0.125
Resultsofone-waymeasuresanalysisofvariancetest. BMI,BodyMassIndex;ROM,RangeofMotion;(◦),degrees.
a p<0.05.
ensembleaverageoftheankle,kneeandhipjoint displace-mentsofFMandELDarepresentonFig.2.
Therewerenegativecorrelationwithpelvicrotationand gluteuspain(r=-0.69;p<0.05),andbetweenpelvicobliquity andgreatertrochanterpain(r=-0.69;p<0.05)intheFM.No othersignificantcorrelationsweredetectedbetweentender pointsandkinematicparameters(p>0.05).
Discussion
Fibromyalgia is a chronic condition characterized by widespreadpain and muscle weakness,1 which may cause
changesingaittowardsanagingpattern.Themainfinding ofthe studywas thatwomenwithFMpresentedapattern whichresemblesthatgenerallyreportedintheelderly.
Walkingspeedhasbeenproposedasoneofthebest kine-maticfallpredictors.12,19,20 Ithasbeenproposedthatagait
speedreductionof0.1m.s–1 representsa10%decrement in theabilitytoperforminstrumentaldailylifeactivities.28The
kinematicanalysisshowedthatwomenwithFMinthisstudy exhibitedasimilarslowwalkingspeed(0.93m.s–1)toother studiesthathaveassessedwomenwithFM(from0.9to1.1 m.s–1)andperformedcomparisonswithacontrolgroup.9,10
ThesimilaritiesbetweenFMandELDinanumberof mea-suredgaitparametersfoundinthisstudyaresuggestivethat adeclineinmobilitymayoccurearlierinlifewithFMpatients. Therefore,theriskoffallmaybefurtherincreasedlaterinlife, whenthecumulativeeffectsofdegenerativeageingprocesses maysuperimpose theinfluenceofthe FMon gait parame-ters.Cadencewascomparablebetweengroupsandreinforces the ideathat gaitpattern in subjectswith FMdeteriorates earlierinlifewhenit iscomparedtohealthy age-matched individuals.9
Therefore,itisnotsurprisingthatreportsshowthatthe numberoffallsamongpatientswithFMisgreater than in
the elderly.17,21,22,29 Itcanbespeculatedthatsimilaritiesin
gait pattern (stride length, walking speed, hip, ankle and knee range of motion), between women with FM and the elderly,mayhaveoccurredduetopainduringtheeccentric phaseinthestance, whereinternalmuscle-tendontension isgreaterthaninotherconcentricphasesofthemovement. Paschalis et al.,15 reported significant reductions on knee
rangeofmotioninresponsetoinducedmusclepain. Inter-estingly,thecomparisonbetweenELDandFMgroupsshowed acomparablekneerangeofmotion,butwithaverydifferent patternfromnormativedatavaluesofhealthyage-matched subjects. For instance, normal subjects present a range of motionfrom20◦(ROM1)to15◦(ROM2),whileFMgroupshowed arange65.3%(ROM1)and38.5%(ROM2)smallerthanhealthy counterparts.30
Interestingly,differences between groupsin the present study did not occur around the knee, but around the hip jointandthepelvis.Thepelvisshowedagreaterrotationin women withFM incomparison tothe elderly. Other stud-ies have pointedout theimportance ofthe hip andpelvis ingaitperformance.13,31Pelvicrotationincrementcausesthe
swing segment to be placedadvanced furtherforwards in thegroundandincreasesthestridelength.13,32Consequently,
thegreaterpelvicrotationfoundinsubjectswith fibromyal-giamaybeviewedasastrategytoincreasestridelengthas acompensatorymechanismtosustainapattern.The find-ingsofPierrynowskietal.33corroboratewiththesearguments,
astheyhaveshownreduced anklepowersaccompaniedby increasedhippoweratpush-offphaseinwomenwithFM.
100 80
60 40 20
100 80 60 40 20
0 0 20 40 60 80 100
100 80 60 40 20 0 40
0 20 40 60
100 80 60 40 20 0
20 40 60
100 80 60 40 20 0 90 100 110
100 80 60 40 20 0 80 85 90 50
60 70 80 90
50 60 70 80 90 100
50 60 70 80 90 100
100 80 60 40 20 0 50
40 60 70 80
Ankle angle (
º)
Ankle angle (
º)
Knee angle (
º)
Hip angle (
º)
Hip angle (
º)
FM group ELD group
Pelvic rotation angle (
º)
Pelvic rotation angle (
º)
Percent of Gait Cycle
Percent of Gait Cycle Percent of Gait Cycle
Percent of Gait Cycle
Knee angle (
º)
Percent of Gait Cycle
Percent of Gait Cycle Percent of Gait Cycle
Percent of Gait Cycle
Figure2–Theensembleaverageoftheankle,kneeandhipjointdisplacementsandpelvicrotationofFibromyalgia(FM)
andElderlygroup(ELD).
bealsopossiblethatsubjectswithFMusemorepronounced actionsaroundthehipdespiteofthediscomfortcausedby theirchronicpaincondition.
Therefore,clinical symptomsmay notfully reflect com-pensatorystrategiesperformedtosustainacertainoutcome. AsproposedbyPierrynowskietal.,33itmaybeviewedasa
strategyoftheneuromuscularsystemthatreliesmoreinthe
proximalmusclesthanthe distalonesduringwalking.Itis likelythatstrategiesappliedaroundtheankleareimportant toreducetheimpactofpain-constrainedmovements.
ornotwomenwithFMpresentaprematurepattern,which resemblestheoneobservedintheelderly.Besides,the liter-atureshowthatwomenwithFMpresentadifferentpattern whencomparedtothecontrolgroup;9,10 (c)absenceofpain
assessment in the elderly group, which could interfere in theirgaitparameters,althoughtheydidnotreportthe pres-enceofapainthatcouldinfluencetheirgaitpattern.Finally, (d)theBMIofbothgroupswererelativelyhighanddeemed overweight/obese.Thus,gaitpatternmayhavealsosuffered influenceofbody mass, althoughgroups were paired with respecttoBMI.
Conclusion
Inconclusion,thegaitpatternofmiddle-agedwomenwith fibromyalgiawasfoundcomparabletotheonepresentedby elderlysubjects,whichraisesconcernsastheymaybe pre-maturely exposed to the adverse effects of the syndrome, whichincludesreducedmobilityandincreasedriskoffalls.It isfurtherconcerningthefactthatmiddle-agedwomenwith fibromyalgiaalreadypresentapatternsimilartotheelderly, whichisknownastobemorepronetofallsthanmiddle-aged counterparts.Laterinlife,therisk offallsinpatients with fibromyalgiacanbefurtherincreasedandmaycauseasevere impactonqualityoflife.Otherstudies,withlargersamplesize arerequiredtodeterminewhetherregularprogramsof physi-calactivitiesareeffectivetomodifygaitparametersinpatients withfibromyalgia.Itisalsonecessarytoanalyzethegait pat-ternand fallincidenceinelderly womenwithfibromyalgia usinglongitudinalapproaches.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
Theauthors wish toacknowledge the financialsupport of CAPES(Coordinationofimprovementforgraduated person-nel),anagencyoftheBrazilianGovernmentwhichallowed thetrainingandpreparationofhumanresources;alsotothe participantsandtheresearchteaminvolvedinthisstudy.
r
e
f
e
r
e
n
c
e
s
1. WolfeF,ClauwDJ,FitzcharlesMA,GoldenbergDL,KatzRS, MeaseP,etal.TheAmericanCollegeofRheumatology preliminarydiagnosticcriteriaforfibromyalgiaand measurementofsymptomseverity.ArthritisCareRes. 2010;62:600–10.
2. WolfeF,SmytheHA,YunusMB,BennettRM,BombardierC, GoldenbergDL,etal.,TheAmericanCollegeofRheumatology 1990.Criteriafortheclassificationoffibromyalgia.Reportof theMulticenterCriteriaCommittee.ArthritisRheum. 1990;33:160–72.
3. HomannD,StefanelloJM,GoesSM,LeiteN.Impaired functionalcapacityandexacerbationofpainandexertion duringthe6-minutewalktestinwomenwithfibromyalgia. RevBrasFisioter.2011;15:474–80.
4.MannerkorpiK,SvantessonU,BrobergC.Relationships betweenperformance-basedtestsandpatients’ratingsof activitylimitations,self-efficacy,andpaininfibromyalgia. ArchPhysMedRehabil.2006;87:259–64.
5.BaraniukJN,WhalenG,CunninghamJ,ClauwDJ.
Cerebrospinalfluidlevelsofopioidpeptidesinfibromyalgia andchroniclowbackpain.BMCMusculoskeletDisord. 2004;5:48.
6.JonesJ,RutledgeDN,JonesKD,MatallanaL,RooksDS. Self-AssessedPhysicalFunctionLevelsOfWomenwith Fibromyalgia.ANationalSurvey.Women’sHealthIssues. 2008;18:406–12.
7.KhanWLM.StudyingtheRiskofFallsinPatientswith Fibromyalgia.AdvanceforPhysicalTherapists.2006;17:10. 8.BennettRM,JonesJ,TurkDC,RussellIJ,MatallanaL.An
internetsurveyof2,596peoplewithfibromyalgia.BMC MusculoskeletDisord.2007:8.
9.HerediaJimenezJM,AparicioGarcia-MolinaVA,Porres FoulquieJM,DelgadoFernandezM,SotoHermosoVM. Spatial-temporalparametersofgaitinwomenwith fibromyalgia.ClinRheumatol.2009;28:595–8.
10.AuvinetB,BileckotR,AlixAS,ChaleilD,BarreyE.Gait disordersinpatientswithfibromyalgia.JointBoneSpine. 2006;73:543–6.
11.TiidusPM,PierrynowskiM,DawsonKA.Influenceof moderatetrainingongaitandworkcapacityoffibromyalgia patients:Apreliminaryfieldstudy.JSportsSciMed.2002;1: 122–7.
12.PerschLN,UgrinowitschC,PereiraG,RodackiAL.Strength trainingimprovesfall-relatedgaitkinematicsintheelderly:a randomizedcontrolledtrial.ClinBiomech(Bristol,Avon). 2009;24:819–25.
13.RodackiAL,SouzaRM,UgrinowitschC,CristopoliskiF,Fowler NE.Transienteffectsofstretchingexercisesongait
parametersofelderlywomen.ManTher.2009;14:167–72. 14.PavolMJ,PaiYC.Deficientlimbsupportisamajorcontributor
toagedifferencesinfalling.JBiomech.2007;40:1318–25. 15.PaschalisV,GiakasG,BaltzopoulosV,JamurtasAZ,Theoharis
V,KotzamanidisC,etal.Theeffectsofmuscledamage followingeccentricexerciseongaitbiomechanics.Gait Posture.2007;25:236–42.
16.BentoPCB,PereiraG,UgrinowitschC,RodackiALF.Peak torqueandrateoftorquedevelopmentinelderlywithand withoutfallhistory.ClinBiomech.2010;25:450–4.
17.GoesSM,LeiteN,ShayBL,HomannD,StefanelloJM,Rodacki AL.Functionalcapacity,musclestrengthandfallsinwomen withfibromyalgia.ClinBiomech(Bristol,Avon).2012. 18.GuimarãesJMN,FarinattiPdTV.Análisedescritivade
variáveisteoricamenteassociadasaoriscodequedasem mulheresidosas.RevBrasMedEsporte.2005;11:299–305. 19.CaoZB,MaedaA,ShimaN,KurataH,NishizonoH.Theeffect
ofa12-weekcombinedexerciseinterventionprogramon physicalperformanceandgaitkinematicsin
community-dwellingelderlywomen.JPhysiolAnthropol. 2007;26:325–32.
20.Montero-OdassoM,SchapiraM,SorianoER,VarelaM,Kaplan R,CameraLA,etal.Gaitvelocityasasinglepredictorof adverseeventsinhealthyseniorsaged75yearsandolder.J GerontolABiolSciMedSci.2005;60:1304–9.
21.RutledgeDN,CherryBJ,RoseDJ,RakovskiC,JonesCJ.Dofall predictorsinmiddleagedandolderadultspredictfallstatus inpersons50+withfibromyalgia?AnexploratorystudyRes NursHealth.2010;33:192–206.
22.RussekLN,FulkGD.Pilotstudyassessingbalanceinwomen withFibromyalgia.PhysiotherTheoryPract.2009;25:555–65. 23.PavolMJ,OwingsTM,FoleyKT,GrabinerMD.Influenceof
24.VoermansNC,SnijdersAH,SchoonY,BloemBR.Whyold peoplefall(andhowtostopthem).PractNeurol. 2007;7:158–71.
25.PardiniR,MatsudoS,AraújoT,MatsudoV,AndradeE, BraggionG,etal.Validac¸ãodoquestionáriointernacionalde níveldeatividadefísica(IPAQ-versão6):estudopilotoem adultosjovensbrasileiros.RBrasCieMov.2003;9:45–51. 26.ACSM.AmericanCollegeofSportsMedicine’sGuidelinesfor
ExerciseTestingandPrescription.8ed.Philadelphia,2010. 27.KerriganDC,Xenopoulos-OddssonA,SullivanMJ,LelasJJ,
RileyPO.Effectofahipflexor-Stretchingprogramongaitin theelderly.ArchPhysMedRehabil.2003;84:1–6.
28.LopopoloRB,GrecoM,SullivanD,CraikRL,MangioneKK. Effectoftherapeuticexerciseongaitspeedin
community-dwellingelderlypeople:Ameta-analysis.Phys Ther.2006;86:520–40.
29.JonesKD,HorakFB,Winters-StoneK,IrvineJM,BennettRM. Fibromyalgiaisassociatedwithimpairedbalanceandfalls.J ClinRheumatol.2009;15:16–21.
30.PerryJ,BurnfieldJM.GaitAnalysis:NormalandPathological Function.Thorofare:Slack.2010.
31.KerriganDC,LeeLW,CollinsJJ,RileyPO,LipsitzLA.Reduced hipextensionduringwalking:Healthyelderlyandfallers versusyoungadults.ArchPhysMedRehabil.2001;82: 26–30.
32.RoseJ,GambleJG.Humanwalking.Baltimore:Williams& Wilkins;2006.