w w w . r b o . o r g . b r
Original
article
Evaluation
of
the
quality
of
life
of
patients
undergoing
hemiarthroplasty
of
the
hip
夽
Eduardo
Lima
de
Abreu,
Medre
Henrique
Araújo
de
Oliveira
∗Fundac¸ãoHospitalAdrianoJorge,Manaus,AM,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received16August2014 Accepted11September2014 Availableonline20August2015
Keywords: Qualityoflife Hiparthroplasty Femoralneckfracture
a
b
s
t
r
a
c
t
Objective:Thiswasacomparativeanalysisonthequalityoflifeofpatientswhounderwent hemiarthroplastyofthehip,assessedbeforetheoperationand3and6monthsafterthe operation,bymeansoftheSF-36questionnaire(MedicalOutcomesStudy36-ItemShort Formhealthsurvey).
Methods:Aprospectivestudywasconductedon12patientswithfemoralneckfractures whounderwentpartialhiparthroplastybetweenJune2013andJuly2014.Femalepatients predominated(58.3%).Themeanagewas83yearsand,in91.7%,thefracturewasdueto fallingfromastandingposition.TheSF-36questionnairewasappliedbeforetheoperation and3and6monthsaftertheoperation.
Results:Withregardtophysicalhealth,thepatientspresentedlowscoresforfunctional capacityandphysicalaspects.Theyhadgoodscoresforthesubitemofgeneralstateand highscoresregardingpain.Vitality,socialaspectandmentalhealthhadmoderatescores andemotionalaspectshadalowscore.
Conclusion:Withthesampleanalyzedhere,wecansaythatthehiphemiarthroplasty proce-dureforcasesofunstablefemoralneckfractures,inpatientswithlowfunctionaldemands analyzedoverapostoperativeperiodof6months,doesindeedallowqualityoflifetobe maintained.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
Avaliac¸ão
da
qualidade
de
vida
dos
pacientes
submetidos
à
hemiartroplastia
do
quadril
Palavras-chave: Qualidadedevida Artroplastiadequadril Fraturadocolofemoral
r
e
s
u
m
o
Objetivo:Análisecomparativadaqualidadedevidadospacientessubmetidosà hemiartro-plastiadoquadril,nopré-operatório, comtrêse seismesesde operados, pormeiodo questionárioSF-36(MedicalOutcomesStudy36-Itemshortformhealthsurvey).
Métodos:Estudoprospectivoem12pacientescomfraturadocolodofêmur,submetidosà artroplastiaparcialdoquadril,dejunhode2013ajulhode2014.Houvepredomíniodosexo
夽
WorkperformedintheOrthopedicsandTraumatologyService,Fundac¸ãoHospitalAdrianoJorge,Manaus,AM,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](M.H.A.deOliveira). http://dx.doi.org/10.1016/j.rboe.2015.08.006
feminino,com58,3%.Amédiadeidadefoide83anoseem91,7%foidecorrentedequedada própriaaltura.ForamaplicadososquestionáriosSF-36nopré-operatórioetrêseseismeses dopós-operatório.
Resultados: Comrelac¸ãoàsaúdefísica,ospacientesapresentarambaixapontuac¸ãona capacidadefuncional e nosaspectosfísicos.Boapontuac¸ão nosubitem estadogeral e altapontuac¸ãonoquesitodor.Avitalidade,osaspectossociaiseasaúdementaltiveram pontuac¸õesmoderadaebaixanoquedizrespeitoaosaspectosemocionais.
Conclusão:Comaamostraanalisada,podemosdizerqueoprocedimentode hemiartroplas-tiadoquadril,nasfraturasdocolodofêmurinstáveis,empacientescombaixademanda funcionalanalisadosnoperíodopós-operatóriodeseismeses,permite,sim,amanutenc¸ão daqualidadedevida.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Theadvanceofmedicine,withregardtocontrollingsilent dis-eases,particularlycardiopulmonary,endocrineandvascular disorders,hasledtoimprovementsinpatients’conditionsand qualityoflife,thusalsoimprovingthepopulation’smeanlife expectancy.AccordingtotheBrazilianInstituteforGeography andStatistics(InstitutoBrasileirodeGeografiaeEstatística,IBGE), oneinevery10individualsis60yearsofageoroverandithas beenestimatedthat,by2050,thisratiowillhaverisentoone infiveworldwide.InBrazil,elderlyindividualscorresponded to8.6%ofthepopulationin2000andby2020theyareexpected tocorrespondto14%,i.e.around31millionpeople.1
Thisincrease in the population’s life expectancy brings along the problemsofthis age group, suchas fractures of the proximalfemur, and particularly ofthefemoral neck.2 HungriaNetoetal.1observedtheirprevalenceinindividuals withoneormoreassociatedcomorbidities.Femalepatients predominated(2:1),withameanageof78.2years.However, greaterriskwasassociatedespeciallywiththeagegroupof 81–85years,andthisappliedtobothmenandwomen.Men presentedslightlylowerprevalence(75.5years).
Theenergyofthistraumaistypicallylowandisrelatedto factorssuchasosteoporosis,malnutrition,decreased activi-tiesofdailyliving,diminishedvisualacuity,decreasedreflexes andweakenedmusculature.3–5
Porteretal.6demonstratedthatthemainfactorthatleads toanincreaseintheincidenceofthesefracturesabovethe age of60 years isthe presenceofosteoporosis, as well as greater incidenceoffalls.Approximately onethird of Cau-casianwomenabovetheageof65yearshaveosteoporosis7 and30%ofelderlywomenfallatleastonceayear.8Ithasbeen estimatedthatsixmillionindividualsworldwidewillsuffer fracturesoftheproximalfemureveryyearby2050.6
Treatment options include percutaneous fixation, open reduction, internal fixation and partial or total hip arthroplasty.9
Decisionsregardingtreatmentforfemoralneckfractures arecommonlybasedontwofactors.Thefirstisthepatient’s clinicalcondition,whichincludesage,levelofactivity,mental stateandcomorbiditiesthatmayinterfereinthesurgical pro-cedureand/orrehabilitation.Thesecondisthetypeoffracture
and,morespecifically,whetheritisstableorinstable. Physio-logicallyelderlypatientswithunstablefemoralneckfractures, who place lowdemandonthese structures,are treatedby meansofhiphemiarthroplasty.10
Some studies have correlated the results from treating femoralneck fracture withthe surgicaltechnique used.9,11 However,littlehasbeendescribedregardingthequalityoflife aftersurgeryofpatientswhounderwentsurgicaltreatment.12 Thepresent studyhad the mainobjective ofcomparing thequalityoflifeofpatientswhounderwenthip hemiarthro-plasty, bymeans ofthe SF-36questionnaireappliedbefore surgeryand3and6monthsaftertheprocedure.
Materials
and
methods
ThepresentstudywassubmittedtotheEthicsCommitteefor ResearchInvolvingHumanBeingsand wasapprovedunder
CAAENo.04298712.2.0000.0007.
Thepopulationstudiedwascomposedof12patientswho hadsufferedfemoralneckfractureandthenunderwent par-tialhiparthroplasty,betweenJune2013andJuly2014.
Their ages ranged from 72 to93 years,with amean of 83years.Fivepatients(41.7%)weremaleand seven(58.3%) female.
Theinclusioncriteriaamongtheseelderlypatientswere thattheyneededtohavearadiographicdiagnosisoffemoral neck fracture, underwent hip hemiarthroplasty and volun-tarilyagreedtoparticipateinthestudybysigningafreeand informedconsentstatement.
Patients who were notelderlyand elderly patientswho didnotacceptparticipationinthestudywereexcluded,along withpatientswhounderwenttreatmentwithmethodsother thanhiphemiarthroplasty.
Inthewalkingcapacityevaluation,thepatientswere clas-sifiedintofourgroups:communitywalker(patientabletowalk withinand outsideoftheirhome,but mayrequire a walk-ingaid);homewalker(patientabletowalkonlywithintheir home,usuallyrequiringawalkingaid);non-functionalwalker (patientwhoonlywalksduringphysiotherapysessions);and non-walker(patientunabletowalk).14
To evaluate quality of life, the SF-36 questionnaire (a genericquestionnairethatiseasilyadministeredand com-prehended)wasappliedbeforesurgeryand3and6months after the procedure. It is composed of 36 items that are encompassedineightscalesorcomponentswithnon-specific conceptsforagivenage,diseaseortreatmentgroup,andit allowscomparisonsbetweendifferentdisordersandbetween differenttreatments.15Itneedstobeemphasizedthatinthe presentstudy,the questionnairewas appliedwiththe pur-poseofascertainingthechanges(positiveornegative)from thebeginningtotheendoftheprogram.
Regardingthesurgicaltechnique,patientswerepositioned in lateral decubitus, and the procedure was carried out through the access route ofKocher and Langenbeck apud Letournel.16 After resection ofthe head of the femur, the wholefemoralneckalsounderwentresectionwiththeproper instrumentsand,then,thecementedunipolarprosthesiswas installed.
Regarding pain, the Sikorski and Barrington scale was used,17whichisaquestionnairethathasbeenvalidatedfor thePortugueselanguage.Thisscalewaschosenbecauseitis easytoapplyandcanbeansweredbythepatientandbytheir companions.Thisscale evaluatesthe presenceofpainand whetherthereisneedforanalgesicsandthefrequencyoftheir use.
AllthepatientswerereferredtotheHipGroupoutpatient serviceforperiodicfollow-upandradiographsofthepelvis wereobtainedinAPview.
Thevariables were tabulatedintheExcelsoftware. The data were analyzed descriptively and organized in tables andgraphs.Thequality-of-lifeevaluationwasperformedin accordancewiththeSF-36methodology.Comparisonofthe SF-36resultsfrombeforeandaftertheoperation(3months afterwards)wasdonebymeansoftheMann–Whitney non-parametrictest,sincetheresultsfromtheSF-36domainswere notconsideredtohavenormaldistribution.Thesignificance levelwastakentobe5%forallcomparisons.
Results
Samplecharacterization
Thesamplewascomposedof12patients:fivemen(41.7%)and sevenwomen(58.3%)(Fig.1).
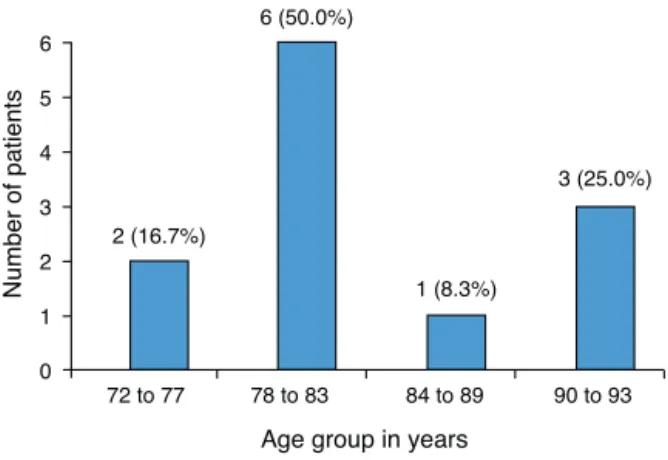
Theagesofthepatientsevaluatedrangedfrom72years (minimum)to93years(maximum),withameanof83±6years (Fig.2).
Clinicalfactors
Amongthepatientsevaluated,fallingfromastandingposition wasthemostfrequenttraumamechanismobserved:11ofthe
Female 58.3%
Male 41.7%
Fig.1–Distributionofthepatientsevaluatedaccordingto
sex.
12patients(91.7%)presentedthischaracteristic.Sevenofthe patients(58.3%)wereaffectedontheirright-handside.Seven (58.3%)alsopresentedalevelIIsurgicalrisk(Goldman)and six(50%)presentedalevelIVGardenclassification.Regarding classificationofwalkingabilities,six(50%)wereclassifiedas communitywalkersandsix(50%)ashomewalkers(Table1).
Regardingthepainanalysis,inaccordancewiththescale proposedbySikorskiandBarrington,17sevenpatients(58.3%) wereatgrade2,meaningthattheyfeltmoderateoccasional pain,whichdidnotrequireanalgesic(Fig.3).
A total of 16 comorbidities were observed among the patients.Themostfrequentwerehypertension(50%)and dia-betesmellitus(18.8%)(Fig.4).
Qualityoflifeofthepatients–SF36
Thisfactorwasassessedatthreetimes:beforesurgery (pre-operatively)and3and6monthsaftersurgery.
Incomparingthepreandpostoperativeanalyses,the high-estmeans(medians)amongthecomponentsevaluatedwere observed for pain and for physical, social and emotional aspects.Theseaspectsweremostaffectedamongthepatients whounderwenthiphemiarthroplasty(Table2).
Age group in years
Number of patients
72 to 77 2 (16.7%)
6 (50.0%)
1 (8.3%)
3 (25.0%)
0 1 2 3 4 5 6
78 to 83 84 to 89 90 to 93
Fig.2–Distributionofthepatientsevaluatedaccordingto
Table1–Clinicalcharacteristicsofthepatients evaluated.
Characteristics Frequency
n=12
%
Traumamechanism
Fallingfromstandingposition 11 91.7
Fallingfrom1meterheight 1 8.3
Sideaffected
Right 7 58.3
Left 5 41.7
Goldman(surgicalrisk)
I 1 8.3
II 7 58.3
III 4 33.3
Garden(classification)
I 1 8.3
III 5 41.7
IV 6 50.0
Walkingclassification
Communitywalker 6 50.0
Homewalker 6 50.0
Source:Presentauthor(2014).
Constant pain (grade 3)
8.3%
Moderate pain (grade 2)
58.3%
Absence of pain (grade 1)
33.3%
Fig.3–Painevaluationamongthepatients.
1 (6.3%) 1 (6.3%) 1 (6.3%)
2 (12.5%) 3 (18.8%)
8 (50.0%)
Frequency/%
0 Gastritis Hypothyroidism Parklnson Alzheimer Diabetes mellitus Hypertension
2 4 6 8 10
Fig.4–Frequencyofcomorbiditiesfoundamongthe
patients.
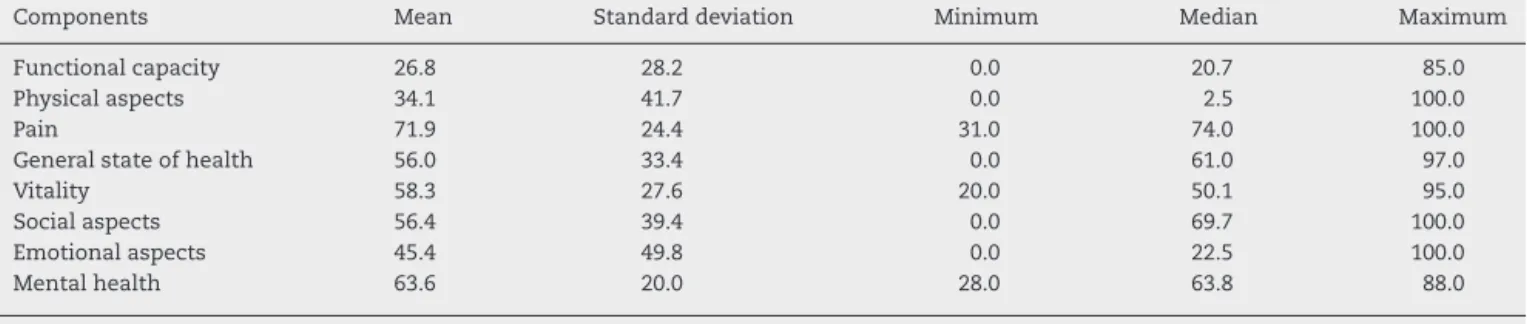
Three months after the surgery, the median level of pain was 74, which amounted to a 17.8% decrease in relation to the preoperative period. However, the physi-calaspects wereseverelyaffected (median=2.5).Thesame occurredwiththesocialaspects(median=69.7)andemotional aspects(median=22.5).Themostpositivecomponentwasthe decreaseinpain(Table3).
Over6months,thepatients’quality-of-lifestandardhardly underwentanyalterations.However,thecomponentsof vital-ity(median=57.6)andphysicalaspects(median=12.5)grew, respectively,by15%and400%from3to6months(Table4).
In comparing each component of the SF-36, significant changes were only observed regardingfunctional capacity, physicalaspects,painandemotionalaspects,withregardto changesfrombeforetheoperationto3monthsaftersurgery (Table5).
Thefunctionalcapacityofthepatientsbeforesurgerywas significantlydifferentfromtheircapacity3monthsafterwards (p=0.0464).Moreover,beforesurgerythiscapacitywas signif-icantlygreaterthanat3monthsafterwards(p=0.0232).
Regardingphysicalaspects,therewasstrongevidencethat, 3monthsaftersurgerythiscomponentwasgreatly compro-mised,givenitssignificantdecreaseaftersurgery(p=0.0083). There was a reasonable decrease in pain, meaning that there was evidence that surgery was what caused it (p=0.0499).
Table2–ValuesobtainedforeachcomponentoftheSF-36questionnairefromthepatientsevaluated,beforethe
operation.
Components Mean Standard
deviation
Minimum Median Maximum
Functionalcapacity 50.4 27.3 5.0 52.5 90.0
Physicalaspects 81.3 38.6 0.0 100.0 100.0
Pain 87.5 8.7 60.0 90.0 90.0
Generalstateofhealth 71.1 20.1 30.0 72.0 100.0
Vitality 68.3 25.7 15.0 75.0 95.0
Socialaspects 78.1 29.7 25.0 93.8 100.0
Emotionalaspects 83.3 38.9 0.0 100.0 100.0
Mentalhealth 71.3 22.7 20.0 76.0 96.0
Table3–ValuesobtainedforeachcomponentoftheSF-36questionnairefromthepatientsevaluated,3monthsafter surgery.
Components Mean Standarddeviation Minimum Median Maximum
Functionalcapacity 26.8 28.2 0.0 20.7 85.0
Physicalaspects 34.1 41.7 0.0 2.5 100.0
Pain 71.9 24.4 31.0 74.0 100.0
Generalstateofhealth 56.0 33.4 0.0 61.0 97.0
Vitality 58.3 27.6 20.0 50.1 95.0
Socialaspects 56.4 39.4 0.0 69.7 100.0
Emotionalaspects 45.4 49.8 0.0 22.5 100.0
Mentalhealth 63.6 20.0 28.0 63.8 88.0
Source:Presentauthor(2014).
Table4–ValuesobtainedforeachcomponentoftheSF-36questionnairefromthepatientsevaluated,6monthsafter
surgery.
Components Mean Standarddeviation Minimum Median Maximum
Functionalcapacity 26.8 28.2 0.0 20.7 85.0
Physicalaspects 34.1 41.7 0.0 12.5 100.0
Pain 71.1 24.9 31.0 74.0 100.0
Generalstateofhealth 56.4 35.5 0.0 56.0 97.0
Vitality 60.0 27.0 20.0 57.6 95.0
Socialaspects 56.4 39.4 0.0 69.7 100.0
Emotionalaspects 45.4 49.8 0.0 22.5 100.0
Mentalhealth 63.6 20.0 28.0 63.8 88.0
Source:Presentauthor(2014).
Table5–ComparisonbetweentheSF-36resultsfrombeforetheoperationand3monthsaftersurgery.
Components Median pvaluea pvalueb
Beforeoperation Threemonthsafterwards
Functionalcapacity 52.50 20.70 0.0464* 0.0232*
Physicalaspects 100.00 12.50 0.0166* 0.0083*
Pain 90.00 74.00 0.0999 0.0499*
Generalstateofhealth 72.00 61.00 0.2145 0.1072
Vitality 75.00 50.05 0.4357 0.2179
Socialaspects 93.75 69.70 0.119 0.0595
Emotionalaspects 100.00 22.50 0.0999 0.0499*
Mentalhealth 76.00 63.80 0.2366 0.1183
a Thepvalueofthedatainthepreoperativeperiod. b Thepvalueofthedataofthree-monthpostoperative.
∗ Mann–Whitneytest:thevaluesaresignificantforp<0.05.
Regardingemotionalaspects3monthsaftersurgery,there wasasignificantdecreaseinthiscomponent(p=0.0499).
Discussion
TheWorldHealthOrganizationclassifiesqualityoflifeasthe individualperceptionofcompletephysical,mentalandsocial wellbeing.However,thereisnowincreasinginterestamong doctorsandresearcherstowardtransformingqualityoflife intoaquantitativemeasurementthatcanbeusedinclinical trials.Resultsthus obtainedcouldbecomparedamong dif-ferentpopulationsandevenamongdifferentdiseases.Inan environmentwithlimitedresources,questionnaireresultsare particularlyimportantforcomparingthecost-benefit relation-shipsofmedicalinterventions.18
Therapidgrowth oftheelderly populationhasresulted inaproportional increaseinthenumberofelderly individ-ualswithchronicincapacityduringthisphaseoflife.Fallsare aseriouspublichealthissueamongtheelderly,becauseof theirfrequency,morbidityandhighsocioeconomicimpact.19 Themostfrequenttraumamechanismobservedamongthis sampleofpatientswasfallingfromastandingposition,which affected91.7%ofthecases.
the lower bone mineral density among females after the menopause.22
InastudyconductedinthecityofSãoPaulo,Onoetal.10 observedthatthemeanageofpatientswithfracturesofthe femoralneckwhounderwentpartialhiparthroplastywas83.1 years(range:58–99).Likeinthepresentstudy,Chikudeetal.12 reportedameanageof83yearsinananalysisonpatientswith fracturesofthefemoralneck.
Thefunctional capacity evaluation scale identifies both thepresenceand theextentoflimitationsregarding physi-calcapacity.Theevaluation scalesrelating tophysicaland emotional aspects address not onlythe limitations of the typeandamountofwork,butalsohowmuchthese limita-tions makethepatient’s work and activities ofdailyliving harder.Inthepresentstudy,fromtheperspectiveof physi-calhealth,lowfunctionalcapacitywasobservedamongthe patientsafter6monthsoffollow-up,withameanvalueof 26.8,althoughitisknownthatfunctionalcapacityamongthe elderlyisusuallylow.Thefearofanewfallwasseentobe directlyrelatedtorestrictionsondailyactivities,aspreviously observed by Luukinen et al.23 Regarding physical aspects, therewasanincreaseof15%between3and6monthsafter surgery.Although functional capacityand physical aspects werelow,thepatientsweresatisfiedwiththesurgical treat-ment.Thisfindingwasconfirmedbythevitalitycomponent, which showed a 400% increase from 3 to 6 months after surgery.Thus,performing hemiarthroplastyonfractures of thefemoralneckwasjustifiedforpatientswithlowfunctional demand,whichwasalsoobservedinthestudy byChikude etal.12
Inthepresentstudy,painduringthepostoperativeperiod wasinfrequent amongmost ofthe patientsevaluated and did not limit individuals regarding their daily activities. According to the scale of Sikorski and Barrington,17 one patient(8.3%)presentedintensepainandneededanalgesics, while91.6% either did notpresent pain or presented only moderatepainanddidnotneedanalgesics,whichwas con-firmedthrough the SF-36analysis (median of74) and was alsoobservedinother studies.10,12,24 Lowpresenceofpain is an important factor for good postoperative quality of life.
Furthermore,inthe itemofphysicalhealth,the general statepresentedasatisfactorymedian,ofcloseto61,which demonstratesthatthepartialhiparthroplastyprocedure con-tributedtowardincreasingthepatients’chancesofsurvival, aswellasallowingbetterqualityoflife.
Socialaspectsare consideredtobeasubitemofmental healthandpresentedhighscores,reachingamedianof69.70. Thisdemonstratedthatduringthepostoperativeperiod,the patientswereaidedbytheirrelatives,whichshowsthat sup-portandlivingtogetherwithfamilyandfriendsisimportant forthesepatients’recovery.
Regardingtheitemofemotionalaspects,thepatientsof the present study presented low scores, witha median of 22.50.Thisreflectsthateitherdepressionoranxietyoccurred atsomemomentduringthepostoperativeperiod.However, within mental health aspects, the patients were seen to presentgoodconditions,withamedianof63.80.Thisisan importantitem,becauseit directlyinterfereswithpatients’ self-esteem. It demonstrates that in addition to support
fromrelatives,multidisciplinaryfollow-upisoffundamental importance.
Thedatashowthatthesurgicalprocedureshouldnotbe the onlyconcern.Comprehensionamongrelativesand the attention from a multidisciplinary team are necessary for patientstohavegoodqualityoflife.
Onelimitationofthepresentstudywastheshortfollow-up time,aswellasthesmallsamplesize.Thiswasduetolossof patientswhocouldnotbelocatedlaterorwhodiedduringthe studyperiod.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.HungriaNetoJS,DiasCR,AlmeidaJDB.Característica epidemiológicasecausadasfraturasdoterc¸oproximaldo fêmuremidosos.RevBrasOrtop.2011;46(6):660–7. 2.AlfframPA.Anepidemiologicstudyofcervicaland
trochantericfracturesofthefemurintheurbanpopulation. ActaOrthopScand.1964;65Suppl.:1–109.
3.VilasBoasJuniorA,VercesiAE,BodachneL,VialleLR.Estudo epidemiológicodefraturasdefêmurproximalemidosos. ActaOrtopBras.1996;4(3):122–6.
4.KyleRF,CabanelaME,RussellTA,SwiontkowskiMF,Winquist RA,ZuckermanJD,etal.Fracturesoftheproximalpartofthe femur.InstrCourseLect.1995;44:227–53.
5.BroosPL,VanHaaftenKI,StappaertsKH,GruwezJA.Hip fracturesintheelderly.Mortality,functionalresultsand socialreadaptation.IntSurg.1989;74(3):191–4.
6.PorterRW,MillerCG,GraingerD,PalmerSB.Predictionofhip fractureinelderlywomen:aprospectivestudy.BMJ. 1990;301(6753):638–41.
7.GuarnieroR,OliveiraLG.Osteoporose:atualizac¸ãono diagnosticoeprincípiosbásicosparaotratamento.RevBras Ortop.2004;49(9):477–85.
8.CarvalhoMI.Osteoporose:visãodoortopedista.RevBras Ortop.2006;41(4):91–7.
9.MiyamotoRG,KaplanKM,LevineBR,EgolKA,ZuckermanJD. Surgicalman-agementofhipfractures:anevidence-based reviewoftheliterature.I.Femoralneckfractures.JAmAcad OrthopSurg.2008;16(10):596–607.
10.OnoNK,LimaGDA,HondaEK,PoleselloGC,GuimarãesRP, JúniorWR,etal.Artroplastiaparcialnotratamentodas fraturasdocolodofêmur.RevBrasOrtop.2010;45(4):382–8. 11.ThompsonRF.Vitalliumintramedullaryhipprosthesis:
preliminaryreport.NYStateJMed.1952;52(24):3011–20. 12.ChikudeT,FujikiEN,HondaEK,OnoNK,MilaniC.Avaliac¸ão
dequalidadedevidadospacientesidososcomfraturadocolo defêmurtratadoscirurgicamentepelaartroplastiaparcialdo quadril.ActaOrtopBras.2007;15(4):197–9.
13.GardenRS.Low-anglefixationinfracturesofthefemoral neck.JBoneJointSurgBr.1961;43:647–63.
14.HofferMM,FeiwellE,PerryR,PerryJ,BonnettC.Functional ambulationinpatientswithmyelomeningocele.JBoneJoint SurgAm.1973;55(1):137–48.
15.MartinezMC,Dissertac¸ãoAsrelac¸õesentreasatisfac¸ãocom aspectospsicossociaisnotrabalhoeasaúdedotrabalhador. SãoPaulo:FaculdadedeSaúdePúblicadaUniversidadede SãoPaulo;2002.
17.SikorskiJM,BarringtonR.Internalfixationversus
hemiarthroplastyforthedisplacedsubcapitalfractureofthe femur.Aprospectiverandomisedstudy.JBoneJointSurgBr. 1981;63(3):357–61.
18.WiklundI,RomanusB.Acomparisonofqualityoflifebefore andafterarthroplastyinpatientswhohadarthrosisofthe hipjoint.JBoneJointSurgAm.1991;73(5):765–9.
19.TinettiME,WilliamsTF,MayewskiR.Fallriskindexforelderly patientsbasedonnumberofchronicdisabilities.AmJMed. 1986;80(3):429–34.
20.ArlianiGG,AsturDC,LinharesGK,BalbachevskyD,Fernandes HJA,ReisFB.Correlac¸ãoentretempoparaotratamento cirúrgicoemortalidadeempacientesidososcomfraturada extremidadeproximaldofemur.RevBrasOrtop.
2011;46(2):189–94.
21.RochaMA,CarvalhoWS,ZanquetaC,LemosSC.Estudo epidemiológicoretrospectivodasfraturasdofêmurproximal tratadosnoHospitalEscoladaFaculdadedeMedicinado TriânguloMineiro.RevBrasOrtop.2001;36(8):311–6.
22.CummingsSR,KelseyJL,NevittMC,O’DowdKJ.Epidemiology ofosteoporosisandosteoporoticfractures.EpidemiolRev. 1985;7:178–208.
23.LuukinenH,KoskiK,LaippalaP,KivelaSL.Factorspredicting fracturesduringfallingimpactsamonghome-dwellingolder adults.JAmGeriatrSoc.1997;45(11):1302–9.