rev bras reumatol.2015;55(2):167–173
w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Review
article
Effects
of
muscle
stretching
exercises
in
the
treatment
of
fibromyalgia:
a
systematic
review
夽
Suélem
Barros
de
Lorena
∗,
Maria
do
Carmo
Correia
de
Lima,
Aline
Ranzolin,
Ângela
Luiza
Branco
Pinto
Duarte
UniversidadeFederaldePernambuco,Recife,PE,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received16March2014
Accepted17August2014
Availableonline6January2015
Keywords:
Fibromyalgia Stretching Physiotherapy
a
b
s
t
r
a
c
t
Objective:thisstudyhastheobjectivetosystematizescientificevidencesabouttheuseof
musclestretchingexercisesinthetreatmentofFM.
Methodology:itwasperformedfromretrospectiveresearchwithoutchronologicaland
lin-guisticlimits,atdatabasesofMEDLINE,LILACS,SciELOandPEDro,aswellasatPubMed
searchtool.DatacollectionwasperformedbytwoindependentreviewersinOctober2012,
withthesearchstrategyformulatedbycrossingdescriptorsandrelevanttermstothetopic
inEnglish,PortugueseandSpanishlanguages.Randomizedclinicaltrials,onlywithpatients
withaclinicaldiagnosisoffibromyalgiaandmusclestretchingexercisesasatherapeutic
measureatleastinoneoftheinterventiongroupswereincluded.Includedstudieswere
assessed formethodological qualityusingPEDroscaleandtheirreferences analyzedto
highlightadditionalsources.Thesearchamountedtoanaverageof6,794items.Onlyfive
articleswereselected,onebeingexcludedbecauseofitslowmethodologicalquality.Pain
wasassessedunanimously.Themethodandtimingofinterventionsvariedwidely,there
waspoormentionoftheparametersusedinthestretchesandabsenceofspecificphysical
examinations.
Results:therewassignificantimprovementinallstudiesregardingpain,besidesasrelated
toqualityoflifeandphysicalcondition.
Conclusion: itiscleartheimportanceofmusclestretchinginthetreatmentofFM,however,
thereisaneedforfurtherstudiestoestablishtherealbenefitsofthetechnique,because
themajorityofpublishedstudiesshowslowmethodologicalqualityandthereisalackof
standardizationregardingtheuseofthisresource.
©2014ElsevierEditoraLtda.Allrightsreserved.
夽
Institution:Post-GraduatePrograminHealthSciences,UniversidadeFederaldePernambuco,Recife,PE,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](S.B.d.Lorena).
http://dx.doi.org/10.1016/j.rbre.2014.08.014
168
rev bras reumatol.2015;55(2):167–173Efeitos
dos
exercícios
de
alongamento
muscular
no
tratamento
da
fibromialgia:
uma
revisão
sistemática
Palavras-chave:
Fibromialgia Alongamento Fisioterapia
r
e
s
u
m
o
Objetivo: opresentetrabalhotemcomoobjetivosistematizarevidênciascientíficassobrea
utilizac¸ãodosexercíciosdealongamentomuscularnotratamentodafibromialgia(FM).
Metodologia: foirealizadoapartirdeconsultaretrospectiva,semlimitecronológicoe
lin-guístico,àsbasesdedadosMedLine,LILACS,SciELOePEDro,alémdaferramentadebusca
PubMed.Acoletafoirealizadapordoisrevisoresindependentes,emoutubrode2012,sendo
aestratégiadebuscaformuladapormeiodocruzamentodedescritoresetermosrelevantes
paraotemanosidiomasinglês,portuguêseespanhol.Foramincluídosensaiosclínicos
randomizados(ECRs)compostosapenasporpacientescomdiagnósticoclínicodeFMecom
exercíciosdealongamentomuscularcomomedidaterapêuticaempelomenosumdos
gru-posdeintervenc¸ão.Osestudosincluídosforamavaliadosquantoàqualidademetodológica
pormeiodaescalaPEDro,esuasreferênciasbibliográficas,analisadas,parasedestacar
fontesadicionais.Abuscatotalizou6.794artigos.Cincoartigosforamselecionados,sendo
um delesexcluídoporapresentarbaixaqualidademetodológica.Ador foiavaliadapor
unanimidade.Ométodoeotempodasintervenc¸õesvariaramamplamente,houvefalta
demenc¸ãodeparâmetrosnautilizac¸ãodosalongamentoseausênciadeexamesfísicos
específicos.
Resultados: houvemelhorasignificativaemtodososestudosquantoàdor,alémdeaspectos
relacionadosaqualidadedevidaecondic¸ãofísica.
Conclusão:éevidenteaimportânciadoalongamentomuscularnotratamentodaFM,porém
observa-seanecessidadedenovosestudosparaseestabelecerosreaisbenefíciosdatécnica,
vistoqueamaioriadostrabalhospublicadosapresentabaixaqualidademetodológicae
ausênciadepadronizac¸ãoquantoaousodesserecurso.
©2014ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Fibromyalgia(FM)isarheumaticsyndromeofunknown
etiol-ogythatoccurspredominantlyinwomenaged30-55years.1
Itis characterizedbya chronic, widespread
musculoskele-talpain, withgreater than threemonthsduration,causing
physicalandemotionalproblemsinterferingdirectlyin
func-tional capacityand quality oflife.2 The diagnosis isbased
on the clinical condition of the patient,3 and the
treat-ment advocates pain control through global strategies of
an interdisciplinary approach, with interventions in
phys-ical,pharmacological, cognitive-behavioraland educational
spheres.1,4
Acting directly in the physical domain of FM patients,
physiotherapy,aprofessionalmodalityconsistingofan
arse-naloftechniquesresponsibleforbreakingtheviciouscycle
of symptoms characteristic of chronic patients, deserves
to be highlighted.4–6 Scientific evidence shows that
cine-siotherapeuticexercisesminimizepain,fatigueandmuscle
tension,improvinglevelsofstress,anxietyanddepressionin
fibromyalgiapatients,whenperformedonaregularbasisand
undermonitorization.7,8
Thestretchingexercises,inturn,allowfunctionalmuscle
lengthrecovery,providingstressrelief,posturalrealignment
andimprovementinamplitude,aswellasfreedomand
aware-nessofmovement.9,10However,althoughextensivelyusedin
physicaltherapyclinicalroutinebybeingeasytoperformand
tolerate,theredoesnotseemtoexist??aconsensusonthe
moresuitablestretchingtype,frequencyandintensityforthe
treatmentofpatientswithFM.4,7
Thus,theaimofthisarticleistosystematizethe
scien-tificevidenceontheuseofmusclestretchingexercisesinthe
treatmentofFM.
Material
and
methods
A systematic literature review was performed from a
ret-rospectiveconsultationwithnochronologicalandlinguistic
limits, to Literature Analysisand RetrievalMedical System
Online (MEDLINE), Latin American and Caribbean
Litera-tureonHealthSciences(LILACS),ScientificElectronicLibrary
Online(SciELO)andPhysiotherapyEvidenceDatabase(PEDro)
databases, aswell the search engine PubMed. Thepapers’
collection washeld inOctober2012, withthesearch
strat-egyformulatedbycrossingofdescriptors(DeCSandMmeSHs)
andtermsrelevanttothesubject(freeterms–FT),inEnglish,
PortugueseandSpanishidioms.
OnMedline,LILACS,SciELOandPEDro,thefollowing
cross-ings:“Fibromyalgia”(DeCS)AND“Stretching”(FT)OR“Muscle
stretching exercises” (DeCS)OR “Flexibility” (FT)OR
“phys-iotherapy “(DeCS) OR” Physical Therapy Modalities” (DeCS)
OR“Exercise”(TL)OR“Rehabilitation”(DeCS)were used.On
PubMed,thearticleswereobtainedfromthecrossingbetween
“Fibromyalgia” (MeSH) AND “Stretching” (FT) OR “Muscle
stretchingexercises”(MeSH)OR“Flexibility”(FT)OR“Range
rev bras reumatol.2015;55(2):167–173
169
“Physical Therapy Specialty” (MeSH) OR “Physical Therapy
Modalities”(MeSH)OR“Exercise[major]”(MeSH)OR
“Reha-bilitation”(MeSH).
RCTscomposedonlybypatientswithclinicaldiagnosisof
FMandpresentingmusclestretchingexercisesasa
therapeu-ticmeasureinatleastoneoftheinterventiongroupswere
included.Thesearchandselectionofarticles,aswellasthe
analysisofresults,werejudiciouslyperformedbytwo
inde-pendentreviewers. Initially, articleswere excluded bytitle,
followedbysummaryand,finally,byfullreadingofthestudy.
Thestudieswhichmettheinclusioncriteriawereassessed
formethodological qualityusingPEDroscale11,12 consisting
of10 questions about thestudy, withatotal scoreof 0-10
points.Surveyswith<3pointswereexcluded,forshowinglow
methodologicalqualityandwithfewpossibilitiesof
extrapo-latingtheirresultstoclinicalpractice.Thereferencesatthe
endofselectedarticleswere analyzedinordertohighlight
additionalsources.
Duetothesmallnumberofclinicaltrialsonthesubject
andthelargevariabilityamongtheproposedinterventions,
acriticalreviewanalysisofthecontents,withnopossibility
ofastatisticalanalysisbymeta-analysis,wasperformed.The
relevantinformationwaspresentedinthe formof
descrip-tivetables,consideringthefollowingvariables:year,country,
sample,evaluatedoutcomes/assessmenttools,
methodologi-caldesign,interventionandeffectsfound.
Results
Thesearch indatabasestotaled anaverage of6,794items,
withthelargestnumberofstudiesfoundthroughMEDLINE
viaBIREME(n=3,068)andPubMed(n=3,181).Accordingto
eli-gibilitycriteria,onlyfivearticleswereselected, andthatby
Bressanetal.(2008)13wasexcludedbecauseofitslow
method-ologicalquality(PEDroscale=2).Asafinalresult,fourarticles,
presentedinchronologicalorderinTable1and
methodologi-callyevaluatedaccordingtoTable2,wereanalyzed.
Discussion
Analyzing the results obtained by the search strategy, we
observedahigherconcentrationofstudiesinthe2000s;10,15,16
there is only one publication in the year 1986.14 It is
worthnotingthatallinvestigationswereconductedinNorth
American14,15 and South American countries,10,16 and the
pioneer14researchwaspublishedinCanada,thehostcountry
ofthe1stInternationalConferenceonHealthPromotion,also
heldintheyear198617fromthismeeting,discussionsabout
improvingqualityoflifeworldwidewereinitiated,duetothe
broadeningoftheconceptofhealthandtheidentificationof
anevergrowingagingpopulation.17,18
Giventhechanging epidemiologicalprofileofthe
popu-lation, anincreaseinthe prevalenceofchronicdiseases is
observed,resultinginaneedforresearchconsidering
ther-apeuticapproachesconsistentwiththenewreality.18In1990,
theAmericanCollegeofRheumatologypublisheddiagnostic
criteria forFM19 and strengthened researcheson the
syn-dromeintheAmericas,withtheconsolidationofgroupsof
researchersonthesubject,ascouldbeseeninthisreview,with
theselectionoftwoitemsdevelopedbythesameauthorsin
SãoPaulo,Brazil.10,16
OnlythestudiesofJonesetal.(2002)15andofBerssaneti&
Marques(2010)16describethecalculationofminimumsample
size,establishedwithbasisonthevariables“isokineticmuscle
strength”and“qualityoflife”,respectively.Therulesofwriting
andpublicationofRCTs,constituentsofCONSORT,highlight
theimportanceofdeterminingthesamplesizefor
extrapola-tionofresultsfound.20Therefore,inouranalysistherewasno
homogeneitywithrespecttothenumberofparticipants.
Incontrast,althoughthe authors havedefineddifferent
agegroupsintheinclusioncriteriaofvolunteers,themean
age ofthe samplesfrom analyzedstudiescorresponded to
the middle-aged population, which is consistent with the
literature.21–23 These samestudies pointtoahigh
percent-ageofwomenwithFM,21–23 afactalsonotedinthisreview,
inwhichmenwereincludedonlyinthestudyconductedby
McCain(1986),14probablyduetothelowmethodologicalrigor
requiredininterventionalresearchesdevelopedinthe1980s.
The variable “pain” was the onlyselected unanimously
fortheresearchers’hypothesistesting;however,inthestudy
publishedin198614thedolorimetrytesttoassesspain
thresh-old wasperformedinadifferentway,beingappliedinfive
specific points, because the diagnosis criteria for FMwere
establishedonlylater,inthe1990s.19 Therewasconsensus
ontheapplicationofFIQandSF-36questionnairesfor
assess-mentofsymptomsandqualityoflifeinfibromyalgiapatients;
both are validatedfor theBrazilian populationand exhibit
goodsensitivityandspecificity,beingreliableandreproducible
tools.24,25
Themanuscriptsrevealavarietyofphysicaltestsapplied,
withtheexceptionofMatsutanietal.(2007);16theseauthors,
faithful to their purposes, considered adequate to analyze
onlyvariablesofasubjectivecharacter.Amongtheflexibility
testschosen,Jonesetal.(2002)15werelimitedtothe
evalua-tionofupperlimbsthroughactivefunctionaltestsofinternal
andexternalshoulderrotators;Berssaneti&Marques(2010)16
electedthethirdfinger-floortest,26widelyusedinthe
evalu-ationofflexibilityoftheposteriormusclesofthetrunkand
lowerlimbs,butthatrequiresexperienceoftheevaluatorto
avoid compensationduring its execution, such asopening
thetibiotarsalangleordecreasinghipflexion.Constraintson
thechoiceofthetestemployedcanbeexplainedbylackof
physicalexaminationsspecificallyvalidatedforpatientswith
fibromyalgia.
Heterogeneityininterventiontimesandinthefrequencyof
sessions,aswellasintheintensityofexercise,wereobserved,
corroboratingpreviousfindings4,7whichreportedlackof
con-sensusregardingtheapplicationofthetherapeuticstretching
approachinpatients withFM.However,we emphasizethe
educationalcontributionsincorporatedinthemethodologies
ofthestudiesbyJonesetal.(2002),15Matsutanietal.(2007)16
andBerssaneti&Marques(2010),10highlightingtheneedfor
anawarenessofpatients,withtheaimtoincreasetheir
adher-encetothetreatment,andalsotoobtainsomeguarantee,to
theextentpossible,ofcontinuityoftherapy.
Asfortheresultsfound,astatisticallysignificant
improve-ment in almost all parameters evaluated by the analyzed
studies in this systematic review was observed. When
170
r
e
v
b
r
a
s
r
e
u
m
a
t
o
l
.
2
0
1
5;
5
5(2)
:167–173
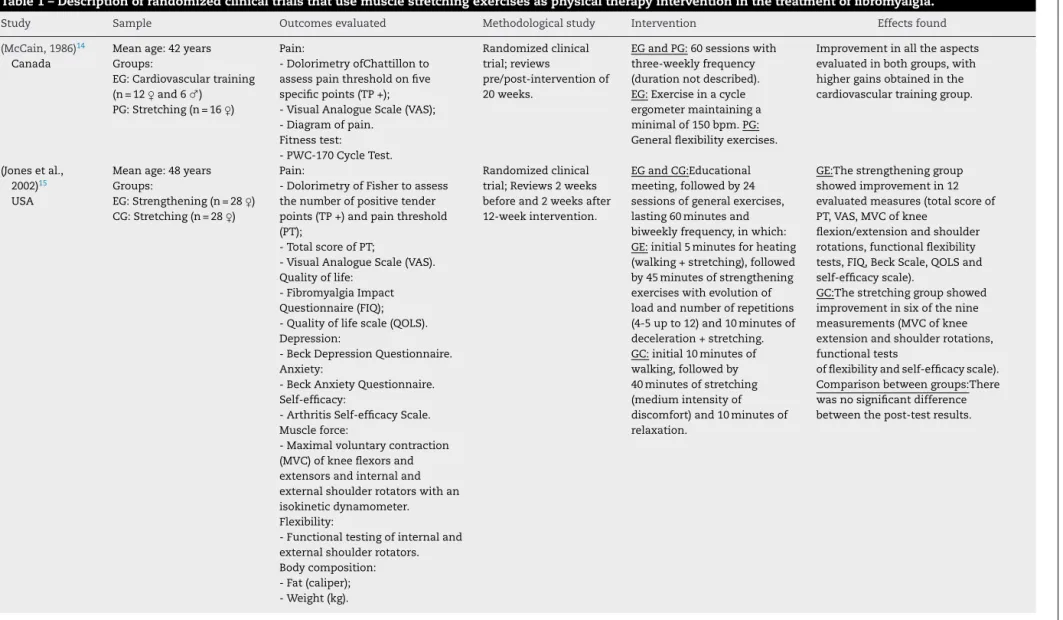
Table1–Descriptionofrandomizedclinicaltrialsthatusemusclestretchingexercisesasphysicaltherapyinterventioninthetreatmentoffibromyalgia.
Study Sample Outcomesevaluated Methodologicalstudy Intervention Effectsfound
(McCain,1986)14
Canada
Meanage:42years Groups:
EG:Cardiovasculartraining (n=12♀and6♂)
PG:Stretching(n=16♀)
Pain:
-DolorimetryofChattillonto assesspainthresholdonfive specificpoints(TP+); -VisualAnalogueScale(VAS); -Diagramofpain.
Fitnesstest: -PWC-170CycleTest.
Randomizedclinical trial;reviews
pre/post-interventionof 20weeks.
EGandPG:60sessionswith three-weeklyfrequency (durationnotdescribed). EG:Exerciseinacycle ergometermaintaininga minimalof150bpm.PG: Generalflexibilityexercises.
Improvementinalltheaspects evaluatedinbothgroups,with highergainsobtainedinthe cardiovasculartraininggroup.
(Jonesetal., 2002)15
USA
Meanage:48years Groups:
EG:Strengthening(n=28♀) CG:Stretching(n=28♀)
Pain:
-DolorimetryofFishertoassess thenumberofpositivetender points(TP+)andpainthreshold (PT);
-TotalscoreofPT;
-VisualAnalogueScale(VAS). Qualityoflife:
-FibromyalgiaImpact Questionnaire(FIQ); -Qualityoflifescale(QOLS). Depression:
-BeckDepressionQuestionnaire. Anxiety:
-BeckAnxietyQuestionnaire. Self-efficacy:
-ArthritisSelf-efficacyScale. Muscleforce:
-Maximalvoluntarycontraction (MVC)ofkneeflexorsand extensorsandinternaland externalshoulderrotatorswithan isokineticdynamometer. Flexibility:
-Functionaltestingofinternaland externalshoulderrotators. Bodycomposition: -Fat(caliper); -Weight(kg).
Randomizedclinical trial;Reviews2weeks beforeand2weeksafter 12-weekintervention.
EGandCG:Educational meeting,followedby24 sessionsofgeneralexercises, lasting60minutesand biweeklyfrequency,inwhich: GE:initial5minutesforheating (walking+stretching),followed by45minutesofstrengthening exerciseswithevolutionof loadandnumberofrepetitions (4-5upto12)and10minutesof deceleration+stretching. GC:initial10minutesof walking,followedby 40minutesofstretching (mediumintensityof discomfort)and10minutesof relaxation.
GE:Thestrengtheninggroup showedimprovementin12 evaluatedmeasures(totalscoreof PT,VAS,MVCofknee
flexion/extensionandshoulder rotations,functionalflexibility tests,FIQ,BeckScale,QOLSand self-efficacyscale).
GC:Thestretchinggroupshowed improvementinsixofthenine measurements(MVCofknee extensionandshoulderrotations, functionaltests
r
e
v
b
r
a
s
r
e
u
m
a
t
o
l
.
2
0
1
5;
5
5(2)
:167–173
171
–Table1(Continued)
Study Sample Outcomesevaluated Methodologicalstudy Intervention Effectsfound
(Matsutanietal., 2007)16
Brazil
Meanage:45years
Groups:
EG:Stretching/Laser(n=10 ♀)
CG:Stretching(n=10♀)
Pain:
-DolorimetryofFishertoassess thenumberofpositivetender pointspositive(TP+); -VisualAnalogueScale(VAS). Qualityoflife:
-FibromyalgiaImpact Questionnaire(FIQ);-SF-36.
Randomizedclinical trial;reviews pre/post-5-week intervention.
EGandCG: initialeducational guidelinesandin10treatment sessionslasting1hourand withbiweeklyfrequency. EG:Applicationoflaserin tenderpoints(3J/cm2,830nm, 30mW)andgeneralstretching exercises.
CG:generalstretching exercises.
Improvementinallaspects evaluated,withnodifference betweentheinterventiongroups.
(Berssaneti& Marques, 2010)10
Brazil
Meanage:46years Groups:
EG1:Stretching(n=14♀) EG2:Strengthening(n=16 ♀)
CG:Notreatment(n=14♀)
Pain:
-DolorimetryofFishertoassess painthresholdontenderpoints (PT)andnumberofpositivetender points(TP+);
-VisualAnalogueScale(VAS). Symptoms:
-FibromyalgiaImpact Questionnaire(FIQ). Qualityoflife: -SF-36. Flexibility:
-3rdfinger-floorTest(3FF). Muscleforce:
-Maximumvoluntaryisometric contraction(MVC)oftheknee flexorsandextensorswithload cell(EMGSystemofBrazil).
Randomizedclinical trial;reviews pre/post-12-week intervention.
GE:educationalguidelinesin 24generalexercisesessions, lasting40minutesand biweeklyfrequency,inwhich: EG1:initially3setsof
30seconds,increasingmonthly until5series;medium intensityofdiscomfort. EG2:1setof8repsinitially unloaded,withadditionof 0.5kgweekly,sincethepatient presentsBorgScale=13. CG:Patientrevisedafter12 weeks,withoutintervention.
SG1:Improvementinvariables:PT, 3FF,fatigue,sleep,stiffness,FIQ totalscore,functionalcapacity, vitality,mentalhealth,painand physicalandemotionaltotalsof SF-36.
EG2:Improvementinvariables:PT, TP+,3FF,MVCofkneeflexion, fatigue,sleep,stiffness,anxiety, depression,FIQtotalscore, functionalcapacity,vitality, mentalhealthandemotionaltotal ofSF-36.
GC:Noimprovement.
Comparisonbetweengroups:stretching andstrengtheningexercises
significantlyimprovepain,FM symptomsandqualityoflifeand canbeconsideredcomplementary, becausetheyactondifferent aspects.
172
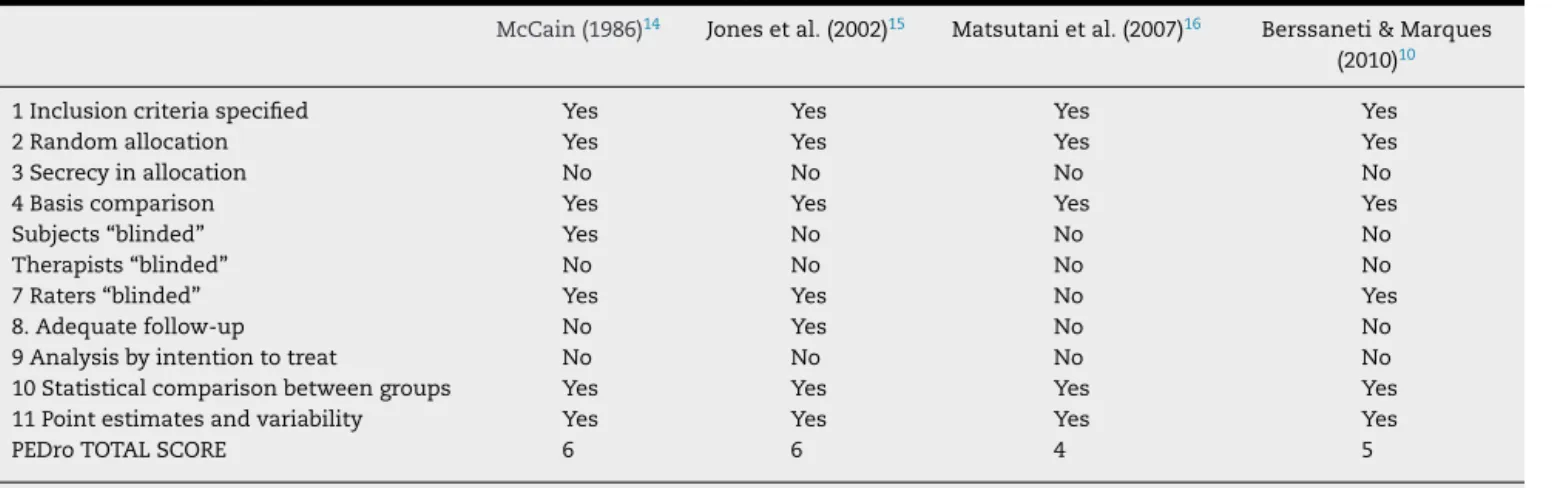
rev bras reumatol.2015;55(2):167–173Table2–MethodologicalclassificationofstudiesselectedbythePEDroScale.
McCain(1986)14 Jonesetal.(2002)15 Matsutanietal.(2007)16 Berssaneti&Marques
(2010)10
1Inclusioncriteriaspecified Yes Yes Yes Yes
2Randomallocation Yes Yes Yes Yes
3Secrecyinallocation No No No No
4Basiscomparison Yes Yes Yes Yes
Subjects“blinded” Yes No No No
Therapists“blinded” No No No No
7Raters“blinded” Yes Yes No Yes
8.Adequatefollow-up No Yes No No
9Analysisbyintentiontotreat No No No No
10Statisticalcomparisonbetweengroups Yes Yes Yes Yes
11Pointestimatesandvariability Yes Yes Yes Yes
PEDroTOTALSCORE 6 6 4 5
OBS.:Specificationoftheinclusioncriteria(item1)doesnotreceivePEDroscores.
exercisesinthestudiesbyJonesetal.(2002)15andBerssaneti&
Marques(2010),10orwiththeuseoflaserinaphototherapeutic
studybyMatsutanietal.(2007),16therewasnosuperiorityof
benefitsamongthetechniques,confirmingthatpatientswith
FMneednotonlyaninterdisciplinarytreatment,butalsoan
approachthatencompassesdifferentresourcesduringtheir
therapy.6,7,27
Conclusion
Giventheabove,itisevidenttheimportanceofconducting
therapeuticexercisesforphysicalandmentalimprovement
inpatientswithFM.However,wemustemphasizetheneed
forclinical trialswithgreater methodologicalrigorinorder
that,infact,therealbenefitsofphysiotherapyresourcesused,
especially those with muscle stretching exercises, become
known.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. SmithHS,HarrisR,ClauwD.Fibromyalgia:anafferent processingdisorderleadingtoacomplexpaingeneralized syndrome.PainPhysician.2011;14:E217–45.
2. CardosoFS,CurtoloM,NatourJ,LombardiJúniorI.Avaliac¸ão daqualidadedevida,forc¸amuscularecapacidadefuncional emmulherescomfibromialgia.RevBrasReumatol.
2011;51:338–50.
3. WolfeF,ClauwDJ,FitzcharlesMA,GoldenbergD,KatzRS, MeaseP,etal.TheAmericanCollegeofRheumatology PreliminaryDiagnosticCriteriaforFibromyalgiaand MeasurementofSymptomSeverity.ArthritisCare& Research.2010;62:600–10.
4. GürA.Physicaltherapymodalitiesinmanagementof fibromyalgia.CurrPharmDes.2006;12:29–35.
5. WinkelmannA,HäuserW,FriedelE,Moog-EganM,SeegerD, SettanM,etal.Physiotherapyandphysicalagenttherapies forfibromyalgiasyndrome.Systematicreview,meta-analysis andguidelines.DerSchmerz.2012;26:276–86.
6.MendesEV.Ocuidadodascondic¸õescrônicasnaatenc¸ão primáriaàsaúde:Oimperativodaconsolidac¸ãodaestratégia dasaúdedafamília.Brasília:Organizac¸ãoPan-Americanada Saúde;2012.
7.BuschAJ,BarberKA,OverendTJ,PelosoPM,SchachterCL. Exercisefortreatingfibromyalgiasyndrome.Cochrane DatabaseSystRev.2007;17:CD003786.
8.JonesKD,LiptanGL.ExercisesinterventioninFibromyalgia: clinicalapplicationsfromtheevidence.RheumDisClinNorth Am.2009;35:374–91.
9.AndersC,SprottH,ScholleHC,SurfaceEMG.ofthelumbar partoftheerectortruncimuscleinpatientswith
fibromyalgia.ClinExpRheumatol.2001;19:453–5.
10.BerssanetiAA.Exercíciosdealongamentoefortalecimento muscularnotratamentodepacientescomfibromialgia:um ensaioclínicorandomizado[tesededoutorado].SãoPaulo: UniversidadedeSãoPaulo,FaculdadedeMedicina;2010.
11.MaherCG,SherringtonC,HerbertRD,MoseleyAM,ElkinsM. ReliabilityofthePEDroScaleforRatingQualityof
RandomizedControlledTrials.PhysicalTherapy. 2003;83:713–21.
12.MortonNA.ThePEDroScaleisavalidmeasureofthe methodologicalqualityofclinicaltrials:ademographicstudy. AustralianJournalofPhysiotherapy.2009;55:129–33.
13.BressanLR,MatsutaniLA,Assumpc¸ãoA,MarquesAP,Cabral CM.Efeitosdoalongamentomuscularecondicionamento físiconotratamentofisioterápicodepacientescom Fibromialgia.RevBrasFisioter.2008;12:88–93.
14.McCainGA.RoleofPhysicalFitnessTraininginthe Fibrositis/FibromyalgiaSyndrome.JAMA.1986;81 Suppl3A:73–7.
15.JonesKD,BurckhardtCS,ClarkSR,BennettRM,PotempaKM. Arandomizedcontrolledtrialofmusclestrengtheningversus flexibilitytraininginfibromyalgia.JRheumatol.2002;29, 1041:8.
16.MatsutaniLA,MarquesAP,FerreiraEAG,Assumpc¸ãoA,Lage LV,CasarottoRA,etal.Effectivenessofmusclestretching exerciseswithandwithoutlasertherapyattenderpointsfor patientswithfibromyalgia.ClinExpRheumatol.
2007;25:410–5.
17.MinistériodaSaúde(Brasil),SecretariadePolíticasdeSaúde. ProjetoPromoc¸ãodaSaúde.AsCartasdaPromoc¸ãodaSaúde. Brasília:MinistériodaSaúde;2002.p.56.
18.WorldHealthOrganization.Envelhecimentoativo:uma políticadesaúde.Brasília:Organizac¸ãoPan-Americanada Saúde;2005.p.60.
rev bras reumatol.2015;55(2):167–173
173
1990CriteriafortheClassificationofFibromyalgia.Reportof theMulticenterCriteriaCommittee.ArthritisRheum. 1990;33:160–72.
20.SchulzKF,AltmanDG,MoherD,ConsortGroup.CONSORT 2010Statement:updatedguidelinesforreportingparallel grouprandomisedtrials.BMCMedicine.2010;8:18.
21.WolfeF,RossK,AndersonJ,RussellJ,HerbertL.The prevalenceandcharacteristicsofFibromyalgiainthegeneral population.ArthritisRheum.1995;38:19–28.
22.WhiteKP,SpeenchleyM,HarthM,OstbyeT.Comparing self-reportedfunctionandworkdisabilityin100community casesoffibromyalgiasyndromeversuscontrolsinLondon. OntarioArthritisRheum.1999;42:76–83.
23.Assumpc¸ãoA,CavalcanteAB,CapelaCE,SauerJF,ChalotSD, PereiraCA,etal.Prevalenceoffibromyalgiainalow
socioeconomicstatuspopulation.BMCMusculoskeletDisord. 2009;10:64.
24.MarquesAP,SantosAMB,Assumpc¸ãoA,MatsutaniLA,Lage LV,PereiraCA.Validac¸ãodaversãobrasileiradoFibromyalgia ImpactQuestionnaire(FIQ).RevBrasReumatol.2006;46: 24–31.
25.CiconelliRM,FerrazMB,SantosW,MeinãoL,QuaresmaMR. Traduc¸ãoparaalínguaportuguesaevalidac¸ãodo
questionáriogenéricodeavaliac¸ãodequalidadedevida SF-36(BrasilSF-36).RevBrasReumatol.1999;39:143–50.
26.PerretC,PoiraudeauS,FermanianJ,ColauMM,Benhamou MA,RevelM.Validity,reliability,andresponsivenessofthe fingertip-to-floortest.ArchPhysMedRehabil.
2001;82:1566–70.