w w w . r b o . o r g . b r
Original
article
Correlation
between
anthropometric
data
and
length
and
thickness
of
the
tendons
of
the
semitendinosus
and
gracilis
muscles
used
for
grafts
in
reconstruction
of
the
anterior
cruciate
ligament
夽
Rafael
Noschang
Pereira
∗,
Francisco
Consoli
Karam,
Roberto
Luís
Schwanke,
Rubens
Millman,
Zilmar
Minetto
Foletto,
Carla
Helena
Augustin
Schwanke
PontifíciaUniversidadeCatólicadoRioGrandedoSul(PUC-RS),PortoAlegre,RS,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received1September2014 Accepted5May2015
Availableonline9February2016
Keywords:
Anteriorcruciateligament Anthropometry
Transplantationautologous Tendons
a
b
s
t
r
a
c
t
Objective:Preoperativeestimationofthelengthanddiameterofthesemitendinosus(ST) andgracilis(G)tendonscanassistsurgeonsandallowthemtohavetheopportunityto choosealternativegrafts.Theaimofthisstudywastoinvestigatewhetheranthropometric measurementssuchasheight,weightandbodymassindex(BMI)orthepatient’sageand sexhaveanycorrelationwiththethicknessandthelengthofSTandGtendons.
Methods:Dataweregatheredfrom64patientswhounderwentthesurgicalprocedureof anteriorcruciateligamentreconstructionusingthetendonsoftheSTandGmusclesas grafts,betweenJune2012andAugust2013.Variablessuchasage,sex,weight,height,body massindex(BMI)andlengthanddiameterofthetendonsoftheSTandGmuscleswere analyzed.
Results:There wasa positivecorrelation betweenthe heightand totaldiameter ofthe quadruplegraft(r=0.254;p=0.043),totallengthoftheSTtendon(r=0.450;p<0.01),diameter ofthedoubleST(r=0.270;p=0.031),tripleST(r=0.347;p=0.005),lengthofGtendon(r=0.249;
p=0.047)anddiameterofthedouble-G(r=0.258;p=0.039).However,age(r=-0.015;p=0.908), weight(r=0.165;p=0.193)andbodymassindex(r=0.012;p=0.926)showednocorrelation.
Conclusion: Ourresultsshowthatage,weightandBMIdidnotcorrelatewiththediameter andlengthofthegraft,whiletheheighthadapositivecorrelationwiththetotallengthof theflexortendonsandthediameterofthegraftfromtheflexors(STandG).
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
夽
WorkperformedatHospitalSãoLucas,PontifíciaUniversidadeCatólicadoRioGrandedoSul(PUC-RS),HospitalMãedeDeusand HospitalDivinaProvidência,PortoAlegre,RS,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](R.N.Pereira).
http://dx.doi.org/10.1016/j.rboe.2016.01.011
Correlac¸ão
entre
dados
antropométricos
e
comprimento
e
espessura
dos
tendões
dos
músculos
semitendinoso
e
grácil
usados
como
enxerto
na
reconstruc¸ão
do
ligamento
cruzado
anterior
Palavras-chave:
Ligamentocruzadoanterior Antropometria
Transplanteautólogo Tendões
r
e
s
u
m
o
Objetivo:Aestimativapré-operatóriadocomprimentoedodiâmetrodostendões semitendi-noso(ST)egrácil(G)podeauxiliarepermitirqueoscirurgiõestenhamaoportunidadede escolheropc¸õesdeenxerto.Oobjetivodesteestudofoipesquisarseexistecorrelac¸ãoentre asmedidasantropométricas,comoaltura,peso,índicedemassacorpórea(IMC),idadee sexodopaciente,comaespessuraeocomprimentodostendõesSTeG.
Métodos:Entrejunhode2012eagostode2013,foramcoletadososdadosde64pacientesque sesubmeteramaoprocedimentocirúrgicodereconstruc¸ãodoligamentocruzadoanterior emqueseusaramcomoenxertoostendõesdosmúsculosSTeG.Foramanalisadasvariáveis comoidade,sexo,peso,alturaeíndicedemassacorporal(IMC),comprimentoediâmetro dostendõesdosmúsculosSTeG.
Resultados: Houveumacorrelac¸ãopositivaentrealturaediâmetrototaldoenxertode quá-druplo(r=0,254p=0,043),comprimentototaldotendãoST(r=0,450,p<0,01),diâmetrodo STduplo(r=0,270p=0,031),STtriplo(r=0,347p=0,005),comprimentodotendãoG(r=0,249 p=0,047)ediâmetrodoGduplo(r=0,258p=0,039).Noentanto,idade(r=-0,015p=0,908), peso(r=0,165p=0,193)eíndicedemassacorporal(r=0,012p=0,926)nãoapresentaram correlac¸ão.
Conclusão:Nossosresultadosmostramqueidade,pesoeIMCnãosecorrelacionaramcomo diâmetroecomprimentodoenxerto,enquantoaalturatinhaumacorrelac¸ãopositivacom ocomprimentototaldostendõesflexoresecomodiâmetrodoenxertodosflexores(STeG). ©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Thegrowing trendtoward practicing sports,together with greatercomplexityofsportsmovementshasincreasinglybeen causingknee jointinjuriestoappear.Theanteriorcruciate ligament(ACL)isamongmostcommonlyaffectedligaments, and surgical treatment is chosen for most patients who presentpainandinstability.1Theautologousgraftsmost
fre-quentlyusedinACLreconstructionsarethepatellar,gracilis (G),semitendinosus(ST)andquadricepstendons.Each tech-niquehas its adherents and indications,and selecting the graftdependsonmanyfactors,includingthesurgeon’s pref-erenceandthepatient’sageandlevelofactivity.Thesurgical techniqueusingthetendonsoftheSTandGmusclesasgrafts presentsresults thatare similartothose from thepatellar tendontechniqueandenablesmootherandlesspainful reha-bilitation.Themaindisadvantagesofthistechniqueinclude theindividualvariabilityinlengthandthicknessofthegraft fromthetendonsandthepotentialcomplicationsduringgraft harvesting.2–5Afterthetendonshavebeenremovedfromthe
semitendinosusandgracilismuscles,andbeforethegrafthas beenconstructed,surgeonsarefacedwithmanypossibilities forthefinalconfigurationofthegraft.Theseincludeusingthe semitendinosustendonindouble,triple orquadruple form alone,orindoubleforminassociationwiththetendonofthe gracilismuscle,alsoindoubleform(thusmakingaquadruple graft),orevenothercombinations.Preoperativeestimationof thelengthanddiameteroftheSTandGtendonsmayhelpand allowsurgeonstohavetheopportunitytochooseanothergraft
optionifthetendonthatmightbeharvesteddoesnotmeet theneedsofagivenpatient.However,nomethodcapableof preciselydeterminingthelengthanddiameterofSTandG tendonsbeforeACLreconstructionsurgeryisperformedhas yetbeendescribedintheliterature.
The objective of this study was to investigate whether anthropometricmeasurementssuchasthepatient’sheight, weight,bodymassindex(BMI),ageandsexwouldhaveany correlation withthe thicknessandlengthofthehamstring tendons(STandG).
Materials
and
methods
consentstatementwereexcludedfromthesample.Thestudy wasconductedamongpatientswhowereevaluatedthrough anamnesis, physical examination and magnetic resonance imaging,andforwhomtherewasanindicationforsurgical reconstruction ofthe ACL inwhich the ST and G tendons wereusedtoconstructthegraft.Thisinvestigationdidnot changetheroutineofstepstobefollowedduringthesurgical procedureindicated.Thedata-gatheringdidnotaddriskto theprocedure.Thisstudywasapprovedbyouruniversityand bytheresearchethicscommitteesoftheinstitutionsinvolved. Thefollowingvariables were analyzed:age, sex,weight, height,bodymassindex(BMI), lengthofthetendonofthe semitendinosusmuscle,lengthofthetendonofthegracilis muscle,diameterofthetendonofthesemitendinosus mus-clewhen folded inthe middle (double) and in threeparts (triple),diameterofthetendonofthegracilismusclewhen foldedinthemiddle(double)andthediameterofthetendons ofthesemitendinosusandgracilismuscleswhenfoldedinthe middleandgrouped(quadruple).
Firstly,demographicdata(ageandsex)and anthropomet-ricinformation(weightand height)reported atthe timeof thesurgerywereobtainedandnotedinthemedicalfile.Soon afterwards,duringthesurgicalprocedure,measurementson thetendonsofthesemitendinosusandgracilismusclesthat wereusedforconstructingthegraftsweremade.
The technique for obtaining the grafts during the ACL reconstructionsurgeryconsistedofanobliqueanteromedial incisionintheproximaltibia,attheleveloftheinsertionof theSTandGmuscles.Following this,thetendonoftheST musclewasdissectedand wasthen deinsertedagainstthe boneandremovedusingagraftextractor.Thesame proce-durewas repeatedin relationtothe tendonofthe gracilis muscle.Afterthetendonshadbeenpreparedthroughremoval ofthe musclelayer, the length(cm)and diameter (MM)of thegraftswereobtainedusingarulerandmeasuring cylin-derthathadpreviouslybeensterilized.Thediametersofthe semitendinosusandgracilisgraftsweremeasuredusingaset ofcylindrical tubesrangingindimensionfrom6to12mm, instepsof0.5mmbetween cylinders.Both ofthe tendons weremeasured.Inthecaseofthetendonderivedfromthe semitendinosusmuscle,its totallengthand diameterwere measured twice. Firstly, it was folded in the middle (dou-ble)andthenitwasfoldedintothreeparts(triple).Thetotal lengthand diameter ofthe graft derived from the gracilis muscleweremeasuredwiththetendonfoldedinthemiddle (double).Lastly,thelengthanddiameterofthetwotendons foldedinthemiddleandgroupedtogether(quadruple)were measured.Themeasurementsweremadewithoutsuturing thread,whichmighthavehinderedobtainingthereal dimen-sionsofthetendons(Figs.1and2).
Thedatagatheredwereanalyzedthroughdescriptiveand analytical statistics. IN the descriptive phase, means and standarddeviationswereused.Inthe analyticalphase,the variableswerecomparedinrelationtothedifferentlengths anddiametersofthetendonsofthesemitendinosusand gra-cilismuscles.Thettestforindependentsampleswasused toidentifydifferencesintheclinicalandintraoperative vari-ables.Pearson’scorrelation coefficient(r)andsimplelinear regressionwereusedtodeterminetherelationshipbetween theresultvariables(diameterofthequadruplegraftandthe
Fig.1–Removalofflexortendons.
lengthsofthesemitendinosusandgracilistendons)andthe predictivevariables(age,sex,height,weightandBMI). Differ-enceswereconsideredtobesignificantwhenPvalueswere lessthan0.05.TheanalysiswasdoneusingtheSPSSsoftware, version17.0.
Results
Among the 64 individuals analyzed between June 2012 and August 2013, 60 (94%) were male and four (6%) were female.Thepatients’meanagewas31.78±8.26years(range: 15–48 years); among the females, it was 32±13.49 years,
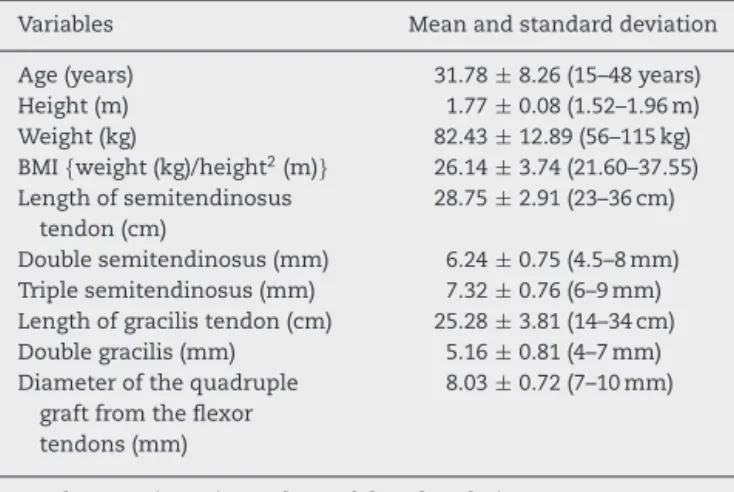
Table1–Resultsfrommeasurementsonanthropometric data.
Variables Meanandstandarddeviation
Age(years) 31.78±8.26(15–48years)
Height(m) 1.77±0.08(1.52–1.96m)
Weight(kg) 82.43±12.89(56–115kg)
BMI{weight(kg)/height2(m)} 26.14±3.74(21.60–37.55)
Lengthofsemitendinosus tendon(cm)
28.75±2.91(23–36cm)
Doublesemitendinosus(mm) 6.24±0.75(4.5–8mm) Triplesemitendinosus(mm) 7.32±0.76(6–9mm) Lengthofgracilistendon(cm) 25.28±3.81(14–34cm) Doublegracilis(mm) 5.16±0.81(4–7mm) Diameterofthequadruple
graftfromtheflexor tendons(mm)
8.03±0.72(7–10mm)
Total=64patients(60malesandfourfemales).
and amongthemales,it was 31.76±7.97 years.Themean heightwas1.77±0.08cm(range:1.52–1.96cm);meanweight 82.43±12.89kg(range:56–115kg);andmeanBMI26.14±3.74 (range: 21.60–37.55). The mean tendon lengths measured duringthe operationwere28.75±2.91cm(range: 23–36cm) forthesemitendinosusand25.28±3.81cm(range:14–34cm) forthe gracilis.Themeans tendon thicknesses(diameters) were6.24±0.75mm(range: 4.5–8mm)forthedouble semi-tendinosus; 7.32±0.76mm (range: 6–9mm) for the triple semitendinosus;and6.24±0.75mm(range:4.5–8mm)forthe doublegracilis.Themeantotaldiameterofthequadruple ten-dongraft (STand G) was 8.03±0.72mm(range: 7–10mm). During the study period, wedid notobtain any quadruple flexorgraftssmallerthan7mmorlargerthan10mm(Table1). Intotal,75% ofthe patientshad quadrupleflexorgrafts ofdiameter7–8mm,while25%ofthegraftswerelargerthan
0
14
2
32
15
1 0
5 10 15 20 25 30 35
10 9
8 7.5 7
6
Number of occurrences
Diameters of quadruple grafts from flexors (mm)
Distribution of the diameters of quadruple grafts from flexors
Fig.3–Distributionofthediametersofquadruplegrafts
fromflexors.
8mm. Thefrequenciesofdifferentdiameters ofquadruple flexorgraftswereasfollows:7mm(22%),7.5mm(3%),8mm (50%),9mm(23.5%)and10mm(1.5%)(Fig.3).
Therewerepositivecorrelationsbetweenheightandthe totaldiameterofthequadruplegraftfromtheflexortendons (r=0.254; p=0.043);totallengthofthe semitendinosus ten-don(r=0.450;p<0.01);diameterofthedoublesemitendinosus (r=0.270; p=0.031); diameter of the triple semitendinosus (r=0.347;p=0.005);totallengthofthegracilistendon(r=0.249;
p=0.047); and diameter of the double gracilis (r=0.258;
p=0.039).However,age(r=−0.015;p=0.908),weight(r=0.165;
p=0.193) and body mass index (r=0.012; p=0.926) did not presentanycorrelationwiththetotaldiameterofthe quadru-plegraftorwiththelengthsofthesemitendinosusandgracilis tendons(Table2).
Table2–Correlationofthedimensionsofthegracilisandsemitendinosustendonswithanthropometricvariablesand age.
Tendons Age(years) Weight(kg) Height(m) BMI(kg/m2)
r p
r p
r p
r p
Totallengthofgracilis(cm) 0.064 0.221 0.249 0.076
0.613 0.079 0.047a 0.550
Doublegracilis(mm) −0.141 0.233 0.258a 0.101
0.265 0.063 0.039 0.427
Totallengthofsemitendinosus(cm) 0.171 0.214 0.450 −0.063
0.177 0.089 0.000a 0.621
Doublesemitendinosus(mm) −0.054 0.256a 0.270a 0.116
0.671 0.041 0.031 0.361
Triplesemitendinosus(mm) 0.132 0.176 0.347a −0.030
0.300 0.164 0.005 0.812
Thicknessofquadruplegraft(mm) −0.015 0.165 0.254 0.012
0.908 0.193 0.043a 0.926
Discussion
Useofflexortendongraftshasbecomeanincreasinglypopular choiceamongorthopedicsurgeonsforACLreconstructions.6
Anatomicalstudieshavedemonstratedthatthemean diam-eterofthenormalACLisapproximately11mm,witharange from 6 to 12mm. Although the parameters foracceptable graftsizethat are necessaryinordertoachieve a satisfac-toryresult after ACL reconstruction have not been clearly defined,adiameterofatleast7mmhastraditionallybeen recommended.7–9 However,in a recent study, greater
inci-denceofACLreconstruction failurewasshown withgrafts smallerthan8mm.10Studiesonanimalmodelsthatevaluated
theinfluenceofgraftdiameteron graftstrength and resis-tancehavedemonstratedthatingraftssmallerthan8mm, failuredue totearingofthetendon materialoccurs,while in grafts larger than 10mm, failure occurs at the fixation screws,duetotraction.11Thus,acapacitytopredictwhich
patientspresentgreaterriskofhavinghamstringtendonsof insufficientdiameter,beforetheoperation,maybebeneficial forsurgicalplanning,therebyavoidingdisagreeable intercur-rencesduringtheoperation.7–10
Inourpatients,weusedavarietyofgraft combinations, suchastripleSTalone,quadrupleSTalone,doubleSTwith doubleG,tripleSTwithdoubleGandtripleSTwithtripleG. Theaimwasalwaystoseekgraftsofdiametergreaterthan 8mm,ofadequatelength.
Thecapacitytopredictthediameterandlengthofthegraft maybeusefulforcertainsurgicaltechniquesandmay pro-videoptionsforthesurgeon.Throughabiomechanicalstudy, Hamneretal.12 demonstrated thatthe resistance,stiffness
andbiomechanicalpropertiesofthegrafttendonareaffected byitsdiameter.However,theresultsfromthefewstudiesin theliteraturecorrelatingpatients’anthropometricdatawith thelengthanddiameterofflexorgraftscontinuetobe contra-dictory.
Inourstudy,weinvestigatedthepredictivevalueofsimple anthropometricmeasurementssuchasheight,weight, BMI andageinrelationtothelengthsofthesemitendinosusand gracilisflexortendonsandthediameterofthequadruplegraft fromtheflexors.Ourresultsshowedthatage,weightandBMI didnotcorrelatewiththelengthordiameterofthegraft,while heighthadapositivecorrelationwiththetotallengthofthe graftsfromthesemitendinosus(r=0.450;p<0.01)andgracilis (r=0.249;p=0.047),andalsowiththediameterofthe quadru-plegraftfromtheflexors(r=0.254;p=0.043).Adeeperanalysis using step-by-stepregression revealed that heightwas the clinicalparameterofgreatestimportanceforpredictingthe thicknessofthegraft.
Tumanetal.13analyzed106patientswhounderwentACL
reconstructionandreportedthatamongtheanthropometric dataanalyzedintheirstudy,suchasheight,weight,sexand age,heightwasthebestpredictorforthediameterofgrafts fromthehamstringsinbothsexes,andparticularlyamong women.Fromtheiranalysis,theyconcludedthatwomen pre-sentedgraft diametersthat were significantlysmallerthan thoseofmen,andthatinpatientswhoseheightwaslessthan 147cm,itwaslikelythatthegraftwouldbeinsufficient,with adiameteroflessthan7mm.
Maetal.14 retrospectivelyanalyzedpreoperative
anthro-pometricdatafrom536patients. Theirresultsshowedthat heightandsexweresignificantpredictorsforthediameterof flexortendongrafts.Malepatientshadgraftsthatwere signif-icantlylargerthanthoseoffemales.Itwasalsodemonstrated thatheightwasaspecificindicatorsolelyforthemen,without anysignificantresultsforthewomen.
Inastudyon119patientswhounderwentACL reconstruc-tion,Schwartzberget al.15reportedthattherewasastrong
correlation betweenleglengthand thelengthoftheflexor tendonsusedasgrafts(r=0.73;p<0.001).Inthesamestudy, weight(r=0.51;p<0.001)andleglength(r=0.42;p<0.001)only showed moderate correlations withgraft diameter.All the other correlationswere weakin relationto height.Weight measurementsandagedidnotshowanyrelationshipwiththe lengthanddiameteroftheflexortendons,andthesefindings were concordantwiththeresultsreportedbySchwartzberg etal.15
InanalysesbyTremeetal.16onthelengthanddiameterof
thesemitendinosusandgracilistendonsof50patientswho underwentACLreconstruction,astrongcorrelationwasfound betweenthelengthofthegraftandthepatient’sheightand lower-limblength.Thediameterofthegraft wascorrelated withthepatient’sweightandthighcircumference.
Althoughourstudy didnotconfirmall thepositive cor-relationsofotherstudies,12–17 ourresultsfavoredthenotion
thatindividualanthropometricvariablessuchasheightmay bepredictorsforthelengthanddiameteroftheflexortendons (STandG)thatareusedinACLreconstruction.Ourresultsalso showedthatheighthadapositivecorrelationwiththetotal lengthofthesemitendinosusandgracilistendonsandwith thediametersofdoubleST,tripleST,doubleGand quadru-plegrafts,andtheywerealsoconcordantwiththefindingsof Tumanetal.13Moreover,ourresultsdemonstratedthatheight
wasthemostimportantvariable,especiallyamongwomen, whereasSchwatzberg etal.15 foundthatheighthadaweak
correlationwiththighdiameterand thatweightand lower-limbdiameterhadamoderatecorrelationwithgraftdiameter. Thereislimitedevidenceintheliteraturecorrelatingthe patient’sfitnessandphysicalactivitylevelwiththelengthand diameteroftheflexortendons.Tremeetal.16reportedthat
theyhadnotfoundanycorrelationbetweenthediameterof theflexorgraftsandthepatient’ssportsandactivitylevels. SimilarresultswererecordedbyPichleretal.17intheirstudy
oncadavers.
Other studies in the literature have used radiological imaging examinations such as computed tomography and magneticresonanceimaging(MRI)inanattempttopredict thelengthanddiameterofflexorgraftsbeforetheoperation. Althoughsomestudieshaveshowngoodcorrelationsbetween measurementsofcross-sectionalareaandtendonthickness, othershavenotshownanycorrelation.18–20Nevertheless,the
lackofstandardizationinrelationtothelevelatwhich mea-surementsaremadeandregardingthetrustworthinessand precisionofthe examinationsgivesrisetolimitations that make the results obtainedquestionable. Yasumoto et al.19
Hamadaetal.20showedthatMRIwasimpracticalfor
evalu-atingthesizesofthetendons,giventhatalongsweeptime wouldbeneededandthecostishigh.
Conclusion
Thecapacitytopreciselypredictthelengthanddiameterof thehamstringtendons(STandG)usedinACLreconstructions continuestobeanimportantfactorindecision-makingandin choosingthebestsurgicaltechniqueandtheappropriategraft. Ourresultsshowedthatage,weightandBMIdidnotcorrelate withthediameterandlengthofthegraft,whileheightshowed apositivecorrelationwiththetotallengthoftheflexor ten-donsandwiththediameterofthegraftfromtheflexors(ST andG).
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
SpecialthankstothephysiciansLuizAntonioSilveiraSimões PiresandGuilhermeIslerPereira,whocontributedequallyto data-gatheringandconductingthisstudy.
r
e
f
e
r
e
n
c
e
s
1. DunnWR,LymanS,LincolnAE,AmorosoPJ,WickiewiczT, MarxRG.Theeffectofanteriorcruciateligament
reconstructionontheriskofkneereinjury.AmJSportsMed. 2004;32(8):1906–14.
2. ProdromosCC,HanYS,KellerBL,BolyardRJ.Stabilityresults ofhamstringanteriorcruciateligamentreconstructionat 2-to8-yearfollow-up.Arthroscopy.2005;21(2):138–46.
3. BiauDJ,TournouxC,KatsahianS,SchranzPJ,NizardRS. Bone-patellartendon-boneautograftsversushamstring autograftsforreconstructionofanteriorcruciateligament: meta-analysis.BMJ.2006;332(7548):995–1001.
4. AgliettiP,GironF,BuzziR,BiddauF,SassoF.Anteriorcruciate ligamentreconstruction:bone-patellartendon-bone comparedwithdoublesemitendinosusandgracilistendon grafts.Aprospective,randomizedclinicaltrial.JBoneJoint SurgAm.2004;86-A(10):2143–55.
5. FuFH,BennettCH,LattermannC,MaCB.Currenttrendsin anteriorcruciateligamentreconstruction.Part1:biologyand biomechanicsofreconstruction.AmJSportsMed.
1999;27(6):821–30.
6. GianottiSM,MarshallSW,HumePA,BuntL.Incidenceof anteriorcruciateligamentinjuryandotherkneeligament injuries:anationalpopulation-basedstudy.JSciMedSport. 2009;12(6):622–7.
7.HamadaM,ShinoK,HoribeS,MitsuokaT,ToritsukaY, NakamuraN.Changesincross-sectionalareaofhamstring anteriorcruciateligamentgraftsasafunctionoftime followingtransplantation.Arthroscopy.2005;21(8): 917–22.
8.GroodES,Walz-HasselfeldKA,HoldenJP,NoyesFR,LevyMS, ButlerDL,etal.Thecorrelationbetweenanterior–posterior translationandcross-sectionalareaofanteriorcruciate ligamentreconstructions.JOrthopRes.1992;10(6):878–85.
9.ScottWN,InsallJN.Injuriesoftheknee.In:RockwoodDPJr, GreenDP,BucholzRW,editors.RockwoodandGreen’s fracturesinadults.Philadelphia:LippincottWilliams& Wilkins;1996.p.1799–816.
10.MagnussenRA,LawrenceJT,WestRL,TothAP,TaylorDC, GarrettWE.Graftsizeandpatientagearepredictorsofearly revisionafteranteriorcruciateligamentreconstructionwith hamstringautograft.Arthroscopy.2012;28(4):526–31.
11.TeliM,ChiodiniF,SottocasaR,VillaT.Influenceofthe diametersoftendongraftandbonetunnelinhamstringACL reconstruction.Abovinemodel.ChirOrganiMov.
2005;90(3):281–5.
12.HamnerDL,BrownCH,SteinerME,HeckerAT,HayesWC. Hamstringtendongraftsforreconstructionoftheanterior cruciateligament:biomechanicalevaluationofthemultiple strandsandtensioningtechniques.JBoneJointSurgAm. 1999;81(4):549–57.
13.TumanJM,DiduchDR,RubinoLJ,BaumfeldJA,NguyenHS, HartJM.Predictorsforhamstringgraftdiameterinanterior cruciateligamentreconstruction.AmJSportsMed. 2007;35(11):1945–9.
14.MaCB,KeifaE,DunnW,FuFH,HarnerCD.Canpre-operative measurespredictquadruplehamstringgraftdiameter?Knee. 2010;17(1):81–3.
15.SchwartzbergR,BurkhartB,LariviereC.Predictionof hamstringtendonautograftdiameterandlengthforanterior cruciateligamentreconstruction.AmJOrthop(BelleMead NJ).2008;37(3):157–9.
16.TremeG,DiduchDR,BillanteMJ,MillerMD,HartJM. Hamstringgraftsizeprediction:aprospectiveclinical evaluation.AmJSportsMed.2008;36(11):2204–9.
17.PichlerW,TeschNP,SchwantzerG,FronhöferG,BoldinC, HausleitnerL,etal.Differencesinlengthandcross-sectionof semitendinosusandgracilistendonsandtheireffecton anteriorcruciateligamentreconstruction:acadaverstudy.J BoneJointSurgBr.2008;90(4):516–9.
18.WerneckeG,HarrisIA,HouangMT,SeetoBG,ChenDB, MacDessiSJ.Usingmagneticresonanceimagingtopredict adequategraftdiametersforautologoushamstring double-bundleanteriorcruciateligamentreconstruction. Arthroscopy.2011;27(8):1055–9.
19.YasumotoM,DeieM,SunagawaT,AdachiN,KobayashiK, OchiM.Predictivevalueofpreoperative3-dimensional computertomographymeasurementofsemitendinosus tendonharvestedforanteriorcruciateligament reconstruction.Arthroscopy.2006;22(3):259–64.