JPediatr(RioJ).2017;93(6):576---584
www.jped.com.br
ORIGINAL
ARTICLE
Early
neonatal
deaths
associated
with
perinatal
asphyxia
in
infants
≥
2500
g
in
Brazil
夽
,
夽夽
Maria
Fernanda
Branco
de
Almeida
a,
Mandira
Daripa
Kawakami
a,
Lícia
Maria
Oliveira
Moreira
b,
Rosa
Maria
Vaz
dos
Santos
c,
Lêni
Márcia
Anchieta
d,
Ruth
Guinsburg
a,∗aUniversidadeFederaldeSãoPaulo(UNIFESP),EscolaPaulistadeMedicina,DepartamentodePediatria,SãoPaulo,SP,Brazil bUniversidadeFederaldaBahia(UFBA),DepartamentodePediatria,Salvador,BA,Brazil
cUniversidadeFederaldoRioGrandedoNorte(UFRN),DepartamentodePediatria,Natal,RN,Brazil dUniversidadeFederaldeMinasGerais(UFMG),DepartamentodePediatria,BeloHorizonte,MG,Brazil
Received1July2016;accepted30November2016 Availableonline19March2017
KEYWORDS
Asphyxia neonatorum; Earlyneonatal mortality;
Meconiumaspiration syndrome;
Infant; Newborn; Brazil
Abstract
Objective: Toassess the annual burden ofearly neonataldeaths associated with perinatal
asphyxiaininfantsweighing≥2500ginBrazilfrom2005to2010.
Methods: Thepopulationstudyenrolledalllivebirthsofinfantswithbirthweight≥2500gand
withoutmalformations whodiedup tosixdays after birthwithperinatalasphyxia, defined asintrauterinehypoxia, asphyxiaat birth,ormeconium aspirationsyndrome.The causeof deathwaswritteninanyfieldofthedeathcertificate,accordingtoInternationalClassification
ofDiseases,10thRevision(P20.0,P21.0, andP24.0).An activesearchwasperformedin27
Brazilianfederativeunits.Thechi-squaredtestfortrendwasappliedtoanalyzeearlyneonatal mortalityratiosassociatedwithperinatalasphyxiabystudyyear.
Results: A total of10,675 infants weighing ≥2500g without malformations died within six
daysafter birthwithperinatalasphyxia. Deathsoccurred inthefirst 24hafter birthin71% ofthe infants.Meconiumaspiration syndromewas reportedin4076(38%) ofthese deaths. Theasphyxia-specificearlyneonatalmortalityratiodecreasedfrom0.81in2005to0.65per
1000livebirthsin2010inBrazil(p<0.001);themeconiumaspirationsyndrome-specificearly
neonatalmortalityratioremainedbetween0.20and0.29per1000livebirthsduringthestudy period.
夽
Pleasecitethisarticleas:AlmeidaMF,KawakamiMD,MoreiraLM,SantosRM,AnchietaLM,GuinsburgR.Earlyneonataldeathsassociated withperinatalasphyxiaininfants≥2500ginBrazil.JPediatr(RioJ).2017;93:576---84.
夽夽
StudyconductedatSociedadeBrasileiradePediatria,ProgramadeReanimac¸ãoNeonatal,SãoPaulo,SP,Brazil. ∗Correspondingauthor.
E-mail:[email protected](R.Guinsburg).
http://dx.doi.org/10.1016/j.jped.2016.11.008
0021-7557/©2017SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-ND
Conclusions: DespitethedecreasingratesinBrazilfrom2005to2010,earlyneonatalmortality ratesassociatedwithperinatalasphyxiaininfantsinthebetterspectrumofbirthweightand withoutcongenital malformations arestill high,andmeconiumaspirationsyndromeplays a majorrole.
©2017SociedadeBrasileiradePediatria.PublishedbyElsevierEditoraLtda.Thisisanopen accessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/ 4.0/).
PALAVRAS-CHAVE
Asfixianeonatal; Mortalidadeneonatal precoce;
Síndromede aspirac¸ãode mecônio; Neonato; Recém-nascido; Brasil
Óbitosneonataisprecocesassociadosàasfixiaperinatalemneonatos≥2.500g noBrasil
Resumo
Objetivo: Avaliarataxaanualdeóbitosneonataisprecocesassociadosàasfixiaperinatalem
neonatosdepeso≥2.500gnoBrasilde2005a2010.
Métodos: Apopulac¸ãodoestudoenvolveutodososnascidosvivosdeneonatoscompesoao
nascer≥2.500gesemmalformac¸õesquemorreramatéseisdiasapósonascimentoporasfixia perinatal,definidacomohipóxiaintrauterina,asfixianonascimentoousíndromedeaspirac¸ão demecônio.A causadoóbitofoiescritaemqualquerlinhadoatestado deóbito,deacordo comaClassificac¸ãoInternacionaldeDoenc¸as,10aRevisão(P20.0,P21.0eP24.0).Foifeitauma
pesquisaativaem27unidadesfederativasbrasileiras.OtesteQui-quadradodetendênciafoi aplicadoparaanalisarosíndicesdemortalidadeneonatalassociadosaasfixiaperinatalatéo anodoestudo.
Resultados: Umtotal de10.675neonatoscompeso≥2.500gsemmalformac¸ões morreuaté
0-6diasapósonascimentoporasfixiaperinatal.Osóbitosocorreramnasprimeiras24horas apósonascimentoem71%dosneonatos.Asíndromedeaspirac¸ãodemecôniofoirelatadaem 4.076 (38%)dosóbitos.Oíndicedemortalidadeneonatalprecocerelacionadaàasfixiacaiu de0,81em2005para0,65por1.000nascidosvivosem2010noBrasil(p<0,001);oíndicede mortalidadeneonatalprecocerelacionadaasíndromedeaspirac¸ãodemecôniopermaneceu entre0,20-0,29por1.000nascidosvivosduranteoperíododoestudo.
Conclusões: Apesar dareduc¸ãonastaxasnoBrasil de2005a2010,astaxasdemortalidade
neonatalprecoceassociadas àasfixiaperinatalemneonatosnomelhorespectrodepesoao nasceresemmalformac¸õescongênitasaindasãoaltas,easíndromedeaspirac¸ãodemecônio desempenhaumimportantepapel.
©2017SociedadeBrasileiradePediatria.PublicadoporElsevierEditoraLtda.Este ´eumartigo OpenAccesssobumalicenc¸aCCBY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4. 0/).
Introduction
Recently,thedeathsofchildrenyoungerthan5yearsofage havedecreaseddramatically,with3.6millionfewerdeaths in 2013when comparedwith2000.1 This reductionis pri-marilyattributedtoprogressin preventionandtreatment ofinfectiousdiseasesinpost-neonatalinfantsandchildren aged1---4 years.2 Withthis decrease ininfections, neona-tal conditionshave gained prominence.In 1990, neonatal deathsaccounted for 37.4% of deathsin children younger than 5 years of age, compared with 41.6% in 2013.3 The three leading causes of the 2.9 million annual neonatal deathsworldwidearepretermbirthcomplications(1.0 mil-lion), intrapartum conditions(0.7 million), and infections (0.6 million). Intrapartum-related conditions and preterm birthdominateintheearlyneonatalperiod.4
In 2013, the Maternal and Child Epidemiology Esti-mation Group reported that intrapartum-related events accounted for 24% of neonatal deaths in the world.1 Two-thirds of these deaths occured in South Asia and Africa.5 High-income countries have a low incidence of
asphyxia-relateddeaths,atapproximately12%.6Conversely, around 740,000---1,480,000 yearly neonatal deaths world-wideoccuramonginfantswithbirthweight≥2500g;in low-andmiddle-incomecountries,mostofthesedeathsare asso-ciatedwithintrapartumasphyxia.7
578 AlmeidaMFetal.
Terminfantshavethelowestriskofneonatalandinfant mortality.In11countriesofWesternEurope,theinfant mor-talityratesforthoseborn≥37weeksgestationwerebelow 2.0per 1000live birthsin 2010.11 The neonatalmortality rate for infants with a birth weight≥2500g in 2010 was 0.73per1000livebirthsintheUnitedStates12 and2.63in Brazil.10Theburdenofintrapartum-relatedconditions asso-ciatedwiththishighneonatalmortalityrateinnon-lowbirth weightinfantsinBrazilhasnotbeenwellevaluated.
The present study assessed the yearly burden and the primaryepidemiologicalcharacteristicsofearlydeaths asso-ciatedwithperinatalasphyxiaofinfantswithbirthweight ≥2500g without congenital malformations in Brazil from 2005 to 2010, considering the presence of intrauterine hypoxia,birthasphyxia,or meconiumaspirationsyndrome inanyfieldofthedeathcertificates.
Methods
Thiswasapopulation-basedstudyofalllivebirthsweighing
≥2500gwithout congenital malformations,whodied with
birthasphyxiaupto168hafterbirthfromJanuary1,2005 toDecember31,2010inBrazil.Theprojectwasapprovedby theResearchEthicsCommitteeoftheUniversidadeFederal deSãoPaulo,whichwastheleadingcenterforthisproject. Ineachofthe27statesofBrazil,twoinvestigatorsmade anactivesearchofallneonateswhohaddiedwithinthefirst weekafterbirth.Bothinvestigatorswerethelocal coordi-natorsoftheNeonatalResuscitationProgramoftheBrazilian PediatricSociety.Theoriginaldeathcertificatesand/orthe electronicfileswereobtainedat theStateHealth Depart-mentsof26statesandfromtheStateDataAnalysisSystem Foundation(Fundac¸ãoSistemaEstadualdeAnálisedeDados) forthestateofSãoPaulo.
The deaths associated with the presence of perinatal asphyxiaincludedinthestudywerereportedinanyfieldof thedeathcertificateasanyofthefollowingcauses, accord-ing to the International Classification of Diseases, 10th Revision(ICD10):P20.0−intrauterinehypoxiafirstnoted
before the onset of labor; P20.1 − intrauterine hypoxia
first noted during labor and delivery; P20.9 −
intrauter-ine hypoxia, unspecified; P21.0 − severe birth asphyxia;
P21.1--- mild andmoderate birth asphyxia; P21.9− birth
asphyxia, unspecified; or P24.0 − neonatal aspiration of
meconium.13 This study did not include deaths caused by neonatal aspiration of secretions other than meco-nium, deaths described as neonatal cerebral depression, orfetaldeaths.Allnewbornswithacongenital malforma-tion reported in any field of the death certificate were excluded.
Twoindependentprofessionalsenteredthedataforeach deathintoanelectronicfilethatwasspecificallycreatedfor thestudy.Therecordedvariablesextractedfromthedeath certificates were:date andtime of birth and death; city andstatewherethemotherlivedandwherethebabydied; placewheretheneonatedied(hospital,otherhealth facil-ity,home,street);maternalage,yearsofschooling(none, 1---3, 4---7, 8---11, ≥12) and place of work (home, outside home);numberofpreviousbirths;weeksofgestation(<22, 22---27,28---31,32---36,37---41,≥42);singleormultiple gesta-tion;cesareansectionorvaginaldelivery;birthweight(g);
neonatalsexandrace(white,black,Asian,NativeBrazilian; mulatto);andICD-10codeatfieldsIa,Ib,Ic,Id,andII.
Inordertocalculatetheperinatalasphyxia-specific mor-talityratioandthemeconiumaspirationsyndrome-specific mortalityratio,thenumberoflivebirthsfrom2005to2010 withweight≥2500gwithoutmalformationsreportedinthe birthcertificateswasobtainedatthenationalopen-access publichealthsystemdatabasemaintainedbytheBrazilian Ministry of Health.10 Such ratioswere analyzed yearlyfor thecountryasawholeandfor eachof thefiveregions of Brazil.
Maternal and neonatal characteristics were compared acrossthe yearsofthestudy.Allof thecomparisonsused adescriptivestatisticalanalysis,chi-squaredtest,andSPSS software(IBMSPSSStatisticsforWindows,version21.0,USA) todeterminetrends.
Results
This study found 27,800 early neonatal deaths associ-ated with perinatal asphyxia between 2005 and 2010 in Brazil. Among them, 2767 (10%) had a diagnosis of con-genital malformation on the death certificate and 823 (3%)werenon-viable infantswitheither agestationalage <22 weeks or a birth weight <400g. Among the 24,210 potentially viable infants without congenital malforma-tions,2861 (12%)didnothave birthweightdata.Patients withandwithout birthweightdataweresimilarregarding maternal age, occupation and parity, multiple gestation, gestational age, and neonatal gender. Among the 21,349 deaths with birth weight information, the study found 10,675 (50%) infants withbirth weight≥2500gand
with-outmalformationswhodiedwithperinatalasphyxiarelated conditions.
In Brazil,the rate of early neonatal deaths associated with perinatal asphyxia per 1000 live births of infants withbirthweight≥2500gwithoutcongenitalmalformations
decreasedfrom0.81in2005to0.65in2010(p<0.001).This reductionwassignificantinallBrazilianregionsofthe coun-try(Fig.1A).Theratioofearlyneonataldeathsassociated withmeconiumaspirationsyndromeper1000livebirthsof infants weighing≥2500gwithout malformationsremained between 0.20 and 0.29 during the study period in Brazil, withareductiononly inthesoutheastregionofthe coun-try:from0.24per1000livebirthsin2005to0.18in 2010 (p=0.005;Fig.1B).
early
neonatal
deaths
in
Brazil
579
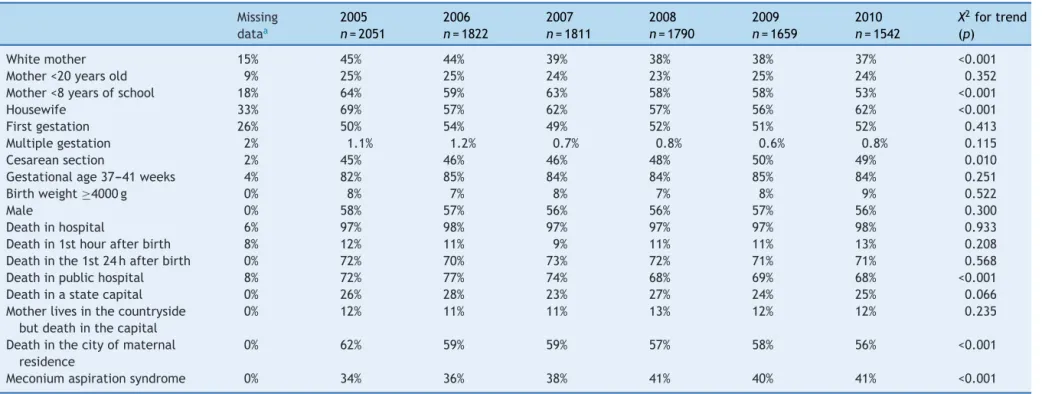
Table1 Characteristicsofthe10,675earlyneonataldeathsassociatedwithperinatalasphyxiaininfantswithbirthweight≥2500gwithoutmalformations,accordingtoyear ofdeath.
Missing dataa
2005
n=2051
2006
n=1822
2007
n=1811
2008
n=1790
2009
n=1659
2010
n=1542
X2fortrend
(p)
Whitemother 15% 45% 44% 39% 38% 38% 37% <0.001
Mother<20yearsold 9% 25% 25% 24% 23% 25% 24% 0.352
Mother<8yearsofschool 18% 64% 59% 63% 58% 58% 53% <0.001
Housewife 33% 69% 57% 62% 57% 56% 62% <0.001
Firstgestation 26% 50% 54% 49% 52% 51% 52% 0.413
Multiplegestation 2% 1.1% 1.2% 0.7% 0.8% 0.6% 0.8% 0.115
Cesareansection 2% 45% 46% 46% 48% 50% 49% 0.010
Gestationalage37---41weeks 4% 82% 85% 84% 84% 85% 84% 0.251
Birthweight≥4000g 0% 8% 7% 8% 7% 8% 9% 0.522
Male 0% 58% 57% 56% 56% 57% 56% 0.300
Deathinhospital 6% 97% 98% 97% 97% 97% 98% 0.933
Deathin1sthourafterbirth 8% 12% 11% 9% 11% 11% 13% 0.208
Deathinthe1st24hafterbirth 0% 72% 70% 73% 72% 71% 71% 0.568
Deathinpublichospital 8% 72% 77% 74% 68% 69% 68% <0.001
Deathinastatecapital 0% 26% 28% 23% 27% 24% 25% 0.066
Motherlivesinthecountryside butdeathinthecapital
0% 12% 11% 11% 13% 12% 12% 0.235
Deathinthecityofmaternal residence
0% 62% 59% 59% 57% 58% 56% <0.001
Meconiumaspirationsyndrome 0% 34% 36% 38% 41% 40% 41% <0.001
580 AlmeidaMFetal.
1.20
Per thousand live births
A
B
Per thousand live births
0.60
0.50
0.40
0.30
0.20
0.10
0.00 1.00
0.80
0.60
0.40
0.20
0.00
Brazil North Northeast Southeast South Midwest
∗chi-square for trend: P<0.01
2005 2006 2007 2008 2009 2010 2005 2006 2007 2008 2009 2010
Figure1 Birthasphyxia-specific(A)andmeconiumaspirationsyndrome-specific(B)earlyneonatalmortalityratioper1000live birthswithbirthweight≥2500gwithoutcongenitalanomalies,accordingtoyearofdeathandregionofBrazil.
The characteristics of the 10,675 infants weighing
≥2500g without malformations who had an early
neona-tal death associated with perinatal asphyxia are shown in Table 1. The contribution of the North and Northeast Brazilianregions toearly neonataldeathsassociated with perinatalasphyxiaincreasedfrom58%in2005to60%in2010 (p=0.040).
Thecharacteristicsofthe4076infantsweighing≥2500g without malformations who had an early neonatal death associated withmeconium aspiration syndrome according toyearofdeathareshown inTable2.Thecontributionof theNorthandNortheast Brazilian regionstothesedeaths increased from 48% in 2005 to 55% in 2010 (p=0.010). Cesareansectionwasperformedmorefrequentlyininfants who had an early neonatal death associated with meco-niumaspirationsyndromewhencomparedwiththetotallive births10(51%vs.48%;p<0.001),especiallyintheNorth(49%
5000
4000
3000
2000
1000
0
2005 2006
Deaths <7 days
Deaths <7 days with perinatal asphyxia Number of deaths
Deaths <7 days with meconium aspiration syndrome
2007 2008 2009 2010
Figure2 Numberofearlyneonataldeathswithbirthweight ≥2500g without congenital anomalies associated with birth asphyxiaandmeconiumaspirationsyndromeinBrazil,according toyearofdeath.
vs.47%;p<0.001),Northeast(43%vs.38%;p<0.001),and Southeast (59% vs. 55%; p<0.001) regions of the country. Neonatalhospitalcarewasequallyavailableininfantswho hadanearlyneonataldeathassociatedwithmeconium aspi-rationsyndromewhencomparedwiththetotallivebirths10 (98%vs.98%;p=0.22),butavailabilityofneonatalhospital care washigher in infants whodied withmeconium aspi-rationsyndromewhen comparedwiththetotallivebirths intheNorth(97%vs.92%;p<0.001)andNortheast(98%vs. 96%;p=0.008)regions.
Discussion
Thisstudyfoundthat10,675infantsweighing≥2500g
with-out malformationsdied within sixdays afterbirth due to perinatal asphyxia; the burden of these deaths per day decreased from 5.6 in 2005 to 4.2 in 2010. Despite the decreasingmortalityratiosinallregionsofthecountry,the NorthandNortheastBrazilianregionspresentedthe great-estburdenofdeaths.Themajorityofthesedeathsoccurred in the first day of life. Perinatal asphyxiacontributed to 40%ofallneonatalBraziliandeathsoflow-riskneonatesin the study period. Notably,40% of deaths associated with asphyxia in this group of infants occurred in a hospital located inadifferent municipalitythan thematernal res-idence.Amongthe10,675earlydeathsofinfantsweighing
≥2500g without malformations and with asphyxia, 4076
early
neonatal
deaths
in
Brazil
581
Table2 Characteristicsofthe4076earlyneonataldeathsassociatedwithmeconiumaspirationsyndromeininfantswithbirthweight≥2500gwithoutmalformations,according toyearofdeath.
Missing dataa
2005
n=698
2006
n=650
2007
n=689
2008
n=741
2009
n=661
2010
n=637
X2fortrend
(p)
Whitemother 13% 46% 46% 43% 39% 42% 39% 0.002
Mother<20yearsold 9% 23% 23% 23% 22% 24% 22% 0.867
Mother<8yearsofschool 19% 62% 59% 61% 58% 58% 52% 0.001
Housewife 34% 76% 62% 68% 60% 58% 63% <0.001
Firstgestation 26% 51% 57% 49% 56% 55% 53% 0.465
Multiplegestation 2% 0.7% 0.9% 0.0% 0.5% 0.8% 0.5% 0.634
Cesareansection 2% 52% 49% 50% 51% 53% 51% 0.555
Gestationalage37---41weeks 4% 84% 87% 87% 87% 87% 87% 0.206
Gestationalage≥42weeks 4% 11% 8% 7% 7% 7% 7% 0.033
Birthweight≥4000g 0% 8% 7% 7% 5% 8% 9% 0.443
Male 0% 52% 51% 52% 51% 50% 51% 0.474
Deathinhospital 6% 98% 98% 99% 97% 97% 99% 0.493
Deathin1sthourafterbirth 7% 7% 9% 6% 8% 8% 9% 0.506
Deathinthe1st24hafterbirth 0% 73% 71% 74% 71% 72% 70% 0.404
Deathinpublichospital 8% 75% 79% 77% 71% 72% 70% <0.001
Deathinastatecapital 0% 31% 35% 28% 32% 28% 28% 0.075
Motherlivesinthecountryside butdeathinthecapital
0% 18% 15% 16% 19% 16% 16% 0.786
Deathinthecityofmaternal residence
0% 62% 62% 61% 59% 58% 56% 0.003
582 AlmeidaMFetal.
acauseofdeath.Itshouldbenotedthat2100neonateswho diedofmeconiumaspirationsyndromedidnothaveany ICD-10coderelatedtointrauterinehypoxiaorbirthasphyxia.
Therewasareductioninperinatalasphyxia-relatedearly neonatal deaths from 0.81 to 0.61 per 1000 live births weighing ≥2500g without malformations throughout the
study period.This decrease wasa result of multiple fac-tors.The primaryforcesthat likelydrove theindexdown includethesocioeconomicanddemographicchanges,with economicgrowth,reductioninincomedisparities, urbaniza-tion,improvededucationofwomen,anddecreasedfertility rates.14,15 From 2003 to 2008, there was a reduction in inequalities in infantand child mortalities at the individ-uallevel, according tomaternal educationand household incomepercapitainBrazil.16DataofallBrazilianlivebirths showthat, during thestudy period (2005---2010), the pro-portion of adolescent mothers decreased from 21.8% to 19.3%,thefrequencyofmotherswithlessthaneightyears ofschool alsodecreased from 48.5%to 34.1%,and hospi-talbirthsincreased from97.1%to98.1%.10 Inthe present study,despite the fact that it covered only early neona-taldeaths, thefrequency of motherswithless than eight yearsof educationdecreased from 64% to53% from2005 to2010,andthefrequencyofmotherswhoarepartofthe workforceincreasedfrom31% to38%in thesame period. ItshouldbenotedthatBrazilexperiencesextremeregional differences,especiallyinsocialindicators,suchashealth, infantmortality,andnutrition.ThericherSouthand South-eastregions present better indicators thanthe Northand Northeast.8 This situationis shown in Fig.1A,which indi-catesthatperinatalasphyxia-relatedearlyneonataldeaths ininfantsweighing≥2500gwithoutmalformationsweretwo timeshigherintheNorthandNortheastwhencomparedwith theSouthandSoutheastregionsofBrazil.
Progress in neonatal survival should include workforce planningtoincreasethenumbersandupgradespecificskills forcareatbirth.17InChina,policychangespermitted mid-wives to initiate resuscitation and required resuscitation training for licensure. From 2003 to 2008, over 110,659 professionalsreceived resuscitation training in 322 repre-sentativehospitals.Perinatalasphyxia-relateddeathsinthe delivery room decreased from 0.75 to 0.34 per 1000 in thisperiod.18 The large-scaleeducationprogramaimedat improving the skills of providers, the Brazilian Neonatal ResuscitationProgram,mayhavecontributedtothe reduc-tioninperinatalasphyxia-relatedearlyneonataldeathsof Brazilian infants weighing ≥2500g without malformations from 2005 to 2010.19 This program trained over 75,000 providerswhoworkinthedeliveryroomsusinganetworkof morethan800instructorsinallBrazilianstatessince1994 accordingtoguidelinesbasedonthebestavailable global evidenceandupdatedeveryfiveyears.20---22
Areviewofstudiesdemonstratedthatmeconium-stained amniotic fluid occurs in 13% of pregnancies and that aspiration syndrome occurs in 4% of those born with meconium-stained fluid, with a mortality rate of 10 per 100,000 live births.23 The mortality ratios attributed to meconium aspiration syndrome ranged from 1 to 5 per 100,000 live births in developed countries in the last decade.24,25 In Brazil, from 2005 to 2010, the meconium aspirationsyndrome-specificearlyneonatalmortalityratio ininfantsweighing≥2500gwithoutmalformationswas23.3
per100,000livebirths,whichisfourto23timeshigherthan thosepreviouslyreported.Despitethedecreaseinperinatal asphyxia-relatedearlyneonataldeathsinthepresentseries, notonly didthedeathsassociated withmeconium aspira-tionsyndromenotdecrease,butalsotheircontributionto perinatalasphyxia-relatedearlyneonataldeathsincreased from34%in2005to41%in2010.Itisnoteworthythatthis findingoccurreddespitetheastonishingincreasingratesof cesarean section in Brazil from43.3% in 2005 to52.3% in 2010.10Itmaybespeculatedwhethersurgicaldeliveriesand neonatalhospital carewere notavailable for infants who diedwithmeconiumaspirationsyndrome,butthepresent results indicate that this was not the case. In North and Northeast regions, in which the highest burden of meco-niumaspirationsyndromeonearly neonatalmortalitywas observed(Fig.1B),theavailabilityofcesareandeliveryand neonatalhospitalcarewasevenhigherinthestudiedinfants when compared with all live births of the same regions. One of the reasons for this highly specific early neonatal mortality rateis likelyrelated toproblems in the organi-zationoftheBrazilianperinatalcaresystem,whichforces womenreadytogivebirthtoapproachmorethanone hospi-talbeforebeingadmittedtoamaternityward,occasionally inamunicipalitydistantfromtheirresidences.26 Addition-ally,sincesecondary referralhospitals,especiallyinNorth andNortheast Brazil,donothave neonatalintensive care units,pregnantwomenareusuallytransferredwhenthere is evidenceoffetaldistress, leadingtodelaysinreaching thereferralhealthcarefacilityand,consequently,todelays in receivingtimely andadequate care.27 According tothe present data,amongtheinfantswhodiedfrommeconium aspirationsyndrome,38%oftheirmotherslivedinacity dif-ferentfromthefacilitywheretheinfantdeathoccurredin 2005,andthisincidenceincreasedto44%in2010.
thefederalgovernmenttoimprovematernalandneonatal health afterwards. In 2011, the Ministry of Health estab-lishedtheRedeCegonha(StorkNetwork),aimingtoexpand the access to and improve the quality of prenatal care andassistanceduringdelivery,postpartumcare,andchild care.29 The impactof these actions may have decreased neonatalmortalityassociatedwithperinatalasphyxiainthe followingyears.
A safe birth and healthy start in life are the heart of humancapitalandeconomicprogress.4,30Thisstudy demon-stratedthatearlyneonatalmortalityratesduetoperinatal asphyxiaofinfants inthebetterspectrumof birthweight and without congenital malformations are still high, and meconium aspiration syndrome plays a major role. The results of thisstudy mayhelp toenhance national health planningby identifyingandovercoming bottlenecksin the maternalandneonatalcaretoimprovenewbornsurvival.
Funding
Fundac¸ão Sociedade Brasileira de Pediatria funded the software for data entry, the professionals that entered the data in the database, and the English translation of the manuscript by American Journal Experts. Fundac¸ão SociedadeBrasileiradePediatriadidnothaveanyroleinthe studydesign;inthecollection,analysis,andinterpretation ofdata;inthewritingofthereport;norinthedecisionto submitthemanuscriptforpublication.Noneoftheauthors werepaidtowritethismanuscript.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
The authorswouldliketothanktheStateCoordinatorsof BrazilianNeonatalResuscitationProgramfrom2005to2012, the State Health Departments, and the Fundac¸ão SEADE (ProcessoUnifesp23089000057/2014-95)fordatacollection ineachfederativeunitofBrazil.Theauthorswouldalsolike tothanktheBrazilian PediatricSocietyforthe continuous supporttotheNeonatalResuscitationProgram.
References
1.LiuL,OzaS,HoganD,PerinJ,RudanI,LawnJE,etal.Global, regional,andnationalcausesofchildmortalityin2000---13,with projectionstoinformpost-2015priorities:anupdated system-aticanalysis.Lancet.2015;385:430---40.
2.Lawn JE, Bahl R, Bergstrom S, Bhutta ZA, Darmstadt GL, Ellis M, et al. Setting research priorities to reduce almost one million deaths from birth asphyxia by 2015. PLoS Med. 2011;8:e1000389.
3.WangH,LiddellCA,CoatesMM,MooneyMD,LevitzCE, Schu-macher AE, et al. Global, regional, and national levels of neonatal,infant, andunder-5mortalityduring1990---2013:a systematicanalysisfortheGlobalBurdenofDiseaseStudy2013. Lancet.2014;384:957---79.
4.LawnJE,BlencoweH,OzaS,YouD,LeeAC,WaiswaP,etal. Everynewborn:progress,priorities,andpotentialbeyond sur-vival.Lancet.2014;384:189---205.
5.LawnJE,LeeAC,KinneyM,SibleyL,CarloWA,PaulVK,etal. Twomillionintrapartum-relatedstillbirthsandneonataldeaths: where, why, and what canbe done?Int JGynaecol Obstet. 2009;107:S5---19.
6.Ariff S, Lee AC, Lawn J, Bhutta ZA. Global burden, epi-demiologic trends, and prevention of intrapartum-related deaths in low-resource settings. Clin Perinatol. 2016;43: 593---608.
7.LawnJE,CousensS,ZupanJ,LancetNeonatalSurvivalSteering Team.4millionneonataldeaths:when?where?why?Lancet. 2005;365:891---900.
8.TheWorldBank.Brazil:overview;2015[cited1Jul2016]. Avail-ablefrom:http://www.worldbank.org/en/country/brazil
9.Millennium Development Goals Indicators. MDG country
progress snapshot: Brazil; 2015 [cited 1 Jul 2016].
Avail-able from: http://mdgs.un.org/unsd/mdg/Resources/Static/
Products/Progress2015/Snapshots/BRA.pdf
10.Brasil.MinistériodaSaúde. PortaldaSaúdeDatasus:
estatís-ticasvitais.[cited1Jul2016].Availablefrom:http://www2.
datasus.gov.br/DATASUS/index.php?area=0205.
11.MacDorman MF, Matthews TJ, Mohangoo AD, Zeitlin J. Internationalcomparisonsofinfantmortalityandrelated fac-tors: United States and Europe, 2010. Natl Vital Stat Rep. 2014;63:1---6.
12.MatthewsTJ,MacDormanMF.Infantmortalitystatisticsfrom the2010periodlinkedbirth/infantdeathdataset.NatlVital StatRep.2013;62:1---26.
13.WorldHealthOrganization(WHO).Internationalstatistical clas-sification ofdiseases and relatedhealth problems.10threv. Geneve:WHO;2010.
14.VictoraCG,AquinoEM,doCarmoLealM,MonteiroCA,Barros FC,SzwarcwaldCL.MaternalandchildhealthinBrazil:progress andchallenges.Lancet.2011;377:1863---76.
15.Victora CG, Barreto ML, do Carmo Leal M, Monteiro CA, Schmidt MI, Paim J, et al. Health conditions and health-policyinnovationsinBrazil:thewayforward.Lancet.2011;377: 2042---53.
16.GarciaLP,SantanaLR.[Evolutionofsocioeconomicinequalities ininfantand childmortalityinBrazil,1993---20].CienSaude Colet.2011;16:3717---28.
17.Dickson KE, Simen-Kapeu A, Kinney MV, Huicho L, Vesel L, LackritzE,et al.EveryNewborn:health-systemsbottlenecks and strategies to accelerate scale-up in countries. Lancet. 2014;384:438---54.
18.XuT,WangHS,YeHM,YuRJ,HuangXH,WangDH,etal.Impact ofanationwidetrainingprogramforneonatalresuscitationin China.ChinMedJ(Engl).2012;125:1448---56.
19.Niermeyer S. From the Neonatal Resuscitation Program to Helping Babies Breathe: global impact of educational pro-grams in neonatal resuscitation. Semin Fetal Neonatal Med. 2015;20:300---8.
20.Perlman JM, Wyllie J, Kattwinkel J, Atkins DL, Chameides L, GoldsmithJP, et al.Part11:Neonatal resuscitation:2010 internationalconsensusoncardiopulmonaryresuscitationand emergencycardiovascularcaresciencewithtreatment recom-mendations.Circulation.2010;122:S516---38.
21.PerlmanJ,KattwinkelJ,WyllieJ,GuinsburgR,VelaphiS,Nalini Singhal for the Neonatal ILCOR TaskForce Group. Neonatal resuscitation:inpursuitofevidencegapsinknowledge. Resus-citation.2012;83:545---50.
22.Sociedade Brasileira de Pediatria. Programa de
Reanimac¸ão Neonatal. [cited 1 Jul 2016]. Available from:
http://www.sbp.com.br/reanimacao
584 AlmeidaMFetal.
24.DargavillePA,CopnellB,AustralianandNewZealandNeonatal Network.Theepidemiologyofmeconiumaspirationsyndrome: incidence, risk factors, therapies, and outcome. Pediatrics. 2006;117:1712---21.
25.Fischer C,RybakowskiC,FerdynusC,Sagot P,GouyonJB.A population-based studyof meconium aspiration syndrome in neonates born between 37and 43weeks ofgestation.Int J Pediatr.2012;2012:321545.
26.LanskyS,LimaFricheAA,SilvaAA,CamposD,Azevedo Bitten-courtSD, CarvalhoML,etal.BirthinBrazilsurvey:neonatal mortality,pregnancyandchildbirthqualityofcare.CadSaude Publ.2014;30:S1---15.
27.WallSN,LeeAC,CarloW, GoldenbergR,NiermeyerS, Darm-stadtGL,etal.Reducingintrapartum-relatedneonataldeaths
inlow-andmiddle-incomecountries-whatworks?Semin Peri-natol.2010;34:395---407.
28.Brasil. Ministério da Saúde. Portal da Saúde. Datasus
Indi-cadores demográficos: razão entre óbitos informados e
estimados.[cited1Jul2016].Available from:http://tabnet.
datasus.gov.br/cgi/idb2011/a1802b.htm.
29.Angulo-Tuesta A, Santos LM, Natalizi DA. Impact of health researchonadvancesinknowledge,researchcapacity-building and evidence-informed policies: a case study on mater-nal mortality and morbidity in Brazil. Sao Paulo Med J. 2016;134:153---62.