www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Epidemiology
of
communication
disorders
in
childhood
phoniatric
clinical
practice
夽
,
夽夽
Marta
Gonc
¸alves
Gimenez
Baptista
a,b,∗,
Beatriz
Cavalcanti
Albuquerque
Caiuby
Novaes
c,d,
Mariana
Lopes
Favero
c,daProgramofGraduateStudiesinPhonoaudiology,PontifíciaUniversidadedeSãoPaulo(PUC-SP),SãoPaulo,SP,Brazil bClínicaInterdisciplinarProf.Dr.MauroSpinelli,SãoPaulo,SP,Brazil
cPontifíciaUniversidadeCatólicadeSãoPaulo(PUC-SP),SãoPaulo,SP,Brazil dDerdic,PontifíciaUniversidadeCatólicadeSãoPaulo(PUC-SP),SãoPaulo,SP,Brazil
Received16January2014;accepted6January2015 Availableonline9June2015
KEYWORDS
Childlanguage;
Language development;
Speechdisorders;
Epidemiology
Abstract
Introduction:Languageacquisitionanddevelopmentrequireanunderstandingofphysicaland psychosocialaspectsduringdiagnosisandtreatment.Atthispoint,apartnershipbetween pho-niatricphysiciansandotherhealthprofessionalsisoftenadeterminantforfavorableprognosis.
Objective:Toidentifytheclinicalandepidemiologicalcharacteristicsofapediatricpopulation attendingaphoniatricclinicalpractice.
Methods:Study design: Cross-sectional cohort. Retrospective, epidemiologicalstudy of297 children,seeninphoniatricappointmentsbetween1976and2005.Outcome variableswere referralorigin,gender,age,meanage,diagnosis,andtreatmentapproach.
Results:66%weremaleand34%werefemale,withameanageof6.4years.Thelargestnumber ofreferralsfor phoniatrictreatmentscame fromspeech therapists(38%).Thepredominant complaintwas alteration inspeech (35%);thediagnostics inspeech,language, andfluency (49.5%)arenoteworthy.Consideringthetotalofthepatientsanalyzed,28.2%werereferredfor speechtherapyand11.8%forpsychotherapy.
Conclusion:The studiedpopulationis predominantlymale,thediagnosis pointstoahigher incidenceincasesofimpairmentinspeech,language,andfluency;themostcommontreatment wasspeechtherapy.
© 2015Associac¸ãoBrasileira de Otorrinolaringologiae CirurgiaCérvico-Facial. Publishedby ElsevierEditoraLtda.Allrightsreserved.
夽
Pleasecitethisarticleas:BaptistaMGG,CaiubyNovaesBCA,FaveroML.Epidemiologyofcommunicationdisordersinchildhoodphoniatric clinicalpractice.BrazJOtorhinolaryngol.2015;81:368---73.
夽夽Institution:PontifíciaUniversidadedeSãoPaulo(PUC-SP),SãoPaulo,SP,Brazil.
∗Correspondingauthor.
E-mail:[email protected](M.G.G.Baptista).
http://dx.doi.org/10.1016/j.bjorl.2015.01.006
PALAVRAS-CHAVE
Linguageminfantil;
Desenvolvimentoda
linguagem;
Distúrbiosdafala;
Epidemiologia
Epidemiologiadosdistúrbiosdecomunicac¸ãonainfânciaemclínicafoniátrica
Resumo
Introduc¸ão: Aquisic¸ão e desenvolvimento da linguagem demandam cuidados exigindo com-preensão dos aspectos orgânicos e psíquicos no diagnóstico e tratamento. Assim, parceria entre foniatra e outros profissionais é, muitas vezes, determinante de um prognóstico favorável.
Objetivo: Caracterizarclínicaeepidemiologicamenteosdistúrbiosdecomunicac¸ãoemcrianc¸as napráticaclínica.
Método: Coortetransversalhistórica.Estudoepidemiológicoretrospectivode297prontuários de crianc¸as atendidas em consulta foniátrica no período entre 1976 a 2005. Variáveis: origem do encaminhamento, gênero, média da idade, diagnóstico e conduta para trata-mento.
Resultados: 66%foramdogêneromasculinoe34%dofemininocommédiadeidadede6,4anos. Maiornúmerodeencaminhamentosfoirealizadoporfonoaudiólogos(38%).Aqueixa predomi-nanteeradealterac¸õesnafala35%eressaltam-seosdiagnósticosnaáreadafala,linguageme fluência(49,5%).Dototaldestacaram-seosencaminhamentospara:28,2%fonoterapiae11,8% psicoterapia.
Conclusão:A populac¸ão atendida foi predominantemente masculina, o diagnóstico aponta maiorincidênciaemquadrosdecomprometimentonafala,linguagemefluênciaeotratamento maisindicadofoifonoterapia.
©2015Associac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial.Publicado por ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
For the establishment of proper diagnosis and
appropri-ate treatment, children with language disorders require
the services of a coordinated medical and phoniatric
team capable of considering that organic, psychological,
and social factors can be part of the genesis of this
problem.1
Evenincaseswherethereisanobviousfunctional
abnor-malityofanorganorsystem,e.g.,incasesofhearingloss,
cleftpalate,andencephalopathy,itiscriticaltounderstand
that the problems that arise in patients with
communi-cation difficulties are complexand sometimes difficult to
understand. Affected children and their families, when
seeking help for communication difficulties look for
clini-calresponsesthatappreciatethebiopsychicfoundationsof
theirlanguagedisorder.2
Theotorhinolaryngologistinvolvedinphoniatricsplaysa
keyroleinthiscomplexprocessofhumancommunication,
notonly at the timeof diagnosis, but alsoduring his/her
communicationwiththeteamhelpingtoformulatethebest
conduct and the most appropriate intervention for each
patient.3
Similarly,duetothelargenumberofpotentialdiagnoses
forachildwithalanguagedisorder---forexample,specific
languageimpairment,languagedelay,andarticulation
dis-orders,webelieve thatepidemiologicalstudiesareuseful
tohelpinselectingthecompositionoftheteamnecessary
to care for these children. In this sense, the aim of this
studywastoepidemiologicallycharacterizethepracticeand
thereferralsmadetoaphoniatricclinicforcommunication
disordersoccurringinchildhood
Methods
ThestudydesignwasapprovedbytheEthicsCommitteeof
PontifíciaUniversidadeCatólicadeSãoPaulo,accordingto
Declarationno.06919712.6.0000.5482.
A retrospective study of a historical cross-sectional
cohortwas conducted. Froma total of 843 patients with
complaints of a disorder of communication submitted to
phoniatricassessment andtreatment inaprivateclinic in
the city of São Paulo between June of 1976 and January
of2005half,wereanalyzed(thoseregisteredwithaneven
number).Fromthesemedicalrecords,onlychildrenofboth
gendersofbetweenages1yearand11yearsand11months
wereincluded,totaling422records.
Exclusioncriteria:incompleteorillegiblerecords
Duringthephoniatricconsultation,onesemi-openinterview
tookplace, where datawere collectedon thecomplaint,
previoushistoryofthecomplaint,familyhistory,schooling,
familyroutine,feedinghabits,neuropsychomotor
develop-ment,andsocialandfamilyrelationships.
In addition to an otorhinolaryngological examination,
the phoniatrist used games and symbolic play, drawing,
and writing (depending on the child’s age) to investigate
aspectsrelated to global and oral motor functions,
audi-tory and visual perceptual functions, static and dynamic
balance,and spatial orientation at body and graphic
lev-els.Theexaminationsprovidedbythechild’sparentsduring
the consultation were also considered, and the physician
orderedotherappropriateteststocomplementthedatafor
0%
P≤0.01 Pho
noaudiologist Physi
cian School
Acquainta nce
Not i nformed
Psycho logist
Psyc hopedagogi
st
Insti
tution Dentist Nurse Teac
her
Spontaneously attended the clinic 38.0%
19.9%
10.4%
8.4% 7.7% 5.4%
3.7% 3.4%
1.3% 0.7% 0.3% 0.3% 35%
30%
25%
15%
10%
5% 20%
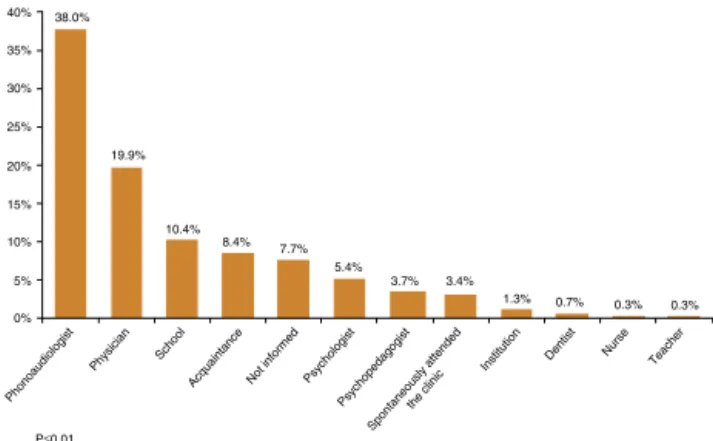
Figure1 Distributionofreferrals acceptedby phoniatrists, accordingtothesourcesoforigin.
Fortheanalysis,thefollowingvariableswereused:
gen-der,meanage,referralsource,familycomplaint,diagnosis,
andconduct.
The statistical analysis wasperformed usingan ANOVA
parametrictest(quantitativeandcontinuousdata)andthe
equalityoftwoproportionsnonparametrictest(qualitative
data).Asignificancelevelofp=0.05(5%)witha95%
confi-denceintervalwasestablished.4
Results
Of422medicalrecords,22wereexcludedfor
incomplete-nessand103forbeingoutsidethestipulatedage.Thus,297
medicalrecordswereevaluated.Ofthissample,most
chil-drenweremale(n=196;66%)comparedtofemales(n=101;
34%;p<0.001)andthemeanagewas6.3±0.3years.Mostof
thepatientscamefromthecityofSãoPaulo,i.e.,65.32%of
cases(p<0.01%).Mostreferralstophoniatricconsultation
were made by speech therapists, 38% (Fig.1). The main
familycomplaintwasachangeinspeech(p≤0.01;Fig.2),
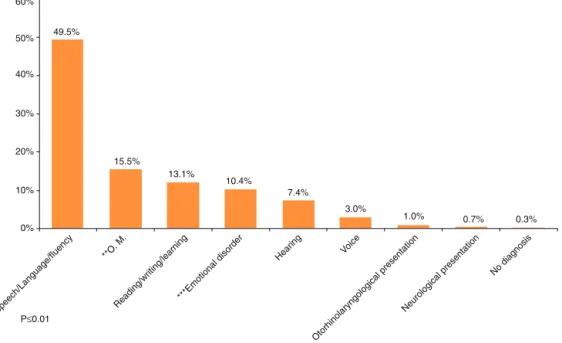
and the most frequent diagnosis was established in the
speech/language/fluencyarea(49.5%;p≤0.01;Fig.3).
Inthe analysis of the gender and diagnostic variables,
nostatisticallysignificantdifferenceswerefoundbetween
thetwogenderswithrespectto‘‘hearing,’’‘‘neurological
picture,’’and‘‘voice’’diagnoses(andalsoin‘‘no
diagno-sis’’cases).Astatisticallysignificantdifferencewasfoundin
thosediagnosesrelatedtospeech/language/fluencyareas,
with a prevalence of 63.9% in boys and 36.1% in girls
(p<0.001)(Table1).
Thephoniatricdiagnosiswasanalyzedconsideringthree
age groups, distributed as follows: 0---5 years, >5 and
≤10 years, and >10 years. In the first two age groups,
speech/language/fluency was the most common
diagno-sis. However, in the group of children over 10 years of
age, the most frequent diagnosis was established in the
reading/writing/learning area, with 33.3%, but therewas
no statistical differencevs. the diagnoses established for
speech/language/fluencyandemotionaldisturbance(30.3%
and15.2%,respectively;Table2).
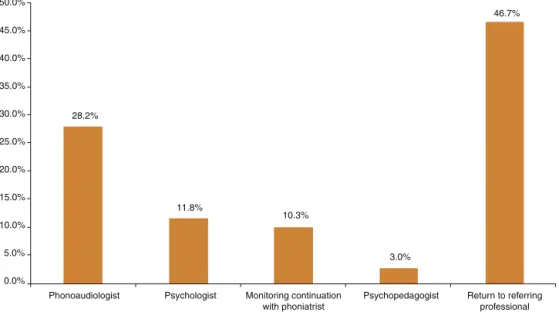
Thephoniatristreturned46.7%ofthesepatientstothe
professionalsresponsibleforthepatient’sreferral:28.2%for
speechtherapy,11.8%forpsychotherapy,and3%for
educa-tionalpsychology,asshowninFig.4.Theremainingpatients
(10.3%)weretoreturntothephoniatristformonitoring.
Discussion
Phoniatrics is an areaof otorhinolaryngologywhich treats
humancommunicationdisorders,focusingonvoice,speech,
language,hearing,andswallowingfunctions.1Asafunction
of the complexity of the process of human
communica-tion and of the enormous range of possible diagnoses, it
0%
P≤0.01 5% 10% 15% 20% 25% 30% 35% 35.0%
19.5% 16.8%
5.7%
3.7% 3.0% 3.0%
1.3% 1.3% 1.0% 1.0% 1.0% 0.7% 0.7% 0.7% 40%
Alterations in speech Learning
Delayed speech/language Speech fluency
Voic e
Behavior
Alterations in speech + learning
Alterations in speech + orofacial motricity Global development
Alterations in speech + global development Learning + behavior
Questioning about the theoretical approach used in speech therapy Alterations in speech + behavior
Hearing
Orofacial motricity
0%
P≤0.01
*Speech/Language/fluency
**O. M.
Reading/writing/learnin g
***Emotional disorde r
Hearing Voice
Neurological presentatio n
No diagnosis
Otorhinolaryngological presentation
10% 20% 30% 40% 50% 60%
49.5%
15.5%
13.1%
10.4%
7.4%
3.0%
1.0% 0.7% 0.3%
Figure3 Diagnosisdistributionaccordingtomaindisordersfound.*Speech/language/fluency---languagedeviations,language deviationsdelay,speechdisorders,specificlanguagedisorder,dyspraxia, anddisfluency.** Articulationdisorders,alterationsin chewing,swallowing,andrespiration,sigmatism,malocclusion,andtonedeficitofOFA(O.M.=oralmotricity).***Inhibition,clinical picturesofpsychosis,autism,psychicimbalance,anddepression.
Table1 Distributionofdiagnosticsbygender.
Disturbances(byarea) Female Male p-Value
n % n %
Hearing 10 45.5% 12 54.5% 0.546
Emotional 10 32.3% 21 67.7% 0.005
Speech/language/fluency 53 36.1% 94 63.9% <0.001
Reading/writing/learning 8 22.2% 28 77.8% <0.001
Oralmotricity 15 33.3% 31 66.7% 0.002
Neurologicalpicture 1 50.0% 1 50.0% 1.000
Otorhinolaryngological 0 0% 3 100% 0.014
Voice 3 33.3% 6 66.7% 0.157
Withoutadiagnosisa 1 100% 0 0% 0.157
a Medicalrecordwithoutadiagnosis.
Table2 Distributionofmaindiagnosesbyagegroup.
Disturbances(byarea) ≤5years >5and≤10years >10years
n % n % n %
Hearing 5 4.8% 14 9.8% 3 8.8%
Emotional 10 9.5% 16 11.2% 5 14.7%
Speech/language/fluency 73 69.5% 66 46.1% 10 29.4%
Reading/writing/learning 0 0.0% 23 16.1% 12 35.3%
Oralmotricity 17 16.2% 24 16.8% 4 11.8%
is believed thatthesuccess of thetreatment for
commu-nication disorders in childhoodis intimately linked to an
interdisciplinarystrategyandtoaneffective interlocution
amongtheteammembers.
The analysis of the population representedby the 297
successfullyevaluatedmedicalrecordsreflectsthefindings
in the literature. A significant majority of families
0.0%
Phonoaudiologist Psychologist Psychopedagogist Return to referring professional Monitoring continuation
with phoniatrist 5.0%
10.0% 15.0% 20.0% 25.0% 30.0% 35.0% 40.0% 45.0% 50.0%
28.2%
11.8%
10.3%
3.0%
46.7%
Figure4 Distributionofphoniatristconduct.
appointmentwithacomplaintofspeechdisorder(Fig.2).5
However,whenanalyzing thephoniatric diagnosis(divided
into broad areas, as a result of statistical adjustments),
itcan be notedthat malegender representsa significant
majorityofalterationsbothinthespeech/language/fluency
area, the most frequent diagnosis group (Fig. 3) that
includeslanguagedeviations,delaysinlanguageacquisition,
speech disorders, specific language disturbance,
dysprax-ias, anddysfluency, aswell asin the reading and writing
alterations, oral motricity problems, emotional disorders,
andotorhinolaryngologicaldisorders(Table1).Thiscouldbe
explainedbyhormonalissuesinboysandtheirslower
neuro-logicalmaturity,and,accordingtosomestudies,alsobythe
socialdemandsthatareincurredinthesechildren,when,by
culturalimposition,theyarecalledupontospeakcorrectly.
Thereareseveralexplanationsforthemalepredominance
intheliterature,butthereisnodefinitiveconsensus.6---8
Theageofchildrenatthetimeofthephoniatric
assess-mentwasaround6years,withameanageof6.4±0.4years,
which may coincide with their entrance into elementary
school.Inthiscontext,thechildisinsertedintothesocial
group,interactingwithpeers andteachers;thus, thereis
agreater demand for communication, and thismay
high-lighttheexistingdifferencesinthegroup,9,10stimulatingthe
child’sreferralandthesearchforaphoniatricevaluation.
However,inmanycases---anddependingontheseverity
of this delay --- seeking specialized care and/or a
phoni-atricdiagnosisonly whenthechildreaches 6yearsofage
mayhavenegativedevelopmentalconsequencessincegood
communicationisessential forphysical andmental
devel-opmentWhile 60%of children withlanguagedelay at the
age of 2 years achieve language development similar to
thatoftheirnormalpeersin12monthswithouttreatment,
thepersistenceoftheirsymptomsbringsadverseeffectson
learning,behavior,socialskills,andmentalhealthin
adult-hood;therefore,theyshouldnotbeoverlooked.11
Itmustalsobeconsideredthatattheageof6,thechild
beginstolearnhowtoreadandwrite,bothnecessary for
developingliteracy. Achild whohasnotconsolidated oral
languagemayhavelowerchancesofadvancinginthe
writ-tenlanguageatthesamepaceofotherchildren,considering
thatpartoforalskillsareusedinthewritingprocess.12
Table2documentshowspeechandlanguagedelayscan
belong-lastingthroughout childhood;thisis themost
fre-quent diagnosis under 5 years of age and between 5 and
10 years of age, and is almost as common as the
read-ing/writing/learningalterationsinchildrenover10years.
We believe that an interdisciplinary approach in the
phoniatricscliniciscriticaltoagoodprognosisfor
commu-nicationdisorders. Fig.4 presentsa goodexample of the
interdisciplinarynatureand,especially,ofthecomposition
of theteam, sincemost ofthe patients returnedtotheir
originalcareprovidersattheconclusionoftheirphoniatric
assessment,toproceedwiththetreatment.
In the formation of this team, a partnership between
thephoniatristandthespeechtherapist isoffundamental
importance, whether in the treatment of clinically
com-plexcases, in longitudinal follow-uppursuing adiagnosis,
or interpreting specific data stemming fromthe language
assessment.
Thespeechtherapiststandsoutastheprofessionalwho
often directs patients to phoniatric evaluation (Fig. 1);
furthermore, he/she is the professionalwho receives the
greatestnumberofindicationsofpatientsbasedonthe
pho-niatrist’s clinical conduct (Fig.4). Itmust be emphasized
that well-coordinated work between these specialties
---phonoaudiologyandphoniatrics---cancontributetogreater
efficacyinthetreatment ofchildrenwithspeechand
lan-guagedisorders.13,14
Theimportanceofthepsychologistasamemberofthe
interdisciplinaryteamfortreatingcommunicationdisorders
isworthmentioning. Inthisseries,11.8%ofpatientswere
referredbythespeechspecialistforapsychological
evalu-ation(Fig.4).Consideringthatpsychologicaldisordersand
sufferingaredirectlyrelatedtolanguageproblems,15---17and
are frequently the primary cause of the delay, an
inter-vention that considers the child’s psychic and language
Conclusion
Thepopulationstudiedcomprisedpredominantlymales,and
thediagnosispointstoahigheroccurrenceofproblemsin
thespeech,languageandfluencyarea.Themostcommonly
recommendedtreatmentwasspeechtherapy.
Funding
This study was supported by CAPES (Coordenac¸ão de
Aperfeic¸oamentodePessoaldeNívelSuperior).
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.Union Europeenne des medecins specialists (UEMS/Union of theEuropeanPhoniatricians(UEP).Traininglogbookof phoni-atrics.VersãoOctober1st,2010.Availablefrom:http://www. orluems.com/gestor/upload/file/7%20Logbook%20Phoniatrics
[accessed31.01.13].
2.Spinelli M. O diagnóstico foniátrico nos transtornos da lin-guagem.DistúrbiosComun,SãoPaulo.2003;15:143---9.
3.TabithAJr.Distúrbiosdodesenvolvimentodalinguagem: aspec-tosfoniátricos.Fórum:INES,RiodeJaneiro.2005;12:16---27.
4.Vieira S. Bio Estatística Tópicos Avanc¸ados. 2nd ed.Rio de Janeiro:Ed.Campus;2004.
5.Lima BPS, GuimarãesJATI, Rocha MCG. Características epi-demiológicas das alterac¸ões de linguagem em um centro fonoaudiológicodo primeiro setor. RevSoc Bras Fonoaudiol. 2008;13:376---80.
6.ChoudhuryN, BenasichAA. A family aggregation study: the influenceoffamilyhistoryandotherriskfactorsonlanguage development.JSpeechLangHearRes.2003;46:261---72.
7.Fávero ML, Higino TC, Pires AP, Burke PR, Silva FL, Tabith JúniorA.Pediatricphoniatryoutpatientward:clinicaland epi-demiologicalcharacteristics.BrazJOtorhinolaryngol.2013;79: 1---5.
8.Spinelli M, Tabith A. Distúrbios Específico de linguagem aspectos conceituais, fundamentos biológicos e dados clíni-cos. In: Massari IC, Spinelli M, Goro A, Sollero DC, Penido JCA, editors.Quando ainteligência nãoencontrapalavras ---Distúrbio Específico de Linguagem. São Paulo: LCTE; 2014. p.13---23.
9.BergèsJB.Porquecincovezesmaismeninosnãoaprendem?In: BergèsJ,Bergès-BounesM,Calmettes-JaeanS,editors.Oque aprendemoscomcrianc¸asquenãoaprendem?PortoAlegre:CMC Ed.;2008.p.69---72.
10.Vygotsky L. SA pré-história da linguagem escrita. In: A formac¸ãosocial da mente.São Paulo: MartinsFontes; 1984. p.117---34.
11.BoyleJ.Speechandlanguagedelaysinpreschoolchildren.BMJ. 2011:343[Editorials].
12.NicolietoAP,FernendesGB,GarciaVL,HageSRV.Desempenho escolar de crianc¸as com Distúrbio Específico de Linguagem: relac¸õescomhabilidadesmetafonológicasememóriadecurto prazo.RevBrasFonoaudiol.2008;13:246---50.
13.Spinelli M. Distúrbiosno Desenvolvimentoda Linguagem.In: Assumpc¸ãoFBJr,editor.PsiquiatriadaInfânciaeda Adolescên-cia.SãoPaulo:Santos;1994.p.171---9.
14.JerusalinskyA, CoriatE.Aspectosestruturaiseinstrumentos dodesenvolvimentoinfantil.Escritosdacrianc¸a,vol.4.Porto Alegre:CentroLydiaCoriat;1996.
15.Gupta AR, State MW. Autism: genetics. Rev Bras Psiquiatr. 2006;28:S29---38.
16.SpinelliM.DistúrbiosSeverosdeLinguagemnacrianc¸a. Termi-nologiaeaspectosclínicos. In:PaivaAF,SpinelliM,VieiraS, editors.DistúrbiosdeComunicac¸ão:EstudosInterdisciplinares. SãoPaulo:Cortez;1981.p.15---31.