w w w . r b h h . o r g
Revista
Brasileira
de
Hematologia
e
Hemoterapia
Brazilian
Journal
of
Hematology
and
Hemotherapy
Original
article
Socioeconomic
and
demographic
characteristics
of
sickle
cell
disease
patients
from
a
low-income
region
of
northeastern
Brazil
Thales
Allyrio
Araújo
de
Medeiros
Fernandes
a,∗,
Tereza
Maria
Dantas
de
Medeiros
b,
Jayra
Juliana
Paiva
Alves
b,
Christiane
Medeiros
Bezerra
b,
José
Veríssimo
Fernandes
b,
Édvis
Santos
Soares
Serafim
c,
Maria
Zélia
Fernandes
d,
Maria
de
Fatima
Sonati
eaUniversidadedoEstadodoRioGrandedoNorte(UERN),Mossoró,RN,Brazil bUniversidadeFederaldoRioGrandedoNorte(UFRN),Natal,RN,Brazil cHemocentroDaltonCunha(HEMONORTE),Natal,RN,Brazil
dHospitalInfantilVarelaSantiago,Natal,RN,Brazil
eUniversidadeEstadualdeCampinas(UNICAMP),Campinas,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received27October2014 Accepted27February2015 Availableonline14April2015
Keywords:
Anemia Sicklecell
Socioeconomicfactors Hydroxyurea
Vaccination Penicillin
a
b
s
t
r
a
c
t
Objective:Tocharacterizethesocioeconomicanddemographicaspectsofsicklecelldisease patientsfromthestateofRioGrandedoNorte(RN),NortheastBrazil,andtheiradherence totherecommendedtreatment.
Methods:Thiscross-sectionaldescriptivestudywasperformedatreferralcentersforthe treatmentofhematologicaldiseases.Onehundredandfifty-fiveunrelatedindividualswith sicklecelldiseasewhowenttothesecentersforoutpatientvisitswereanalyzed.Allthe patients,ortheircaregivers,wereinformedabouttheresearchproceduresandobjectives, andansweredastandardizedquestionnaire.
Results:The patients were predominantly younger than 12 years old, self-declared as mulatto,livedinsmalltownsfairlydistantfromthereferralcenter,andhadlow educa-tionandsocioeconomiclevels.Individualswhoweretenor youngerwerediagnosedat anearlierage.Almost50%ofthepatientsweretakinghydroxyurea,91.4%reported hav-ingreceivedpneumococcal/meningococcalvaccinationsand76.1%receivedpenicillinas antibioticprophylaxis.However,themajorityofthemreportedhavingdifficulties follow-ingtherecommendationsofthephysicians,mainlyinrespecttoattainingtheprescribed medicationsandtransportationtothereferralcenters.
Conclusion:Theseindividualshaveavulnerablesocioeconomicsituationthatcanleadto anaggravationoftheirgeneralhealthandthusdeservespecialattentionfromthe med-icalandpsychosocial perspectives.Thus,itisnecessarytoimprovepublicpoliciesthat provideBraziliansicklecelldiseasepatientswithbetteraccesstomedicaltreatment,living conditions,andintegrationintosociety.
©2015Associac¸ãoBrasileiradeHematologia,HemoterapiaeTerapiaCelular.Published byElsevierEditoraLtda.Allrightsreserved.
∗ Correspondingauthorat:RuaMiguelAntôniodaSilvaNeto,S/N,Aeroporto,59607-030Mossoró,RN,Brazil. E-mailaddress:[email protected](T.A.A.d.M.Fernandes).
http://dx.doi.org/10.1016/j.bjhh.2015.03.013
Introduction
Sicklecelldisease(SCD)isoneofthemostcommonsevere monogenicdisordersworldwide.1 Theunderlyingmolecular
defectisasinglenucleotidesubstitution(S–HBB;GAG>GTG; glu→val;rs334)inthegenethatencodesthe-globinchain ofhemoglobin.TheresultinghemoglobinS(HbS)polymerizes whendeoxygenated,causing polymer-associatedlesions of theredbloodcells.1,2SCDincludesseveraldifferentgenotypes
includingsicklecellanemia(HbSS)andcompound heterozy-gotesofHbSwith-thalassemia(HbS/-thal)orwithother typesofhemoglobinopathies.3
TheWorldHealthOrganizationrecognizedSCDasaglobal publichealthproblem,astheoverallnumberofbabiesborn withSCDbetween2010and2050isestimatedatabout14.24 million.4 Data from the Ministry of Health estimates that
around3500childrenarebornwithsicklecellanemiaeach year in Brazil and the number of cases of the disease is between25,000and30,000.5
Thecomplicationsofthisdiseasearenumerousandcan affecteveryorganandtissueinthebody.Themostcommon complicationsarepaincrises,chronicanemiaanditsacute exacerbations,stroke,acutechest syndrome,infection, pri-apism,legulcerations,osteonecrosis,andcardiacandrenal problems.6Complicationscanbeacute,producingdramatic
clinicalfindings,orchronic,disabling,andcausepremature death.2
Specificphenotypicmanifestationsofthediseasevary con-siderablyinfrequencyandseveritybetweenpatientsandeven inthesamepatientovertime.6Bothgeneticandacquired
fac-torscontributetothisclinicalvariation.Amongtheacquired factors,the mostimportant isthe patient’s socioeconomic conditions.7
Knowledgeofthedemographicandsocioeconomicprofile ofSCD patientsisessentialtoidentifytheirneeds,to con-tributeto improving resource allocation and tocreate and implementpublichealthpoliciesthatbenefitthispopulation.8
However,studiesthat address theseaspectsofthe disease arerelatively scarceinboththeBrazilianandinternational literature.
Thus,thisstudy aimedtocharacterizethedemographic andsocioeconomicaspectsofSCDpatientsfromthestateof RioGrandedoNorte(RN),asocioeconomicvulnerableareaof northeasternBrazil,andtheiradherencetotherecommended treatment.
Methods
Across-sectionaldescriptive studywasperformed at refer-ralcentersforthetreatmentofhematologicaldiseasesinRN: HemocentroDalton Cunha (Natal), Hospital Infantil Varela Santiago(Natal),andtheCentrodeOncologiaeHematologia deMossoró(Mossoró).TheparticipantswereunrelatedSCD patientswithout cognitive impairment,who went tothese centersfromMarch2011toOctober2013foroutpatientvisits. Allthepatients,ortheircaregivers,wereinformedabout theresearchproceduresandobjectives,andthosewhoagreed toparticipateinthestudysignedaninformedconsentform andansweredastandardizedquestionnaire.Whenthepatient
wasyoungerthan18yearsold,itwasansweredbythe care-giver.
Thequestionswereorallyaskedbytheinterviewer with-outinducingresponses.Questionsaimedtocollectmedical historyandthedemographicandsocioeconomicdataofthe patient,includingage,ethnicity,ancestry,residence, school-ing,employmentsituation,familyincome,ageatdiagnosis, use ofhydroxyurea, prophylactic penicillin, immunization, anddifficultiesinfollowingtreatment,amongothers. Clini-callyrelevantdatawerealsotakendirectlyfromthepatient’s healthrecords.
Data were collected in singleindividual interviews, and aftercollectiontheywereinputinto aMicrosoft Excel2010 spreadsheet.Frequencydistributiontableswereusedforthe descriptive analysisofthe categoricalor nominalvariables andthesignificanceofdifferencesbetweenclinical character-isticsbyagegroupwereestimatedusingtheChi-squared(2)
orFisherexacttest,asappropriate.Thecomparisonoftheage atdiagnosisofSCDinagegroupsemployedtheKruskal–Wallis analysisofvariance(ANOVA)test,followedbymultiple com-parisonsofmeanranks,usingtheStatisticasoftware(version 7).Differenceswithap-value≤0.05wereconsidered statisti-callysignificant.
ThisstudywasconductedinaccordancewiththeHelsinki Declaration as revised in 2008, and was approved by the Research Ethics Committeeofthe Universidade Federaldo RioGrandedoNorte(UFRN,underprotocolnumber 193/09) accordingtoresolution196/96ofthe ConselhoNacionalde Saúde,Brazil.
Results
Onehundredandseventy-sevenpatientswithclinicaland lab-oratorydiagnosisofSCDwereinterviewed.However,22were first-orsecond-degreerelativesofotherpatientsparticipating inthestudyandwerethereforeexcludedfromtheanalysis. Amongtheremaining155individuals,109(70.3%)hadHbSS, 23(14.8%)wereheterozygousforHbSand-thalassemia,21 (13.5%)wereheterozygousforHbSandHbC,andtwo(1.3%) presentedtheassociationbetweenHbSandhereditary per-sistenceoffetalhemoglobin(HPFH).
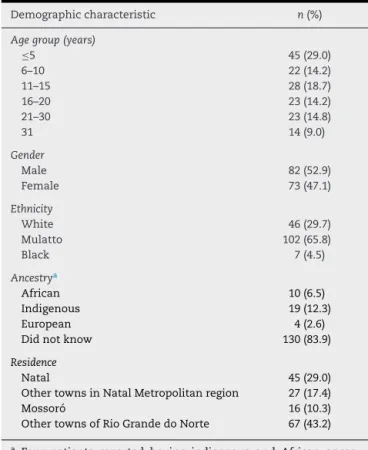
Theagesofthepatientsrangedfromsevenmonthsto48 years,withamedianageof12years;thehighestfrequency ofindividualswasintheagegroup≤5years(29.0%),followed bythe11-to15-year-oldgroup(18.7%).Themajorityofthe individualswere male(52.9%),andself-declaredasmulatto (65.8%), but with noinformation about their ethnic ances-try (83.9%).However,indigenousancestrywaspredominant (12.3%)amongpatientswhoinformedtheirancestry.Ahigh percentageofthepatients(43.2%)livedinsmalltowns,atleast 60kmawayfromthereferralcenters(Table1).
Table1–Demographiccharacteristicsofsicklecell diseasepatients.
Demographiccharacteristic n(%)
Agegroup(years)
≤5 45(29.0)
6–10 22(14.2)
11–15 28(18.7)
16–20 23(14.2)
21–30 23(14.8)
31 14(9.0)
Gender
Male 82(52.9)
Female 73(47.1)
Ethnicity
White 46(29.7)
Mulatto 102(65.8)
Black 7(4.5)
Ancestrya
African 10(6.5)
Indigenous 19(12.3)
European 4(2.6)
Didnotknow 130(83.9)
Residence
Natal 45(29.0)
OthertownsinNatalMetropolitanregion 27(17.4)
Mossoró 16(10.3)
OthertownsofRioGrandedoNorte 67(43.2)
a Four patientsreported havingindigenousandAfrican
ances-try,threereportedindigenousandEuropean,andonereported AfricanandEuropeanancestry.
thegovernment.Amongthosewhodidreceivebenefits,the Program of Continuous Cash Benefit for Social Assistance (BPC-LOAS)wasthemostprevalent(37.4%–Table2).
Themedian age atdiagnosis ofSCD was eight months (minimum: one month; maximum: eight years), two years (minimum:onemonth;maximum:14 years)andfiveyears (minimum:onemonth;maximum:47years)forindividualsin theunder11-year-old,11-to20-year-old,andover20-year-old agegroups,respectively.Astatisticallysignificantdifference wasobservedinthemedianageatdiagnosisofSCDbetween agegroups(Figure1).
60
50
40
30
P<.0001∗ P<.0001∗
P=.0001∗ P<.06812∗
20
10
0
≤10 11-20
Age of diagnosis (years)
Age group (years)
≥21
Figure1–Medianageatdiagnosisofsicklecelldisease stratifiedbyagegroup.
Table2–Socioeconomiccharacteristicsofthepatients withsicklecelldiseaseanalyzedinthisstudy. Socioeconomic
characteristic
Numberofpatients(%)
<18yearsa ≥18years Total
Schoolinga
NeverStudied 5(4.8) 3(5.8) 8(5.2) Incomplete
primaryschool
35(34.0) 15(28.8) 50(32.3)
Complete primaryschool
26(25.2) 9(17.3) 35(22.6)
Complete secondary education
31(30.1) 24(46.1) 55(35.5)
Complete higher education
3(2.9) 1(1.9) 4(2.6)
Didnotanswer 3(2.9) – 3(1.9)
Employmentsituationa
Working 57(55.3) 14(26.9) 71(45.8) Notworking 22(21.4) 26(50.0) 48(31.0) Other 24(23.2) 12(23.0) 36(23.2)
HouseholdIncome(Brazilianminimumwage) Upto1 81(52.3) From1to2 13(8.4) From2to3 53(34.2) Morethan3 8(5.2)
Benefitsfromthefederalgovernmentb
BPC-LOAS 58(37.4) Family
allowance
51(32.9)
Others 8(5.2)
Didnotreceive socialbenefits
53(34.2)
a Theschoolingandemploymentsituationofthecaregiverswas
considered.
b 15patientsreceivedbothProgramofContinuousCashBenefitfor
SocialAssistance(BPC-LOAS)andfamilyallowance.
Themajorityofthepatients(50.3%)reportedhaving diffi-cultiesfollowingtherecommendationsofthephysicians,in particulardifficultiestoacquiretheprescribedmedications, especially hydroxyurea, and transportation to the referral centerswhenneeded(Table3).
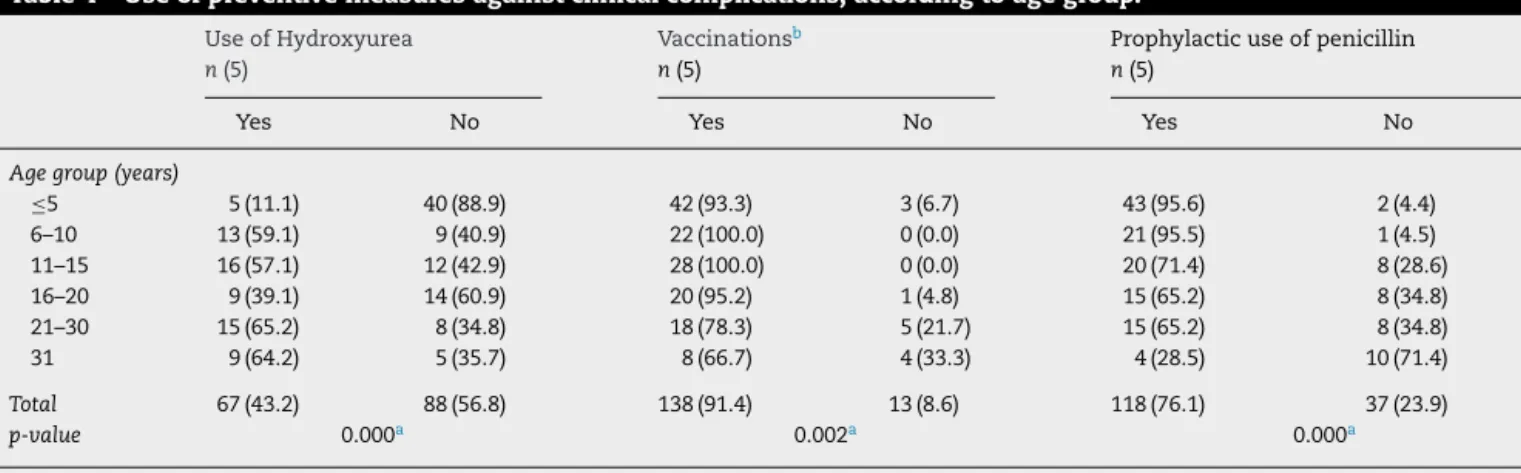
Regarding the use of preventive measures against clin-ical complications, it was observed that hydroxyurea was
Table3–Majordifficultiesreportedbypatientstofollow prescribedtreatment.
Treatmentdifficulty n(%)
Achievetheprescribedmedication 49(31.6)
Transporttoreferralcenters 27(17.4)
Others 13(8.4)
Didnothavedifficulties 77(49.7)
Table4–Useofpreventivemeasuresagainstclinicalcomplications,accordingtoagegroup. UseofHydroxyurea
n(5)
Vaccinationsb n(5)
Prophylacticuseofpenicillin n(5)
Yes No Yes No Yes No
Agegroup(years)
≤5 5(11.1) 40(88.9) 42(93.3) 3(6.7) 43(95.6) 2(4.4) 6–10 13(59.1) 9(40.9) 22(100.0) 0(0.0) 21(95.5) 1(4.5) 11–15 16(57.1) 12(42.9) 28(100.0) 0(0.0) 20(71.4) 8(28.6) 16–20 9(39.1) 14(60.9) 20(95.2) 1(4.8) 15(65.2) 8(34.8) 21–30 15(65.2) 8(34.8) 18(78.3) 5(21.7) 15(65.2) 8(34.8) 31 9(64.2) 5(35.7) 8(66.7) 4(33.3) 4(28.5) 10(71.4)
Total 67(43.2) 88(56.8) 138(91.4) 13(8.6) 118(76.1) 37(23.9)
p-value 0.000a 0.002a 0.000a
p-valueComparisonoftheuseofpreventivemeasuresamongtheagegroupscalculatedbyFisherExacttest. a Statisticallysignificant.
b Pneumococcal/meningococcalvaccinations(Fourpatientsdidnotrememberiftheyhadeverreceivedpneumococcalvaccinations).
regularlyusedby43.2%ofthepatients,withthispercentage being significantly lower in the youngest age group. Fur-thermore,itwasfoundthatthemajority(91.4%)ofpatients reportedhavingreceivedpneumococcal/meningococcal vac-cinations and penicillin as antibiotic prophylaxis (76.1%). However,thesepercentagesweremuchlowerintheoldestage groupanditwasnotpossibletoverifywhetherthevaccination wascompleteorincompleteforallpatients(Table4).
Discussion
SCD is achronic, degenerative and self-incapacitating dis-easeaffectingthepatientandtheirfamilyinanintenseand permanent way. The clinical complications and the recur-renthospitalizationsandbloodtransfusions,associatedwith externaldomainssuchasunemployment,lowincome,and lackofaccesstohealthservices,negativelyinfluencethelife ofthispopulation.7
Peopleinavulnerablesocioeconomicsituation aremore exposed to the determining social factors of the disease, which can lead to an aggravation of the patients’ general health.Therefore,theseindividualsdeservespecialattention inrespecttomedicalandpsychosocialperspectives.9
RioGrandedoNorteisalow-incomeareaofBrazil, hav-ingaHumanDevelopmentIndexof0.684(16thofallBrazilian states),10anilliteracyrateof19.8%,andachildmortalityof
17.0%.Moreover,62.6%offamilieshaveamonthlypercapita incomeofuptooneminimumwage(aboutUS$240.00).11
Inthisstudy,patientswerepredominantlyyoungerthan 12years,self-declaredasmulattoandlivingintownsfairly distant from referral centers for the treatment of SCD. Additionally,morethanonethirdofthepatients,ortheir care-givers,hadonlyfinishedelementaryschool,werenotworking, hadaverylowhouseholdincome,andwerenotreceivingany socialbenefitsfromthegovernment.
Theagegroupprofileofthisstudywassimilartothatfound byMaximo12inRiodeJaneiro,Brazil.Thepredominanceof
childrenandadolescentsseemstodemonstratetheseverity ofthedisease,withpatientspresentinglowlifeexpectancy, despiteimportantadvancesthatemergedinthelastdecades
forthepreventionandtreatmentofcomplicationsofthe dis-ease.
Thepredominanceofmulattoesamongpatientsisrelated to theethnic background ofthe populationofthe stateof RioGrandedoNorte accordingtothe BrazilianInstituteof Geography and Statistics (IBGE),11 where the influence of
AfricanslaveswasnotsostrongasinsomeotherBrazilian states.13Thepredominanceofindigenousancestryamongthe
patientswhoinformedanyancestrycorroboratesthis hypoth-esis.However,manystudiesworldwidehaveshownthatSCD is more common in individuals ofblack ethnicity, that is, Africandescent.5,14Therefore,itislikelythatthedistribution
ofthisself-reportedethnicitymayhavebeeninfluencednot onlybythehighdegreeofmiscegenation,butalsobyacertain degreeofbiasoftheindividualsanalyzed,whooftenpreferto declarethemselvesasmulattoesinsteadofBlacks.
The low education level and socioeconomic status of the patients were similar to those found in studies con-ductedinEngland,15theUSA,16Nigeria17andotherstatesof
Brazil.7,8,18,19Thisgeneratesaconditionofsocial
vulnerabil-itythataffectsthequalityoflifeofpatientsandmakesthem moredependentongovernmentprogramsforfinancial bene-fitsand healthcare.Additionally,onethirdoftheanalyzed patients were notreceiving any social benefits,asituation thatimpairstheirlivingconditionsevenfurther.These vul-nerableconditionsalsoinfluenceadherencetothetreatment recommendedbythephysician.20
Despite the complexity and multifactorial pathophysi-ology of the disease, relatively straightforward measures have greatly improved outcomes for children with SCD. SuchmeasuresincludeearlyidentificationofSCDby neona-tal screening programs and the prompt establishment of preventivemeasureswithprophylacticpenicillinand immun-izations,andtherapeuticinterventions,suchastransfusions andhydroxyurea.21
ishigherthan that reportedbyother studies conductedin Brazil18,22 and the USA,23,24 and demonstratesgood
adher-enceofthepatientstotreatmentandthehealthcareteam’s confidence in the efficacy of the medicine. However, only 11% ofunder 5-year-old childrenwere takinghydroxyurea, whichseemstoreflecttheconcernsabouttheoverallsafety ofthismedicine,mainlyinveryyoungchildren.Theresultsof thePediatricsHydroxyureaPhase3ClinicalTrial(BabyHUG) demonstrated bothsafety and beneficial effectsof hydrox-yureainasymptomaticandsymptomaticyoungchildrenwith SCA,andsuggeststhatcliniciansshouldconsiderchanging theirpracticetoprescribe hydroxyureatherapy forallvery youngchildrenwithSCA,ratherthantreatingonlythosemost severelyaffected.25
Theratesofvaccination (91.4%)andprophylacticuse of penicillin(76.1%)foundinthisstudyalsodemonstrategood adhesionofhealthstaffandpatientstogeneral recommen-dations forthe treatment of SCD. Improved immunization against Streptococcus pneumoniae and Haemophilus influenza, and the use of penicillin prophylaxis have dramatically reducedthefrequencyofseriousbacterialinfectionsand mor-talityofinfantswithSCA.26,27
ThisimmunizationcoverageofpatientswithSCDwas sim-ilartothoseobtainedbyFrauchesetal.28inthestateofEspírito
Santo,Brazil,andbyHardieetal.29inpatientsfromJamaica.
On the other hand, the prophylactic use ofpenicillin was higherthantheratereportedbyWarrenetal.30intheUSA,
andsimilartothosedescribedinothersstudiescarriedoutin Brazil31andJamaica.32Howeveritwasnotpossibletodirectly
assessthevaccinationrecordcardofallindividuals,nor ver-ifyadherencetoprophylacticpenicillinbyothermethods;it ispossiblethatourresultsareoverestimated.Lowerratesof adherencetothesepracticesintheolderagegroupscanbe explainedbythefactthattheserecommendationswere estab-lishedinthe1980sand1990s.
Despitethis adherence totreatmentand use of preven-tive measures, a significant percentage (31.6%) ofpatients reportedproblemsinachievingtheprescribed medications, especiallyhydroxyurea.Thehighcostsofthesemedicinesand lowsocioeconomicstatusofpatientsmakethemdependent onpublicprogramsfordispensingmedicines.Therefore,the occurrenceoffinancialandadministrativeproblemsinthese programscanmakeaccesstotherecommendedtherapyquite difficult.
Thedistancetoreferencecentersconstitutesabarrierto the implementation of a comprehensive care program for SCDpatients,asitgenerallyrestrictstransportationtohealth services.33Addedtothis,theneedtotraveltogettreatment
endangers patients’ lives.Astudy conductedbyFernandes andViana34pointedoutdifficultiesingettingtransportation
tothehealthcenter asacontributingfactor forpremature deathsoftheseindividuals.Inourstudy,almosthalfofthe analyzedindividuals lived intowns fairlydistant from the referralcentersand17.4%reporteddifficultiesinarrivingat thecenterstoperformtherecommendedtreatment.
Therefore, it is necessary toimprove publicpolicies for theseindividuals,takingintoaccounttheirlowsocioeconomic status,demographiccharacteristics,anddifficultiesin achiev-ingtherecommendedtreatment.Andtobeeffective,these measuresneedtoprovidepsychosocialcounselingnecessary
forthedevelopmentofthepatient’sintegrationintosociety, as well as accessto medicaltreatment, allowingfavorable improvementsintherealityexperiencedbyBrazilianswith thisdisease.
Certainlimitations ofthecurrent studyshouldbetaken intoaccount,especiallywithregardtoadherencetothe rec-ommended medical treatment. As it was not possible to analyzethevaccinationrecordcardsofallpatients,wewere notabletoassesstheadequacyofthevaccineprogram. Fur-thermore,theuseofhydroxyureaandprophylacticpenicillin wasevaluatedtakingintoaccountonlythepatients’reports. Therefore,theirregularandproperuseofthesedrugscould notbeproven.
Conclusions
SCD patients from the state of Rio Grandedo Norte have a vulnerable socioeconomic situation that can lead to an aggravation oftheir generalhealthand thus deserves spe-cialattentionfromthemedicalandpsychosocialperspectives. Therefore, it is necessary to improve public policies that provide BrazilianswithSCDbetteraccesstomedical treat-ment,livingconditions,andintegrationintosociety.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgments
Thisstudy wassupportedbyConselhoNacionalde Desen-volvimento Científico e Tecnológico (CNPq, grant no. 402022/2010-6) and Fundac¸ão de Amparo à Pesquisa do Estado de São Paulo (FAPESP, grant no. 08/57441-0). We would liketothankthestaffofHemocentroDaltonCunha, HospitalInfantilVarelaSantiago,andCentrodeOncologiae HematologiadeMossorófortheaccessprovidedtopatients.
r
e
f
e
r
e
n
c
e
s
1.ReesDC,WilliamsTN,GladwinMT.Sickle-celldisease. Lancet.2010;376(9757):2018–31.
2.SteinbergM.Sicklecelldisease.In:SteinbergM,ForgetB, HiggsD,WeatheralD,editors.Disordersofhemoglobin– genetics,pathophysiologyandclinicalmanagement.2nded. Cambridge:CambridgeUniversityPress;2009.p.435–6.
3.SteinbergMH,SebastianiP.Geneticmodifiersofsicklecell disease.AmJHematol.2012;87(8):795–803.
4.PielFB,HaySI,GuptaS,WeatherallDJ,WilliamsTN.Global burdenofsicklecellanaemiainchildrenunderfive, 2010–2050:modellingbasedondemographics,excess mortality,andinterventions.PLoSMed.2013;10(7):e1001484.
5.Canc¸adoRD,JesusJA.Adoenc¸afalciformenoBrasil.RevBras HematolHemoter.2007;29(3):204–6.
7. PereiraSA,BrenerS,CardosoCS,ProiettiAB.Sicklecell disease:qualityoflifeinpatientswithhemoglobinSSandSC disorders.RevBrasHematolHemoter.2013;35(5):325–31.
8. SantosJP,GomesNetoM.Sociodemographicaspectsand qualityoflifeofpatientswithsicklecellanemia.RevBras HematolHemoter.2013;35(4):242–5.
9. PaivaeSilvaRB,RamalhoAS,CassorlaRM.Sicklecelldisease asapublichealthprobleminBrazil.RevSaudePublica. 1993;27(1):54–8.
10.Nac¸õesUnidasRankingIDHMUnidadesdaFederac¸ão2010. Availablefrom:http://www.pnud.org.br/atlas/ranking/ Ranking-IDHM-UF-2010.aspx[cited30.01.15].
11.InstitutoBrasileirodeGeografiaeEstatística–IBGE.Síntese deindicadoressociais–umaanálisedascondic¸õesdevidada populac¸ãobrasileira.RiodeJaneiro:IBGE;2014,214pp.
12.MaximoC[thesis]Thepolicyforcomprehensivecareof personswithsicklecelldiseaseinRiodeJaneiroandthe challengeofdecentralization.Riodejaneiro:Fundac¸ão OswaldoCruz–EscolaNacionaldeSaudePublica;2009, 104pp.
13.CascudoLC.HistóriadoRioGrandedoNorte.RiodeJaneiro: DepartamentodeImprensaNacional;1955.
14.BrousseauDC,PanepintoJA,NimmerM,HoffmannRG.The numberofpeoplewithsickle-celldiseaseintheUnitedStates –nationalandstateestimates.AmJHematol.2010;85(1):77–8.
15.AljuburiG,LavertyAA,GreenSA,PhekooKJ,BellD,MajeedA. Socio-economicdeprivationandriskofemergency
readmissionandinpatientmortalityinpeoplewithsicklecell diseaseinEngland:observationalstudy.JPublicHealth. 2013;35(4):510–7.
16.McCavitTL,LinH,ZhangS,AhnC,QuinnCT,FloresG. Hospitalvolume,hospitalteachingstatus,patient
socioeconomicstatus,andoutcomesinpatientshospitalized withsicklecelldisease.AmJHematol.2011;86(4):377–80.
17.AdegokeSA,AdeoduOO,AdekileAD.Sicklecelldisease clinicalphenotypesinchildrenfromSouth-Western,Nigeria. NigerJClinPract.2015;18(1):95–101.
18.FelixAA,SouzaHM.Epidemiologic,RibeiroS.B.socialaspects ofsicklecelldisease.RevBrasHematolHemoter.
2010;32(3):203–8.
19.LoureiroMM,RozenfeldS,PortugalRD.Acuteclinicalevents inpatientswithsicklecelldisease:epidemiologyand treatment.RevBrasHematolHemoter.2008;30(2):95–100.
20.ReinersAA,AzevedoRC,VieiraMA,deArrudaAL.
Bibliographicproductionaboutadherence/non-adherenceto therapy.CienSaudeColet.2008;13Suppl.2:2299–306.
21.McGannPT,NeroAC,WareRE.Currentmanagementofsickle cellanemia.ColdSpringHarbPerspectMed.2013;3(8),pii: a011817.
22.SilvaJuniorGB,LibórioAB,VieiraAP,BemAX,LopesFilhoAS, FigueiredoFilhoAC,etal.Evaluationofrenalfunctionin sicklecelldiseasepatientsinBrazil.BrazJMedBiolRes. 2012;45(7):652–5.
23.BrandowAM,JirovecDL,PenepintoJA.Hydroxyureain childrenwithsicklecelldisease–practicepatternsand barrierstoutilization.AmJHematol.2010;85(8):611–3.
24.ZumbergMS,ReddyS,BoyetteRL,SchwartzRJ,KonradTR, LottenbergR.Hydroxyureatherapyforsicklecelldiseasein community-basedpractices–asurveyofFloridaandNorth Carolinahematologists/oncologists.AmJHematol. 2005;79:107–13.
25.ThornburgCD,FilesBA,LuoZ,MillerST,KalpatthiR,IyerR, etal.ImpactofhydroxyureaonclinicaleventsintheBABY HUGtrial.Blood.2012;120(22):4304–10.
26.GastonMH,VerterJI,WoodsG,PegelowC,KelleherJ, PresburryG,etal.Prophylaxiswithoralpenicillininchildren withsicklecellanemiaArandomizedtrial.NEnglJMed. 1986;314(25):1593–9.
27.HalasaNB,ShankarSM,TalbotTR,ArbogastPG,MitchelEF, WangWC,etal.Incidenceofinvasivepneumococcaldisease amongindividualswithsicklecelldiseasebeforeandafter theintroductionofthepneumococcalconjugatevaccine.Clin InfectDis.2007;44(11):1428–33.
28.FrauchesDO,MatosPA,VatanabeJH,OliveiraJF,LimaAP, Moreira-SilvaSF.Vaccinationagainstpneumococcusin childrenwithsicklecellanemiainthestateofEspiritoSanto, Brazil,between2004and2007.EpidemiolServSaude. 2010;19(2):165–72.
29.HardieR,KingL,FraserR,ReidM.Prevalenceof
pneumococcalpolysaccharidevaccineadministrationand incidenceofinvasivepneumococcaldiseaseinchildrenin Jamaicaagedover4yearswithsicklecelldiseasediagnosed bynewbornscreening.AnnTropPaediatr.2009;29(3): 197–202.
30.WarrenMD,ArbogastPG,DudleyJA,KaltenbachL,RayWA, WangWC,etal.Adherlaticantibioticguidelinesamong Medicaidinfantswithsicklecelldisease.ArchPediatr AdolescMed.2010;164(3):298–9.
31.GomesLM,ReisTC,VieiraMM,deAndrade-BarbosaTL, CaldeiraAP.Qualityofassistanceprovidedtochildrenwith sicklecelldiseasebyprimaryhealthcareservices.RevBras HematolHemoter.2011;33(4):277–82.
32.KingL,AliS,Knight-MaddenJ,MooSangM,ReidM. Compliancewithintramuscularpenicillinprophylaxisin childrenwithsicklecelldiseaseinJamaica.WestIndianMed J.2011;60(2):177–80.
33.WolfsonJA,SchragerSM,KhannaR,CoatesTD,KipkeMD. SicklecelldiseaseinCalifornia:sociodemographicpredictors ofemergencydepartmentutilization.PediatrBloodCancer. 2012;58(1):66–73.