w w w . r b h h . o r g
Revista
Brasileira
de
Hematologia
e
Hemoterapia
Brazilian
Journal
of
Hematology
and
Hemotherapy
Original
article
Is
it
feasible
to
use
granulocyte-colony
stimulating
factor
alone
to
mobilize
progenitor
cells
in
multiple
myeloma
patients
induced
with
a
cyclophosphamide,
thalidomide
and
dexamethasone
regimen?
Edvan
de
Queiroz
Crusoe
a,∗,
Fabiana
Higashi
a,
Gracia
Aparecida
Martinez
b,
José
Carlos
Barros
a,
Marcelo
Bellesso
b,
Marina
Rossato
a,
Ana
Cinira
F.
Marret
a,
Carlos
Sérgio
Chiattone
a,
Vania
Tietsch
de
Moraes
Hungria
aaFaculdadedeCiênciasMédicasdaSantaCasadeSãoPaulo(FCMSCSP),SãoPaulo,SP,Brazil
bUniversidadedeSãoPaulo(USP),FaculdadedeMedicina,HospitaldasClínicas,InstitutodoCâncerdoEstadodeSãoPauloOctavio
FriasdeOliveira(ICESP),SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received4April2016 Accepted6June2016 Availableonline29July2016
Keywords:
Bonemarrowtransplantation Multiplemyeloma
Granulocyte-colonystimulating factor
Cyclophosphamide
a
b
s
t
r
a
c
t
Background:Cyclophosphamide plus thalidomide as induction for multiple myeloma patientseligibleforautologousstemcelltransplantationmaybealimitingfactorforcell mobilization.Theminimumacceptablemobilizedperipheralbloodstemcellcountto pre-ventdeleteriouseffectsduringtransplantationis2.0×106CD34+cells/kg.Combiningother treatmentstogranulocyte-colonystimulatingfactor,suchascyclophosphamide,could over-comethemobilizationlimitation.Theobjectiveofthisstudywastoassessthenumber ofCD34+ cellsmobilized usinggranulocyte-colony stimulatingfactor withand without cyclophosphamideafterinductionwithcyclophosphamide,thalidomideand dexametha-sone.
Methods:Aretrospectivestudywasperformedofacohortofmultiplemyelomapatients submittedtoautologousstemcelltransplantationsattwoBraziliancentersbetweenMay 2009andJuly2013.Theoralcyclophosphamideandthalidomideinductiondosesusedwere 1500mg/monthand100–200mg/day, respectively.Mobilizationdoses were10–15mcg/kg granulocyte-colonystimulatingfactorwith2–4g/m2cyclophosphamide,or15–20mcg/kg granulocyte-colonystimulatingfactoralonefor5days.Collectionof>2.0×106CD34+cells/kg wasconsideredsufficient.
Results:Eighty-eight patients were analyzed; only 18 received cyclophosphamide. The medianagewas58 yearsold(range:51–62)forthegranulocyte-colony stimulating fac-torgroupand56.5yearsold(range:54–60)forgranulocyte-colonystimulatingfactorplus
∗ Correspondingauthorat:DepartamentodeHematologiaeOncologia,FaculdadedeCiênciasMédicasdaSantaCasadeSãoPaulo
(FCMSCSP),RuaDr.CesárioMottaJr.,61,01221-020SãoPaulo,SP,Brazil. E-mailaddress:[email protected](E.Q.Crusoe).
http://dx.doi.org/10.1016/j.bjhh.2016.06.004
cyclophosphamidegroup.Fifty-twopatientsweremale.Eightycases(90.9%)were Durie-Salmon StagingSystem III-A/B and38 (44.7%) and20 cases (23.5%)wereInternational StagingSystem2and3,respectively.Thegroupthatreceivedcyclophosphamidecollected a highermediannumberofprogenitorcells[3.8(range:3.1–4.4)vs. 3.2(range:2.3–3.8)] (p-value=0.008).Nocorrelationwasobservedbetweenbetterresponsesornumberof induc-tioncyclesandthenumberofcellscollected.
Conclusion:Thenumberofcellsmobilizedwithgranulocyte-colonystimulatingfactorplus cyclophosphamidewashigher.However,inbothgroups,themediannumberofCD34+cells wassufficient toperforma singleautologousstem celltransplantation;nodeleterious effectswerereportedduringharvesting.
©2016Associac¸ ˜aoBrasileiradeHematologia,HemoterapiaeTerapiaCelular.Published byElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Theuseofhigh-dosechemotherapyplusautologousstemcell transplantation(ASCT)asconsolidationafterchemotherapy inductionhasbeenthefirstlineoftreatmentforeligible mul-tiple myeloma patients for over three decades.1 Currently, themost commonlyemployedinductionstrategy istouse a number of cycles (4–6) with three drugs.1 The introduc-tion of triple combinations of novel agents for induction, suchas the immunomodulators thalidomideand lenalido-mideortheproteasomeinhibitorbortezomib,hassignificantly changedasthesedrugsresultedinbetteroutcomesand tol-erability comparedto classicregimens suchas vincristine, doxorubicinanddexamethasone(VAD).1However,the induc-tion regimens should not affect hematopoietic progenitors in the mobilization process.2–6 Recently, this influence on mobilizationhasbeengainingincreasedattentionduetothe use of chemotherapy combinations involving novel agents suchasimmunomodulators(lenalidomide)and,in particu-lar,alkylatingagents(cyclophosphamide)whichcanincrease hematologictoxicity.2,6Auneretal.2foundthatthe combina-tionofcyclophosphamide,thalidomideanddexamethasone (CTD)intheinductionofpatientswithmultiplemyeloma sig-nificantlyreducedmobilizationofprogenitorcellscompared tothe classicVAD orVAD-likeregimens, evenwhenusing cyclophosphamide inassociation with granulocyte colony-stimulatingfactor (G-CSF)duringmobilization. In aneffort to overcome this mobilization problem, other agents have beenassociatedwithG-CSF,mostnotablyplerixafor.7 How-ever, the high cost of plerixafor limits its use in many centers. Chemotherapy associated with G-CSF can signifi-cantlyincreasethe mobilizationofprogenitorcells.Oneof themostusedchemotherapydrugsinmobilizationbasedona combinationwithG-CSFiscyclophosphamide,administered ata typicaldose of2–4g/m2.8 However,thistreatment has somedrawbacks giventhat itraises the costofthe proce-dureowingto theneed forhospitalizationofpatients and canleadtoslowerbonemarrowengraftment,greater toxic-itywithpancytopenia,neutropenia,infectionsanddeath.9–12 Thenumber ofCD34+ collected forASCT depends on sev-eralfactorsthemostimportantofwhicharethenumberof transplantations planned and the leastimpact interms of
timeonthemobilizedperipheralbloodstemcells. Tradition-ally,thetargetforCD34+ cellcollectionforsingleASCThas been 4–6×106cells/kg, with the value also hinging on the deleteriousimpactofharvesting atcountsofbelow2×106 CD34+cells/kg,definedasthelowestacceptablelevel.3Greater numbersofCD34+cellshavenotbeenassociatedwithany sig-nificantbenefitintheparametersstudied.6Anotherobjective inthequantityofcellsmobilizedistoallowforacellreserve forasecond ASCTasrescueintheevent offuture disease relapse,renderingthetargetcellcountinthefirstmobilization ≥4×106CD34+ cells/kg.8,13 SomepeculiaritiesexistinBrazil whichhampertheuseofASCTsuchaslownumberofbeds fortransplantationsand theshortageoffrozencellstorage forsecondtransplantswithintheBrazilianNational Health System(SUS).Thethree-druginductionregimenwidelyused inBrazilformultiplemyelomapatientsiscyclophosphamide, thalidomideanddexamethasone(CTD).14Theprimary objec-tiveofthis study was todeterminewhether the collection of progenitor cells using G-CSF alone is sufficient to per-formatleastoneASCT,comparedwithagroupundergoing mobilizationwithG-CSFassociatedwithcyclophosphamide, inpatientssubmittedtotheCTDchemotherapyregimenfor induction.
Methods
(2–4g/m2splitin2doses)associatedwithG-CSF(10–15mcg/kg until the collection of cells), and Group 2 received G-CSF (15–20mcg/kgfor5days)alone.Allpatientsweresubmitted toanoutpatientmobilizationprotocol.TheCD34+ cellcount for collection was determined by flow cytometry using a FACSCaliburBDdevicewithdoubleplatformandemploying thecellquestprogramandISHAGEprotocol.Apheresiswas performedaccordingtotheCD34+countinperipheralblood (≥10×103/mL)startingbetweenDay7and10inGroup1and Day4and10inGroup2,withthemediandayofcollection beingDays7and4aftercommencingG-CSFforGroups1and 2,respectively.Thepatientsweresubmittedtoalargevolume leukapheresisprotocolwithamedianoffourblood volume apheresis (range: 3–6). The Cobe® Spectra Marc Terumo BCTapheresissystemwasusedinbothcenters.CD34+ cell collectionwasconsideredadequatewithacount≥2.0×106 CD34+ cells/kg. Asthe CD34+ cells forthe transplants had comefrompatientswhohadtheircellscollectedpreviously, itwasnotpossibletoanalyzedataonfailureofmobilization. Progression-freesurvival(PFS)andoverallsurvival(OS)were analyzed.PFSwasdefinedasthetimeelapsedbetweenthe startofinductiontreatmenttodiseaseprogressionordeath, withcensureonthedateoflastcontact.OSwasdefinedasthe timeelapsedbetweenthestartofinductiontreatmentuntil death,withcensureonthedateoflastcontact.Theunpaired
t-testwasusedtocomparemeansofvariableswithanormal distribution,whereastheMann–Whitneytestwasemployed tocomparevariableswithanon-normaldistribution. Cate-gorical variables, including response rates, were compared using the Chi-square or Fisher exact tests, as applicable. Survivalanalyseswere carried out using the Kaplan–Meier technique whilethe comparisonbetween groups was per-formedwiththelogranktest.Medianfollow-upforOSwas calculatedusingthereverseKaplan–Meiermethod.Analyses were carried out using the MedCalc software (Mariakerke, Belgium,v.11.3.3.0).Valueswithatwo-tailed p-value<0.05 wereconsidered statisticallysignificant.Thestudyprotocol wasapprovedbybothinstitutions,withdatacollectedfrom a database derived from the Grupo Brasileiro de Mieloma Múltiplo(GBRAM003)study.Thisstudywasapprovedbythe ResearchEthicsCommitteeoftheHospitaldaIrmandadeda SantaCasadeMisericórdiadeSãoPauloandaconsentform waswaivedgiventheretrospectivenatureofthestudy.
Results
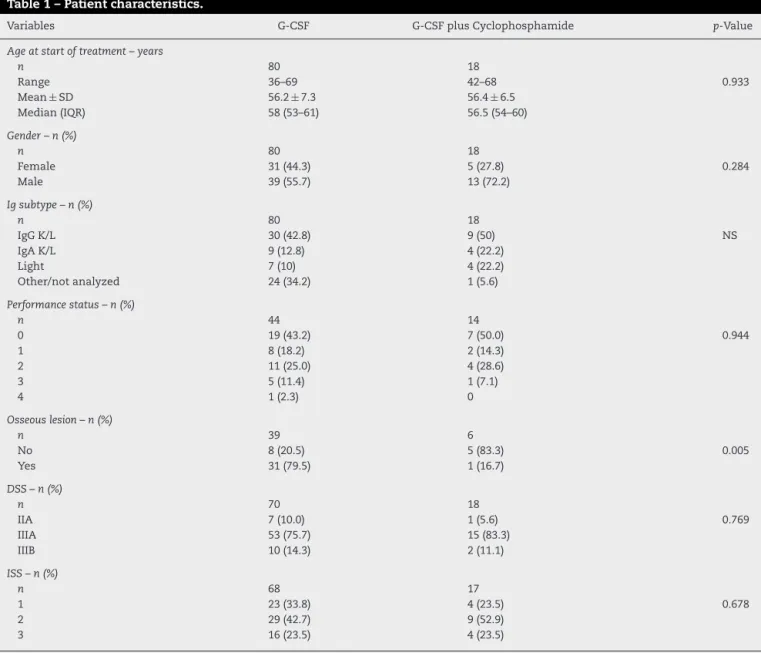
Demographicandbaselineclinicalcharacteristicsof patients
Atotalof88patients withmultiplemyelomasubmitted to ASCTafterinductionusingCTDwereincluded.Regardingthe mobilization scheme, 70 patients receivedfilgrastim alone, and18receivedacombinationoffilgrastimand cyclophos-phamide.Themaindemographicandclinicalcharacteristics ofthe88patientsstratifiedbymobilizationschemeareshown inTable1.Thegroupsdidnotdifferinrespecttoage(median: 58;range:51–62years)orgenderandthegroupswerebalanced in terms ofperformance status or prognostic index using the Durie-Salmon Staging System (DSS) and International
StagingSystem(ISS).Table2depictsthedistributionofthe mainlaboratoryvariablesatthetimeofdiagnosis.No signif-icantdifferencewasfoundbetweenthegroupsforanyofthe variablesstudied.Giventheretrospectivenatureofthestudy, therewasalargeamountofmissingdataforsomevariables (totalcalcium,ionizedcalcium,creatinine,lactate dehydroge-nase(LDH),Beta-2microglobulin)inthegroupsubmittedto mobilizationusingG-CSFalone.
Mobilizationofprogenitorcells
ThedataonthenumberofCD34+collectedwasavailablefor allpatients,whereasthenumberofdaysofapheresisrequired forcollectionwasavailableforonly77cases.Thegroup receiv-ingG-CSFaloneharvestedameanof3.4±1.3×106/kganda medianof3.2×106/kg(range:2.3–3.8×106/kg)ofCD34+cells. Onthe otherhand,thegroupthatreceivedfilgrastim com-binedwithcyclophosphamideharvestedahighernumberof progenitorcellswithameanof6.4±7.7×106/kgandmedian of3.8×106/kg(range:3.1–4.4×106/kg)(p-value=0.008).No sig-nificantdifferenceinthenumberofdaysforcollectionwas observedbetweenthegroups(p-value=0.077).Asummaryof thenumberofcellsmobilizedanddaysofapheresisforthe twogroupsisshowninTable3.
Pre-transplantresponserates,numberofchemotherapy cycles,quantityofcellsmobilizedandadverseevents relatedtothemobilizationprotocol
The mobilizedCD34+-cell countwasnot influenced bythe number of chemotherapy cycles administered, nor by the responseratepriortoASCT(Figure1andTable4).Noadverse eventswere recordedinthedatabaseregister forthegroup thatreceivedcyclophosphamideassociatedwithG-CSF.
Overallsurvivalforthetwogroups
Atthe time ofanalysis, 39 ofthe 88patients had suffered diseaseprogression,andfourhaddied.Themedianfollow-up was 28.6 months and the overall PFS was 24 months. No significant difference was found between the two groups. MedianPFSwas25.7monthsfortheG-CSFalonegroupand the PFS had notbeen attainedfor the groupthat received
40
0 2 4 6 8
P=.390
Number cycles
CD34
10 12 14
35
30
25
20
15
10
5
0
Table1–Patientcharacteristics.
Variables G-CSF G-CSFplusCyclophosphamide p-Value
Ageatstartoftreatment–years
n 80 18
Range 36–69 42–68 0.933
Mean±SD 56.2±7.3 56.4±6.5
Median(IQR) 58(53–61) 56.5(54–60)
Gender–n(%)
n 80 18
Female 31(44.3) 5(27.8) 0.284
Male 39(55.7) 13(72.2)
Igsubtype–n(%)
n 80 18
IgGK/L 30(42.8) 9(50) NS
IgAK/L 9(12.8) 4(22.2)
Light 7(10) 4(22.2)
Other/notanalyzed 24(34.2) 1(5.6)
Performancestatus–n(%)
n 44 14
0 19(43.2) 7(50.0) 0.944
1 8(18.2) 2(14.3)
2 11(25.0) 4(28.6)
3 5(11.4) 1(7.1)
4 1(2.3) 0
Osseouslesion–n(%)
n 39 6
No 8(20.5) 5(83.3) 0.005
Yes 31(79.5) 1(16.7)
DSS–n(%)
n 70 18
IIA 7(10.0) 1(5.6) 0.769
IIIA 53(75.7) 15(83.3)
IIIB 10(14.3) 2(11.1)
ISS–n(%)
n 68 17
1 23(33.8) 4(23.5) 0.678
2 29(42.7) 9(52.9)
3 16(23.5) 4(23.5)
G-CSF:granulocyte-colonystimulatingfactor;SD:standarddeviation;IQR:interquartilerange;DSS:Durie-SalmonStaging;ISS:International StagingSystem.
associatedcyclophosphamide(Figure2).Similarly,no
differ-encewasobservedbetweenthetwogroupsforOS.MedianOS hadnotbeenattainedineitherofthegroups.Thehazardratio forOSwas0.65(95%confidenceinterval:0.18–2.27)favoring thecyclophosphamideregimenbutnotreachingsignificance (p-value=0.495)(Figure3).
Discussion
Theaimofthe present study was to analyzethe quantity ofmobilized progenitorcells with the use ofG-CSF alone orincombinationwiththechemotherapyagent cyclophos-phamide,inpatientswithnewlydiagnosedmultiplemyeloma submittedtochemotherapyinductionusingtheCTDprotocol. Thisisthe firstanalysisofitskind publishedinthe litera-ture.Thetargetquantityofmobilizedcells differsbetween centersassomeplandoubleASCT,orallowforthefreezingof somecellsforasecondtransplantintheeventofrelapsewhile
Table2–Laboratoryvariables.
Variable G-CSF G-CSFplusCyclophosphamide p-Value
Hemoglobin–g/dL
n 66 18
Mean±SD 9.6±2.5 9.7±1.6 0.972
Creatinine–mg/dL
n 54 18
Mean±SD 1.2±0.8 1.5±1.4 0.443
Median(IQR) 0.9(0.7–1.5) 1.05(0.8–1.5)
Totalcalcium–mg/dL
n 49 18
Mean±SD 9.9±1.6 10.2±1.7 0.099
Median(IQR) 9.3(9.0–10.1) 9.75(9.6–10.6)
Ionizedcalcium–mol/L
n 22 17
Mean±SD 5.6±2.0 5.5±0.7 0.955
Median(IQR) 5.3(4.9–6.5) 5.3(5.2–5.6)
ˇ2-microglobulin–mg/L
n 51 17
Mean±SD 4.3±3.2 7.3±7.1 0.128
Median(IQR) 3.3(2.2–5.4) 3.8(3.0–7.5)
C-reactiveprotein–mg/dL
n 29 15
Mean±SD 13.6±25.5 22.8±50.2 0.063
Median(IQR) 2.3(0.4–11.9) 7.2(3.3–16.2)
LDH–U/L
n 27 18
Mean±SD 278±193 335±181 0.320
Albumin–g/dL
n 45 18
Mean±SD 3.6±0.7 3.5±0.6 0.840
Mcomponent–g/dL
n 25 18
Mean±SD 3.6±2.2 4.9±3.1 0.136
Plasmocytes–%
n 55 18
Mean±SD 40.7±27.0 41.0±32.4 0.960
G-CSF:granulocyte-colonystimulatingfactor;LDH:lacticdehydrogenase;Mcomponent:monoclonalcomponent.
multiplemyelomaeligibleforASCTvariesbetweencenters
worldwideintermsoftypeand combinationofthe agents
employed.Thereisastrong,almostuniversal tendencyfor
theuseofnovelagentssuchasbortezomib,lenalidomideand
thalidomide,ascombinationsorwithcorticosteroidsand/or
alkylatingagents.18–21Theuseofacombinationofthreedrugs
ininductionasopposedtotwodrugsyieldsgreaterbenefitsin responseandsurvival.1InBrazil,theonlyagentavailablefor
Table3–QuantityofmobilizedcellsanddaysofapheresisfortheG-CSFandG-CSFpluscyclophosphamidemobilization regimens.
Variable G-CSF G-CSF/Cyclophosphamide p-Value
Cellcount–×106/kg
n 70 18
Mean±SD 3.4±1.3 6.4±7.7 0.008
Median(IQR) 3.2(2.3–3.8) 3.8(3.1–4.4)
Apheresis–days
n 60 17
Mean±SD 1.5±0.6 1.2±0.5 0.077
Median(IQR) 1(1–2) 1(1–1)
Table4–Relationshipbetweenresponsetypeoninductionandnumberofmobilizedcells.
Responsetypeandtimepoint Response Noresponse p-Value
Afterfourcycles≥PR
Cellcount–×106/kg n=74 n=14
Mean±SD 4.2±4.1 3.1±0.8 0.176
Median(IQR) 3.35(2.7–4.0) 3.15(2.3–3.3)
Pre-aHSCT≥PR
Cellcount–×106/kg n=80 n=8
Mean±SD 4.1±4.0 3.3±0.8 0.780
Median(IQR) 3.3(2.6–4.05) 3.3(2.95–3.55)
Afterfourcycles≥VGPR
Cellcount–×106/kg n=36 n=52
Mean±SD 5.0±5.6 3.4±1.4 0.228
Median(IQR) 3.35(2.95–5.25) 3.3(2.35–3.8)
Pre-aHSCT≥VGPR
Cellcount–×106/kg n=47 n=41
Mean±SD 4.6±5.0 3.4±1.5 0.135
Median(IQR) 3.4(3.025–4.275) 3.2(2.3–3.825)
aHSCT:autologoushematopoieticstemcelltransplantation;PR:partialresponse;VGPR:verygoodpartialresponse.
useinthepublichealthsystemisthalidomide.Thebest
com-binationidentifiedandwidelyusedinBraziliancentersisthe
CTDprotocol.Currently,centersindevelopedcountries
pre-fertouseotherdrugsforinductionhowever,combinations
withthalidomidearestillinuseinBrazilandinother
devel-opingcountries.Thisprotocolwascomparedinarandomized
phaseIIIstudyagainsttheVADpluscyclophosphamide
regi-meninover1000patientswiththeCTDarmprovidingbetter
responserates.20Thepatientsstudiedinthepresent
inves-tigation were selected from two national centers that use differentprotocols forthe use ofcyclophosphamide. How-ever,the finalmonthlydose (1500mg)isthe sameinboth: Center1usesacontinuousdailyoraldoseof50mg;Center2 usesadoseof500mg/weekforthreeweeksevery28days.In theonlystudypublishedassessingtheeffectonmobilization
Progression-free survival
Number at risk Group: 1
70 48 33 10 3 1
18 14 5 3 0 0
Group: 2
Sur
viv
al probabillty
, %
Time (months) Regimen
G-CSF G-CSF/Cy
100
90
80
70
60
50
40
30
20
10
0
0 10 20 30 40 50
Figure2–Progression-freesurvivalforG-CSFand G-CSF+cyclophosphamidegroups.
inpatientsundergoingCTD,Auneretal.2reported mobiliza-tionfailureinattemptstoperformatleastoneASCT.Failure ratesforcellnumbercut-offsof≥4×106CD34+cells/kgand of≥2×106 CD34+ cells/kg were 39% and25% ofthe cases, respectively.InanotherstudycomparingCTDvs.aregimen ofVAD plus cyclophosphamideasinduction,Morganet al. identifiedamobilizationfailurerateof1%ofcases.19Inthese studies,thecombinationofG-CSFandcyclophosphamidewas usedformobilizationinallcases.Transplant centersdiffer withregardtothestandardconductforharvesting progen-itor cells. The use of cyclophosphamide, while promoting bettercellcollection,prolongsthewholeprocessduetothe waitfor cell productionrecovery.Generally, this process is performed with the patient hospitalized and is associated withincreasedriskoffebrileneutropeniaandotherinfectious
Overall survival
Number at risk Group: 1
70 53 41 23 10 1
18 16 8 4 0 0
Group: 2
Sur
viv
al probabillty
, %
Time (months) Regimen
G-CSF G-CSF/Cy
100
90
80
70
60
50
40
30
20
10
0
0 10 20 30 40 50
complications.6Forbothofthecentersinthepresent analy-sis,theminimumacceptablenumberofcollectedcellswas 2×106CD34+cells/kg,therebyallowingforatleastoneASCT to becarried out.A difference betweengroups was noted forthemobilizationofprogenitorcells,withthegroupthat receivedG-CSF pluscyclophosphamideharvestingahigher meanof6.4(±7.7)×106/kgvs.3.4(±1.3)×106/kgforthegroup thatreceivedG-CSFalone(p-value=0.008).However,the num-berofcellsinbothgroupswassufficienttoperformatleast oneASCT.Auneret al.reportedadifferentnumberofdays ofapheresis in cases that received CTD vs. those induced usinga VAD orVAD-likeprotocol.In the currentstudy,no differenceinthenumberofdaysofapheresiswasobserved betweenthegroups(p-value=0.07).Nostudiesexistthat sup-portanincreaseininductiontimeprecedingmobilizationto enhancesuccessfulcellcollection.22Inthepresentstudy,no associationwasfoundbetweenbetterresponseandimproved survival.Thecyclophosphamideusedinmobilization,in addi-tiontoitsabilitytopromotereleaseofprogenitorcellsfrom thebonemarrowforperipheralcollection,hasareputation ofreducingthediseasefurther(debulking)duringthe collec-tionofprogenitorcells.Retrospectivestudieshavefailedto confirmthiseffectandhaveshownnoadvantageintermsof survival.22Similarly,inthepresent study,noadvantagesof cyclophosphamideusewerefoundintermsofmobilization, improvedresponseorsurvival.Assessingthesituationinthe Braziliancontextwithregardstolimitationsforperforming ASCT,difficultiesinfrozenstorageofcells,andtheneedto cutcosts,thepresentstudyrevealedthatsufficientprogenitor cellscanbemobilizedtoperformatleastoneASCTwiththe useofG-CSFaloneinpatientsinducedusingtheCTDprotocol.
Conclusion
TheuseofG-CSFalonetomobilizeprogenitorcellsisfeasible in multiple myeloma patients induced with a cyclophos-phamide,thalidomideanddexamethasoneprotocol.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. MohtyM,HarousseauJL.Treatmentofautologousstemcell transplant-eligiblemultiplemyelomapatients:tenquestions andanswers.Haematologica.2014;99(3):408–16.
2. AunerHW,MazzarellaL,CookL,SzydloR,SaltarelliF,PavluJ, etal.Highrateofstemcellmobilizationfailureafter thalidomideandoralcyclophosphamideinductiontherapy formultiplemyeloma.BoneMarrowTransplant.
2011;46(3):364–7.
3. DesikanKR,TricotG,MunshiNC,AnaissieE,SpoonD,Fassas A,etal.Precedingchemotherapy,tumourloadandage influenceengraftmentinmultiplemyelomapatients mobilizedwithgranulocytecolony-stimulatingfactoralone. BrJHaematol.2001;112(1):242–7.
4. KumarS,DispenzieriA,LacyMQ,HaymanSR,BuadiFK, GastineauDA,etal.Impactoflenalidomidetherapyonstem cellmobilizationandengraftmentpost-peripheralbloodstem
celltransplantationinpatientswithnewlydiagnosed myeloma.Leukemia.2007;21(9):2035–42.
5.BreitkreutzI,LokhorstHM,RaabMS,HoltBv,CremerFW, HerrmannD,etal.Thalidomideinnewlydiagnosedmultiple myeloma:influenceofthalidomidetreatmentonperipheral bloodstemcellcollectionyield.Leukemia.2007;21(6):1294–9.
6.KumarS,GiraltS,StadtmauerEA,HarousseauJL,PalumboA, BensingerW,etal.Mobilizationinmyelomarevisited:IMWG consensusperspectivesonstemcellcollectionfollowing initialtherapywiththalidomide-,lenalidomide-,or
bortezomib-containingregimens.Blood.2009;114(9):1729–35.
7.DiPersioJF,StadtmauerEA,NademaneeA,MicallefIN,StiffPJ, KaufmanJL,etal.PlerixaforandG-CSFversusplaceboand G-CSFtomobilizehematopoieticstemcellsforautologous stemcelltransplantationinpatientswithmultiplemyeloma. Blood.2009;113(23):5720–6.
8.BensingerW,DiPersioJF,McCartyJM.Improvingstemcell mobilizationstrategies:futuredirections.BoneMarrow Transplant.2009;43(3):181–95.
9.GertzMA.Currentstatusofstemcellmobilization.BrJ Haematol.2010;150(6):647–62.
10.FitoussiO,PerreauV,BoironJM,BouzigonE,Cony-MakhoulP, PigneuxA,etal.Acomparisonoftoxicityfollowingtwo differentdosesofcyclophosphamideformobilizationof peripheralbloodprogenitorcellsin116multiplemyeloma patients.BoneMarrowTransplant.2001;27(8):837–42.
11.SungAD,GrimaDT,BernardLM,BrownS,CarrumG, HolmbergL,etal.Outcomesandcostsofautologousstemcell mobilizationwithchemotherapyplusG-CSFvsG-CSFalone. BoneMarrowTransplant.2013;48(11):1444–9.
12.ToorAA,vanBurikJA,WeisdorfDJ.Infectionsduring mobilizingchemotherapyandfollowingautologousstemcell transplantation.BoneMarrowTransplant.2001;28(2):1129–34.
13.MohtyM,HoAD.Inandoutoftheniche:perspectivesin mobilizationofhematopoieticstemcells.ExpHematol. 2011;39(7):723–9.
14.HungriaVT,CrusoeEQ,QueroAA,SampaioM,MaiolinoA, BernardoWM.Guidelinesonthediagnosisandmanagement ofmultiplemyelomatreatment:Associac¸ãoBrasileirade HematologiaeHemoterapiaeTerapiaCelularProject guidelines:Associac¸ãoMédicaBrasileira–2012.RevBras HematolHemoter.2013;35(3):201–17.
15.PalumboA,AndersonK.Multiplemyeloma.NEnglJMed. 2011;364(11):1046–60.
16.SanchoJM,MorgadesM,GrifolsJR,JuncàJ,GuardiaR,VivesS, etal.Predictivefactorsforpoorperipheralbloodstemcell mobilizationandpeakCD34(+)cellcounttoguide
pre-emptiveorimmediaterescuemobilization.Cytotherapy. 2012;14(7):823–9.
17.MaritG,ThiessardF,FaberesC,Cony-MakhoulP,BoironJM, BernardP.Factorsaffectingbothperipheralbloodprogenitor cellmobilizationandhematopoieticrecoveryfollowing autologousbloodprogenitorcelltransplantationinmultiple myelomapatients:amonocentricstudy.Leukemia. 1998;12(9):1447–56.
18.CavoM,TacchettiP,PatriarcaF,PetrucciMT,PantaniL,Galli M,etal.Bortezomibwiththalidomideplusdexamethasone comparedwiththalidomideplusdexamethasoneas inductiontherapybefore,andconsolidationtherapyafter, doubleautologousstem-celltransplantationinnewly diagnosedmultiplemyeloma:arandomisedphase3study. Lancet.2010;376(9758):2075–85.
19.RajkumarSV,RosinolL,HusseinM,CatalanoJ,JedrzejczakW, LucyL,etal.Multicenter,randomized,double-blind,
20.MorganGJ,DaviesFE,GregoryWM,BellSE,SzubertAJ, NavarroCoyN,etal.Cyclophosphamide,thalidomide,and dexamethasoneasinductiontherapyfornewlydiagnosed multiplemyelomapatientsdestinedforautologousstem-cell transplantation:MRCMyelomaIXrandomizedtrialresults. Haematologica.2012;97(3):442–50.
21.RichardsonPG,WellerE,LonialS,JakubowiakAJ,JagannathS, RajeNS,etal.Lenalidomide,bortezomib,anddexamethasone
combinationtherapyinpatientswithnewlydiagnosed multiplemyeloma.Blood.2010;116(5):679–86.
22.TuchmanSA,BaconWA,HuangLW,LongG,RizzieriD, HorwitzM,etal.Cyclophosphamide-basedhematopoietic stemcellmobilizationbeforeautologousstemcell