RevBrasAnestesiol.2016;66(6):657---660
REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
PublicaçãoOficialdaSociedadeBrasileiradeAnestesiologiawww.sba.com.br
CLINICAL
INFORMATION
Anesthesia
in
pregnant
women
with
HELLP
syndrome:
case
report
Eduardo
Barbin
Zuccolotto,
Eugenio
Pagnussatt
Neto
∗,
Glínia
Cavalcante
Nogueira,
José
Roberto
Nociti
CentrodeEnsinoeTreinamentoemAnestesiologia(CET-SBA)daClínicadeAnestesiologiadeRibeirãoPreto(CARP),Ribeirão Preto,SP,Brazil
Received6March2014;accepted5May2014
Availableonline1October2016
KEYWORDS
HELLPsyndrome; Cesareansection; Propofol;
Remifentanil
Abstract
Backgroundandobjectives: HELLPsyndrome,characterizedbyhemolysis,highlevelsofliver enzyme,andlowplateletcount,isanadvancedclinicalstageofpre-eclampsia,progressingto highmaternal(24%)andperinatal(up40%)mortality,despitechildbirthcareinatimelymanner. The goalistodescribetheanesthetic managementofacasewithindicationtoemergency cesarean.
Casereport: Femalepatient,36yearsold,gestationalageof24weeks,withhypertensivecrisis (BP180/100mmHg)andsevereheadache,wasadmittedtotheoperatingroomforacesarean sectionafterdiagnosisofHELLPsyndrome.Indicatedforgeneralanesthesia,weoptedfortotal intravenouswithintubationafterrapidsequenceinductionwithpropofolandremifentanilin continuous target-controlled infusion, androcuroniumatadose of1.2mg/kg.Maintenance wasachievedwithpropofolandremifentanil.Thesurgicalprocedurewasuneventful,thechild wasbornwithAPGAR1/5andtransferredtotheNICU.Attheendofsurgery,thepatientwas extubatedintheoperatingroomandtakentotheICU.Thepostoperativeperiodwasuneventful withnochangesworthyofnoteandthepatientwasdischargedonthesixthpostoperativeday.
Conclusion: WhengeneralanesthesiaisthechoiceinparturientwithHELLPsyndrome,tracheal intubationwithrapidsequenceinductionduetopossibledifficultairway,aswellastheuseof drugs tocontrolthehemodynamicresponsecanminimizethecomplicationsassociatedwith theprocedure,asoccurredinthiscase.
©2014SociedadeBrasileiradeAnestesiologia.Publishedby ElsevierEditoraLtda.Thisisan openaccessarticleundertheCCBY-NC-NDlicense( http://creativecommons.org/licenses/by-nc-nd/4.0/).
∗Correspondingauthor.
E-mail:[email protected](E.PagnussattNeto).
http://dx.doi.org/10.1016/j.bjane.2014.05.013
658 E.B.Zuccolottoetal.
PALAVRAS-CHAVE
SíndromeHELLP; Cesariana; Propofol; Remifentanil
AnestesiaparagestantecomsíndromeHELLP:relatodecaso
Resumo
Justificativaeobjetivos: AsíndromeHELLP,caracterizadaporhemólise,elevac¸ãodos níveis deenzimashepáticaseplaquetopenia,representaestágioclínicoavanc¸adodapré-eclâmpsia, cursandocomelevadamortalidadematerna(24%)eperinatal(até40%),apesardaassistência ao partode formaoportuna.O objetivoé descrever omanejoanestésico de um casocom indicac¸ãodecesarianadeemergência.
Relatodecaso:Pacientedosexofeminino,36anos,idadegestacional24semanas,comcrise hipertensiva(PA180/100mmHg)ecefaleiaintensa,éencaminhadaaoCentroCirúrgicopara operac¸ão cesarianaapósdiagnóstico de síndromeHELLP. Indicadaanestesia geral, optou-se por venosa total comintubac¸ão após induc¸ão sequencial rápida, compropofol e remifen-tanilem infusãocontínuaalvo-controlada erocurônionadosede1,2mg/kg. Amanutenc¸ão foiobtidacompropofoleremifentanil.Oprocedimentocirúrgicotranscorreusem anormali-dades,acrianc¸anasceucomAPGAR1/5efoiencaminhadaàUTINeonatal.Aofinaldacirurgia, procedeu-seàextubac¸ãonasalacirúrgicaeapacientefoiencaminhadaaoCTI.Opós-operatório decorreusemalterac¸õesdignasdenotaeapacientetevealtanosextodiapós-operatório.
Conclusão:Quando se opta pela anestesia geral em parturiente com síndrome HELLP, a intubac¸ãotraquealcomtécnicadeinduc¸ãosequencialrápidaemfunc¸ãodepossívelviaaérea difícil,bemcomooempregodedrogasquecontrolemarespostahemodinâmica,podem mini-mizarascomplicac¸õesassociadasaoprocedimento,comoocorreunopresentecaso.
©2014SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Este ´eum artigoOpen Accesssobumalicenc¸aCCBY-NC-ND( http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Hypertension induced by pregnancy has various clinical
forms,sometimespresentingwithslightincreasesinblood
pressure and sometimes as a severe enough disease to
involve various organs or systems.1 Preeclampsia is a
complexmultisystem disorder of unknown etiology,
char-acterized by the combined development of hypertension
and proteinuria (>300mg within 24h) after the first 20
weeks of pregnancy.1,2 Edema is no longer a diagnostic
criterion.Preeclampsia isa clinicaldiagnosis. Riskfactors
include obesity, nulliparity, and advanced maternal age.
Preeclampsia has an incidence ranging from 1.5% to3.8%
in all pregnancies in developed countries,while in Brazil
it maybe ashigh as7.5%.3 The HemolysisElevated Liver
enzymes Low Platelets (HELLP) syndrome is an advanced
stageofpreeclampsia.Regardingplateletcount,HELLP
syn-drome is divided into three classes3: class I if platelets
countlessthan50,000mm−3;classIIifbetween50,000and
100,000mm−3;and classIIIif greater than100,000mm−3.
HELLP syndrome etiology is not fully known. Its clinical
manifestationsresultfromunknowninsulttoplatelet
acti-vation and microvascular endothelial damage. Hemolysis,
defined by the presence of microangiopathic hemolytic
anemia, is the most important disorder. The following
diagnostic criteria are suggested: (1) hemolysis, defined
by abnormal peripheral bleeding and increased bilirubin
levels (1.2mgdL−1 or more); (2) elevated liver enzymes,
defined by glutamic---oxaloacetic transaminase (AST) of
70UL−1 or more and lactate dehydrogenase (LDH) above
600UL−1;(3)lowplateletcount(lessthan100,000mm−3).4
HELLPsyndromemayaffect4---12%ofpatientswithsevere
preeclampsiaandmaycontributetohighmaternal(24%)and
perinatal(upto40%)mortality,despitethedeliverycarein
a timely manner.3,5 Given the importanceof this
involve-ment during pregnancy and the frequency in anesthesia,
appropriatemanagementofpregnantpatientswithsevere
preeclampsiaisextremelyimportant.
Case
report
Femalepatient,36yearsold,24weeksgestationalage,with
a historyof malaiseandheadachefor a week,presenting
a hypertensive crisis (BP 180/100mmHg) and intensive
headacheathospitaladmission.Shehadnoseizuresathome
or in the emergency room. Test results on admission are
showninTable1.Afterexpertevaluation,thepatientwas
taken to the operating room for an emergency cesarean
diagnosed withHELLP syndrome.She arrives at the
oper-ating roomawake,lucid andoriented, withhemodynamic
stability,receivingmagnesiumsulfateschemeasobstetrical
management. Giventhe case severityand the
contraindi-cationstoneuraxial blockadethat willbediscussed later,
totalintravenousanesthesiawasindicated.Thepatientwas
positionedonthesurgicaltableandmonitoredasroutine,
withmultiparametermonitors(non-invasivebloodpressure,
cardioscopy,pulseoximetry).Peripheralvenousaccesswas
performed withJelconumber18 Gandfluid replacement
started with heated Ringer’s lactate solution. Anesthesia
inductionwasproposedaccordingtotheneedfortracheal
intubation by the rapid sequence technique, with oxygen
underFiO2100%,propofoltarget-controlledcontinuous
infu-sion(4ngmL−1),remifentaniltarget-controlledcontinuous
infusion(3ngmL−1),androcuronium(1.2mgkg−1).Tracheal
intubation was uneventfully performed. Anesthetic
AnesthesiainpregnantwomenwithHELLPsyndrome:casereport 659
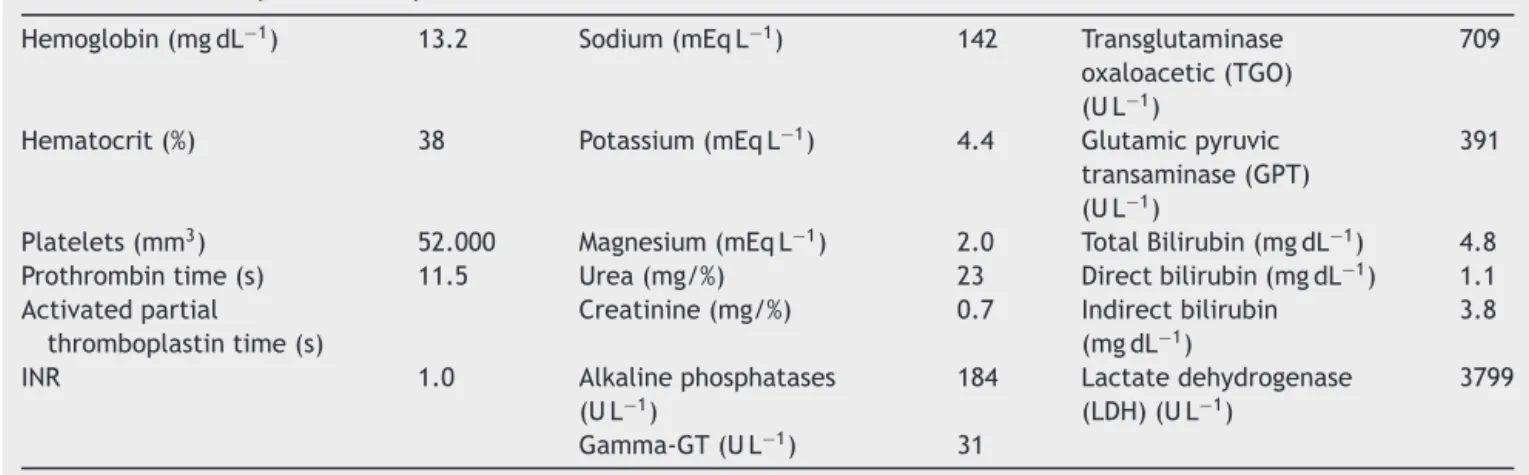
Table1 Laboratorytestsathospitaladmission.
Hemoglobin(mgdL−1) 13.2 Sodium(mEqL−1) 142 Transglutaminase oxaloacetic(TGO) (UL−1)
709
Hematocrit(%) 38 Potassium(mEqL−1) 4.4 Glutamicpyruvic transaminase(GPT) (UL−1)
391
Platelets(mm3) 52.000 Magnesium(mEqL−1) 2.0 TotalBilirubin(mgdL−1) 4.8
Prothrombintime(s) 11.5 Urea(mg/%) 23 Directbilirubin(mgdL−1) 1.1 Activatedpartial
thromboplastintime(s)
Creatinine(mg/%) 0.7 Indirectbilirubin (mgdL−1)
3.8
INR 1.0 Alkalinephosphatases (UL−1)
184 Lactatedehydrogenase (LDH)(UL−1)
3799
Gamma-GT(UL−1) 31
propofol(3ngmL−1)andremifentanil(3ngmL−1). Mechani-calventilationwithcycledvolume,tidalvolume=8mLkg−1, andFiO2=50%in air.The surgicalprocedurewas unevent-ful. The babywas born alive, APGAR 1 (1st min)/5 (10th min),andwassenttotheneonatalintensivecareunit(NICU) forpediatricrigorousevaluation.Attheendofsurgery,the patientwasextubatedstillintheoperatingroom,remaining stableand admittedtothe intensive care unit(ICU). The patientwasdischargedonthe6thpostoperativeday with-outcomplications.ThechildremainedintheNICUandwas dischargedonthe26thdaywithgoodhealth and develop-ment.
Discussion
As a severe form of preeclampsia, HELLP syndrome ori-ginates from abnormal placental development, followed by the production of factors that promote endothe-lial injury through the activation of platelets and/or vasoconstrictors.6,7Endothelialinjuryofthehepaticvessels,
followedbyplateletactivation,aggregationand
consump-tion,resultinginhepatocyteischemiaanddeath,isthemain
hypothesistoexplainthecharacteristiclaboratoryfindings
of HELLP syndrome.6 This is a complication in
approxi-mately6---8%ofpregnanciesandtogetherwitheclampsiaitis responsibleforsignificantmorbidityandmortalityin
obstet-ricpatients.Severepreeclampsiainvolvesorgandamage.It
is characterized by blood pressure valuesgreater than or
equalto160/110mmHgatrest,severeproteinuriaand
olig-uria(<400mL24h−1),changesinvision,headache,andother
brainchanges,epigastricpain,signsofpulmonaryedema,
cyanosis,andHELLPsyndrome.1PatientswithHELLPare
sus-ceptibletohighincidenceofstroke,heartdisease,placental
rupture, need for blood transfusion,pleural effusion, and
infections.ManyHELLPcasesoccurinthepretermperiod,
but 20% may occur in the post-term period with higher
incidence of acute pulmonary edema.4 Studies reported
thatof 309patients whodeveloped HELLPsyndrome,69%
hadit beforeand 31% afterdelivery; when itoccurs
dur-ingthepostpartumperiod,itsonsetoccursmainly24---48h
after birth of the fetus, although it is described that its
onsetmayoccurwithinhoursorupto6daysafterbirth.1,4
Case reports in the international literature confirm the
occurrenceofHELLPsyndromeupto8haftertheprocedure,
withthesamenosologicalfeaturesalreadyreported.8
Thedecisiononanesthesiaforpatientswith
preeclamp-siadependsmainlyonanoverallassessmentofthebenefits
andrisksthattheanesthesiaeffectcancausebothto
moth-ersandbabies.WhenpreeclampsiaismanifestedwithHELLP
syndrome,coagulopathy,andseveredysfunctionofmultiple
organs and cesarean delivery is indicated, general
anes-thesia may be a safer method than the neuraxial block,
aslongasasuccessfulairwaymanagementisprovided.9---11
Severepreeclampsia withHELLPsyndrome shouldmeana
changeinanestheticplanning.Thepresenceof
coagulopa-thy with thrombocytopenia predisposes to an increase in
the risk of epidural hematoma with neuraxial anesthesia
techniques.Guidelinesrecommendaplateletcountgreater
than100,000mm−3tominimizethisrisk,althoughthereis
nostatisticaldata in theliterature onneuraxialblockade
complicationsinpatientswithHELLPsyndromeandplatelet
count less than the cited value.10 A retrospective study3
evaluatedatotalof102cases,includingsevenpatientswith
HELLPsyndromeafterdeliveryand95patientswithHELLP
syndromebefore delivery. In the latter, 37 patients were
submittedtogeneral anesthesia, 53 underwent combined
neuraxial blockade (spinal-epidural), and 12 underwent
spinalblockade. Inpatients undergoingcombined
neurax-ialblockade, preoperative platelet countremained about
113,000,withnodifferencetospinalblock(95,000)and
gen-eralanesthesia(88,000).Twopatientsunderwentcombined
blockade,evenwithplateletcountlessthan50,000mm−3.
Therewerenocasesofepiduralhematoma,demonstrating
safetyand feasibilityin the use of neuraxial blockade in
selectedcasesofHELLPsyndrome.12 Anesthesia forHELLP
syndrome in a patient with adequate platelet count and
absenceofcoagulopathyiscontroversialas,inspiteofthe
foregoing,there are literature reports of post-anesthetic
puncturespinalhematomas;thus,itsuseshouldbeavoided
andcomplicationsreadilyrecognized.13
Whengeneralanesthesiaisconsidered,thetechniqueof
rapidsequenceintubationwithlikelydifficultairway
assess-ment and drugs that control the hemodynamic response
canminimizecomplicationsassociatedwiththeprocedure.
660 E.B.Zuccolottoetal.
andlidocaine.10Remifentanilisoftenusedtopromote
short-term analgesia with cardiovascular stability in high-risk
patients.14 In the case presented here, remifentanil was
theoptionusedforinductionandmaintenanceof
anesthe-sia.Arecentstudyreportedthreecasesofgoodresultsfor thechoiceofgeneralanesthesiawithsevofluraneinsteadof
epiduralspinal blockforcesarean sectioninpatients with
HELLPsyndrome,duetoseverethrombocytopenia.Noneof
thecomplicationsreportedintheliterature(renalfailure,
pulmonaryedema, cerebralhemorrhage,andhepatic
rup-ture)wasobservedin thethreepostoperativedaysinthe
reportedcases.15
Conclusion
Recent evidence about the anesthetic management of
patientswithHELLPsyndromewhoshouldundergocesarean
section is not clear regarding the best approach
indica-tion.However,given the rangeof possible complications,
itappearsthatthe generalanesthesiatechnique with
air-waycontrol(intubation)afterrapidsequenceinductionisa
goodchoice.Theavailablepharmacologicalarsenalshould
beusedwithdiscretion,withattentiontodrugsthatbring
greater stability during surgery. However, further studies
areneededtoindicate,basedonevidence,thebest
tech-niquetobeusedincasesofseverepreeclampsiaandHEELP
syndrome.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.GanemEM,CastigliaYMM.AnestesianaPré-Eclâmpsia.RevBras Anestesiol.2002;52:484---97.
2.Snegovskikh D,Braveman FR. Stoelting’s anesthesia and co-existing disease, 6th ed. Philadelphia: Elsevier; 2012. p. 181---217.
3.FonsecaPC, BezerraM,AraujoACPF,etal. SíndromeHELLP: considerac¸ões acerca de diagnóstico e conduta. FEMINA. 2007;35:9.
4.Fleischer L. Anesthesia and uncommon diseases, 6th ed. Philadelphia:Elsevier;2012.p.267---9.
5.JagiaM,TaqiS,HanafiM,etal.Thrombocytopenia-associated multiple organ failure or severe haemolysis, elevated liver enzymes, lowplatelet count in a postpartum case. IndianJ Anaesth.2013;57:62---5.
6.PereiraMN,MontenegroCAB,RezendeJ.SíndromeHELLP: diag-nósticoeconduta.FEMINA,Fevereiro.2008;36:2.
7.GargR,NathMP,BhallaAP,etal.Disseminatedintravascular coagulationcomplicatingHELLPsyndrome:perioperative man-agement.BMJCaseRep.2009.Publishedonline2009April17.
8.Chan SM,LuCC,Ho ST, et al. Eclampsia followingcesarean sectionwithHELLPsyndromeandmultipleorganfailure.Acta AnaesthesiolTaiwan.2008;46:46---8.
9.Xu S, Shen X, Wang F. Pesando riscos e benefícios: lic¸ões aprendidascomasintervenc¸õesterapêuticasdeumcasocom pré-eclâmpsiagrave.RevBrasAnestesiol.2013;63:290---5.
10.AnkichettySP,ChinKJ,ChanVW,etal.Regionalanesthesiain patientswithpregnancyinducedhypertension.JAnaesthesiol ClinPharmacol.2013;29:435---44.
11.NeliganPJ,LaffJG.Clinicalreview:specialpopulations--- crit-icalillnessandpregnancy.CritCare.2011;15:227.
12.Palit S, Palit G, Vercauteren M, et al. Regional anaesthesia forprimarycaesareansectioninpatientswithpretermHELLP Syndrome:a reviewof 102 cases. ClinExp Obstet Gynecol. 2009;36:230---4.
13.KoyamaS.Spinalsubarachnoidhematomafollowingspinal anes-thesiainapatientwithHELLPsyndrome.IntJObstetAnesth. 2010;19:87---91.
14.Richa F, Yazigi A, Nasser E, et al. General anesthesia with remifentanilforCesareansectioninapatientwithHELLP Syn-drome.ActaAnaesthesiolScand.2005;49:418---20.