REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
OfficialPublicationoftheBrazilianSocietyofAnesthesiologywww.sba.com.br
SCIENTIFIC
ARTICLE
The
effect
of
esmolol
on
corrected-QT
interval,
corrected-QT
interval
dispersion
changes
seen
during
anesthesia
induction
in
hypertensive
patients
taking
an
angiotensin-converting
enzyme
inhibitor
Zahit
C
¸eker,
Suna
Akın
Takmaz
∗,
Bülent
Baltaci,
Hülya
Bas
¸ar
DepartmentofAnesthesiolgyandReanimation,AnkaraTrainingandResearchHospital,MinistryofHealth,Ankara,Turkey
Received16January2014;accepted19March2014 Availableonline1May2014
KEYWORDS Esmolol;
QTinterval;
QTdispersion;
ACEinhibitor
Abstract
Backgroundandobjectives: The importance of minimizing the exaggerated sympatho-adrenergicresponses andQTinterval andQT intervaldispersion changes thatmay develop duetolaryngoscopyandtrachealintubationduringanesthesiainductioninthehypertensive patientsisclear.Esmololdecreasesthehemodynamicresponsetolaryngoscopyandintubation. However,theeffectofesmololindecreasingtheprolongedQTintervalandQTinterval disper-sionasinducedbylaryngoscopyandintubationiscontroversial.Weinvestigatedtheeffectof esmololonthehemodynamic,andcorrected-QTintervalandcorrected-QTintervaldispersion changesseenduringanesthesiainductioninhypertensivepatientsusingangiotensinconverting enzymeinhibitors.
Methods:60ASAI---IIpatients,withessentialhypertensionusingangiotensinconvertingenzyme inhibitorswereincludedinthestudy.Theesmololgroupreceivedesmololatabolusdoseof 500mcg/kgfollowed bya100mcg/kg/min infusionwhich continueduntilthe4thmin after intubation. The controlgroupreceived 0.9%salinesimilar tothe esmololgroup.The mean bloodpressure,heartratevaluesandtheelectrocardiogramrecordswereobtainedasbaseline valuesbeforetheanesthesia,5minafteresmololandsalineadministration, 3minafterthe inductionand30s,2minand4minafterintubation.
Results:Thecorrected-QTintervalwasshorterintheesmololgroup(p=0.012),the corrected-QTintervaldispersionintervalwaslongerinthecontrolgroup(p=0.034)andthemeanheart ratewas higherinthecontrolgroup(p=0.022)30safter intubation.Theriskofarrhythmia frequencywashigherinthecontrolgroupinthe4-minperiodfollowingintubation(p=0.038). Conclusion:Endotrachealintubationwasfoundtoprolongcorrected-QTintervaland corrected-QTintervaldispersion,andincreasetheheartrateduringanesthesiainductionwithpropofol
∗Correspondingauthor.
E-mail:[email protected](S.A.Takmaz). http://dx.doi.org/10.1016/j.bjane.2014.03.008
inhypertensivepatientsusing angiotensinconvertingenzymeinhibitors. Theseeffectswere preventedwithesmolol(500mcg/kgbolus,followedby100mcg/kg/mininfusion).During induc-tion,thebloodpressuretendstodecreasewithesmololwherecareisneeded.
© 2014SociedadeBrasileirade Anestesiologia.Publishedby ElsevierEditoraLtda.Allrights reserved.
PALAVRAS-CHAVE Esmolol;
IntervaloQT;
DispersãodoQT;
InibidoresdaEnzima
Conversorade
Angiotensina(ECA)
EfeitodeesmololsobreointervaloQTcorrigidoealterac¸õesdadispersãodo intervaloQTcorrigidoobservadasduranteainduc¸ãodaanestesiaempacientes hipertensosquereceberamuminibidordaenzimaconversoradeangiotensina
Resumo
Justificativaeobjetivo: Éóbviaaimportânciademinimizarasrespostassimpatoadrenérgicas exageradaseointervaloQTeadispersão dointervaloQTquepodemocorrerporcausade laringoscopiaeintubac¸ãotraquealduranteainduc¸ãodaanestesiaempacienteshipertensos. Esmololdiminuiarespostahemodinâmicaàlaringoscopiaeàintubac¸ão.Porém, oefeitode esmololsobreareduc¸ãodointervaloQTprolongadoeadispersãodointervaloQTinduzidapela laringoscopiaeintubac¸ãoécontroverso.Pesquisamosoefeitodeesmololsobreahemodinâmica eointervaloQTcorrigidoeasalterac¸õesdadispersãodointervaloQTobservadasdurantea induc¸ãodaanestesiaempacienteshipertensosquereceberaminibidoresdaenzimaconversora deangiotensina(IECA).
Métodos: Foram incluídos no estudo 60 pacientes, estado físico ASA I-II, com hipertensão arterial essencial e que receberam IECA. Ogrupo esmolol recebeu uma dose em bolus de 500mcgkg−1,seguidaporinfusãocontínuade100mcgkg−1min−1atéoquartominutoapósa
intubac¸ão.Ogrupocontrolerecebeusoluc¸ãosalinaa0,9%,semelhantementeaogrupoesmolol. Osvaloresdapressãoarterialmédiaedafrequênciacardíacaeosregistrosdo eletrocardio-gramaforamobtidosduranteafaseinicialpré-anestesia,cincominutosapósaadministrac¸ão de esmolole soluc¸ãosalina, trêsminutosapósainduc¸ãoe30segundos,doisminutose qua-trominutosapósaintubac¸ão.
Resultados: OintervaloQTcorrigidofoimenornogrupoesmolol(p=0,012),ointervalode dis-persãodointervaloQTcorrigidofoimaiornogrupocontrole(p=0,034)eafrequênciacardíaca médiafoimaiornogrupocontrole(p=0,022)30segundosapósaintubac¸ão.Oriscoda frequên-ciadearritmiafoimaiornogrupocontrolenoquartominutoapósaintubac¸ão(p=0,038). Conclusão:Descobrimosqueaintubac¸ãotraquealprolongaointervaloeadispersãodointervalo QTcorrigidoeaumentaafrequênciacardíacaduranteainduc¸ãodaanestesiacompropofolem pacienteshipertensosquereceberamIECA.Essesefeitosforamprevenidoscomesmolol(bolus de500mcgkg−1,seguidode100mcgkg−1min−1deinfusão).Duranteainduc¸ão,apressãotende
adiminuircomesmolol.Portanto,cuidadossãonecessários.
©2014SociedadeBrasileira deAnestesiologia.PublicadoporElsevierEditoraLtda.Todosos direitosreservados.
Introduction
A prolonged QT interval and corrected-QT interval (QTc)
combinedwithQTintervaldispersion(QTD)and
corrected-QTD (QTcD) are knownto increase the incidence of fatal
arrhythmiassuchaspolymorphicventriculararrhythmiaor
ventricular fibrillation and cause sudden deaths by
caus-ingcardiacirritability.1,2Anincreaseinsympatheticactivity
andplasmacatecholamineconcentrationsisknowntocause prolongation ofthe QTinterval andQTdispersion. Laryn-goscopyandtrachealintubationhavebeenshowntocause hyperdynamic responses such as hypertension, tachycar-dia, arrhythmia and prolongation of the QT interval.3,4
Althoughtheobservedhemodynamicresponsesare tempo-rary,theymaycauseseriouscomplicationssuchascerebral
hemorrhage, arrhythmia, myocardial ischemia or even infarctioninthepresenceofaccompanyingcerebrovascular disease,coronaryarterydiseaseorhypertension.5,6
Essentialhypertensionisthemostcommon accompany-ingdisorderinpatientsadmittedforsurgery.7Thedisturbed
cardiovascular homeostasis in hypertensive patients has been shown to cause a sympatho-vagal imbalance char-acterized by decreased vagal modulation and increased sympathetic activity.8 The response to laryngoscopy is
significantly different in hypertensive patients compared to normotensive patients. The blood pressure changes that develop immediately following anesthesia induction aremuch larger in hypertensive patients. These patients
have marked hypotension with induction and marked
pressure fluctuation of more than 20% in hypertensive patients has been shown to be associated with perioper-ative complications. The most common cause of sudden cardiac death in hypertensive cases unaccompanied by coronary artery disease has been reported to be ventri-cular arrhythmias10 and QTD prolongation in hypertensive
patients has been found to be associated with sudden death.11 The importance of minimizing the exaggerated
sympatho-adrenergic responses and QT interval and QTD changes during anesthesia induction in the hypertensive patient group is therefore clear. To prevent such detri-mental events different classes of drugs have been used. Esmololisacardioselectivebeta-adrenergicblockingagent with a rapid onset of action and quite short elimina-tionhalf-time. It is known todecrease the hemodynamic response to laryngoscopy and intubation.12,13 However,
the results of the limited number of studies where the effectofesmolol in decreasing the prolongedQT interval and QTD as induced by laryngoscopy and intubation are controversial.
There is a consensus on continuing antihypertensive medication until the morning of the day of surgery at present.However,theuseofangiotensinconvertingenzyme inhibitors(ACEIs)isdebatedduetothepotentialof devel-opinghypotensionresistant tovasopressors.Someauthors report the need to continue,14 while others believe they
should be discontinued.15 We did not find any studies on
theeffect of esmolol on the hemodynamic andQT inter-valand QTD changes seen during anesthesiainduction in hypertensivepatientstakingaACEIs.
The aim of thisstudy wastoinvestigate the effectof esmololonthehemodynamic,QTcandQTcDchangesduring anesthesiainductionseeninhypertensivepatientstakinga ACEIs.
Methods
Atotalof60patientsaged20---65yearsandtakingaACEIs withregulatedessential hypertension,whowereabout to undergoelectivesurgerywereincludedinthisprospective, randomized,double-blindstudyafterobtainingethic com-mitteeapprovalandwrittenpatientconsent.Patientswith unstableangina,severeconductiondisorderorarrhythmia, chronicobstructivepulmonarydisease,cardiacfailureand cardiacvalvedisease,thoseusingdrugsknowntoprolong the QT interval (such as tricyclic antidepressants, quini-dine,disopyramid,sotolol, Ca channel blockers),patients with electrolyte disorders or abnormal blood coagulation profiles, patientsknowntobe hypersensitivetothe med-icationtobeusedandpregnantwomenwereexcludedfrom thestudy.Patientstowhomthe intubationcouldbe diffi-cultandthosewhowereintubatedafterseveralattempts werenot included in thestudy.Information was provided onthemethodtobeusedandverbalandwritten consent wereobtainedfromthepatientsonthepreoperativevisit thedaybeforesurgery.Antihypertensivetreatmentwas con-tinueduntilthe morning ofsurgery but nopremedication wasadministered.
Following vascular access with a 20G intracath in the operating room, the patients were monitored for pulse oximetry(Draegerinfinitydeltamonitor,USA),non-invasive
blood pressure(Draegerinfinitydelta monitor,USA) anda 12-leadelectrocardiogram(ECG)device(Trismed,Cardipia 400).Theinitialheartrate(HR),meanbloodpressure(MBP) valuesand12-leadECG wererecorded.The patientswere prospectivelyrandomizedbycomputertooneoftheesmolol andcontrolgroups.Esmolol(Breviblock,Eczacıbas¸ı-Baxter Co)wasadministeredasa100mcg/kg/mininfusion follow-inga500mcg/kgbolusdose(in5mLofvolume,within30s) intheesmololgroup.Theesmololinfusionwascontinuedup to4min aftertheintubation.A bolusandinfusion admin-istrationsimilartotheesmololgroup wasperformedwith 0.9% saline in the control group. Anesthesia wasinduced with 2mg/kg propofol and 1mcg/kg fentanyl 5min after esmolol or saline induction in both groups. Patients were intubated within 3min of vecuronium (1mg/kg) adminis-tration by an experienced anesthetist and the procedure lasted 20s onaverage. Patients whose MBP decreased to below55mmHgandtheHRtobelow50/min were admin-istered 5mg ephedrine and 0.5mg atropine. The esmolol infusion was discontinued if there was no response to medication. The MBP, HRs and ECG (at a sweep rate of 50mms)ofthepatientswererecordedasabaselinevalue before the anesthesia (T0), 5min after esmolol or saline administration(T1),3minafterinductionmedication(T2), 30s after the intubation (T3), 2min after the intubation (T4), and 4min after the intubation (T5) for a total of 6times.
The study drugs were preparedby an anesthetist who wasnotincludedinthestudyanddidnotknowthepatient groups.Therecordswerekeptbyanotheranesthetistwho again didnotknow the patientgroups. ECG recordswere evaluatedby acardiologist whodidnot know thepatient groups. The distance from the start of the QRS complex to the end of the T wave wasaccepted as the QT inter-val. When the T wave was bi-notched, the end of the T wave was accepted as the point where the first wave’s extension reached the isoelectric line when the second notch wassmaller than 50% of the first notch andas the point where thesecond wave reached theisoelectricline ifit waslargerthan50% ofthe firstnotch.Three QT dis-tances were measured for each derivation and averaged. QT intervals corrected for HR (QTc) were calculated for allderivationsusingBazett’sformula(QTc=QT(ms)/RR(sn)1/2). The averageoftheQTcvaluesofthreeconsecutive heart-beatsateach derivationwasaccepted astheQTcinterval of that derivation. QTD was calculated as the differ-ence between the longest QT distance and the shortest QT distance at each interval while QTcD was calculated as the difference between the longest and shortest QTc values.
Table1 Demographicandclinicaldata(mean±SD).
Esmolol(n=30) Control(n=30) p-value
Age(years) 57.0±6.9 57.9±6.8 0.589
Gender(female/male) 7/23 9/21 0.559
ASA(I/II) 16/14 21/9 0.184
Height(cm) 159.8±7.6 162.2±7.7 0.120
Weight(kg) 73.1±14.4 78.2±13.2 0.184
Results
There was no difference between the groups regarding
demographicdata(Table1).Themeanbasalbloodpressure,
HR,QTcintervaland QTcDvalues weresimilarin thetwo groups.
TheMBPwaslowerintheesmololgroupthanthecontrol groupattheT1(84.1±17.4vs.98.2±14.7),T2(62.8±8.5 vs. 87.7±11.5) and T3 (75.4±6.8 vs. 91.3±21.2) mea-surementtimes (Fig.1).There wasamarked decreasein MBPlevelscomparedtobaselineatallmeasurementtimes aftertheinductiondrugswereadministered(T2)inthe con-trol group (T2:p=0.001; T3: p=0.020; T4: p=0.025; T5:
p=0.001)andatallmeasurementtimesafteresmololwas administered(T1)inthe esmololgroup (T1:p=0.001;T2:
p=0.001; T3: p=0.001; T4: p=0.002; T5: p=0.001). The esmololgroup, incontrasttothecontrolgroup, showeda markedlylargerdecreaseinMBPfollowingpropofol induc-tion(T2)(Fig.1)(p=0.001).
ComparisonofmeanHRvaluesshowedasignificant dif-ference between the groups in the measured values 30s after intubation (T3). The mean HRwas markedly higher 30s afterintubation(T3)in thecontrolgroup(84.2±15.6 vs.93.2±13.9,p=0.022).TheHRintheesmololgroupwas lower than the baseline value at all measurement times except T3 (T1:p=0.007; T2: p=0.001; T4: p=0.015; T5:
110
100
90
80
70
60
50
40
T0 T1 T2 T3 T4 T5
Time Mean blood pressure
Mean b
lood pressure (mmHg)
* #
* # * #
#
+ + + + ++ +
¥
Esmolol
Control
Figure1 Mean‘‘bloodpressure’’valuesintheesmololand controlgroups.T0,basalvalue;T1,5minpost-esmolol admin-istration; T2, 2min post-induction drugs administration; T3, 30spost-intubation;T4,2minpost-intubation;T5,4min post-intubation. *p=0.001, when the two groups are compared;
#p=0.001,whencomparedwiththebaseline;¥p=0.002,when
comparedwith thebaseline;+p=0.001,whencompared with
the baseline; ++p=0.020,when compared with the baseline; +++p=0.025,whencomparedwiththebaseline.
p=0.001)whileitwassimilartothebaselinevalue30safter intubation.The HRvaluesinthecontrolgroupwerelower thanbaselineattheT2measurementtime(p=0.003)and higherthanthebaselineatT3(Fig.2)(p=0.001).
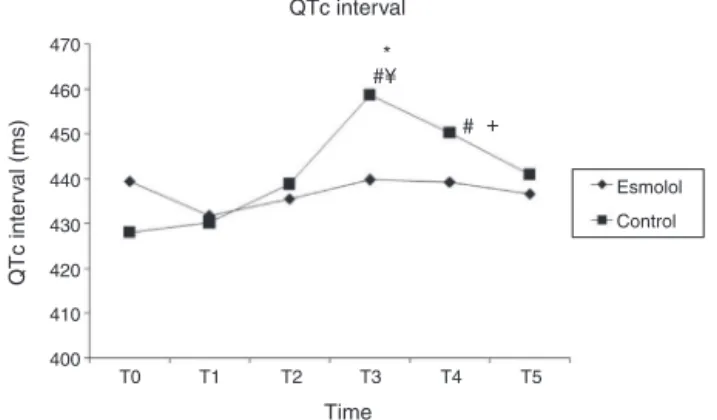
The mean basal QTc values of the patients were simi-lar in the 2 groups. The baseline QTc valueswere higher than 440ms in 12 (40%) patients from the esmolol group and10(33%) patientsfromthecontrol groupwithno dif-ferencebetweenthegroups(p>0.05).TheQTcintervalwas markedlyshorterintheesmololgroupthanthecontrolgroup 30s after intubation (T3) (439.7±27.8 vs. 458.7±29.3
p=0.012).TheQTcintervaldurationshortenedslightlyafter esmololadministrationbutthiswasnotstatistically signif-icant. The QTc interval wassimilar tothe baseline at all measurementtimes(p=0.618).TheQTcintervalvalues30s (T3)and 2min (T4) after intubation in the control group werelongerthanbothbaselinevalues(p=0.001,p=0.001) andthetimeatT1(p=0.001,p=0.003)(Fig.3).
ThemeanbaselineQTcDvaluesofthepatientswere simi-larinthetwogroups.TheQTcDintervalwasmarkedlylonger inthecontrolgroupthantheesmololgroup30safter intuba-tion(T3)(p=0.034).TheQTcDintervalvaluesintheesmolol groupdidnotshowastatisticallysignificantchangeatany measurementtime(p=0.061).TheQTcDvaluesinthe con-trolgroupwerelongerthanthebaselineaftertheinduction drugs(T2)and2minafterintubation(T3)andlongerthan
100
Mean heart rate
Esmolol
Control 95
90
85
80
75
70
65
60
55
50
T0 T1 T2 T3 T4 T5
Time
Hear
t r
ate (bpm)
#
#
#
#
# #
*
Figure 2 Mean ‘‘heart rate’’ values in the esmolol and
controlgroups.T0,basalvalue;T1,5minpost-esmolol admin-istration; T2, 2min post-induction drugs administration; T3, 30spost-intubation;T4,2minpost-intubation;T5,4min post-intubation. *p=0.022, when the two groups are compared;
470
460
450
440
430
420
410
400
T0 T1 T2 T3
Time
QTc inter
val (ms)
T4 T5
* #¥
# +
Esmolol
QTc interval
Control
Figure 3 Mean ‘‘QTc’’ values in the esmolol and control
groups. T0, basal value; T1, 5min post-esmolol administra-tion; T2, 2min post-induction drugs administration; T3, 30s post-intubation; T4, 2min post-intubation; T5, 4min post-intubation. *p=0.012, when the two groups are compared;
#p=0.001,whencomparedwiththebaseline;¥p=0.001,when
comparedwiththeT1;+p=0.003,whencomparedwiththeT1.
40
35
30
25
20
15
10 T0
QTcD (ms)
T1 T2
Time QTc dispersion
Esmolol
Control
T3 T4 T5
+ *#t
¥
Figure4 Mean‘‘QTcD’’ valuesin the esmolol and control
groups. T0, basal value; T1, 5min post-esmolol administra-tion; T2, 2min post-induction drugs administration; T3, 30s post-intubation; T4, 2min post-intubation; T5, 4min post-intubation. *p=0.034, when the two groups are compared;
+p=0.003,whencomparedwiththebaseline;#p=0.001,when
comparedwiththebaseline;¥p=0.006,when comparedwith thebaseline;tp=0.036,whencomparedwiththebaseline.
both the baseline and T1 (post-esmolol) levels 30s after intubation(T3)(Fig.4).
Therewasnoneedtouseatropineinthepatientswhile ephedrinewasrequiredin3patientsintheesmololgroup. The esmolol infusion did not need to be discontinued in anypatient.Theincidenceofarrhythmiadevelopmentwas higher in the 4min after intubation in the control group (p=0.038).Unifocalventricularextrasystolesdevelopedin 2 patients from the esmolol group while multifocal ven-tricularextrasystolesdeveloped in 4patients, ventricular bigeminyin1patient,andunifocalventricularextrasystoles in3patientsfromthecontrolgroup.
Discussion
In this study we investigated the effect of esmolol on the induction hemodynamics, and QTc interval and QTcD
changes in a hypertensive patient group taking ACEIs. The QTc and QTcD prolongation following intubation was kept under control with 500mcg/kg bolus esmolol fol-lowedbya100mcg/kg/mininfusion. Esmololalsostopped the increased HR following intubation. However, esmolol
led to a marked decrease in blood pressure during
induction.
Asfar aswe know, ourstudy is thefirst toinvestigate the effectof esmolol onhemodynamic responses induced by laryngoscopy and tracheal intubation and also on the QTintervalandQTDinahypertensivepatientgrouptaking ACEIs.Althoughtherehavebeenmanystudiesonthe sup-pressionof theintubation-relatedhemodynamic responses withesmolol,thereisnoconsensusontheoptimumtimeand routeofadministration.Alargemeta-analysisbyFigueredo andGarcia-Fuentes13ontheeffectivenessofesmololforthe
suppressionofintubation-relatedhemodynamicresponsesin 2900patientsevaluated11differentregimesanddosesof esmololinasystematicmanner.Theresultwasthatesmolol was effective in suppressing intubation-related hemody-namic responses but it carried a dose-dependent risk of hypotension duringanesthesia induction. The most effec-tivedosewithalowerincidenceandseverityofsideeffects wasa500mcg/kgbolusdosefollowedbyacontinuous infu-sionof200or300mcg/kg/min.Weuseda500mcg/kgbolus dose ofesmolol followedbya 100mcg/kg/mincontinuous infusion. The infusion dose was halved for two reasons. The first was the high rate of hypotension in our pilot study withinfusion dosesof 200mcg/kg/min. The second reason was the use of propofol as the induction agent. Although therearestudies showingthatpropofolprolongs theQT interval,16,17 it isgenerallyaccepted thatpropofol
hasnoor alittleeffectontheQTinterval.18,19 We
there-forepreferredtheuseofpropofolforinductioninsteadof volatileagentsorthiopentalthatareknowntoprolongthe QT interval. However, propofol is also known to be able todecreaseblood pressure20,21 andcausebradycardia22 by
decreasing systemic vascular resistance. Korpinen et al.23
havereportedthatapropofol---esmololcombinationcauses hemodynamic depression in theirstudy where they inves-tigatedtheelectrocardiographicandhemodynamiceffects of esmololcombinedwithmethohexitaland propofol dur-inganesthesiainduction.Takingintoaccountthatourstudy would be performed on the hypertensive patient group where hemodynamicfluctuations aremoreprominent,we decreased the infusion dose soasnot tocausemore car-diovascular depression during esmolol usage.The esmolol dosesweusedpreventedtheincreaseinHRfollowing intu-bationbutpreservedthebeginningHRvaluesinthecontrol group.However,thedecreaseobservedinMBPduring induc-tionismuchhigherthanthedecreaseinthecontrolgroup and noteworthy. We believe that the vasodilation-causing effectofbothpropofolandtheACEinhibitorinthe hyper-tensivepatientgroupbecomespotentiatedwithesmololin thehypertensive patientgroup.However,controlled stud-iesare needed toverifythis opinion. Itmay beuseful to decrease propofol dose to avoid deephypotension during inductioninhypertensivepatientstakingACEIs.Weisenberg etal.24haverecentlypublishedanarticlewherethey
hemodynamic instability. Howeverin this study bispectral index monitorization was not used and optimal hemo-dynamic control was assumed synonymous with optimal anesthesiaincludesanalgesiaandamnesia.Morestudiesare needed todetermine the optimumdose during theuseof esmolol with propofol induction in hypertensive patients takingACEIs.
It is known that there is a close relationship between essentialhypertensionandtheautonomousnervoussystem and that the frequency of cardiac arrhythmias increases inpatientswithdisturbedQTdynamicity.25 IncreasedQTD
in hypertensive patients has been found tobe associated with sudden death11 and various antihypertensive drugs
have been shown to decrease the incidence of QTD and arrhythmia.26,27 Takingintoaccountthatlaryngoscopyand
sympathetic activation also prolong the QT interval and QTD, it may beclinically significant to use methods that decreasethe QTDin hypertensivepatients topreventthe sympatho-adrenergic responses induced by laryngoscopy andtracheal intubation.Beta-blockers knowntodecrease the cardiovascular responses to sympathetic stimuli may decrease the development of arrhythmia in this aspect. Variousresultshavebeenreportedregardingtheeffectof esmolol on the QT interval induced by laryngoscopy and intubation.12,23,28---31 Korpinen et al.30 have reported that
esmolol combined with propofol and alfentanil induction in otolaryngology surgery shortens the QTc interval. The sameinvestigatoralsoreportedintwoseparatestudiesthat esmololshortenstheQTcintervalprolongationseen follow-ingintravenousanesthesicusagebut doesnotshorten the prolongation seen following intubation.28,29 Anotherstudy
bythesameinvestigatorcombiningesmololwith metohex-ital or propofol induction has reported results similar to thesetwostudies.23However,itisnoteworthythatsomeof
thesestudiesusedsuccinylcholine,12,23,29whilesomeused
thiopental,29,30andsomeanticholinergicpremedication.12,23
These agents areknown toprolong the QT interval.Erdil etal.31havepublishedastudywheretheyinvestigatedthe
effectofesmolol ontheQTcintervalchangesseen during anesthesia induction in coronary artery disease patients. This study combinedetomidate, fentanyl and vecuronium inductionwithesmololandreportedthatesmololkeptthe hemodynamic responses to intubation and the QTc inter-valprolongationfollowingintubationundercontrol.Esmolol was usedat a bolus dose of 1000mcg/kg followed by an infusion of250mcg/kg/minandnocardiovascular depres-siondeveloped in thepatients despitethis relativelyhigh dose.Theinvestigatorsfeltthiswasduetotheuseofagents withminimalcardiovasculareffectsduringinduction.Inour study we found that the prolonged QTc and QTcD values thatstartedwithanesthesiainductionandpeakedwith intu-bation inthe controlgroupwere preventedwithesmolol. Besides,arrhythmiaoccurrencefrequencyafterentubation wasalsodecreasedwithesmolol.Recently,Kanekoetal.32
investigatedtheeffectoflandiolol,anultra-shortacting1 adrenoceptorantagonist,onQTintervalandQRdispersion. Similar toour results, theyfound that landiolol prevents increaseinQT,QTc,QTD,andQTcDduringandaftertracheal intubation.
We observed that thebasal QTc valuesof ourpatients wererelativelyhigh(439.4±29.2and428.1±25.4).These highvaluesmaybeduetoourpatientsbeinghypertensive
withhighsympatho-adrenaltonus.Inaddition,thelackof premedicationmayalsohavecontributedtothe sympatho-adrenaltonusincreasebycausinganxiety.
A limitation of our study is that we did not compare patients who continued taking ACEIs with those who dis-continued.As we remarkedbefore,thereis no consensus on whether ACEIs should be continued until the morning of surgery due to the potential for the development of hypotensionresistanttovasopressors.Thereforewecannot definitivelyrecommendwhetherACEIsshouldbecontinued ordiscontinuedespeciallyifesmololinfusionisusedduring anesthesiainduction.HoweverourresultssuggestthatACEIs shouldbecontinued.
Inconclusion,endotrachealintubationduringanesthesia inductionwithpropofolwasfoundtoprolongQTcandQTcD and increase the HR in hypertensive patients using ACEIs while esmolol infusion at a bolus of 500mcg/kg followed by100mcg/kg/mininfusionpreventedtheseresponses. Fur-thermoreitwasalsofoundthatthebloodpressuretendsto decreasewithesmololduringinductionandcareisneeded.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.ChiangCE.CongenitalandacquiredlongQTsyndrome.Current conceptsandmanagement.CardiolRev.2004;12:222---34. 2.Okin PM,DevereuxRB, Howard BV, et al.Assessment ofQT
intervalandQTdispersionforpredictionofallcauseand cardio-vascularmortalityinAmericanIndians.Thestrongheartstudy. Circulation.2000;101:61---6.
3.BookerPD,WhyteSD,LadusansEJ.LongQTsyndromeand anes-thesia.BrJAnaesth.2003;90:349---66.
4.AyB,FakAS,ToprakA,etal.QTdispersionincreasesduring intubationinpatientswithcoranaryarterydiseases.J Electro-cardiol.2003;36:99---104.
5.ThomsonIR.Thehaemodynamicresponsetointubation:a per-spective.CanJAnaesth.1989;36:367---9.
6.KaplanJD,SchusterDP.Physiologicalconsequencesoftracheal intubation.ClinChestMed.1991;12:425---32.
7.Hawel SJ, Sear JW, Foex P. Hypertension, hypertensive heart disease and perioperative cardiac risk. Br J Anaesth. 2004;92:570---83.
8.PrakashES,MadanmohanSethuramanKR,NarayanSK. Cardio-vascularautonomic regulationinsubjects withnormalblood pressure,high-normalbloodpressureandrecent-onset hyper-tension.ClinExpPharmacolPhysiol.2005;32:488---94.
9.MorganGE,MikhailMS.Anaesthesiaforpatientswith cardio-vasculardisease.In:Clinicalanesthesiology.4thed.Stamford: AppletonandLangePress;2002.p.389---95.
10.Messerli FH. Hypertension and sudden cardiac death. Am J Hypertens.1999;12:181---8.
11.GalinierM,BalanescuS,FourcadeJ,etal.Prognosticvalueof ventriculararrhythmiasinsystemichypertension.JHypertens. 1997;15:1779---83.
14.Pigott DW, Nagle C, Allman K, et al. Effect of omitting regular ACE inhibitor medication before cardiac surgery on haemodynamicvariablesandvasoactivedrugrequirements.Br JAnaesth.1999;83:715---20.
15.Coriat P, Richer C, Douraki T, et al. Influence of chronic angiotensin-convertingenzymeinhibitiononanesthetic induc-tion.Anesthesiology.1994;81:229---307.
16.Saarnivaara L, Klemola UM, Lindgren L, et al. QT interval of theECG,heart rateand arterial pressure using propofol, methohexitalormidazolamforinductionofanaesthesia.Acta AnaesthesiolScand.1990;34:276---81.
17.McConachieI,KeavenyJP,HealyTE,etal.Effectofanaesthesia ontheQTinterval.BrJAnaesth.1989;63:558---60.
18.KleinsasserA,KuenszbergE,LoeckingerA,etal.Sevoflurane, butnotpropofol,significantlyprolongstheQ-Tinterval.Anesth Analg.2000;90:25---7.
19.MichaloudisDG,KanakoudisFS,PetrouAM,etal.Theeffectsof midazolamorpropofolfollowedbysuxamethoniumontheQT intervalinhumans.EurJAnaesthesiol.1996;13:364---8. 20.RobinsonBJ,EbertTJ,O’BrienTJ,etal.Mechanismswhereby
propofol mediates peripheral vasodilation in humans. Sym-pathoinhibitionor directvascular relaxation?Anesthesiology. 1997;86:64---72.
21.HokaS,YamauraK,TakenakaT,etal.Propofol-inducedincrease invascularcapacitanceisduetoinhibitionofsympathetic vaso-constrictiveactivity.Anesthesiology.1998;89:1495---500. 22.Tramer MR, Moore RA, McQuay HJ. Propofol and
brady-cardia: causation, frequency and severity. Br J Anaesth. 1997;78:642---51.
23.Korpinen R, Klemola UM, Simola M, et al. The electro-cardiographic and hemodynamic effect of metohexital and propofolwithand withoutesmolol.ActaAnaesthesiol Scand. 2006;50:188---92.
24.WeisenbergM,SesslerDI,TavdiM,etal.Dose-dependent hemo-dynamic effects of propofol induction following brotizolam
premedication in hypertensive patients taking angiotensin-converting enzyme inhibitors. J Clin Anesth. 2010;22: 190---5.
25.Passino C,MagagnaA, Conforti F,etal. Ventricular repolar-izationis prolonged innondipperhypertensivepatients: role ofleftventricularhypertrophyandautonomic dysfunction.J Hypertens.2003;21:445---51.
26.OikarinenL,ViitasaloM,ToivonenL,etal.Anglo-Scandinavian CardiacOutcomesTrialComparativeeffectsofatenolol-based andamlodipine-basedantihypertensivetherapyonQT disper-sioninhypertensivesubjects.JHumHypertens.2001;15Suppl 1:43---5.
27.GalettaF,FranzoniF,MagagnaA,etal.EffectofnebivololonQT dispersioninhypertensivepatientswithleftventricular hyper-trophy.BiomedPharmacother.2005;59:15---9.
28.KorpinenR,SaarnivaaraL,SirenK,etal.Modificationofthe haemodynamicresponsestoinductionofanaesthesiaand tra-chealintubationwithalfentanil,esmololandtheircombination. CanJAnaesth.1995;42:298---304.
29.KorpinenR,SaarnivaaraL,SirenK.QTintervaloftheECG,heart rateandarterialpressureduringanaestheticinduction: com-parativeeffects ofalfentaniland esmolol.Acta Anaesthesiol Scand.1995;39:809---13.
30.Korpinen R, Simola M, Saarnivaara L. Effect of esmolol on the hemodynamic and electrocardiographic changes during laryngomicroscopyunderpropofol---alfentanilanesthesia.Acta AnaesthesiolBelg.1998;49:123---32.
31.ErdilF,Demirbilek S, BegecZ, et al. The effectof esmolol on the QTc interval during induction of anaesthesia in patientswithcoronaryarterydisease. Anaesthesia.2009;64: 246---50.