w w w . r b o . o r g . b r
Original
Article
Tibiotalocalcaneal
arthrodesis
with
retrograde
intramedullary
nailing:
29
patients’
clinical
and
functional
evaluation
夽
,
夽夽
Thiago
Barbosa
Caixeta,
Márcio
Oliveira
Calábria
Júnior,
Régis
Vieira
de
Castro,
Jefferson
Soares
Martins,
Edegmar
Nunes
Costa,
Alexandre
Daher
Albieri,
Frederico
Barra
de
Moraes
∗DepartamentodeOrtopediaeTraumatologia,HospitaldasClínicas,UniversidadeFederaldeGoiás,Goiânia,GO,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received5January2013 Accepted13May2013
Keywords:
Osteoarthritis Arthrodesis Ankle
Fracturefixation Intramedullary
a
b
s
t
r
a
c
t
Objective:Toevaluateclinicallyandfunctionallythepos-operativeresultsofpatients sub-mittedtotibiotalocalcaneal arthrodesisforthetreatment oftraumaticarthropathyand neuropathy.
Methods:Retrospective study of 29 patients undergoing ankle arthrodesis with intramedullary retrograde nail. All patients were evaluated for fusion time, AOFAS andVASscores,satisfaction,andcomplicationsofsurgery.Themeanfollow-upwas36 months(range6–60months).
Results:Theunionratewas82%,andtheconsolidationoccurredonaverageat16weeks (10–24weeks).Thepos-operativeAOFASscoreimprovedin65.5%(averageof57.7on neu-rologicalcasesand75.7oncasespos-traumatic)andVASscoreimproved94.1%(averageof 2.3onneurologicalcasesand4,2onpost-traumaticcases),and86%ofpatientswere satis-fiedwiththeprocedureperformed.Complicationsoccurredin11patients(38%),including pseudoarthrosis(17.24%),infection(17.24%),materialfailure(13.8%)andfracture(13.8%).
Conclusion:Tibiotalocalcanealarthrodesiswithretrogradeintramedullarynailprovedtobe agoodoptionforsavingtheanklejoint,withimprovementofclinicalandfunctionalscores (AOFAS=65.5%andVAS=94.1%).
©2013SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
Artrodese
tibiotalocalcaneana
com
haste
intramedular
retrógrada:
avaliac¸ão
clínica
e
funcional
de
29
pacientes
Palavras-chave:
Osteoartrite Artrodese
r
e
s
u
m
o
Objetivo:avaliar clínica e funcionalmente o pós-operatório de pacientes submetidos à artrodesetibiotalocalcaneanaparaotratamentodasartropatiastraumáticaseneurológicas dotornozelo.
夽Pleasecitethisarticleas:CaixetaTB,JúniorMOC,deCastroRV,MartinsJS,CostaEN,AlbieriAD,etal.Artrodesetibiotalocalcaneana
comhasteintramedularretrógrada:avaliac¸ãoclínicaefuncionalde29pacientes.RevBrasOrtop.2014;49:56–61.
夽夽
StudyconductedattheDepartmentofOrthopedicsandTraumatology,HospitaldasClínicas,UniversidadeFederaldeGoiás,Goiânia, GO,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](F.B.deMoraes).
2255-4971/$–seefrontmatter©2013SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditoraLtda.Allrightsreserved.
Tornozelo
Fixac¸ãointramedulardefraturas
Métodos: estudoretrospectivode29pacientessubmetidosàartrodesedotornozelocom hasteintramedularretrógrada.Todosospacientesforamavaliadosemrelac¸ãoaotempo deconsolidac¸ão,escoresAofaseEVAegraudesatisfac¸ão,alémdecomplicac¸õesdoato cirúrgico.Otempodeseguimentomédiofoide36meses(variac¸ãode6–60).
Resultados: ataxadeuniãofoide82%eotempomédiodeconsolidac¸ãofoide16semanas (10-24).OcritérioAofasmelhorounopós-operatórioem65,5%(médiade57,7noscasos neurológicosede75,7nospós-traumáticos)eaEVAmelhorou94,1%(médiade2,3noscasos neurológicosede4,2nospós-traumáticos)e86%dospacientesmostraram-sesatisfeitos comoprocedimentofeito.Ascomplicac¸õesocorreramem11pacientes(38%),entreelas pseudartrose(17,24%),infecc¸ão(17,24%),falhadomaterial(13,8%)efratura(13,8%).
Conclusão: aartrodesetibiotalocalcaneanacomhasteintramedularretrógradamostrouser umaboaopc¸ãoparaosalvamentodaarticulac¸ãodotornozelo,commelhoriadoscritérios clínicosefuncionais(Aofas=65,5%eEVA=94,1%).
©2013SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Thetibiotalocalcanealarthrodesisisusedasasalvage proce-durefortheanklejointinpatientswithchangesinthesubtalar junction ofthe tibiotarsaljoint.1–4 Theindications forthis
procedurearemostlypost-traumaticarthrodesis,rheumatoid arthritis, sequelae of infection, neuromuscular conditions, and failures oftotalankle arthroplasty.2,5–11 In 1906,Lexer
described forthe first timethe tibiotalocalcaneal arthrode-siswithintramedullary fixation usingcadaveric bonegraft amongthe calcaneus,talusandtibia.12 Sincethe
introduc-tionoftheconceptofanklearthrodesisbycompressionby Charnleyin1951,morethan30techniquesandanumberof technicalmodificationshavebeendescribed.8
Patientswithanklearthropathyoftenpresentwithbone loss, osteopenia or severe deformities (Figs. 1 and 2A/B), which hinders the arthrodesis fixation.2,11,13,14 The
lit-erature has pointed to high infection rates (10–20%) and pseudoarthrosis6,12,15 (10–20%)8 associated with
arthrodesis,especially for the treatmentof neuromuscular arthropathies.5,12,13
Intramedullary fixation in tibiotalocalcaneal arthrodesis representsamodernapproach,withtheadvantageof promot-ingrigidinternalfixationwithminimalperiostealaggression and vascular damage.6,7,15 In addition, the procedure
pro-motescompressioninthefocusofthearthrodesis,withhigh consolidationratios(85%)andanaveragearthrodesisfusion timeofapproximatelythreemonths.14,15However,the
proce-dureisnotfreeofcomplications(30–80%inmostseries).7,14
Thepresentstudyaimedtoevaluateclinicallyand func-tionally patients undergoing tibiotalocalcaneal arthrodesis usingalockedretrogradeintramedullary nailforthe treat-mentofneurologicalandtraumaticarthropathyoftheankle andsubtalarjoint.
Materials
and
methods
Thisisaretrospectivestudywithaconveniencesampleof29 patientswitharthrosisofankleandsubtalarjointsby trau-maticandneurologicalcauses.Themeanagewas41.3years (13–72), and 15 patients (51.7%) were male and 14 (48.3%)
females.Regarding etiology,16 patientshadpost-traumatic arthropathy(55.2%),andin13(44.8%)thelesionhad neuro-logiccauses(Charcotarthropathy,sequelaeofcerebralpalsy andpolio).Theaveragefollow-uptimewas36months(6–60) afterthearthrodesis.
Thesurgicaltechniqueemployed,fromJanuary2005to Jan-uary2011,wastibiotalocalcanealarthrodesiswithretrograde intramedullary nailingofthe ankle.Thesurgicaltechnique followsaprotocolwiththepatientinthelateralposition.By alateralaccessportof10cm,anosteotomyismadeatright anglestotheresectionofdistalfibula.Thejointsurfacesofthe talusanddistaltibiaaredecorticatedbythisaccess.Amedial accessisusedtofacilitatejointdebridementandplacement ofthetalusandthemedialmalleolus.Thesurgeonremoves minimalamountsofbonetopreventshorteningofthelimb. Amedialaccessisusedtofacilitatejointdebridement and placementofthetalus,withthemedialmalleolus.Tomake thefixationwiththeintramedullarynail,thesurgeonmakes anincisionatthejunctionofmiddleanddistalthirdsofthe fatpadoftheheel.Thefootisheldinthedesiredposition; thenthesurgeonpassesaguidewirethroughthecalcaneus andthetalustoreachthecenterofthetibia.Thepositionis checkedintheimageintensifierandthenthe surgeon pro-ceedswiththemilling.Usually,weusethe12mm-nailand the millingis done up to11mm. Afterthe removal ofthe intramedullaryguidewire,thelockingscrewsareinserted per-cutaneouslywiththedrillguide.Weusetwomedialscrews into the tibiaforthe proximallocking,and onescrewinto thetalusandcalcaneusforthedistallocking.Thisprocedure doesnotallowtheshank’sdynamisation,becauseitresults onlyinstaticlocking.Theprocedureswereperformedbythe surgeryofthefootandanklestaff,whoaremembersofthe DepartmentofOrthopedicsandTraumatology, Hospitaldas Clínicas,FederalUniversityofGoiás(UFG-DOT-HC).Thestudy wasapprovedbytheethicscommitteeoftheHC-UFG.
Fig.1–Clinicalappearanceofsequelaeofrighttibialpylonfracture,andevolutionwithinfection.Attemptedarthrodesis wasperformedwithanexternalfixator,withoutsuccess.Thelesionevolvedtoinfectionhealingwithpain,howeverwith mobilityinthefocusofarthrodesis,valgusdeformityofankle,andinabilitytomarch.
VAS(betweeneightand10)wereselectedpreoperativelyfor thearthrodesisprocedure.Aftersurgeryandaftersixmonths ofevolution,thesamepatientsansweredagaintothe ques-tionnaires(AOFASandVAS).Later,wedividedthecasesinto twogroups,accordingtotheetiologyofthearthrosis (trau-maticorneurological)andevaluatedthefollowingvariables: time for the consolidation, smoking habits (more than 20 cigarettes/day),patientsatisfactionandpost-operative com-plications.Thejointfusionwasassessedbyradiographsofthe ankle(anteroposterior[AP]andlateralviews)(Fig.3AandB) andhavebeen consideredasapseudoarthrosisincasesin whichtherewerenosignsofbonehealingandosseous tra-beculationintheAPandlateralviewsuptosixmonths(24 weeks)aftersurgery.
The statistical analysis was descriptive and analytical, using Fischer’sexact and chi-squared testsand comparing
Fig.2–Anteroposterior(A)andlateral(B)ankle
radiographs,depictingnon-consolidationoftheprevious arthrodesis,valgusdeformityandjointdegeneration.
qualitativevariablesbyfrequency.Thedatabaseisstoredin theMicrosoftExcelprogramandanalyzedusingSPSSversion 15.0.
Results
In the evaluation ofthe AOFAS questionnairein the post-operativeperiod,wenotedimprovedscores,whencompared withthevaluesinthepreoperativeperiod,sinceourfindings were34.5%poor(10cases),20.7%fair(sixcases),34.5%good (10cases),and10.3%excellent(threecases)(Table1).When analyzedbyetiology,thepost-operativeAOFASfortraumatic cases(mean75.7)was21.2%bettervs.neurologicalcases(57.7) (Fig.4).
Regarding the VAS questionnaire(Table 2), in the post-operative period we found 48.3% mild (14 cases), 44.8%
Table1–ComparisonbetweenAOFAScriteriain pre-andpost-operativeperiod.
AOFAS Preoperative Post-operative
Poor 29 10 34.5%
Fair 0 6 20.5 65.5%
Good 0 10 34.5%
Excellent 0 3 10.5
0
AOFAS post (0-69 points)
AOFAS post (70-80 points)
AOFAS post (80-90 points)
AOFAS post (90-100 points)
1 2 3 4 5 6 7
Traumatic Neurological
Fig.4–ComparisonbetweenAOFAScriteria post-operativelyaccordingtoetiology(traumaticvs. neurological).
moderate(13cases),and6.9%severe(twocases)–an improve-mentof94.1%(averageof2.3inneurologicalcasesand4.2in post-traumaticcases).Therateofsatisfactionwiththe proce-durewas86%(25of29patients).Ofthe29patients,12were smokers(41.4%).
Of the 29 patients, the arthrodesis consolidation was radiographicallyconfirmedin24(82%),andfive(17.2%)had nonunions.Theaveragehealingtimewas16weeks(10–24). Althoughweobservedatrendtowardanassociationbetween smoking and nonunion (pseudoarthrosis more frequent in smokers)andbetweennonunionandneurologicaletiology,no statisticalsignificancewasobserved,probablybecauseofthe smallsamplesize.
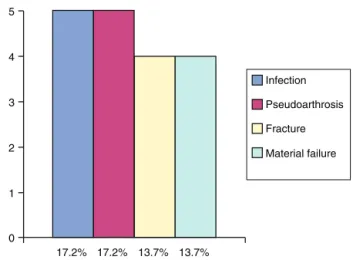
Regardingcomplications,11patients(38%)developedsome kindofcomplication.Ofthose,fivehadmorethanonetypeof complication.So,in29patients,18complicationsoccurred:5
Table2–ComparisonofVisualAnalogScaleforpainin pre-andpost-operativeperiod.
VAS Preoperative Post-operative
Mild 0 14 48.3% 94.1%
Moderate 0 13 44.8%
Severe 29 2 5.9%
VAS,VisualAnalogScale.
0
17.2% 17.2% 13.7% 13.7%
Infection
Pseudoarthrosis
Fracture
Material failure
1 2 3 4 5
Fig.5–Post-operativecomplicationsoftibiotalocalcaneal arthrodesis.
(17.2%)nonunions,5(17.2%)infections,4(13.7%)tibial frac-turesand4(13.7%)materialfailures(Fig.5).
Discussion
Thetreatmentofpatientswitharthritis,painanddeformity oftheankleandsubtalarjunctionisstillachallengeandis extremelydifficulttogetexcellentresults.Themainsurgical goalsofthetibiotalocalcanealarthrodesisaretoreducepain and promoteastableand plantigradefootwithgood func-tionfordeambulation.1,4,9Thisisaprocedurewithhighrisk
ofcomplications.However,inrecentyearstheprocedurehas gainedacceptanceasanoptionforsavingthetibiotarsaland subtalarjoints.2,6,12–15(Table3).
Inthelastdecade,anumberofstudiesreporting complica-tionsandhighratesofnonunion(4–24%)waspublished.13,15,16
Nonunionisnotuncommon,mainlyincasesofsurgical re-approaches,aspreviouslyreportedbyKimetal.14Chouetal.17
reported unionin86%oftheir patientswith amean of19 weeks(12–65).Boeretal.2publishedaminimumconsolidation
periodof12weeks,withameanof20.4weeks(12–72). Men-dicinoet al.12obtained95%offusionsatapproximately4.1
months(17weeks).Niinimäkiet al.15reportedradiographic
signals offusionin26 (76%)of34 patientsafter16 weeks. Peltonetal.6reported88%offusionatameanperiodof3.7
months(16weeks).Hammettetal.13achievedcompletefusion
ofthearthrodesisin88.46%oftheirseriesof52patientsin aboutfourmonths(17weeks).Weobtainedafusionrateof 82.7% inour29patients ata meantimeof3.6months(16 weeks)–findingssimilartotheaverageobservedinthe liter-ature.
In2007,Smithetal.16prospectivelyanalyzedAOFASand
VAS criteria in 10 patients. These authors found a signifi-cant increase of these criteria, with a preoperative AOFAS of39(range14–51) thatincreasedto69(range51–91) post-operatively.16 VAS was also evaluated prospectively and
rangedfrom8.3pointsinthepreoperativeperiodto2points aftertheoperation.16inourseriesof29cases,wealsoobserved
Table3–Comparisonofresultsamongstudiesintheliterature.
Study Pat.Nr. Age Follow-up
(months) Union rate Timefor consolidation (weeks)
AOFAS VAS Satisfaction
Chouetal.17 37 53(19–79) 26(12–168) 86% 19(12–65) 66 – 87%
Hammettetal.13 47 57.1(25–81) 34(8–37) 87% 17(13–39) 63(13–84) – 82%
Peltonetal.6 33 54(32–88) 14 88% 16 – – –
Boeretal.2 50 57.6(22–82) 51(12–84) 96% 20.4(12–72) 70(32–86) – 92%
Niinimäkietal.15 34 57(25–77) 24(6–43) 76% 16(6–45) – 1.9 90%
Smithetal.16 10 60.6(48–78) 14.7(12–18) 80% – 69(14–51) 2(0–7) –
Mendicinoetal.12 19 56(33–81) 19.8(8–42) 95% 17 – – –
Thisstudy 29 41(13–72) 36(6–60) 82% 16(10–24) 69(16–96) 3.5(0–6) 86%
VAS,VisualAnalogScale.
allourcasesevaluatedwaspoorpreoperatively;aftersurgery, themean was69points(range12–96points).VAS hasalso evolved considerably, from a severe pain preoperatively in 100%ofcases,toameanof3.5points.Onlytwopatients(6.9%) remainedwithseverepainpost-operatively.
OtherauthorsalsousedintheirseriestheAOFAScriteria, butonlyafterthesurgery.ThiswasthecaseofBoeretal.,2with
ameanof70pointsinthisregard.Hamettetal.13obtainedan
averageof63points.Chouetal.17foundameanof66points.
Inourstudy,themeanscorebyAOFAS’criteriawas69points (range12–96).
IntheseriesofBoeretal.2therewasonlyonecomplication.
Thepatienthadsensorylossonthedorsumofthefootand radiolucencyatthenailentrypoint.Niinimäkietal.15reported
15%ofcomplicationsin34patients,fourpost-operative infec-tions (two patients in need of implant removal) and one caseofvenousthromboembolism.Smithetal.16reported20%
ofcomplications(nonunions)andrelatedthisoccurrenceto smoking.
Patientsatisfactionwiththeprocedurewasalsoone cri-terionassessedinour study;whencomparedwithdata in theliterature,therewasdiscordanceoffindings.Chouetal.17
found87%satisfactionwiththepost-operativeresult.Intheir series,Hammettetal.13reported82%satisfaction.Boeretal.2
reported92%satisfactionoftheirpatients.Niinimäkietal.15
obtained 90% satisfaction. In our study, 25 of 29 patients (86.2%)weresatisfiedwiththetreatment.
Conclusion
InourstudywefoundafavorableevolutionofAOFAS crite-ria, of 65.5% (mean of 57.7 in neurological and 75.7 in post-traumaticcases) andofVAS,of94.1%(mean of2.3in neurologicaland4.2inpost-traumaticcases)inthepatients assessed.Despitetheincompleteimprovementofpain,most patients(86%)weresatisfiedwiththeendresult.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.O’NeillPJ,LogelKJ,ParksBG,SchonLC.Rigiditycomparisonof lockingplateandintramedullaryfixationfor
tibiotalocalcanealarthrodesis.FootAnkleInt. 2008;29(6):581–6.
2.BoerR,MaderK,PennigD,VerheyenCC.Tibiotalocalcaneal arthrodesisusingareamedretrogradelockingnail.Clin OrthopRelatRes.2007;(463):151–6.
3.LoweryNJ,JosephAM,BurnsPR.Tibiotalocalcaneal arthrodesiswiththeuseofahumerallockingplate.Clin PodiatrMedSurg.2009;26(3):485–92.
4.NoonanT,PinzurM,PaxinosO,HaveyR,PatwardhinA. Tibiotalocalcanealarthrodesiswitharetrograde
intramedullarynail:abiomechanicalanalysisoftheeffectof naillength.FootAnkleInt.2005;26(4):304–8.
5.AhmadJ,PourAE,RaikinSM.Themodifieduseofaproximal humerallockingplatefortibiotalocalcanealarthrodesis.Foot AnkleInt.2007;28(9):977–83.
6.PeltonK,HoferJK,ThordarsonDB.Tibiotalocalcaneal arthrodesisusingadynamicallylockedretrograde intramedullarynail.FootAnkleInt.2006;27(10):759–63.
7.AlfahdU,RothSE,StephenD,WhyneCM.Biomechanical comparisonofintramedullarynailandbladeplatefixation fortibiotalocalcanealarthrodesis.JOrthopTrauma. 2005;19(10):703–8.
8.PickeringRM.Artrodesedetornozelo,joelhoequadril.In: CanaleST,editor.CirurgiaortopédicadeCampbell.10aed. Barueri:Manole;2006.p.155–78.
9.MeansKR,ParksBG,NguyenA,SchonLC.Intramedullarynail fixationwithposterior-to-anteriorcomparedtotransverse distalscrewplacementfortibiotalocalcanealarthrodesis:a biomechanicalinvestigation.FootAnkleInt.
2006;27(12):1137–42.
10.BennettGL,CameronB,NjusG,SaundersM,KayDB. Tibiotalocalcanealarthrodesis:abiomechanicalassessment ofstability.FootAnkleInt.2005;26(7):
530–6.
11.SantangeloJR,GlissonRR,GarrasDN,EasleyME.
Tibiotalocalcanealarthrodesis:abiomechanicalcomparison ofmultiplanarexternalfixationwithintramedullaryfixation. FootAnkleInt.2008;29(9):936–41.
12.MendicinoRW,CatanzaritiAR,SaltrickKR,DombekMF,Tullis BL,StatlerTK,etal.Tibiotalocalcanealarthrodesiswith retrogradeintramedullarynailing.JFootAnkleSurg. 2004;43(2):82–6.
14.KimC,CatanzaritiAR,MendicinoRW.Tibiotalocalcaneal arthrodesisforsalvageofsevereankledegeneration.Clin PodiatrMedSurg.2009;26(2):283–302.
15.NiinimäkiTT,KlemolaTM,LeppilahtiJI.Tibiotalocalcaneal arthrodesiswithacompressiveretrogradeintramedullary nail:areportof34consecutivepatients.FootAnkleInt. 2007;28(4):431–4.
16.SmithJW,MooreTJ,FlemingS,PochatkoD,PrincipeR. Tibiotalocalcanealarthrodesiswitharetrograde intramedullarynail.FootAnkleInt.2007;19(16): 433–6.