SOCIEDADE BRASILEIRA DE ORTOPEDIA E TRAUMATOLOGIA
w w w . r b o . o r g . b r
Original
Article
Does
the
suction
drain
diameter
matter?
Bleeding
analysis
after
total
knee
replacement
comparing
different
suction
drain
gauges
夽
Marcos
George
de
Souza
Leao
∗,
Gladys
Martins
Pedroza
Neta,
Thiago
Montenegro
da
Silva,
Yacov
Machado
Costa
Ferreira,
Waryla
Raissa
Vasconcelos
Dias
Fundac¸ãoHospitalAdrianoJorge,Servic¸odeOrtopediaeTraumatologia,Manaus,AM,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received27November2015 Accepted7January2016 Availableonline30August2016
Keywords:
Bloodloss/surgical
Arthroplasty/replacement/knee Drainage
a
b
s
t
r
a
c
t
Objectives: Toevaluatebleedingandtheestimatedbloodlossinpatientswhounderwent total kneereplacement(TKR)withdifferentclosedsuctiondrains(3.2-mmand4.8-mm gauge).
Methods:Thiswasarandomizedcontrolledtrialwith22patientswhounderwentTKRand weredividedintotwogroups:GroupI,with11patientsinwhomthe3.2-mmsuctiondrain wasused,andGroupII,with11patientsinwhomthe4.8-mmsuctiondrainwasused. Thehematocritwasmeasuredafter24,48and72haftersurgeryinordertocalculatethe estimatedbloodloss.Thedrainedvolumewasmeasured3,6,12,24,and48hafterTKR,and thereafterbothgroupswerecompared.
Results:Regardingthehematocrit,therewerenodifferencesbetweengroupsinmeasured periods(24,48,and72haftersurgery).Thetotalbleedingmeasuredatthesuctiondrains within48hwashigherinGroupII,withastatisticallysignificantdifference(p=0.005);in thefirst24h,therewasmajorbleedinginGroupII(mean893mL),withasignificant differ-ence(p=0.004).Between24and48h,therewasnostatisticallysignificantdifferenceinboth groups(p=0.710).ThetotalestimatedbleedingwashigherinGroupI,withmeanof463mL,
versus409mLinGroupII,withnostatisticalsignificance(p=0.394).
Conclusions: Bleedingwashigherinthegroupthatusedthe4.8mmgaugesuctiondrain, withnodifferencesinhematocritandestimatedbloodloss.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
夽
StudyconductedattheFundac¸ãoHospitalAdrianoJorge,Servic¸odeOrtopediaeTraumatologia,Manaus,AM,Brazil. ∗ Correspondingauthor.
E-mail:[email protected](M.G.Leao). http://dx.doi.org/10.1016/j.rboe.2016.08.014
A
espessura
do
dreno
suctor
importa?
Análise
do
sangramento
após
artroplastia
total
do
joelho
comparando
drenos
suctores
de
diferentes
calibers
Palavras-chave:
Perdasanguíneacirúrgica Artroplastiadojoelho Drenagem
r
e
s
u
m
o
Objetivos:Avaliarosangramentoatravésdodrenosuctor(DS)eaperdasanguíneaestimada empacientessubmetidosàartroplastiatotaldojoelho(ATJ)comDSdediferentescalibers (3,2mme4,8mm).
Métodos: Ensaioclínicorandomizadocom22pacientessubmetidosà ATJ,divididos em doisgrupos;nogrupoI,ospacientesrecebiamoDS3,2mmenoGrupoII,oDS4,8mm.O hematócritofoiaferido24,48e72horasapósacirurgia,afimdecalcularaperdasanguínea estimada.Odébitododrenofoimedido3,6,12,24e48horasapósaATJeosdoisgrupos foramcomparados.
Resultados: Emrelac¸ãoaohematócrito, nãoseobservaramdiferenc¸asestatisticamente significativasentreosgruposnosperíodosaferidos(24,48e72horaspós-operatória).O sangramentototalmedidonoDSnas48horasfoimaiornogrupoII,comdiferenc¸a esta-tisticamentesignificativa(p=0,005);nasprimeiras24horas,houvemaiorsangramentono grupoII(média893mL),comdiferenc¸asignificativa(p=0,004).Entre24e48horas,nãoforam observadasdiferenc¸asestatisticamentesignificativasemambososgrupos(p=0,710).O san-gramentototalestimadofoimaiornoGrupoI,commédiade463mL,enquantonoGrupoII essevalorfoide409mL,semsignificânciaestatística(p=0,394).
Conclusões: OsangramentofoimaiornogrupoqueusouDS4,8mm,semdiferenc¸asno hematócritoenaperdasanguíneaestimada.
©2016SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCCBY-NC-ND(http:// creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Theuseofawoodentubeasadrainintoawoundiscredited toHippocrates,ataround400BC.1
Total knee replacement (TKR) is a standardized surgi-cal procedure with high success rates in the treatment of advanced degenerative osteoarthritis (OA) and rheumatoid arthritis of this joint. Substantial bleeding can occur in the subcutaneous and intra-articular space after TKR; this event can lead to blood transfusions, with their potential complications.2 Drainage is commonly used with the the-oreticalpurpose ofpreventinghematomas, which, in turn, maydecreasejointmobilityandreducelocaltissueperfusion, increasingthepossibilityofinfection.Thus,drainscanalsobe usedtolowertheriskofinfectionandpreventhealingdelay inTKR.3
Primary TKR canlead toa reductioninthe erythrocyte levels.Variousstrategieshavebeenusedinordertoreduce the need forblood products,such as tourniquet placedat thethighroot,coagulationdiathermy,kneeposition,clamped drains, infiltration withvasoconstrictor solutions, antifibri-nolytics(tranexamic acid,Floseal®), and computer-assisted surgeries.4
The use of suction drains (SD) in arthroplasties is still controversial.Itisbelievedthatthedrainageislimitedonly to a restricted area, failing to prevent infection if retro-grademigrationofbacteriaoccurs.Drainscanalsohamper rehabilitationintheimmediatepostoperativeperiod.There
is no obvious advantage of using SDs, other than lower need for dressing changes during surgery; moreover, in patientsundergoingTKRwithSDs,theriskoftransfusionis higher.5
With the aging population, there has been increasing demand for joint replacements, which are effective meth-odstoimprovethequalityoflifewithrecoveryofmovement and improvement in pain, although these surgeries cause large blood loss and lead to dramatic consequences in patientswithchronicillnesses;inprosthesisrevision surger-ies,the losses maybehigher.There areformulastobetter estimate blood loss; they are applied in studies to com-pare blood lossbetweendifferent techniquesperformedin surgery.6
Todate,itisknownthatthereisnodifferenceregarding rate of surgical site infection and problems with surgi-cal wound or postoperative rehabilitation, whether or not drains are used; thereis a tendency togreater blood loss, hematomaformation, higherrateofuseofbloodproducts, anddelayinrecoveryofjointfunctionwhentheyareused.7 In most publications that address TKRs with or without the use ofSD, the study focus is bleedingand the rateof complications.5
Material
and
methods
Thisrandomizedclinicaltrialwith22patientsundergoingTKR wasconductedbetweenAprilandOctober2015.
Aprotocolwascreatedforthestudy.Patientswhomet eligi-bilitycriteriaforTKRwereassignedrandomlyintotwogroups (regardlessofage,gender,anddeformity):GroupIuseda 3.2-mmdiameterPortovacSD,andGroupII,a4.8-mmdiameter PortovacSD,installedinthejointspacepriortotheclosureof thecapsule.
The study included patients regularly registered in the institution where the study was performed, who met the classical indicationforTKR advocatedbyCamanho etal.8: medialorlateralimpingementwithobliterationofthejoint space,varusfemorotibialalignmentgreaterthan15◦;valgus femorotibialalignmentgreaterthan10◦;tibiofemoral sublux-ationinthefrontalplanegreaterthan10mm;anteriorization ofthetibiarelativetothefemurintheprofileX-ray;severe impairmentoftwoofthethreejointcompartmentsoftheknee (medialtibiofemoral,lateraltibiofemoral,orpatellofemoral), andfailedconservativetreatmentforatleastthreemonths when these criteria were not met. Patients with primary degenerativeosteoarthritisoftheknee.Forthisassessment, patientswithosteoarthritis ofthe knee ≥stageIII(Ählback modifiedbyKeys)wereconsidered.9,10
Exclusioncriteriacomprisedpatientsundergoingrevision surgery,thoseinwhomthemedialjointaccesswasnotused, thosewhowerenotoperatedbytheseniorsurgeon,thosewith rheumatoidarthritisormultiplescars,andthosewhorefused tosign or did notunderstand the informed consentform. Anypatient withdecompensateddiabetes mellitus(fasting blood glucose >140mg/dL), uncontrolled hypertension (SBP >200mmHg), peripheral vascular disease, previous throm-boembolism,neoplasia,activeinfection,rheumatoidarthritis, obesewithabodymassindexgreaterthan35kg/m2,orthose withahighsurgicalrisk(AmericanSocietyof Anesthesiolo-gists[ASA]score>III)hadtheirmedicalconditionre-evaluated andsurgerywaspostponed.
Patientswhometinclusioncriteriaforthisstudy(22)were randomizedintogroupsaccordinglytothewaitinglistforthe procedure.Uponadmission,thefirstpatientwasassignedto GroupI,second,toGroupIIandsoon;thus,odd-numbered patients were assigned to Group I and even-numbered, to GroupII. The researcherhad no influence onthe decision process ofwho would beoperated; onlyatthemoment of draininsertionwashemadeawareofwhichgroupthepatient belongedto.
The night before surgery, hemoglobin and hematocrit (Hb-pre,Ht-pre)levelsweremeasured.Thesevalueswere con-sideredascontrols;patientswereweighedinkilogramsand theirheightwasmeasuredincentimeters.
Patients underwent spinal anesthesia and received a prophylacticdoseofantibiotics–cefazolin2g–bythe anes-thesiologist.Apneumatictourniquetwasappliedontheroot ofthethighofthe limbto beoperated,withapressure of 300mmHgforallpatients.Surgicaltechniqueadoptedwasthe standardTKRwithjointaccessviaaclassictrans-quadriceps approachandpatellareversion.Authors’ routineistheuse
ofintramedullaryguidesforfemoralcutsandextramedullary guidesfortibialcuts.Theposteriorcruciateligament(PCL)was resectedinallprocedures.Thepatellawasnotresurfaced,and waspreparedinallcasesasfollows:afterlocaldenervation andsynovectomy,toavoidclunksyndrome,thepatellawas eburnatedandneurotized,andalateralfasciotomywas per-formed.TheprosthesisusedwastheAKSModularBloqueada® (Baumer,MogiMiring,SP,Brazil),anon-PCL-sparing prosthe-sis.PortovacSDs of3.2mmand4.8mmwereplacedinthe jointspacebeforecapsularclosure.Inordertostandardizethe drainagearea,alltheendsofthedrainswerecutsothatthey were10cmlonginthejointandthelateralrecess.The Por-tovacdrainisapost-operativepolyethylenecloseddrainage system, whoseresistanceisdesignedforacontinuous and mildsuction.Ithasavacuumpumpwithacapacityof500mL, withanattachment cord,anintermediate sectionmadeof polyvinylchloride(PVC),aclamp, atwo-orthree-way con-nector,andadrainagecatheterwithasurgical-gradestainless steelneedle (3.2mm,4.8mm,or 6.4mm),used topuncture the drainpassagesite.11 After woundclosure, an inguinal-malleolar compressive occlusiveRobert Jones dressing was applied.Ifsurgerylastedover2h,thetourniquetwasdeflated andtheischemiawasreleased;subsequently,hemostasiswas assessed,insertingdrains,sutures,anddressings.All surger-ies were always performed bythe principal investigatoror underhisdirectassistance.Bloodlosswasmeasuredthough serialHbandHtcountsat24,48,and72h(thelast measure-mentwasconsideredastheHb-postandHt-post)andthrough bloodvolume,seriallymeasuredontheSDat3,6,12,24and 48haftertheendofthesurgicalprocedure.Inthislast mea-surement,theSDwasremovedanddressingwaschanged.The surgeonwasnotinvolvedinthemeasurementofSDvolumes. All patients received thromboprophylaxis with enoxaparin sodiumatadoseof40mgsubcutaneous6hafterthe proce-dure,administeredonceadayfor15days.Allpatientsreceived prophylaxisforsurgicalsiteinfectionwithcefazolinsodium atadoseof1gevery8hforfivedays.
Withthedataonweight,height,andHt-pre,Hb-pre, Ht-post,andHb-post,bloodvolumeofthepatientwascalculated according tothe formula ofNadler et al.,12 and blood loss wasestimatedaccordingtothemethodproposedby Mercuri-aliandInghilleri.13Inthepresentstudy,theauthorschoseto usethethree-daypostoperativehematocritforcalculationof bloodloss,insteadofthefive-dayoriginallydescribed.
Blood volume=Males: 604+0.0003668×height (cm3) +32.2×weight(kg).
Women:183+0.000356×height(cm3)+33×weight(kg). Estimated blood loss: =blood volume×(Ht-pre− Ht-post)+redbloodcellvolume(CH).
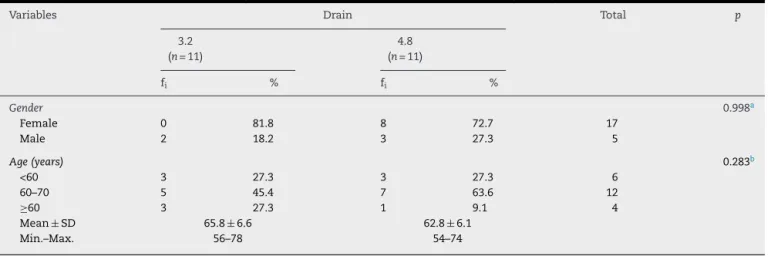
Table1–Distributionbyfrequencyofgenderandageinrelationtosuctiondraingroup(3.2mm×4.8mm).
Variables Drain Total p
3.2 (n=11)
4.8 (n=11)
fi % fi %
Gender 0.998a
Female 0 81.8 8 72.7 17
Male 2 18.2 3 27.3 5
Age(years) 0.283b
<60 3 27.3 3 27.3 6
60–70 5 45.4 7 63.6 12
≥60 3 27.3 1 9.1 4
Mean±SD 65.8±6.6 62.8±6.1
Min.–Max. 56–78 54–74
fi,simpleabsolutefrequency;SD,standarddeviation. a Fisher’sexacttest.
b Student’st-testwasusedtocomparethemeans.
TheEpi-Infosoftwareversion7.1.5forWindows,whichis developedand freelydistributedbytheCentersforDisease ControlandPrevention(www.cdc.gov/epiinfo/7),wasusedfor statisticalanalysis.15
Allpatientsreadandsignedainformedconsentform;the studywassubmittedtotheResearchEthicsCommittee(REC) ofthe institution, withCertificate ofPresentation for Ethi-calAssessment(CAAE)No.43085615.8.0000.0007,andreceived RECopinionNo.1019123.
Results
GroupIconsistedof11patients,ninefemalesandtwomales, aged56–78years,withameanof65.8yearsandSD±6.6years. GroupIIconsistedofeightfemalepatientsandthreemales, withameanageof62.8years(54–74,SD±6.1years). Epidemi-ologicaldataaresummarizedinTable1.
IntheobservationoftheSDbleedingcurveat3,6,12,24, and48h(Fig.1),adecreasewasobservedfrom3honwards; nostatisticallysignificantdifferenceswereobservedforboth groups, except for the interval between 3 and 6h, with increasedbleedinginGroupII(p=0.001).
Regardinghematocrit,accordingtoFig.2,nostatistically significantdifferenceswereobservedbetweenthegroupsin themeasuredperiods(24,48,and72hpostoperative),andthe downwardcurveremainedstablefrom24honwards,witha constantpattern.
ThetotalbleedingmeasuredintheSDwithin48h(Fig.3) washigherinGroupII(mean920mL)thaninGroupI(680mL), withstatisticallysignificantdifference(p=0.005);whensuch bleedingwasstratifiedinto24and48h,itwasobservedthat withinthe first24h (Fig. 4),therewas ahigherbleedingin GroupII (mean893mL),with statisticallysignificant differ-ences(p=0.004).Between24and48h(Fig.5),nostatistically significantdifferenceswereobservedinbothgroups(GroupI: 24mL×GroupII:27mL),p=0.710.
Drain 48h 24h 12h 6h 3h 4.8 3.2 4.8 3.2 4.8 3.2 4.8 3.2 4.8 3.2 500 400 300 200 100 0 mL 401 356 241 127 151 111 100 62 27 24 10.06 44.49 10.79 36.48 59.58 140.42 32.26 91.38 111.00 190.82 75.81 146.92 184.42 297.39 88.75 164.89 301.42 500.39 287.70 425.02
*P=.421 *P=.001 *P=.115 *P=.105 *P=.710
* Student’s t-test. Bold and italic p-values indicate statistically significant difference at the 5% level.
Fig.1–Distribution,accordingtothemeanand95%CI,of bleedingat3,6,12,24,and48h,inrelationtoSDthickness. CI,confidenceinterval;SD,suctiondrain.
Drain 72h 48h 24h Pre 4.8 3.2 4.8 3.2 4.8 3.2 4.8 3.2 40 35 30 25 20 % 36.1 37.3 28.8 29.1 26.7
27.3 27.7 28.1
26.22 30.02 24.92 30.39 24.87 28.48 23.95 30.63 26.67 30.91 25.22 32.89 33.79 38.43 34.96 39.64
*P=.430 *P=.894 *P=.720 *P=.760
* Student’s t-test
Fig.2–Distribution,accordingtothemeanand95%CI,of preoperativehematocritat24,48,and72hpostoperatively inrelationtoSD.
4.8 3.2
1.100
1.000
900
800
700
600
Drain
P=.005 (Student’s t-test).
mL
920
680
789.00 1051.00
576.14 783.86
Fig.3–Distribution,accordingtothemeanand95%CI,of thetotalbloodlossinrelationtoSDthicknessinpatients whounderwenttotalkneereplacement.
CI,confidenceinterval;SD,suctiondrain.
EstimatedbloodlossbytheformulaproposedbyMercuriali andInghilleri14(Fig.6)washigherinGroupI,withameanof 463mLversusGroupII,409mL,withnostatisticalsignificance,
p=0.394.Theuseofbloodproductswassimilarinbothgroups –twounitsofredblood cellswith300mLeachunit.Inthe studyperiod,therewasonlyonecaseofcomplicationinGroup II:blisterformationinthewoundofapatientwhorequiredtwo concentratedunitsofredbloodcells.
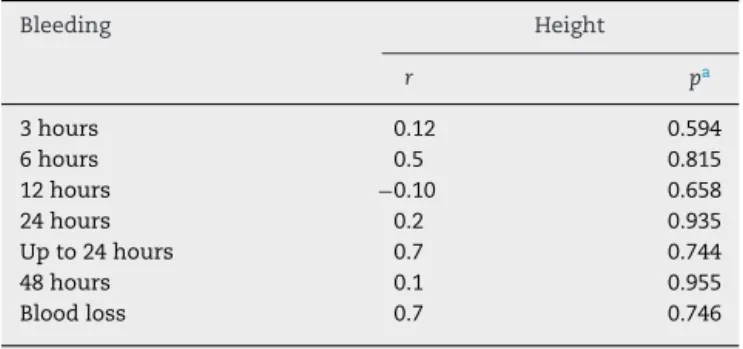
Student’st-testwasusedtoassesswhether therewas a correlationbetweenbleedingandheight,andbetweenweight andbleeding.Nocorrelationswereobservedbetweenthese variables(Tables2and3),inwhichthevaluesofthecoefficient closestto1and−1indicateastrongevidenceofcorrelation.
Discussion
Although there is no established evidence to confirm the use of drains in TKR, it is postulated that it can reduce hematoma formation and the incidence ofdeep infection. Esleretal.16suggestthattheseperceptionsareincorrect,as
4.8 3.2
1.100
1.000
900
800
700
600
500
Drain
mL
893
656
766.72 1018.74
554.69 758.04
P=.004 (Student’s t-test).
Fig.4–Distribution,accordingtothemeanand95%CI,of bleedinginthefirst24hinrelationtoSDthickness. CI,confidenceinterval;SD,suctiondrain.
4.8 3.2
50
40
30
20
10
Drain
mL 27
24
10.06 44.49
10.79 36.48
P=.710 (Student’s t-test).
Fig.5–Distribution,accordingtothemeanand95%CI,of bleedinginbetween24and48hinrelationtoSDthickness. CI,confidenceinterval;SD,suctiondrain.
4.8 3.2
600
550
500
450
400
350
300
250
Drain
mL 409
463
309.37 507.90
364.96 561.58
P=.394 (Student’s t-test).
Fig.6–Distribution,accordingtothemeanand95%CI,of theestimatedbloodloss(MercurialliandInghilleri13)in relationtoSDgaugeinpatientswhounderwenttotalknee replacement.
CI,confidenceinterval;SD,suctiondrain.
theirstudyfailedtodemonstrateastatisticallysignificant ben-efitwiththe useofintra-articulardrain oncementedTKR. TheuseofSDsmayevenbeharmful.Surgeonsare usedto place drainsand the fearofmorbidity ofdeepinfection is
Table2–Correlationofbleedingtimeandheightof
patientswhounderwenttotalkneereplacement.
Bleeding Height
r pa
3hours 0.12 0.594
6hours 0.5 0.815
12hours −0.10 0.658
24hours 0.2 0.935
Upto24hours 0.7 0.744
48hours 0.1 0.955
Bloodloss 0.7 0.746
r,correlationcoefficient.
Table3–Correlationofbleedingtimeandweight(inkg)
ofpatientswhounderwenttotalkneereplacement.
Bleeding Weight
r pa
3hours 0.3 0.886
6hours 0.39 0.72
12hours −0.1 0.977
24hours −0.12 0.568
Upto24hours 0.16 0.486
48hours 0.23 0.295
Bloodloss 0.18 0.430
r,correlationcoefficient.
a t-Testforcorrelation.
understandable;therefore,thereisresistancetochangingthis practice.
Parkeret al.17 foundthattheonlydefiniteadvantageof usingdrains,demonstratedinameta-analysis,wastoreduce the bleedingthrough the wound,as shownby thesmaller numberofdressingsinthegroupinwhichdrainswereused. Furthermore,theuseofdrainsreducedlocallesions atthe surgicalsite.
Thenumberofbloodtransfusionsinthisstudywas simi-larinbothgroups(twoconcentratedunitsofredbloodcellsin each).Instudiesuntil2004,theauthorsreportedthatclosed suction drainage increased transfusion requirements after electivehipandkneearthroplasties,andgreaterbenefitswere notobserved.17
OnlySDswereusedinthejointcavity.Thedatainthestudy bySeoetal.2suggestthatsubcutaneousdrainageissimilar tothatusedforclosedsuctionintra-articulardrainage,with equivalentblood lossand withoutadverse effectson func-tionalresults;therefore,theuseofSDinthesubcutaneous isareasonableoptionagainstintra-articular.
Higherbleedingwasobservedinbothgroupswithinthe first 6h, witha highervalue inthe groupofpatients with the4.8-mmdrain,butwithoutastatisticallysignificant differ-ence(p=0.421).Goesetal.18comparedthelaboratoryresultsof openingthedrainatsixand12hafterTKR,anddidnotobserve statisticallysignificantdifferencesinlaboratoryvalues. How-ever,thevolumeofdrainedbloodwashigherwhenthedrain wasopenedafter6h.Thoseauthorsonlyused4.8-mmdrains. Royetal.19 conductedastudy withimmediatedrain open-ing1haftertheendofsurgery;theyobservedbloodlossand increasedneed forblood products inthe group wherethe drainwasopenedimmediately.Theseauthorsdidnot men-tionthethicknessofthedrain;theystatedthattwoaccess routeswereplacedinthejointspaceandwereremovedafter 48h.
It was observed that the bleeding after 24h becomes insignificant; in1991,Willemen etal.20 concluded thatthe clinicalevaluationsofsurgical woundhealingweresimilar forall groups(drainremoved after24 and48h)andclearly showed no advantagein continuinguse of the drain after 24h; ifdrainage ismaintainedforalongerperiod, thereis anincreasedriskofbacterialcontamination.85%ofthetotal
volumewasdrainedduringthefirst24h;inthefollowing24h, anaverageofonly50mLofbloodwasdrained,buttheauthors didnotmentionthegaugeofthedrains.DrinkwaterandNeil21 recommendthatdrainsinhiporkneereplacementsshould alsoberemovedafter24h.
Beeretal.,3intheirclassicalpublicationfrom1991,went further,demonstratingthatthereisnodifferenceregarding the incidence ofedemaor persistentdraining through the wound. Thereturntoactivequadriceps functionand knee rangeofmotioninpatientswhounderwentTKRwasalsonot affectedbytheuseofSDs.Theyconcludedthattheroutine useofdrainsinuncomplicatedsurgeryisunnecessary. Sim-ilarly, Zhang etal.,22 inameta-analysis publishedin2014, concludedthat, forprimarysurgerywithout major compli-cations,it ispreferabletonotuse SDs;the surgeonshould assess the benefits and drawbacks. In the present study, therewasonlyonecomplication(blisters)inthe4.8-mmSD group.
Andradeetal.,23inaBrazilianpublicationthatcompared the useornon-useof3.2-mmSDs, cametotheconclusion that, beyondsixmonthspost-operative,thereisnobenefit in the use ofclosed SD inTKR. However,range ofmotion atthe end ofthe first monthwasbetter inthegroup that usedSD.
Inthepresentstudy,bleedingwashigherwithinthefirst 6h after surgery for both groups, as the drains remained open. Yildizet al.24 took into accountthe clamping ofthe drain for 6h after TKR and observed that, in the group in which the tourniquet was released after the sutures and bandages were applied and the drain was closed for 6h, there was less blood loss. Souza Leão et al.25 did not take into account clamping of the SD in TKR, and com-paredbloodlosswithearlyorlatereleaseofthetourniquet; they found nostatistically significant differences in bleed-ing,buttherewasnomentionofthediameterofthedrains. Hemoglobinandhematocritlevelsalsoweresimilarforboth groups.
In a recent meta-analysis, Li at al.26 concluded that, throughthecurrentevidence,theuseornon-useofSDshas similarutilityandclinicalsignificanceinprimaryTKR. How-ever,duetosomelimitations(fewpatientsinvolvedineach studyandonlythreerandomizedcontrolledtrials),their find-ings should be interpreted with caution. Therefore, future studiesofhighmethodologicalqualityandlong-term follow-up are necessary to update the meta-analysis, in order to betterassesstheimportanceandeffectivenessoftheuseof drains.
day (Ht-post). The hematocrit should be written in deci-malunits.Thisformularequiresthepatient’sbloodvolume to be calculated by the formula postulated by Nadler at al.13 (in milliliters ofblood) and also requires the volume ofblood(redbloodcells)transfused.Theestimateobtained bytheMercurialiformulaisgiveninmillilitersofredblood cells.
Thelimitingfactorsofthepresentstudyincludethesmall follow-uptime(only duringadmission),inwhichno differ-enceswereobservedinjointfunctionandtherateofinfection; othercomplicationswerenottheobjectofthisstudy,which probablywouldshowfurtheradvantagesofonemethodover theother and could abound forfurtherresearch. Painwas alsonotquantified.Asamplewithalargernumberofpatients wouldprovidemorerobustnesstothestatisticalanalysis.As patientswereonthefirstthreedaysofintravenoushydration andbloodcountalsodependsonthehydrationstatus, per-hapsnumberswerehigherthanthenoted,provingthelow useofbloodproducts;however,atheoreticalframeworkthat takesintoaccountthehydrationofpatientswasnotretrieved. AgroupwithoutSD–control–wouldbeidealtocomparethe bloodcountandtheestimatedbloodloss,andhencejustify theuseornon-useofSD.
Conclusions
The present data allows for the conclusion that patients undergoingTKRhavehigherbleedingwhentheyhavea 4.8-mmSDinserted.Estimatedbloodlossissimilar,regardless ofthethicknessofthedrainsused.Bleedingishigherinthe first24haftersurgery,especiallyinthefirst6h;duringthelast 24h,bleedingisnegligible,andthereforetheuseofthedrain isunnecessary.Reductioninhematocritwassimilarforboth groupsandwasmorepronouncedonthefirstday,remaining stablethereafter.BleedingthroughSDinTKRisarealitythat cannotbeunderestimated;the surgeonshouldbeawareof possiblecomplicationsofthiseventandpromptlyresolveit. Rationaluseofthedrainandchoiceofitsgaugeare atthe surgeon’sdiscretion,bearinginmindthatthickerdrainscan causeincreasedbleeding.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1. LevyM.Intraperitonealdrainage.AmJSurg. 1984;147(3):309–14.
2. SeoES,YoonSW,KohIJ,ChangCB,KimTK.Subcutaneous versusintraarticularindwellingclosedsuctiondrainageafter TKA:arandomizedcontrolledtrial.ClinOrthopRelatRes. 2010;468(8):2168–76.
3. BeerKJ,LombardiAVJr,MalloryTH,VaughnBK.Theefficacy ofsuctiondrainsafterroutinetotaljointarthroplasty.JBone JointSurgAm.1991;73(4):584–7.
4.Al-ZahidS,DaviesAP.Closedsuctiondrains,reinfusion drainsornodrainsinprimarytotalkneereplacement?AnnR CollSurgEngl.2012;94(5):347–50.
5.K ˛eskaR,ParadowskiTP,Wito ´nskiD.Outcomeinprimary cementedtotalkneearthroplastywithorwithoutdrain:a prospectivecomparativestudy.IndianJOrthop.
2014;48(4):404–9.
6.GibonE,CourpiedJP,HamadoucheM.Totaljointreplacement andbloodloss:whatisthebestequation?IntOrthop. 2013;37(4):735–9.
7.KumarS,PenematsaS,ParekhS.Aredrainsrequired followingaroutineprimarytotaljointarthroplasty?Int Orthop.2007;31(5):593–6.
8.CamanhoGL,OliviR,CamanhoLF.Artroplastiatotaldejoelho empacientesidososportadoresdeosteoartrose.RevBras Ortop.1998;33:271–4.
9.AhlbäckS.Osteoarthrosisoftheknee.Aradiographic investigation.ActaRadiolDiagn(Stockh).1968;Suppl. 277:7–72.
10.KeyesGW,CarrAJ,MillerRK,GoodfellowJW.Theradiographic classificationofmedialgonarthrosis.Correlationwith operationmethodsin200knees.ActaOrthopScand. 1992;63(5):497–501.
11.ColunistaPortalEduc¸ão.Dreno;2015.Availablefrom: www.portaleducacao.com.br/enfermagem/artigos/36001/ drenos#ixzz3rHTA77pw[accessed12.11.15].
12.NadlerSB,HidalgoJH,BlochT.Predictionofbloodvolumein normalhumanadults.Surgery.1962;51(2):224–32.
13.MercurialiF,InghilleriG.Proposalofanalgorithmtohelpthe choiceofthebesttransfusionstrategy.CurrMedResOpin. 1996;13(8):465–78.
14.VieiraS.Bioestatística–Tópicosavanc¸ados.2nded.Riode Janeiro:Elservier;2004.
15.EPI-INFO.Versão7.4parawindows,produzidoedistribuído gratuitamentepeloCentrodeControledeDoenc¸as–CDC; 2015.Availablefrom:www.cdc.gov/epiinfo[accessed30.01.15]. 16.EslerCN,BlakewayC,FiddianNJ.Theuseofaclosed-suction
drainintotalkneearthroplasty.Aprospective,randomised study.JBoneJointSurgBr.2003;85(2):215–7.
17.ParkerMJ,RobertsCP,HayD.Closedsuctiondrainageforhip andkneearthroplasty.Ameta-analysis.JBoneJointSurgAm. 2004;86(6):1146–52.
18.GoesRFA,SilvaAF,LyraFS,LouresFB,PalmaIM,CobraHAA, etal.Estudoprospectivorandomizadoapósusodedrenona artroplastiatotaldojoelhocomimplante.RevBrasOrtop. 2013;48(3):257–62.
19.RoyN,SmithM,AnwarM,ElsworthC.Delayedreleaseof drainintotalkneereplacementreducesbloodloss.A prospectiverandomisedstudy.ActaOrthopBelg. 2006;72(1):34–8.
20.WillemenD,PaulJ,WhiteSH,CrookDW.Closesuction drainagefollowingkneearthroplasty.Effectivenessandrisks. ClinOrthopRelatRes.1991;264:232–4.
21.DrinkwaterCJ,NeilMJ.Optimaltimingofwounddrain removalfollowingtotaljointarthroplasty.JArthroplasty. 1995;10(2):185–9.
22.ZhangX,LiG,MaJ,MuheT,WangG,CaoL.Ameta-analysis fortheefficacyandsafetyofdrainageafterprimarytotal kneearthroplasty.ZhonghuaYiXueZaZhi.2014;94(29): 2282–5.
23.AndradeMAP,CamposTVO,SilvaBFA,AssisME,BoechatLC, BiondiLF,etal.Avaliac¸ãoprospectivadospacientes
submetidosàartroplastiatotaldojoelhocomesemcolocac¸ão dedrenodesucc¸ão.RevBrasOrtop.2010;45(6):549–53. 24.YildizC,KocaK,KocakN,TunayS,BasbozkurtM.Late
25.SouzaLeãoMG,SouzaHAP,FerreiraYMC.Avaliac¸ãodaperda sanguíneaapósaliberac¸ãoprecoceoutardiadaisquemiaem pacientessubmetidosàartroplastiatotaldojoelho.RevBras Ortop.2013;48(2):152–8.
26.LiN,LiuM,WangD,HeM,XiaL.Comparisonof
complicationsinone-stagebilateraltotalkneearthroplasty
withandwithoutdrainage.JOrthopSurgRes.2015; 10:3.
27.KurtzS,OngK,LauE,MowatF,HalpernM.Projectionsof primaryandrevisionhipandkneearthroplastyintheUnited Statesfrom2005to2030.JBoneJointSurgAm.