THE CURRENT STATUS OF THE CHEMOTHERAPY OF HYDATID DISEASE’ William S. Kammerer, M.D.,* and Miguela V. Perez-Esandi, Lit. Q~irn.~
Hydatid disease remains one of the few major parasitic diseases of man for which no adequate chemotherapy exists. However, the development of drug screening programs in laboratory animals provides a rapid, efficient, and economical means for testing potentially effective compounds.
Introduction
Since the chemotherapy of hydatid disease
was last reviewed (I, 2, 3) the further develop-
ment of laboratory animal models (4, 5, 6, 7, 8)
has made it possible to design large-scale drug
screening programs. Previously, testing of
potentially useful drugs was carried out in vitro
or via costly small-scale trials in humans and
domesticated animals.
The difficulties involved in carrying out
controlled clinical trials in humans severely
compromise this method as a screening tech-
nique. In
vitrotesting is theoretically useful for
identifying potentially effective drugs; however,
extrapolation of the results to the situation
in vivoremains uncertain, due mostly to insuf-
ficient basic information about the metabolism
and permeability characteristics of hydatid
cysts.
The purpose of this article is to point out
certain problems that arise in interpreting the
results of clinical trials in humans reported to
date, and to review the progress of drug
screening programs in laboratory animals.
Human Trials
Several attempts to sterilize or cure hydatid
‘Alsoappearing
in Spanish
in
Boletin de la Oficina Sanitaria Panamericana.aFormerly Parasrtologist,
Pan
American Zoonoses Center, Pan American Health Organization, Ramos Mejia, Buenos Aires, Argentina;presently Assistant
Professor
of Medicine,
Pennsylvania
State University
Medical School, Hershey Medical Center, Hershey, Pennsylvania.3Pan Amencan Zoonoses Center, Pan American Health Organization, Ramos Mejia, Buenos Aires, Argentina.
47
cysts through radiation therapy have met with
only limited success (I, 9). Furthermore, the
size of the cysts and the frequently large
numbers involved make it very doubtful that
radiation therapy will prove to be of any
substantial use.
The theoretical rationale behind “biologic
therapy” for hydatid disease and the results of
clinical trials using it have recently been com-
prehensively reviewed (IO, II). As has been
pointed out, no sound experimental or clinical
evidence has emerged to demonstrate the effi-
cacy of this mode of treatment.
Sporadic attempts to develop effective
chemotherapy for hydatid disease over the past
50 years (12, 13, 14, 15) have, with the
exceptions discussed below, encountered little
success.
In 1951, Cuervo Garcia (16) introduced
chemotherapy using iodinized oil of thymol for
treatment of hepatic and pulmonary hydatid
Adult Echinococcus granuiosus tapeworms like this one can infect dogs and various other Canidae. Their larvae can produce cases of hydatidosis involving large internal cysts and ‘a sometimes fatal course in
48 PAHO BULLETIN . Vol. VU, No. 3. I973
FIGURE 1 -The dog-sheep-dog life-cycle of Echi- nococcusgranulosus. E. muftilocularis, the other agent of hydatidosis, is commonly maintained by a fox-vole- fox cycle.
disease;
his reported “cure” of 12 patients was
ascribed to therapy with this compound. A
critical review of this work, however, makes it
difficult to connect the results observed with
the therapy prescribed. The study lacked simul-
taneously matched controls; patient selection
was biased toward those in whom a dramatic
host response
was probably occurring; diagnosis
was often presumptive; and patient follow-up
was uniformly short. Furthermore, as there is
little reliable information on the natural history
of hydatid disease in all of its forms and stages,
it is possible to conclude that the results
obtained by Cuervo Garcia merely represent
the natural course of the disease. The same
comments can be made about subsequent
clinical reports (17, 21) on the efficacy of
iodinized oil of thymol.
More recently, Panaitesco (22) has suggested
long-term therapy with paludrin for the preven-
tion and treatment of secondary hydatidosis.
Again, however, the absence of controls makes
it difficult to ascertain a cause-and-effect
rela-
tionship between the therapy employed and the
results observed. And, as in the previous case,
the lack of substantial objective criteria for
determining a cure makes it impossible to state
with certainty that Panaitesco’s
patients were in
fact cured.
For example, the frequency with which
secondary hydatidosis develops after spillage of
cyst contents during surgery is variable. Among
the patients who Panaitesco treated with palu-
drin and followed for 2 years or more, 18 per
cent remained infected. Schiller (23) however,
reported an incidence of only 30 per cent of
secondary hydatidosis in patients who received
no therapy after spillage of cyst contents during
surgery and who were followed for 5 years or
more. Statistically, these results do not differ
significantly (p > 0.40).
Trials in Laboratory Animals
Drug screening programs in laboratory
animals have been easier to design and inter-
pret, in that controls are easily included,
objective criteria exist for judging drug efficacy
at necropsy, and the natural history of infec-
tion in laboratory animal models has been
thoroughly studied (7, 8). To date, the results
of trials testing some 36 different compounds
have been reported.
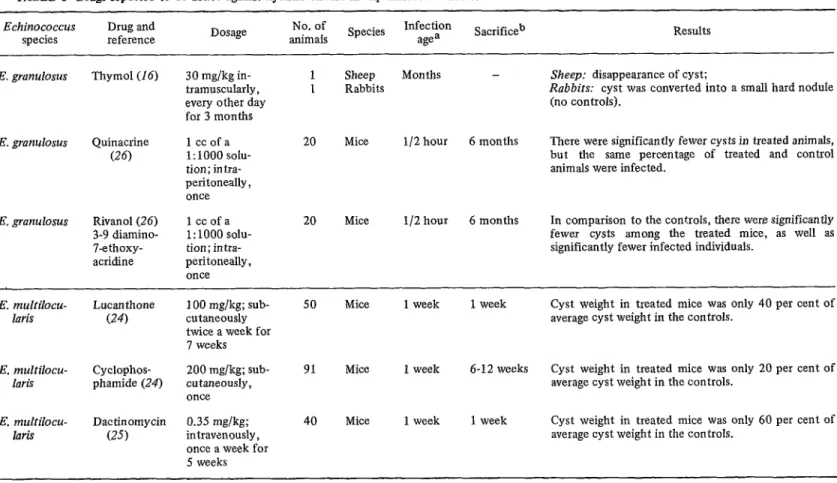
The results of those trials in which drug
effectiveness was reported are summarized in
Table 1. In addition, Lukashenko (27), in a
review of his work, reports that various acridine
derivatives
(e.g.,
2 methoxy-6-chloro-
9-aminoacridine and 2 methoxy-6-chloro-
9-methylaminoacridine) were effective, both
in vitroand
in vivo;but details of the therapy
provided and criteria for evaluating the effect
of these drugs
in vivoare not given.
TABLE l-Drugs reported to be active against hydatid disease in experimental animals.
Echinococcus Drug and
species reference Dosage
No. of Species Infection
animals agea Sacrificeb Results
E. granulosus Thymol(16) 30 mg/kg in- 1 Sheep tramuscularly, I Rabbits every other day
for 3 months
E. granulosus Quinacrine
(26)
1 ccofa 1: 1000 solu- tion; in tra- peritoneally , once
20 Mice
E. granulosus Rivanol(26) 3-9 diamino- 7ethoxy- acridine
lccofa 1: 1000 solu- tion; intra- peritoneally, once
20 Mice
Months - Sheep: disappearance of cyst;
Rabbits: cyst was converted into a small hard nodule (no controls).
l/2 hour 6 months There were significantly fewer cysts in treated animals, but the same percentage of treated and control animals were infected.
l/2 hour 6 months In comparison to the controls, there were significantly fewer cysts among the treated mice, as well as significantly fewer infected individuals.
E. multilocu- laris
Lucanthone (24)
E. multilocu- laris
E. multilocu- laris
Cyclophos- phamide (24)
Dactinomycin (25)
100 mg/kg; sub- cutaneously twice a week for 7 weeks
50 Mice 1 week 1 week
200 mg/kg; sub- cutaneously, once
91 Mice 1 week 6-12 weeks
0.35 mg/kg; intravenously, once a week for 5 weeks
40 Mice 1 week 1 week
Cyst weight in treated mice was only 40 per cent of average cyst weight in the controls.
Cyst weight in treated mice was only 20 per cent of average cyst weight in the controls.
Cyst weight in treated mice was only 60 per cent of average cyst weight in the controls.
aInfection age when therapy started.
50
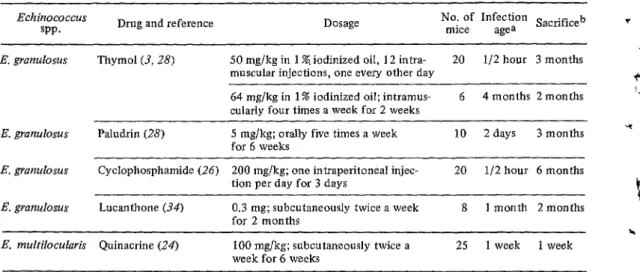
PAHO BULLETIN . Vol. VII, No. 3. I973TABLE 2-Negative results reported in mice, conflicting with results shown in Table 1. (Negative results indicate that there is no statistically significant difference in the number of infected animals or in the size or weight of cysts in treated animals with respect to the control groups.)
Echinococcus
VP. Drug and reference Dosage
No. of Infection Sacrificeb mice agea
E. grunulosus Thymol (3, 28) 50 mg/kg in 1 %, iodinized oil, 12 in&a- 20 l/2 hour 3 months muscular injections, one every other day
64 mg/kg in 1% iodinized oil; intramus- cularly four times a week for 2 weeks 6
4 months 2 months
4
v
E. granulosus Paludrin (28) 5 mg/kg; orally five times a week
for 6 weeks 10 2days 3 months
Y(
E. granulosus Cyclophosphamide (26) 200 mg/kg; one intraperitoneal injec- 20 l/2 hour 6 months tion per day for 3 days
E. granulosus Lucanthone (34) 0.3 mg; subcutaneously twice a week
for 2 months 8 1 month 2months
E. multilocularis Quinacrine (24) 100 mg/kg; subcutaneously twice a week for 6 weeks
25 1 week 1 week
aInfection age when therapy started.
bTime elapsed between end of therapy and sacrifice.
of varying ages before any experimental
therapy in humans is considered. Analogues of
active compounds could then be similarly
studied in an attempt to identify more potent
but less toxic substances.
Drugs reported to be without effect in
laboratory animal infections include: arseno-
benzol (29), kamala (3U), prednisolone (31),
thiabenzadole (32), neosalvarsan (33), chloro-
quin, sodium antimony mercaptosuccinate,
neguvon and tiguvon (24), trimethoprim, pyri-
methamine, metronidazole, diethylcarbamasine,
hycanthone, colchicine, Hoechst S-201 and
S-6 16 (experimental schistosomicides), hydro-
xyurea, vincristine and vinblastine (25), 6-
mercaptopurine (26), gentian violet, ampho-
tericin B, griseofulvin, emetine hydrochloride
(3), astiban and endoxan (34).
Conclusions
At the present time, surgery remains the
only remedy for patients with hydatid disease.
However, many patients are inoperable due to
the extensiveness of their disease, while others
are ineligible for surgery because of medical
contraindications. Furthermore, surgical re-
moval of hydatid cysts is a costly and time-
consuming procedure, and even in the most
experienced hands it is a hazardous under-
taking. At the same time, improved diagnostic
techniques, and increased awareness of the
disease as a result of epidemiologic surveys and
national control campaigns, are bringing more
and more patients to medical attention. Clearly,
if effective chemotherapy were developed it
would find immediate application.
SUMMARY
If an effective chemotherapeutic treatment application. Among other things, there is
for hydatid disease were discovered, there are currently no sure remedy for hydatidosis
good reasons to believe it would find immediate except surgery, diagnostic techniques have re-
i
r
4
.
4 A.
4 ‘(
Kammerer and Phez-Esandi . CHEMOTHERAPY OF HYDATID DlSEASE 51
cently improved, and there is increasing aware- recent work with laboratory animal models has ness of the disease as a result of epidemiologic made it possible to conduct large-scale drug surveys and national control campaigns. screening programs. This article reviews the Initial efforts to test the effects of drugs on results obtained from trials testing over 30 the disease were limited to small-scale trials in different compounds.
humans and domesticated animals. However,
REFERENCES
(I) Lippi, M. “La terapia medica della echinococcosi dell’uomo.” Arch Ital Sci Med Trop Parasit 38. 138-141, 1957.
(2) Lupascu, G., and D. Panaitesco. Hidatidoza. Editura Academici Republici Romania, Bucu- resti, 1968, pp. 213-222.
(3) Sorice, F., S. Pauluzzi, L. Castagnari, and P. Serra. “L’idatidosi sperimentale. II. Azione de1 timolo, de1 violetto di genziana, de1 chlori- drato di emetina, dell’ anfotericina B e deIla griseofulvina nei confronti dell’ infestazione endoperitoneale de1 topino con scolici di Echinococcus granulosus.” Clin Ter 31: 407-416, 1964.
(4) Lubinsky, G. “Growth of the Vegetatively Pro- pagated Strain of Larval Echinococcus multi- locularis in Some Strains of Jackson Mice and in Their Hybrids.” CunJZooZ42r 1099-1013, 1964.
(5) Schwabe, C. W., A. Kilejian, and G. Lainas. “The Propagation of Secondary Cysts of Echino- coccus granulosus in the Mongolian Jird, Meriones unguiculatus.” J Parasit 56: 80-83,
1970.
(6) Williams, J. F., and Cristina W. Colli. “Primary Cystic Infection with Echinococcus granulosus and Taenia hydatigena in Meriones unguicu- latus.“J Parasit 56: 509-5 13, 1970.
(7) Heath, D. D. “The Development of Echino- coccus granulosus Larvae in Laboratory Animals.” Parasitology 60: 449-456, 1970. (8) Colli, Cristina W., and P. M. Schantz. “Estudio y
desarrollo de modelos experimentales de infec- ci6n con huevos de Echinococcus granulosus en roedores de laboratorio.” Paper presented to the X International Conaess on Hvdati- dosis, Arequipa, Peru, 23-27 October 1972. (9) Dorrance, G. M., and .I. W. Bransfield. “The
Evaluation of the Surgical Treatment of Re- current Echinococcic Cysts of the Liver Fol- lowed by Deep X-Rav Therapv.” Am .I TrOD
MedHyg27: 7?,194?. --
(IO) Varela-Diaz, V. M. “Aspectos inmunolbgicos de1 tiatamiento biolbgico de la hidatidosis.” Paper presented to the x International Congress-on Hydatidosis, Arequipa. Peru, 23-27 October _ _
1972.
(II) Marchevsky, N. “Revisi6n de la literatura sobre tratamiento biol&ico de la hidatidosis.” Paper presented to the X International Congress on Hydatidosis, Arequipa, Peru, 23-27 October 1972.
(12) Fairley, N. H. “A Note on the Failure of Tartar Emetic in the Treatment of Two Cases of Hydatid Disease.” Med J Australia I: 94-96, 1922.
(13) Cawston, F. G. “Antimony in the Treatment of Lepers and Hydatid Disease.” J Trop Med Hyg 25: 27-28, 1922.
(14) D&B, F. “A propos du traitement de l’echino- coccose par l’emetioue.” Ann Parasitol 8:
566-568, i930. A
(151 KolbB. C. G. “S&ilisation intraveineuse du kvste hydatique par l’arsgno-benzol ou ses s&L laires.“MouvementMkd 2: 146-148, 1914. (16) Cuervo Garcia, C. “Ensayos de un tratamiento
medico de quiste hidatidico.” Rev Clin &sp 41: 320-328, 1951.
(17) Carol& J., M. Campeau, and A. Paraf. “Traite- ment m6dicale des kystes hydatiques par la methode de Cuervo.” Arch Ma1 ADD Dip 44: _. L
186-193, 1955.
(18) Thiodet, J. “Le traitement medicale de l’hyda- tidose.” Algkie MPd 58: 311-319, 1954. (19) Lahbabi, H. “La maladie hydatique.” Maroc Mkd
36: 446-448, 1957.
(20) Pirvu, D., U. Torjescu, and C. Georgescu. “Consi- deratti privind evolutia chistului hidatic tratat cu timol iodat injectabil.” Microbial Parazitol Epidemio13: 231, 1965.
(21) Hanstein, H. “Medikamentljse Behandlung des Echinococcus multilocularis. ” D tsch Med Wschr 82: 316-317, 1957.
(22) Panaitesco, D. “Contributions expkrimentales B 1’6tude du traitement de l’hydatidose se- condaire avec des antipaludiques de synth&e.” Arch Roum Path Exp Microbial 27: 39.5-406,
1968.
(23) Schiller, C. F. “Complications of Echinococcus Cyst Rupture: A Study of 30 Cases.” JAMA 195: 220-222,1966.
(24) Lubinsky, G. “Attempts at Chemotherapy of Echinococcus multilocularis Infections in Rodents.” Can J 2002 47: 1001-1004, 1969. (2.5) Lubinsky, G., C. F. Lee, and R. W. Baron. “Attempts at Chemotherapy of Echinococcus multilocularis Infections in Rodents: II. A Study of Some Parasiticides and Cytostatic Agents.” Can JZool49: 1301-1304, 1971. (26) Silobrcik, I. S. “A Study of the Medicamentous
52 PAHO BULLETIN . Vol. VII. No. 3. 1973 ’
the author’s summary supplied by Dr. Teodor Wikerhauser, Professor of Parasitology, De- partment of Parasitology and Paras& Dis- eases, Veterinary Faculty, University of Zagreb, Yugoslavia.
(27) Lukashenko, N. P., F. P. Kovalenko, and M. 0.
Kolosova. “0 vliianir nekotorvkh khimi- cheskikh soedinenii na zhiznesposobnost’i dykhanie lichinochnykh skoleksov Alveococcus multilocularis” (Effects of
Several Chemical Compounds on Viability and Respiration of Larval Scolices of Echino- coccus multilocularis). Acta Vet Acad Sci Hung 20: 339-352, 1970.
(28) Kammerer, W. S., and Miguela V. Perez-Esandi. .-
a&no-benzenes.” CR Sot Biol 87. 129-130, 1922.
(30) D&e, F. “Kyste hydatique et kamala.” CR Sot Bio193: 409-410, 1925.
(31) Magud, I. “On the Influence of the Origin of the Parasitic Material and on the Effect of a Corticosteroid Treatment of the Mouse upon the Development of Secondary Echino- coccosis in That Host.” Acta Parasit iugol 2:
79-86,1971.
,
’
I
(32) Beal, C. B., and E. K. Markell. “Experimental c Alveolar Hydatid Disease: Treatment Failure t with Thiabenzadole.” JAMA 198: 193, 1966.
(33) Dive. F.. and I. Pavenneville. “Greffe hvdatiaue et ~nedsalvarsan.” C R Sot Biol 76: 648-649, 1914.
“Quimioterapia experimental en animales de , (34) De Rosa, F., and S. Ciunta. “Primi dati sulla I laboratorio infectados con Echinococcus
granulosus.” Paper presented to the I National chemioterapia della idatidosi sperimentale de1
Congress of Parasitology, Buenos Aires, Argen- topo studrata con metodi quantitativi.” Paper P tina, 26 November-2 December 1972. presented at the VII National Conference of the Italian Society of Parasitology held at c (29) D&e, F., and 1. Payenneville. “Echinococcose et Bologna, Italy, in May 1972.
f
BUBONIC PLAGUE IN THE UNITED STATES OF AMERICA
Human and animal plague has been controlled in the United States to a point where it is now primarily a rural or wilderness area problem. Only rarely does it pose the sort of threat to large urban centers that it did in the early part of this century. Nevertheless, a record 13 cases of human bubonic plague associated with rural exposure were reported in the United States during 1970; two more were detected in 1971, another was found in 1972, and two more occurred in June and July 1973.
Plague activity has remained high among wild rodent populations in those states where human cases have often occurred, notably Arizona, California, Colorado, and New Mexico. During the first half of 1973 epizootic plague was reported among wild rodents from three widely separated California counties: Siskiyou, Tulare, and Riverside. An epizootic among wood rats at Siskiyou
County’s Lava Beds National Monument, detected in March, forced temporary
closure of visitor facilities until vector control measures could be implemented by state officials. In New Mexico, an epizootic among prairie dogs near Shiprock, San Juan County, necessitated vector control operations over a 5,000-acre tract in order to protect the resident Navajo population. This latter
situation was directly related to epizootics among prairie dogs of southwestern Colorado in 1971-1972.
Because it is sporadic and uncommon, human plague is easily overlooked or mistakenly diagnosed. Since it is readily treatable with appropriate antibiotics, recognizing the current status of wild animal plague and the consequent potential for human exposure should provide a basis for suspecting and appropriately handling sporadic cases. [Morbidity and Mortality, weekly report of the U.S. Center for Disease Control, Vol. 22, Nos. 25, 30, and 32, 1973.1
4