492
Ra n za n i, Ma rcelo Fern a n d o , et al.
Pn eu m o n ia lip o íd ica a sso cia d a à fo rm a d ig est iva d a d o en ça d e Ch a g a s
Dig e stive Chag as dise ase w ith co nco m itant lipo id
pneumonia*
MARCELO FERNANDO RANZANI, NILSON SEBASTIÃO MIRANDA, ULISSES FREDERIGUE JUNIOR, SÉRGIO MARRONE RIBEIRO, JUSSARA MARCONDES MACHADO
A 5 0 - ye a r- o ld w o m a n w it h ch a g a sic e so p h a g e a l a ch a la sia a n d m e g a co lo n p re se n t e d w it h n o n p ro d u ct ive co u g h , ch e st p a in a n d d ysp n e a . A ch e st X- ra y sh o we d b ila t e ra l o p a cit y su g g e st ive o f lo b a r p n e u m o n ia . Op e n lu n g b io p sy re ve a le d lip o id p n e u m o n ia re su lt in g fro m a sp ira t io n o f m in era l o il fro m a m in era l o il- b a sed la xa t ive t h a t t h e p a t ien t h a d b een t a kin g reg u la rly fo r t h e la st t h re e ye a rs. Th e a u t h o rs d iscu ss co n co m it a n ce o f ch a g a sic m e g a co lo n a n d e so p h a g e a l a ch a la sia wit h lip o id p n eu m o n ia a n d m a ke reco m m en d a t io n s reg a rd in g t h e u se o f m in era l o il- b a sed p ro d u ct s b y t h e se p a t ie n t s.
.Key words: Pneumonia, aspirtion/etiology. Pneumonia, lipid/etiology. Esophageal achalasia/pathology.
Chagas disease/complications.
*St u d y co n d u ct ed a t t h e Fa cu ld a d e d e Med icin a d e Bo t u ca t u (Bo t u ca t u Sch o o l o f Med icin e) – UNESP.
Co rresp o n d en ce t o : Dep a rt a m en t o d e Do en ça s Tro p ica is e Dia g n ó st ico p o r Im a g em . Ho sp it a l d a s Clín ica s - Fa cu ld a d e d e Med icin a d e Bo t u ca t u - UNESP. Dist rit o d e Ru b iã o J u n io r S/ No - CEP 1 8 61 8 - 9 7 0
Submitted: 17 August 2003. Accepted, after review: 20 November 2003.
INTRODUCTION
A 5 0 - y e a r - o l d w o m a n p r e s e n t e d w i t h n o n p ro d u ct ive co u g h , ch est p ain an d d ysp n ea. Th irt y years p rio r, t h e p at ien t h ad p resen t ed sig n s of in t est in al su bocclusion an d, aft er a laparot omy, was diagn osed wit h m egacolon . On t hat occasion , in d irect h em ag g lu t in at io n fo r Ch ag as d isease was p o sit ive. Th e p at ien t rem ain ed free o f sym p t o m s u n t il 1 5 years lat er, at wh ich t im e sh e b eg an t o exp erien ce ep iso d es o f co n st ip at io n t h at sp an n ed in creasin gly great er periods of t im e, oft en as lon g as 1 0 d ays. Sh e t h en st art ed u sin g laxat ives o n a d aily b asis an d g ivin g h erself weekly en em as.
CASE REPORT
493
Jornal Brasileiro de Pneumologia 3 0 (5 ) - Set/ Out de 2 0 0 4
Figu re 3 – Alveolar space filled wit h n u merou s macrophages co n t a in in g a g rea t q u a n t it y o f lip id va cu o les in t h eir cyt o p la sm
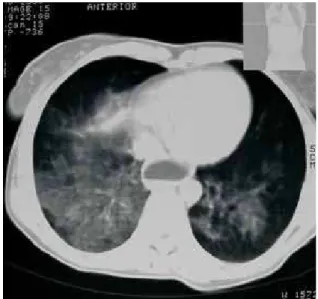
d ry co u g h , m a in ly in t h e m o rn in g . Sh e wa s a d m it t ed u n d er su sp icio n o f h ea rt d isea se. A ch e st X- ra y re ve a le d a lve o la r o p a cit ie s w it h p o o rly- d efin ed b o rd ers in t h e p o st erio r seg m en t o f t h e u p p er lo b e o f t h e rig h t lu n g a n d in t h e lo wer lo b e o f t h e left lu n g , a s well a s a sm a ll o p a cit y in t h e left lu n g b a se (Fig u re 1 ). On t h is o cca sio n , t h e p a t ie n t p re se n t e d n o sig n s o r sym p t o m s o f in fect io n o r co n su m p t io n , wh ich a r e c o m m o n in c a s e s o f t u b e r c u lo s is a n d p u lm o n a ry m yco sis. Th e p a t ien t wa s t h erefo re su b m it t ed t o a co m p u t ed t o m o g ra p h y sca n o f t h e ch est , wh ich revea led a g ro u n d - g la ss p a t t ern wit h poorly- defin ed borders, in volvin g bot h lower lo b es b u t m o re p ro n o u n ced in t h e rig h t lo b e. Eso p h a g ea l a ch a la sia , wit h a n a ir- flu id level, wa s a lso o b served (Fig u re 2 ). Th e p red o m in a n ce o f rig h t - sid ed lesio n s, t o g et h er wit h t h e eso p h a g ea l a c h a la s ia , s u g g e s t e d a s p ir a t io n . Sin c e t h e g ro u n d - g la ss p a t t ern revea led a n in fla m m a t o ry p ro cess o f lig h t in t en sit y, it wa s n o t co n sid ered co m p a t ib le wit h su p p u ra t ive p n eu m o n ia .
An o p e n - l u n g f r e e z e b i o p s y w a s r e c o m m e n d e d a n d p e r f o r m e d , a n d t h e h ist o p at h o lo g ical an alysis sh o wed p art it io n in g o f
t h e a lveo la r wa lls wit h lym p h a t ic ect a sia a n d p n eu m o cyt e h yp erp la sia .
Wit h in t h e alveo lar sp ace, g reat n u m b ers o f h ist io cyt es, wit h m icro vascu larizat io n wit h in t h e cyt o p lasm , were o b served .
Figure 1 – Anteroposterior chest X- ray showing alveolar opacity wit h poorly defin ed borders in t he post erior segmen t of t he lower right lobe an d a small opacit y in t he left lu n g base
494
Ra n za n i, Ma rcelo Fern a n d o , et al.
Pn eu m o n ia lip o íd ica a sso cia d a à fo rm a d ig est iva d a d o en ça d e Ch a g a s
DISCUSSION
Ch a g a s d ise a se is ca u se d b y a p ro t o z o a n
p arasit e kn o wn as Trypan osom a cru zi. Th e in it ial
in fect io n m ay p ass u n n o t iced o r m ay m an ifest as eit h er a m ild o r severe fo rm o f t h e d isease, t h e lat t er b ein g m o re co m m o n in en d em ic reg io n s. Un det ect ed in fect ion is t he more common scen ario. In su ch in d ivid u als, t h e d isease m ay evo lve slo wly an d gradu ally in t o on e of t he chron ic forms of t he disease, which t ypically presen t cardiac or digest ive a b n o rm a lit ies. Th e d ig est ive fo rm m a n ifest s a s dysphagia in t he presen ce of esophageal achalasia a n d , in t h e p resen ce o f m eg a co lo n , a s severe in t est in al con st ipat ion .(4 - 6 )
Th e b a s ic p a t h o g e n ic p h e n o m e n o m t h a t d et erm in es t h e d ig est ive fo rm o f t h e d isease is d en ervat io n wit h in t h e walls o f t h e au t o n o m ic n ervo u s syst em m yen t eric p lexu ses, esp ecially t h e
parasym pat het ic plexu ses.(7 )
In Bra z il, ch ro n ic ch a g a sic co lo p a t h y is a con dit ion t hat is frequ en t ly seen , especially in t he eld erly, an d resu lt s in p ro g ressively m o re severe in t est in al co n st ip at io n an d alt ern at in g p erio d s o f d iarrh ea. In t h e lat er st ag es, aft er m eg aco lo n h as been est ablished, pat ien t s may remain con st ipat ed for ext en ded periods, requ irin g t he aid of laxat ives an d h ig h co lo n ics.(4 )
Ch ag asic eso p h ag o p at h y is an o t h er co m m o n alt erat io n seen in cases o f t h e d ig est ive fo rm o f t h e d is e a s e . Th is c o n d it io n m a in ly a f f e c t s in d ivid u a ls o ld e r t h a n 3 0 a n d m a n if e st s a s dysp h ag ia, p rim arily wh en d ry, h ard o r co ld fo o d s are con su med. Su ch pat ien t s t en d t o in gest great er quantities of liquid at mealtimes in order to facilitate
d eg lu t it io n an d relieve t h e sym p t o m s.(4 )
Eso p h a g ea l d ysfu n ct io n p ro g resses t h ro u g h accu m u lat io n o f in g est ed m at erial in t h e su p erio r port ion of t he esophagu s, facilit at in g t he aspirat ion o f t h is m at erial. Th is co n d it io n is m o re co m m o n in in d ivid u als in wh o m t h e co u g h reflex h as b een lo s t o r s u p p r e s s e d d u e t o n e u r o m u s c u la r d ist u rb an ces, o r d u e t o t h e u se o f sed at ives o r o t h er d ru g s. In su ch cases, asp irat io n p n eu m o n ia
b eco m es est ab lish ed .(8 - 1 0 )
Min eral oil common ly in hibit s airway prot ect ive resp o n ses, su ch as g lo t t al clo su re an d co u g h , an d is also capable of ret ardin g m u cociliary clearan ce. Min e ra l o il a sp ira t io n m a y b e im p e rce p t ib le , creat in g a co n d it io n t h at is easily co n fu sed wit h p n eu m o n ia. Th e su b st an ce is relat ively in ert an d
is n o t m et ab o lized b y t issu e en zym es. It co n sist s of a mixt u re of lon g- chain sat u rat ed hydrocarbon s d erived fro m p et ro leu m . Wh en asp irat ed , m in eral o il em u lsifies an d ap p ears as d ro p s, o r vacu o les, o f f re e lip id s in t h e m a cro p h a g e cyt o p la sm . Th erefo re, a n a rea o f a lveo la r a n d in t erst it ia l accu mu lat ion of lipid- filled macrophages develops, su rro u n d ed b y lym p h o p lasm acyt ic in filt rat e. Over t im e, t h is area evo lves in t o fib ro sis, an d o il- filled g ian t cells en circle t h e sit e, fo rm in g a st ru ct u re kn o wn as a p araffin o m a. Th e ap p earan ce o f t h is t yp e o f lesio n in im ag in g exam s m ay lead t o a d ia g n o sis o f p u lm o n a ry n e o p la sm . Ho w e ve r, m in era l o il a sp ira t io n ca n p resen t a va riet y o f rad io lo g ical fin d in g s. Th o se m o st co m m o n ly seen in lip o id p n eu m o n ia are g ro u n d - g lass o p acit ies, i n t e r s t i t i a l a b n o r m a l i t i e s a n d p u l m o n a r y co n so lid at io n s, an y an d all o f wh ich m ay ap p ear in is o la t io n o r c o n c o m it a n t ly in t h e s a m e p at ien t .(2 ,3 ,11 ,1 2 )
In l i g h t o f t h e p o s s i b i l i t y t h a t t h e s e co m p licat io ns m ay o ccu r, it is reco m m en d ed t h at in dividu als at risk for bron choaspirat ion avoid t he u se o f m in era l o il. In a d d it io n , it is st ro n g ly su g g est ed t h at m in eral o il b e p rescrib ed fo r sh o rt p erio d s (less t h an o n e week) o n ly sin ce ch ro n ic u se in creases t he risk of aspirat ion . The au t hors of t h is rep o rt p ro p o se t h at , in Brazil, m in eral o il n o t b e p re sc rib e d f o r in d ivid u a ls w it h c h a g a sic m eg a co lo n sin ce t h ere is a risk t h a t , in su ch pat ien t s, it s u se will become chron ic. This warn in g ca rries a d d it io n a l weig h t in ca ses o f in t est in a l
Chagas disease in volvin g esophageal achalasia.(13,14)
REFERENCES
1 . Ba n d la HPR, Da vis SH, Ho p kin s NE. Lip o id p n eu m o n ia : a s i l e n t c o m p l i c a t i o n o f m i n e r a l o i l a s p i r a t i o n . Pe d ia t rics. 1 9 9 9 ; 1 0 3 : 1 9 .
2 . Co x J E, Ch o p lin RH, Ch iles C. Ca se rep o rt . Ch em ica l-sh ift MRI o f exo g en o u s lip o id p n eu m o n ia . J Co m p u t Assit To m o g r. 1 9 9 6 ; 2 0 : 4 6 5 - 7 .
3 . Sp ic k a r d A III, Hir s c h m a n n J V. Exo g e n o u s lip o id p n eu m o n ia . Arch In t ern Med . 1 9 9 4 ;1 5 4 :6 8 6 - 9 2 . 4 . Fe r r e i r a M S, Lo p e s ER, Ch a p a d e i r o E, Di a s J CP,
Ost e rm a ye r AL. Do e n ça d e Ch a g a s. In : Ve ro n e si R, Fo c c a c ia R, e d it o re s. Tra t a d o d e in f e c t o lo g ia . Sã o Pa u lo : At h e n e u ; 1 9 9 6 . p .11 7 5 - 2 1 3 .
5 . Ch a g a s C. N o v a e n t i d a d e m ó r b i d a n o h o m e m . Re su m o g e ra l d e e st u d o s e t io ló g ico s e clín ico s. Me m In st Osw a ld o Cru z . 1 911 ; 3 : 2 1 9 - 7 5 .
495
Jornal Brasileiro de Pneumologia 3 0 (5 ) - Set/ Out de 2 0 0 4
Tryp a n o so m a cru z i e d o e n ça d e Ch a g a s. 2 a e d . Rio d e J a n e iro : Gu a n a b a ra - ko o g a n ; 2 0 0 0 . p .2 9 7 - 3 4 3 7 . Lo p e s ER, Ch a p a d e ir o E. An a t o m ia p a t o ló g ic a d a
d o e n ça d e Ch a g a s h u m a n a . In : Dia s J CP, Co u ra J R. Clí n ic a e t e r a p ê u t ic a d a d o e n ç a d e Ch a g a s , u m a a b o rd a g em p rá t ica p a ra o clín ico g era l. Rio d e J a n eiro : Fio cru z; 1 9 9 7 . p .6 7 - 8 4 .
8 . Gim en ez A, Fra n q u et T, Erasm u s J J , Ma rt in ez S, Est ra d a P. Th o ra c ic c o m p lic a t io n s o f e so p h a g e a l d iso rd e rs. Ra d io g ra p h ics. 2 0 0 2 ; 2 2 : 2 4 7 - 5 8 .
9 . Ko b zik L. O p u lm ã o . In : Co t ra n RS, Ku m a r V, Co llin s T. Ro b in s, p a t o lo g ia est ru t u ra l e fu n cio n a l. 6 a ed . Rio d e J a n eiro : Gu a n a b a ra Ko o g a n ; 2 0 0 0 . p .6 2 6 - 7 9 .
1 0 . Berg BW, Sa en g er J S. Exo g en o u s lip o id p n eu m o n ia . N En g l J Med . 1 9 9 8 ;3 3 8 :51 2 .
11 . Lee J S, Im J G, So n g KS, Seo J B, Lim TH. Exo g en o u s lip o id p n e u m o n ia : h ig h - re so lu t io n CT f in d in g s. Eu r Ra d io l. 1 9 9 9 ; 9 : 2 8 7 - 91 .
1 2 . Gim én ez A, Fra n q u et T, Pra t s R, Est ra d a P, Villa lb a F, Ba g u é S. Un su a l p rim a ry lu n g t u m o rs: a ra d io lo g ic – p a t h o lo g ic o ve rvie w. Ra d io g ra p h ics. 2 0 0 2 ; 2 2 : 6 01 - 1 9 1 3 . Lan gdon DE, Bowen DL. A risk of min eral oil. N En gl J
Med . 1 9 9 8 ;3 3 9 :1 9 4 7 - 8 .