THE ROLE OF VIDEOLAPAROSCOPY IN THE DIAGNOSTIC AND
THERAPEUTIC APPROACH OF NONPALPABLE TESTIS
DANIEL G. BITTENCOURT, MÁRCIO L. MIRANDA, ANA P.P. MOREIRA,
SHOJI MIYABARA, J.M. BUSTORFF-SILVA
Section of Pediatric Surgery, School of Medicine, State University of Campinas, Unicamp, Campinas, São Paulo, Brazil
ABSTRACT
Objective: Evaluate the results from the first 5 years of experience with laparoscopy for diagnosis and treatment of nonpalpable testes.
Materials and Methods: Medical records of 51 patients submitted to laparoscopic testicular exploration, during a 5-year period, were retrospectively analyzed. Patients’ mean age was 65.7 months (median = 48) on the first procedure. The youngest patient was 10 months and the oldest was 14 years old on the first surgery. Twenty-four (47%) patients presented nonpalpable testes bilaterally, 7 (14%) only at the right side and 20 (39%) at the left, totaling 75 testicular units assessed. Patients who had their testes palpated after anesthetic induction were excluded from the study, and in all other cases, surgical management was based on the testicular position and viability. During the post-operative follow-up, surgical success was classified as palpable testis in scrotal sac, with adequate consistency and volume.
Results: Nine (12%) testes were not localized, but their vessels and deferent duct were atro-phic. Two (3%) testes were intra-abdominal and atrophic, and 2 (3%) gonads, in the same patient, had a dysmorphic aspect. Nineteen (25%) testicular units were located close to the internal inguinal ring (peeping testes) and, in 22 (29%) units, the spermatic vessels and deferent duct penetrated the internal inguinal ring. Eight (10%) testes were located at a distance of less than 2 cm from the internal inguinal ring and 13 (17%) at a distance greater than 2 cm. The 2 intra-abdominal atrophic testes were re-moved. Inguinotomy was performed in a total of 41 (54%) cases, reaching a surgical success of 89%. Laparoscopic orchiopexy in one stage, without vascular ligation, was performed in 9 (12%) testes, which presented a distance of less than 2 cm from the internal inguinal ring, also with a surgical success index of 89%. Orchiopexy in 2 stages, with ligation of the spermatic vessels, was performed in 13 (17%) testicular units located at a distance greater than 2 cm from the internal inguinal ring, reaching 77% of good results.
Conclusion: Videolaparoscopy is a safe and effective method for diagnosis and treatment of nonpalpable testis.
Key words: testis; cryporchidism; diagnosis; therapeutics; laparoscopy Int Braz J Urol. 2003; 29: 345-52
INTRODUCTION
Cryptorchidism occurs in 0.8 to 1.2% of boys at 1 year old (1,2), and in 20% of them, the testis is nonpalpable (3), and it can be absent, intra-canalicu-lar, or intra-abdominal.
tomog-Table 1 – Laterality and associated pathologies.
Nonpalpable Testis Frequency Associated Pathologies
Bilateral Right Left Total
DR = neuro-psychomotor development retardation; MPH = male pseudo-hermaphroditism; PB = prune-belly syndrome; MGD = mixed gonadal dysgenesis; HP = hypospadias; DS = Down’s syndrome; KT = Klippel-Trenounay syndrome.
raphy, scintigraphy and magnetic resonance, do not offer a similar accuracy (4-7). In 1992, Jordan et al. (8) introduced the therapeutic application of laparoscopy in patients with nonpalpable testes and, since then, in addition to being a diagnostic method, it has been an option for treating this condition.
This work’s objectives were: 1) To analyze the experience of the first 5 years following the in-troduction of videosurgery for diagnosis and treat-ment of nonpalpable testes in our service; 2) To ac-cess the surgical sucac-cess of different orchiopexy tech-niques; 3) To assess the need of exploring the inguinal canal in cases where laparoscopy identifies spermatic vessels and deferent duct penetrating the internal in-guinal ring.
MATERIALS AND METHODS
In the period from March 1996 to April 2001, 51 patients underwent diagnostic and therapeutic laparoscopy in our service. Patients’ mean age was 65.7 months (median = 48) on the first procedure and 64.58 months (median = 50) on the second surgery. The youngest patient was 10 months and the oldest was 14 years old on the first surgery.
Twenty-four (47%) patients presented nonpalpable testes bilaterally, 7 (14%) only at the right side and 20 (39%) at left, totaling 75 testicular units assessed (Table-1).
Twenty-two (43%) patients presented co-morbidities (Table-1). Thirty-nine (76%) patients were White and the others were Mulatto or Black, and there was none patient of Asian origin. Twenty-five (48%) patients underwent pelvic and inguinal
ultrasonography, and in only 10 (40%) the result co-incided with the surgical finding. Stimulation with β-HCG was performed in 5 (9,6%) patients with bi-lateral nonpalpable testes, without change of testicu-lar position at the post-treatment assessment.
All patients were submitted to inhalatory and intravenous general anesthesia, followed by testicu-lar palpation. Those patients who had their testes pal-pated at this moment were excluded from the study and were submitted to inguinotomy. The surgical tech-nique that was employed included gastric stenting, vesical drainage and Trendelenburg’s position; infraumbilical incision and the confection of a pneumoperitoneum with Veress needle, insufflating carbon dioxide at pressures of 8 to 10 mmHg. Then a 10 mm trocar was introduced through the incision, enabling the investigation of the peritoneal cavity with an optic (30°) of 10 mm. First, potential injuries to hollow viscera and other organs were assessed; next, the following was evaluated: region of internal in-guinal ring, spermatic vessels and deferent duct, tes-ticular size and position, in addition to comparison with the contralateral unit.
In cases of absent testicular structure, with spermatic vessels and deferent in blind sac, the laparoscopic procedure was terminated. When the testis was next to the internal inguinal ring(peeping testes), the inguinotomy was preferred, because, in our experience, such testicular position allows for the classic orchiopexy with good results. If elements of the spermatic cord penetrating the internal inguinal ring were identified, the exploration was proceeded by inguinal route and, when a viable testis was iden-tified, orchiopexy was performed.
18 (75%) : 6 DR; 5 MPH; 4 PB; 2 MGD; 1 HP 2 (29%) : 1 DR; 1 HP
2 (10%) : 1 DS; 1 KT 22 (43%)
In all other situations, 2 auxiliary trocars, one of 10 mm and other of 5 mm, were located in both hemiclavicular lines at the level of the umbilicus scar, under direct visualization. Patients with bilateral cryp-torchidism were treated in a single time.
When the testis was located at less than 2 centimeters from the internal inguinal ring, the laparoscopic orchiopexy in one stage was performed, which consisted in the distal section of the guber-naculum, if present; dissection of the peritoneum lat-erally to the spermatic vessels, mobilizing the ves-sels and the deferent for an extension of 8 to 10 cm of their retroperitoneal position. The vessels were pre-served by blunt dissection, avoiding electrocoagula-tion. Upon completing the dissection, the testis was free of adhesions to the posterior abdominal wall, with the spermatic vessels and the deferent duct. At this moment, a laparoscopic clamp (Grasping or Mary-land) was introduced, from a new internal inguinal ring created medially to the obliterated ipsilateral umbilical artery, up to the scrotal sac. A small inci-sion and a sub-dartos pouch were created in the scro-tum, through which a 5 mm trocar, followed by a Grasping clamp, were introduced into the peritoneal cavity. The testis was then driven to his position within the sub-dartos pouch in the scrotum, pulled by the gubernaculum, aiming not to injury its vascular sup-ply. The desufflation of the pneumoperitoneum pro-vided an additional extension to the testicular posi-tion.
In cases of testes that were more than 2 cen-timeters away from the internal inguinal ring, the laparoscopic orchiopexy in 2 times was performed, which consisted initially in ligation of the spermatic vessels with metallic clips and their section. The laparoscopic orchiopexy was performed in a second time, usually with a 6-month interval from the first surgery. Closure of the internal inguinal ring was not performed in any case of laparoscopic orchiopexy.
RESULTS
Laparoscopic Findings
Videolaparoscopy defined the intraabdominal anatomy in all cases. Nine (12%) testes were not lo-calized, however their vessels and vas deferens were
atrophic. Two (3%) testes were intraabdominal and atrophic and 2 (3%) gonads, in the same patient, had a dysmorphic aspect. Nineteen (25%) testicular units were located next to the internal inguinal ring (peep-ing testes) and, in 22 (29%) cases, the spermatic ves-sels and the deferent duct penetrated the internal in-guinal ring. Eight (10%) testes were located at a dis-tance of less than 2 cm from the internal inguinal ring, and 13 (17%) at a distance greater than 2 cm.
Surgical Management
The 2 intraabdominal atrophic testes were removed, by laparoscopic approach in one case, and by inguinal approach on the second one.
The 2 gonads with dysmorphic aspect were biopsied by laparoscopy. The histological analysis showed viable testicular tissue in one of them, with laparoscopic orchiopexy without vascular ligation being performed.
Inguinotomy was performed in a total of 41 (54%) cases: in 19 testicular units located next to the internal inguinal ring and in those 22 where the sper-matic vessels and the vas deferens penetrated the in-ternal inguinal ring. Among those, 13 units presented anorchia or testicular atrophy on inguinotomy, with the excision of testicular remnants being performed. In the remainder 28 units, open orchiopexy was com-pleted.
Laparoscopic orchiopexy without vascular ligation, in one stage, was performed in 9 (12%) tes-tes: 8 that presented a distance of less than 2 cm from the internal inguinal ring, in addition to the unit with dysmorphic aspect that had been submitted to biopsy. Orchiopexy with ligation of spermatic ves-sels in 2 stages was performed in 13 (17%) testicular units located at a distance superior to 2 cm from the internal inguinal ring. The interval between the first and the second procedure was 6 months.
Surgical Result
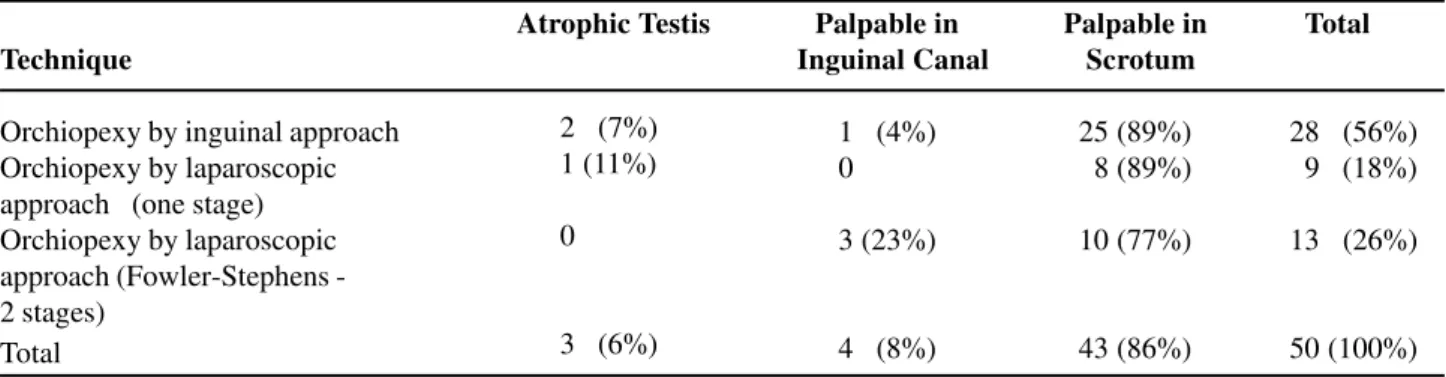
Table 2 – Surgical result according to the technique employed, excluding testes initially atrophic or absent.
Atrophic Testis Palpable in Palpable in Total Technique Inguinal Canal Scrotum
Orchiopexy by inguinal approach Orchiopexy by laparoscopic approach (one stage) Orchiopexy by laparoscopic approach (FowlerStephens -2 stages)
Total
1 (4%) 0 3 (23%)
4 (8%) 2 (7%)
1 (11%) 0
3 (6%)
25 (89%) 8 (89%) 10 (77%)
43 (86%)
28 (56%) 9 (18%) 13 (26%)
50 (100%)
Of the 28 testicular units that were driven to the scrotum by open orchiopexy, 25 (89%) were pal-pable in the scrotum with adequate consistency and volume; one (4%) in low inguinal canal and 2 (7%) evolved with atrophy.
Of the 22 testes driven to the scrotum by videolaparoscopy, 9 were driven to the scrotum with-out vascular ligation, in one stage, with 89% of suc-cess and only one (11%) testicular atrophy. 13 were operated by Fowler-Stephens technique with ligation of vessels, in 2 stages, reaching 77% of good results, with 3 (23%) palpable testes in the inguinal canal. Relative to the non-closing of the internal inguinal ring in cases of laparoscopic orchiopexy, no inguinal herniation was identified in the follow-up.
Pathological Study
It was performed in 17 testes: in the 2 intra-abdominal atrophic testes, it revealed cells in the pre-pubertal developmental stage; in the 2 dysmorphic gonads that were submitted to biopsy, it demonstrated a dysgenic gonad and a rudimentary testis. However, in the 13 units where the spermatic vessels and the vas deferens penetrated the internal inguinal ring, during the inguinal exploration, testicular atrophy or anorchia were identified, demonstrating lack of tes-ticular tissue in 11 cases, scaring tissue in 1 and cells in the prepubertal developmental stage in another.
Second Surgery
Inguinotomy and orchiopexy were performed due to testicular atrophy, detected in the post-opera-tive follow-up, in 3 units: 2 of them were initially located in the internal inguinal ring, and had
under-went orchiopexy by inguinal approach on the first surgery, whereas the third unit had been driven to the scrotum by laparoscopy in one step.
DISCUSSION
The main reasons for investigating nonpalpable testes and their position in the scrotum when present, are to preserve fertility, to make the testicular examination easier anticipating the diagno-sis of an eventual malignant transformation, in addi-tion to esthetic and psychological factors.
The traditional method for investigating a nonpalpable testis consists in an exploration by inguinotomy, or by lower abdominal approach. Videosurgery was used for this purpose, for the first time, in 1976, by Cortesi et al. (9) and, since then, it has been improved and used, as well, for therapeutic purposes.
per-formed in 2 stages, allowing the development of col-lateral circulation (15).
The mean age of patients in our sample was high (mean = 65.7 and median = 48 months), reflect-ing a probable delay in the diagnosis or in the referral of boys with nonpalpable testes to the tertiary care service. Once the follow-up in our service was initi-ated, there was no investment in imaging studies or hormone therapy, due to their limited results accord-ing to the literature. In this series, 48% of patients underwent ultrasonographic investigation, mostly before referral, and in only 40% of the cases, the find-ings coincided with the surgical anatomy.
Analyzing the results on a laterality basis, we observed that among the 24 patients (48 testicu-lar units) who presented nonpalpable testes bilater-ally, 18 (75%) presented associated pathologies, 10 (21%) absent or atrophic testicular units and 13 (27%) units in “high” position (> 2 cm from the in-ternal inguinal ring). Among the 7 patients who pre-sented nonpalpable testes only at the right side, 2 (28%) presented associated pathologies, only 1 (14%) missing unit and none unit in high position. We observed 20 nonpalpable units only at the left side, with 2 (10%) presenting associated patholo-gies, 14 (70%) absence or atrophy and none high unit. The highest incidence of associated patholo-gies in patients with nonpalpable testes bilaterally is probably because patients bearing neuropathies, male pseudo-hermaphroditism, prune-belly syn-drome and mixed gonadal dysgenesis, often evolve with cryptorchidism. The analysis based on lateral-ity also suggests that the “high” position of intra-abdominal testes is more frequent in bilateral de-fects and that anorchia or testicular atrophy are more commonly observed in cases where the defect oc-curs only at the left side.
One of the purposes of this study was to as-sess the surgical result of the 3 different techniques that are used in our service. Orchiopexy by inguinal approach and laparoscopic orchiopexy without liga-tion of vessels presented a surgical success (adequate testicular volume and position) of 89%, whereas laparoscopic orchiopexy in 2 stages (Fowler-Stephens), obtained 77% of good results; values that are consonant to the literature (13-16).
Inguinal exploration, in cases where laparoscopy had identified spermatic vessels and def-erent duct penetrating the internal inguinal ring, proved to be necessary, because in 9 cases (41%) vi-able testes were found and driven successfully to the scrotum. In this sample, such exploration was per-formed by inguinal approach in all cases, due to the team’s larger experience with this approach. How-ever, by retrospectively assessing and based on data from the literature (17-19), we do not see a reason why such exploration is not made by laparoscopic approach, since it has showed to be safe and effec-tive. Such management could avoid the use of 2 ap-proaches (laparoscopy and inguinotomy) for obtain-ing the same objective.
Schleef et al. (19) suggest the inguinal laparoscopic exploration in cases where one can ob-serve hypoplastic elements of the spermatic cord pen-etrating the internal inguinal ring. Such study, based also in findings from other works (20-22), suggests the hypothesis that in cases where hypoplastic ele-ments of the spermatic cord penetrate a closed inter-nal inguiinter-nal ring, there is never a normal testis in the inguinal canal. In our sample, it was possible to iden-tify 2 cases on the definition above, and in none of them a viable testis was found in the inguinal canal. Our sample of inguinal laparoscopic exploration is still small, with a larger number of studies being re-quired to confirm such hypothesis.
Evaluating the literature data about false-negative inguinal explorations (26), in addition to the risk of in-situ carcinoma in cryptorchid testes (27-28), we should engage in the definitive laparoscopic diagnosis. It is worth to remember that some laparoscopic procedures were canceled, with an inguinotomy performed, due to palpation of the tes-tis after anesthetic induction. This results from the fact that the muscle relaxation and the immobiliza-tion of the child contribute to testicular palpaimmobiliza-tion. Despite of this, in 9 cases, testes located in the in-guinal canal were not palpated. Laparoscopy allowed their correct localization and their treatment by in-guinal approach.
CONCLUSION
Laparoscopy showed to be a safe and effec-tive method for assessment and treatment of nonpalpable testes. It enabled that intraabdominal anatomy was accurately defined in all cases, provid-ing higher safety in dissection of delicate structures, under direct visualization. If also offered a fast re-covery to the patient, with excellent esthetic results. Non-closure of the internal inguinal ring did not re-sult in inguinal hernia.
REFERENCES
1. Scorer CG: The descent of the testis. Arch Dis Child. 1964; 39: 605-9.
2. Berkowitz GS, Lapinski RH, Dolgin SE: Prevalence and natural history of cryporchidism. Pediatrics 1993; 92: 44-7.
3. Elder JS: The undescended testis: hormonal and sur-gical management. Surg Clin North Am. 1988; 68:
983-1005.
4. Bloom DA: Two-step orchiopexy with pelviscopic clip ligation of the spermatic vessels. J Urol. 1991; 145: 1030-4.
5. Bogaert GA, Kogan BA, Mevorach RA: Therapeutic laparoscopy for intraabdominal testes. Urology 1993;
42: 182-4.
6. Caldamone AA, Amaral JF: Laparoscopic two-stage Fowler-Stephens orquiopexy. J Urol. 1994; 152: 1253-5.
7. Elder JS: Two-stage Fowler-Stephens orquiopexy in
the management of intraabdominal testes. J Urol. 1992; 148: 1239-42.
8. Jordan GH, Robey EL, Winslow BH: Laparoscopic surgical management of the abdominal/transinguinal undescended testicle. J Endourol. 1992; 6: 159. 9. Cortesi N, Ferrari P, Zambarda E, Manenti A, Baldini
A, Pignatti-Morano F: Diagnosis of bilateral abdominal cryporchidism by laparoscopy. Endoscopy 1976; 8: 33-4.
10. Steinhardt GF, Kroovand RL, Perlmutter AD: Orchio-pexy: planned 2-stage technique. J Urol. 1985; 133: 434-5.
11. Harrison CB, Kaplan GW, Scherz HC, Packer MG, Jones J: Microvascular autotransplantation of the in-tra-abdominal testis. J Urol. 1990; 144: 506-7. 12. Boddy SA, Gordon AC, Thomas DFM, Browning
FSC: Experience with the Fowler-Stephens and mi-crovascular procedures in the management of intra-abdominal testes. Br J Urol. 1991; 68: 199-202. 13. Snyder HM III, Duckett JW: Orchidopexy with
divi-sion of spermatic vessels: review of ten years experi-ence. J Urol. 1984; 131: 126A.
14. Clatworthy HW Jr, Hollabaugh RS, Frosfeld JL: The “long-loop vas” orchidopexy for the high undescended testis. Am Surg. 1972; 38: 69-73.
15. Ransley PG, Vordermark JS, Caldamone AA, Bellinger M: Preliminary ligation of the gonadal vessels prior to orchidopexy for the intra-abdominal testicle: a stage Fowler-Stephens procedure. World J Urol. 1984; 2:
266-8.
16. Dénes FT, Silva FAQ, Girón AM, Arap S: Laparoscopic evaluation and treatment of the impal-pable testis. Braz J Urol. 2001; 27: 380-5.
17. Humphrey GM, Najmaldin AS, Thomas DF: Laparoscopy in the management of the impalpable undescendent testis. Br J Surg. 1998; 85: 983-5. 18. Lindgren W, Franco I, Blick S, Levitt SB, Brock WA,
Palmer LS, et al.: Laparoscopic Fowler-Stephens or-chidopexy for the high abdominal testis. J Urol. 1999; 162: 990-4.
19. Schleef J, von Bismarck S, Burmucic K, Gutmann A, Mayr J: Groin exploration for nonpalpable testes: laparoscopic approach. J Pediatr Surg. 2002; 37: 1552-5.
20. Baillie CT, Fearns G, Kitteringham L, Turnock RR: Management of the impalpable testis: the role of laparoscopy. Arch Dis Child. 1998; 79: 419-22. 21. Grandy RW, Mitchell ME, Carr MC: Laparoscopic and
22. Topuzlu Tekant G, Emir H, Eroglu E, Akman M, Buyukunal C, Danismend N, et al.: Experience with laparoscopy in nonpalpable testis. Eur J Pediatr Surg. 2001; 11: 177-81.
23. Moore RG, Peters CA, Bauer SB, Mandell J, Retik AB: Laparoscopic evaluation of the nonpalpable tes-tis: a prospective assessment of accuracy. J Urol. 1994; 151: 728-31.
24. Duckett JW: Pediatric laparoscopy: prudence, please. J Urol. 1994; 151: 742-3.
25. Molenaar JC, Hazebroek FW: Diagnostic laparoscopy
should not be routinely done in nonpalpable testes. Neder Tijdschr Geneesk. 1993; 137: 582-3.
26. Lakoo K, Thomas DFM, Najmaldin AS: Is inguinal exploration for the impalpable testis an outdated op-eration? Br J Urol. 1996; 77: 452-4.
27. Sexton WJ, Assimos DG: Laparoscopy for the adult cryptorchidic testicle. Tech Urol. 1999; 5: 24-8. 28. Rogers E, Teahan S, Gallagher H, Butler MR, Grainger
R, McDermott TE, et al.: The role of orchiectomy in the management of postpuberal cryptorchidism. J Urol. 1998; 159: 851-4.
EDITORIAL COMMENT
Laparoscopy is already a recognized method for assessment and treatment of nonpalpable testes, and the experience presented by the authors confirms such data.
The therapeutic sequence for the several laparoscopic findings is well defined in this work, giving importance to the reference of distance from the testis to the internal inguinal ring. Therefore, if the distance is less than 2 cm, the orchiopexy can be performed immediately, since the dissection allows to obtain a sufficient length of the spermatic vessels to comfortably fix the testis to the scrotum (most of the times, that occurs when it can be taken to the in-ternal orifice of the contralateral inguinal canal). On the other hand, when the initial distance is greater than 2 cm, probably a sufficient length will not be obtained, even with exhaustive dissection, thus it is more prudent to make the vascular ligation only, and to perform the orchiopexy in a new procedure after 6 months.
Contrarily to the authors, I consider that the identification of the testis next to the internal inguinal ring is a formal indication for laparoscopic orchio-pexy, inclusively when it is located within the her-nial sac (“peeping testis”). However, it is fundamen-tal that the deferent, which can insinuate further be-yond the testis, through the internal orifice of the in-guinal canal, forming a loop in the hernial sac wall, is carefully dissected, avoiding its injury. For that, it is necessary to pull the hernial sac into the abdomi-nal cavity, in order to make its visualization easier. Due to the low testicular position, the length of sper-matic vessels and deferent rarely constitutes a limit-ing factor to the success of primary laparoscopic or-chiopexy.
In the discussion, the authors suggest the possibility of laparoscopic dissection of the inguinal canal to treat canalicular testes, when vessels and deferent are identified penetrating the obliterated in-ternal inguinal orifice. In my opinion, this is a
haz-Received: March 5, 2003 Accepted after revision: July 29, 2003
Correspondence address:
Dr. Daniel Bittencourt
Rua Odila Maia Rocha Brito, 205 Campinas, SP, 13092-010, Brazil Fax: + 55 19 3253-7066
ardous proposal, since in some cases the testis is viable, but is located below the external orifice of the inguinal canal, that is, in the inguinal subcuta-neous tissue, consequently in a site of difficult ac-cess by laparoscopic approach. Moreover, there is a significant risk of trauma to the testis, deferent and spermatic vessels with this laborious dissection, making the orchiopexy unfeasible. Such strategy would be warranted only if all canalicular testes should be removed, due to being atrophic, what is
not confirmed by the authors’ own sample. Addi-tionally, in case of atrophic or vestigial canalicular testes, the inguinotomy allows that, following the orchiectomy, testicular prostheses are inserted at the same time.