Cop
yright
© ABE&M t
odos os dir
eit
os r
eser
vados
.
Rare renal metastases from
differentiated thyroid carcinoma:
early clinical detection and
treatment based on radioiodine
Metástases renais raras de carcinoma diferenciado da tireoide: detecção clínica precoce e tratamento com radioiodoterapiaZhong-Ling Qiu1, Yan-Li Xue1, Quan-Yong Luo1
ABSTRACT
Objective: The aim of this study was to explore the clinical characteristics of renal metastatic cancer, the methods for its detection by radioiodine (131I), and the response to 131I treatment in fourteen pa-tients with renal metastases from differentiated thyroid carcinoma (DTC). Subjects and methods: DTC patients (n = 2,955) that received treatment with 131I were retrospectively analyzed. Scans (131 I-WBS, 31I-SPECT/CT and/or 18F-FDG-PET/CT) were performed after an oral therapeutic dose of 131I. Therapeutic eficacy was evaluated based on changes in Tg and anatomical imaging changes at renal lesions. Results: Among these 14 patients, 11 had avidity for 131I, but three patients did not accumu-late 131I after 131I treatment. In the 11 131I-positive renal lesions, 10 cases were detected by 131I-SPECT/CT combined with another imaging modality and one case by 131I-WBS combined with ultrasonography (US). In the three 131I-negative renal lesions, two cases were detected by 18F-FDG-PET/CT and one case by computed tomography (CT). In 11 patients with 131I-avid renal metastases, Serum Tg levels in 81.82% (9/11) patients showed a gradual decline, and 18.18% (2/11) of the patients showed a signii-cant elevation. There was no marked difference in serum Tg before the last 131I treatment (Z = 0.157; p = 0.875). Only one patient presented partial response, eight patients exhibited stable disease, and re-nal metastases progressed in two patients showing progressive disease. No patients reached com-plete response. Conclusion: 131I-SPECT/CT, combined with another imaging modality after 131I-WBS, can contribute to the early detection of renal metastases of DTC. 131I therapy is a feasible and effective treatment for most DTC renal metastases with avidity for 131I.Arq Bras Endocrinol Metab. 2014;58(3):260-9
Keywords
Differentiated thyroid cancer; renal metastases; radioiodine therapy; 131I-SPECT/CT; 18F-FDG-PET/CT
RESUMO
Objetivo: O objetivo deste estudo foi analisar as características clínicas de metástases renais, os métodos para sua detecção por radioiodo (131I) e a resposta ao tratamento com 131I em 14 pacientes com metástases renais de carcinoma diferenciado da tireoide (DTC). Sujeitos e métodos: Pacien-tes com DTC (n = 2.955) que receberam tratamento com 131I foram analisados retrospectivamente. 131I-PCI, 31I-SPECT/CT e/ou 18F-FDG-PET/CT foram feitos após uma dose terapêutica oral de 131I. A eicácia terapêutica foi baseada nas alterações da Tg e nas imagens anatômicas das lesões renais. Resultados: Dos 14 pacientes, 11 apresentaram lesões ávidas por 131I, mas três pacientes não acu-mularam 131I depois do tratamento com 131I. Nas 11 lesões renais positivas para 131I, 10 casos foram detectados por 131I-SPECT/CT combinado com outra modalidade de exame de imagem e um caso por 131I-WBS combinado com US. Nas três lesões renais negativas para 131I, dois casos foram detectados por 18F-FDG-PET/CT e um caso por tomograia computadorizada (TC). Em 11 pacientes com metástases renais ávidas por 131I, os níveis séricos de Tg em 81,82% (9/11) dos pacientes mos-traram um declínio gradual e 18,18% (2/11) apresentaram uma elevação signiicativa. Não houve diferenças marcadas na Tg sérica antes do último tratamento com 131I (Z = 0,157; p = 0,875). Apenas um paciente apresentou resposta parcial, oito pacientes apresentaram doença estável e as me-tástases renais progrediram em dois pacientes que apresentaram doença progressiva. Nenhum dos pacientes apresentou resposta completa. Conclusão: 131I-SPECT/CT, combinada com outra modalidade de diagnóstico por imagem após 131I-PCI, pode contribuir para a detecção precoce de metástases renais de DTC. O tratamento com 131I é passível de ser feito e eiciente para o tra-tamento da maior parte das metástases renais ávidas por 131I. Arq Bras Endocrinol Metab. 2014;58(3):260-9
Descritores
Carcinoma diferenciado de tireoide; metástases renais; radioiodoterapia; 131I-SPECT/CT; 18F-FDG-PET/CT 1 Department of Nuclear
Medicine, Shanghai Sixth People’s Hospital, Shanghai Jiao Tong University, Shanghai, China
Correspondence to:
Quan-Yong Luo
Department of Nuclear Medicine, Shanghai Sixth People’s Hospital, Shanghai Jiao Tong University, 600 Yishan Road,
Shanghai, 200233, P. R. China [email protected]
Cop
yright
© ABE&M t
odos os dir
eit
os r
eser
vados
.
INTRODUCTION
D
ifferentiated thyroid carcinoma (DTC) is the most common endocrine malignancy and ac-counts for less than 1% of malignant neoplasms in hu-mans (1). The overall prognosis for DTC patients is one of the best among all types of cancer, with a 10-year survival rate over 85-90%, but its incidence is gradually increasing in different parts of the world (2,3). Although DTC is generally characterized by an indolent course with low mortality, patients with distant metastases have strong prognosis of mortality, and more than 50% of these DTC patients die from distant metastatic di-sease during follow-up (4). Distant metastases derived from DTC occur in 5-23% of patients at presentation and during follow-up (5,6).The major sites of distant metastases from DTC are the lungs and bones, while minor sites include the brain, liver, skin, and muscle. In contrast, renal metas-tases from DTC are extremely rare. Ahmed and cols. (7) reported that from December 1975 to September 2005, only one case of DTC metastasizing to the kid-ney was found among 3,500 DTC patients at their in-stitution. To the best of our knowledge, only 26 cases have been reported in the literature to date.
131I has been used as a therapy for distant metastases
from DTC for over 60 years and has been an important component in the management of DTC. Traditionally,
131I whole-body scans (131I-WBS) have been performed
to localize 131I uptake and detect residual (or recurrent)
disease and distant metastases after 131I treatment.
How-ever, the precise anatomical localization of foci with in-creased 131I uptake is dificult on planar images because
of the lack of anatomical landmarks. By precisely local-izing 131I uptake, 131I single photon emission computed
tomography/computed tomography (131I-SPECT/
CT) might improve the diagnostic accuracy of 131I
scan-ning, thus improving the management of diseases in patients (8,9). Scans based on 18F-luorodeoxyglucose
positron emission tomography/computed tomography (18F-FDG-PET/CT) are well established for detecting
recurring or metastatic DTC in patients with a negative
131I-WBS and elevated serum Tg (10,11). Moreover,
noninvasive imaging tools, including ultrasonography (US), enhanced CT, and magnetic resonance imaging (MRI), are useful for the detection of distant metasta-ses (suspected according to clinical symptoms) in the follow-up of DTC.
Because of its limited and rare appearance, renal me-tastasis from DTC has only been occasionally reported, mainly as case reports or a small case series. Therefore, the diagnosis and eficacy of 131I therapy have not been
clearly deined and need further research. In this study, we retrospectively reviewed 14 patients treated with 131I
at Shanghai Sixth People’s Hospital in China. We ex-plored their clinical characteristics, as well as methods for 131I-based detection and treatment of renal
metas-tases from DTC.
SUBJECTS AND METHODS
Subjects
A total of 2,955 DTC patients were enrolled in this stu-dy at the Department of Nuclear Medicine of Shanghai Sixth People’s Hospital, a major referral site in China for
131I treatment. All patients were treated with 131I for the
ablation of postsurgical thyroid remnants, or treatment of metastases after total or near-total thyroidectomy from January 1998 to January 2012. Among them, 14 patients had diagnosis of renal metastases from DTC.
Methods for 131I therapy and follow-up
All patients stopped taking thyroid hormone medication and began a low iodine diet 3-4 weeks before radioio-dine therapy (thyroid stimulating hormone (TSH) rea-ching levels of ≥ 30 mIU/L). The patients received an oral administration of 131I after examinations, including
FT3, FT3, FT4, TSH, Tg and anti-Tg antibody (TgAb) tests, neck ultrasonography, X-ray, CT, MRI, and who-le-body bone scans. 131I-WBS or 131I-SPECT/CT fusion
imaging was performed 5 days after 131I administration.
The irst oral dose of 3.7 GBq of 131I was given to
re-move thyroid remnants. The oral administration of 7.4 GBq of 131I was then given each time for the treatment
of renal metastases. The treatment interval varied from 4 to 12 months, and the treatment was repeated 2-8 times. The time diagnosing renal metastases was establi-shed from 0.4 yrs. to 14.3 yrs. with a median time of 5.8 yrs. after the initial thyroid surgical treatment
Detection and diagnosis of renal metastases from DTC
The detection of renal metastases was carried out by means of one of two approaches: (1) if 131I-WBS (with
or without SPECT/CT) demonstrates 131I uptake in
Cop
yright
© ABE&M t
odos os dir
eit
os r
eser
vados
.
or MRI ) can be used to indicate renal metastasis (se-rum levels of Tg should also be elevated), and (2) if
131I-WBS reveals no 131I uptake, 18F-FDG-PET/CT,
enhanced CT, MRI, or US scans that are positive (with elevated serum Tg) may indicate renal metastases from DTC. The diagnosis of renal metastases was conirmed by pathology results and clinical follow-up of renal le-sions from DTC.
Evaluation of eficacy
The therapeutic effects of 131I therapy for renal
metas-tases from DTC were evaluated based on changes in serum Tg levels and alterations in the anatomical ima-ging of renal metastatic lesions. Serum Tg levels were measured with the Immulite chemiluminescent immu-noassay system (Diagnostic Products Corporation, Los Angeles, CA, USA). Serum TSH and anti-Tg antibody (TgAb) levels were also measured. The evaluation of anatomical images was performed based on methods established by RECIST 1.1. The responses deined by RECIST 1.1 are as follows: complete response (CR): disappearance of all target lesions, any pathological le-sions (target or non-target) must have a reduction in short axis to < 10 mm; partial response (PR): at le-ast a 30% decrease in the diameters of target lesions; progressive disease (PD): at least a 20% increase in the diameters of target lesions, combined with an absolute increase of at least 5 mm in the sum of diameters (in addition, appearance of one or more new lesions was also considered progression); stable disease (SD): nei-ther suficient shrinkage to qualify for PR nor suficient increases to qualify for PD.
Statistical analysis
SPSS17.0 was used for statistical analysis. Tg changes were estimated by the Wilcoxon signed rank test. A p value < 0.05 was considered a statistically signiicant di-fference.
RESULTS
Demographic features of the patients
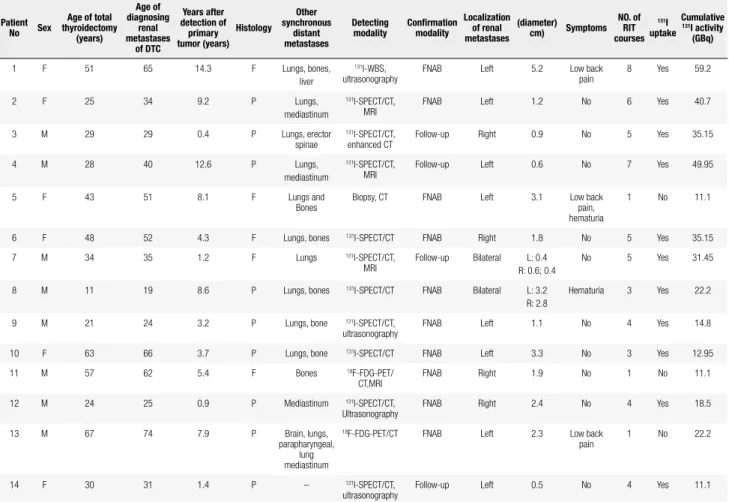
Fourteen patients were diagnosed with renal metastases from DTC with multimodality imaging, with an inci-dence of 0.47% (14/2955). The characteristics of these 14 DTC patients are summarized in table 1. Their ages ranged from 17 to 74 years, with a mean of 43 years.
Seven subjects were over 45 years of age, and seven were less than 45 years. Eight subjects were males and six were females (male-to-female ratio of 1.3:1). The distribution of DTC pathological types included nine cases of papillary thyroid cancer and ive cases of folli-cular thyroid cancer. Of the 14 cases, only one (case 14) had a single renal metastasis, whereas 13 cases presen-ted combined metastases to other organs: 11 patients had lung metastases, seven had bone metastases, three had mediastinal metastases, and there was one case each of metastasis to the brain, muscle, liver, and parapha-ryngeal region. Renal metastases were asymptomatic in nine patients, but found on imaging follow-up studies. Three patients had symptoms of lower back pain, and two had hematuria.
DETECTION OF RENAL METASTASES FROM DTC
Discovery of functional renal metastases
Renal metastases from DTC that were detected with multimodality imaging are shown in igure 1. In the detection of renal metastases from DTC after 131I
tre-atment, 131I-WBS found 21 lesions (indicating
abnor-mal 131I uptake) in the abdomen of 11 DTC patients,
suggesting distant metastases from DTC, of which a total of 10 patients with 13 lesions were located in the kidneys after 131I-SPECT/CT. Four cases with four
le-sions were found in the left kidneys, four cases with four lesions were found in the right kidneys, and two cases with ive lesions were bilateral; among them, one case (case 7) with three lesions was found bilateral in the kidneys, one lesion in the left kidney and two le-sions in the right kidney. Of those 10 patients with 13 renal metastatic lesions revealed by 131I-SPECT/CT, all
patients were SPECT-positive; but only three patients with ive lesions (cases 6, 8, and 10) were CT-positive, with the remaining eight lesions of seven DTC patients (cases 2, 3, 4, 7, 9, 11, and 14) presenting equivocal or negative CT, suggesting early or small renal metastases. In these seven patients, three (cases 2, 4, and 7) were synchronous with MRI (Figure 2), three (cases 9, 12, and 14) with US, and one case (case 3) with enhan-ced CT. Among the remaining eight 131I-uptake foci,
one renal metastatic lesion in a DTC patient with lower back pain (case 1) was shown by 131I-WBS combined
Cop
yright
© ABE&M t
odos os dir
eit
os r
eser
vados
.
Table 1. Characteristics and related data of patients with renal metastases from differentiated thyroid carcinoma
Patient No Sex
Age of total thyroidectomy (years) Age of diagnosing renal metastases of DTC Years after detection of primary tumor (years) Histology Other synchronous distant metastases Detecting modality Conirmation modality Localization of renal metastases (diameter) cm) Symptoms NO. of RIT courses 131I uptake Cumulative
131I activity
(GBq)
1 F 51 65 14.3 F Lungs, bones,
liver
131I-WBS,
ultrasonography
FNAB Left 5.2 Low back
pain
8 Yes 59.2
2 F 25 34 9.2 P Lungs,
mediastinum
131I-SPECT/CT,
MRI
FNAB Left 1.2 No 6 Yes 40.7
3 M 29 29 0.4 P Lungs, erector
spinae
131I-SPECT/CT,
enhanced CT
Follow-up Right 0.9 No 5 Yes 35.15
4 M 28 40 12.6 P Lungs,
mediastinum
131I-SPECT/CT,
MRI
Follow-up Left 0.6 No 7 Yes 49.95
5 F 43 51 8.1 F Lungs and
Bones
Biopsy, CT FNAB Left 3.1 Low back
pain, hematuria
1 No 11.1
6 F 48 52 4.3 F Lungs, bones 131I-SPECT/CT FNAB Right 1.8 No 5 Yes 35.15
7 M 34 35 1.2 F Lungs 131I-SPECT/CT,
MRI
Follow-up Bilateral L: 0.4 R: 0.6; 0.4
No 5 Yes 31.45
8 M 11 19 8.6 P Lungs, bones 131I-SPECT/CT FNAB Bilateral L: 3.2
R: 2.8
Hematuria 3 Yes 22.2
9 M 21 24 3.2 P Lungs, bone 131I-SPECT/CT,
ultrasonography
FNAB Left 1.1 No 4 Yes 14.8
10 F 63 66 3.7 P Lungs, bone 131I-SPECT/CT FNAB Left 3.3 No 3 Yes 12.95
11 M 57 62 5.4 F Bones 18F-FDG-PET/
CT,MRI
FNAB Right 1.9 No 1 No 11.1
12 M 24 25 0.9 P Mediastinum 131I-SPECT/CT,
Ultrasonography
FNAB Right 2.4 No 4 Yes 18.5
13 M 67 74 7.9 P Brain, lungs,
parapharyngeal, lung mediastinum
18F-FDG-PET/CT FNAB Left 2.3 Low back
pain
1 No 22.2
14 F 30 31 1.4 P – 131I-SPECT/CT,
ultrasonography
Follow-up Left 0.5 No 4 Yes 11.1
M: male; F: female; years: years after detection of primary tumor; CT: computed tomography; MRI: magnetic resonance imaging; 131I-SPECT/CT: single-photon emission computed tomography/
computed tomography.
Figure 1. Renal metastases from DTC detected with multimodality imaging.
11 and 13) with renal metastases were observed with
18F-FDG-FET/CT (Figure 3); one lesion in one patient
(case 11) was 18F-FDG-FET–positive but CT-equivocal
and conirmed by MRI, and one patient was positive by 18F-FDG-FET and CT (case 13) (Figure 3). The
re-maining patient (case 5), who had lower back pain and hematuria, but was negative in 131I-WBS with elevated
serum Tg, had renal metastasis identiied by CT.
Diagnosis of renal metastases from DTC
Among 14 DTC patients with renal metastases, ten cases (71.43%) were diagnosed based on pathological results (cases 1, 2, 5, 6, 8, 9, 10, 11, 12, and 13) and the remaining four cases (28.57%) with renal metastases also should be considered by clinical follow-up because lesions were considered too small for a ine-needle as-piration biopsy. Moreover, 131I-SPECT/CT combined
with MRI (cases 4 and 7), enhanced CT (case 3), or US (case 14) showed the existence of renal lesions after several 131I therapy.
Renal metastases from DTC
Post-therapeutic 131I-WBS (n = 14)
Symptoms (n = 1)
Definitive (n = 3)
Equivocal (n = 7)
Definitive (n = 1)
Equivocal (n = 1)
Further confirrmed by US (n = 4), enhanced CT (n = 1), MRI (n = 4) and CT (n = 1)
131I-SPECT/CT (n = 10)
18F-FDG-PET/CT (n = 2)
Symptoms (n = 1) 131I uptake in the abdomen
with high level of Tg or TgAb (n = 11)
No 131I uptake in the abdomen with high level of Tg (n = 3)
Discovery of non-functional renal metastases
Cop
yright
© ABE&M t
odos os dir
eit
os r
eser
vados
.
Figure 2. A 40-year-old male patient who presented mediastinal lymph node and pulmonary metastases from papillary thyroid cancer was treated with
131I for postsurgical thyroid remnants and metastases. An unexpected lesion with 131Iuptake in the left abdomen, mediastinal lymph node, and lungs
(suggesting metastasis) was observed on a 131I-WBS 5 days after an oral therapeutic dose of 131I (A: arrow). To localize this unexpected lesion of 131I
uptake, a subsequent low-dose 131I-SPECT/CT scan was performed using a GE Hawkeye Millennium. Fusion images showed that the lesion was located
in the left kidney (B-D: crossing line). Further examination with MRI revealed a solitary metastatic lesion with a diameter of 8 mm in the upper pole of the left kidney (E-F: arrow).
Figure 3. A 74-year-old male patient with lower back pain was given 131I
treatment after total thyroidectomy. No abnormal 131Iuptake was found in
the post-therapeutic 131I-WBS with elevated serum Tg and 18F-FDG-PET/
CT was performed to search for potential metastatic lesions. Maximum intensity projections in 18FDG-PET revealed more intense 18FDG uptake
lesions in the chest and abdomen (A: arrow). 18F-FDG-PET/CT revealed a
prominent 18FDG uptake lesion with a diameter of 23 mm in the upper pole
of the left kidney (B-D: arrow).
Responses to 131I therapy
Among 14 patients, three patients with renal metasta-ses did not accumulate 131I after 131I treatment;
there-fore, responses to 131I therapy were ineffective for them.
Changes in serum Tg
All eleven 131I-avid patients received approximately
three to eight courses of 131I treatment at an interval of
4-12 months. The median stimulated serum Tg level was 4659 ng/mL (range 87-18191 ng/mL) before the irst 131I treatment, and 4194 ng/mL (range 31701-19
ng/mL) before the last 131I treatment. There were no
marked differences in serum Tg before and after 131I
treatments (Z = 0.157; p = 0.875). Serum Tg levels in 81.82 % (9/11) of the patients showed a gradual de-cline, while 18.18% (2/11) of the patients showed a signiicant elevation. In one patient (case 14), serum Tg level was normal and stabilized at about 2.56 and 9.3 ng/mL; however, TgAbs were obviously high and changed from 327 to 92 u/mL after several 131I
treat-ments (Table 2).
Anatomical imaging changes after 131I therapy
Cop
yright
© ABE&M t
odos os dir
eit
os r
eser
vados
.
indings suggest that the disease remains stable. The re-nal metastases progressed in two patients showing PD. No patient reached CR (Table 2).
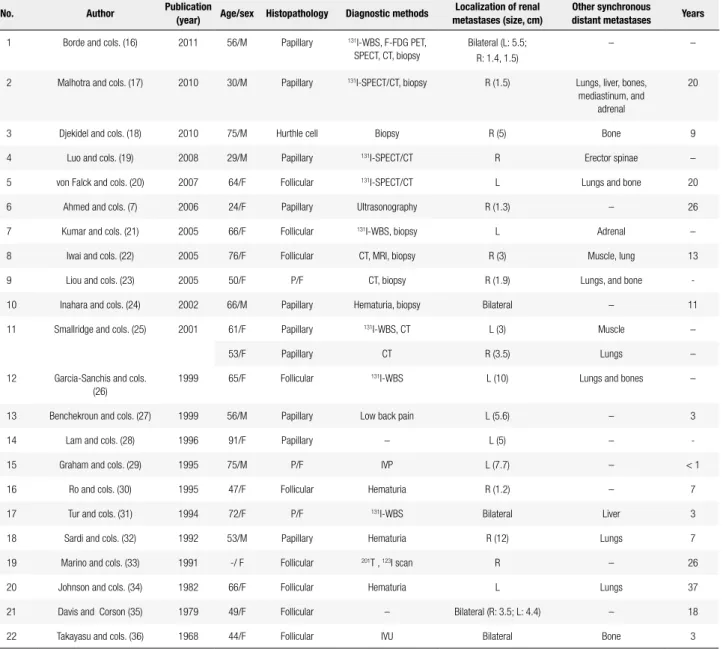
metastasis to the kidneys is quite rare; a retrospective review of the literature revealed only 26 case reports of renal metastases arising from DTC. Of the 26 cases of renal metastasis associated with DTC, full-text studies of three patients were not found using the PubMed and EMBASE databases; the other 23 patients are reviewed in table 3 (7,16-36). We previously reported one case of renal metastases from DTC, a 29-year-old man with concomitant metastases to the erector spinae and lungs (case 7) (19). Most subjects were females over 45 years of age; nine cases were FTC, 10 cases PTC, three cases a follicular variant of PTC, and one case of Hurthle cell thyroid cancer. However, because of its limited ex-pression and rarity, renal metastasis from DTC has only been occasionally reported, mainly as case reports or a small case series. Here, a relatively large number of DTC cases from renal metastasis were described in this study. The overall prevalence of renal metastasis from DTC was about 0.47% (14 of 2,955). Similar to our patients, most of the previously reported patients had advanced DTC with metastases to other organs when renal metastases were found. In our study, a 31-year-old female with a single left renal metastasis from DTC was the only case detected by 131I-SPECT/CT and US
after 131I treatment.
The 131I-WBS is indispensable for inding distant
metastases because of their ability to accumulate 131I
through the sodium iodide (Na+/I-) symporter after
an oral dose of 131I. In our series, most DTC patients
(11/14) with renal metastases have the ability to take up 131I. However, the accurate localization of focal
ac-tivity by 131I-WBS is dificult because of the lack of
ana-tomical markers. Therefore, renal metastases from DTC are easily misinterpreted as an intestinal physiological uptake frequently observed through 131I-WBS in DTC
patients. In recent years, 131I-SPECT/CT has emerged
in this setting as a useful tool for accurately locating sites of pathological uptake and identifying physiologi-cal mimics of disease, thus providing a more accurate staging of prognostic information for risk stratiication which, in its turn, tailors management and follow-up regimens (37). 131I-SPECT/CT for anatomic
localiza-tion of renal metastases has been reported in past re-views (19,20). In our cases, 10 DTC patients with renal metastases were detected by 131I-WBS combined with 131I-SPECT/CT, suggesting that the additional
diag-nostic information provided by 131I-SPECT/CT over 131I-WBS could detect renal metastases from DTC
pa-tients. Patients with renal metastases are usually
asymp-Table 2. Response of DTC patients with renal metastases after 131I
treatment
Patient nº
Stimulated Tg before irst 131I
treatment (ng/mL)
Stimulated Tg before last 131I treatment
(ng/mL)
Imaging change after 131I treatment
1 8,752 6,923 PD
2 640.7 289 SD
3 567 19 SD
4 401 123 SD
6 5,463 6,376 SD
7 18,191 602 PR
8 17,016 31,701 PD
9 87 22 SD
10 39.38 22.64 SD
12 94 52 SD
13 13,562 17,817 PD
14 2.56 9.3 SD
PR: partial response; SD: stable disease; PD: progressive disease.
DISCUSSION
Differentiated thyroid cancer (DTC) has been reported to present initially distant metastases in about 4% of cases. During follow-up, distant metastases develop in 2-34% of cases (12). The presence of distant metastases relects advanced clinical presentation, associated with higher mortality rate, especially in elderly patients (13). However, 131I-WBS combined with elevated serum Tg
can contribute to the early detection of distant metasta-ses (at a time when other radiological studies are nega-tive), and the disease is potentially curable by means of
131I therapy (14,15).
Cop
yright
© ABE&M t
odos os dir
eit
os r
eser
vados
.
Table 3. Renal metastases from differentiated thyroid cancer previously reported in the literature
No. Author Publication
(year) Age/sex Histopathology Diagnostic methods
Localization of renal metastases (size, cm)
Other synchronous
distant metastases Years
1 Borde and cols. (16) 2011 56/M Papillary 131I-WBS, F-FDG PET,
SPECT, CT, biopsy
Bilateral (L: 5.5; R: 1.4, 1.5)
– –
2 Malhotra and cols. (17) 2010 30/M Papillary 131I-SPECT/CT, biopsy R (1.5) Lungs, liver, bones,
mediastinum, and adrenal
20
3 Djekidel and cols. (18) 2010 75/M Hurthle cell Biopsy R (5) Bone 9
4 Luo and cols. (19) 2008 29/M Papillary 131I-SPECT/CT R Erector spinae –
5 von Falck and cols. (20) 2007 64/F Follicular 131I-SPECT/CT L Lungs and bone 20
6 Ahmed and cols. (7) 2006 24/F Papillary Ultrasonography R (1.3) – 26
7 Kumar and cols. (21) 2005 66/F Follicular 131I-WBS, biopsy L Adrenal –
8 Iwai and cols. (22) 2005 76/F Follicular CT, MRI, biopsy R (3) Muscle, lung 13
9 Liou and cols. (23) 2005 50/F P/F CT, biopsy R (1.9) Lungs, and bone
-10 Inahara and cols. (24) 2002 66/M Papillary Hematuria, biopsy Bilateral – 11
11 Smallridge and cols. (25) 2001 61/F Papillary 131I-WBS, CT L (3) Muscle –
53/F Papillary CT R (3.5) Lungs –
12 Garcia-Sanchis and cols.
(26)
1999 65/F Follicular 131I-WBS L (10) Lungs and bones –
13 Benchekroun and cols. (27) 1999 56/M Papillary Low back pain L (5.6) – 3
14 Lam and cols. (28) 1996 91/F Papillary – L (5) –
-15 Graham and cols. (29) 1995 75/M P/F IVP L (7.7) – < 1
16 Ro and cols. (30) 1995 47/F Follicular Hematuria R (1.2) – 7
17 Tur and cols. (31) 1994 72/F P/F 131I-WBS Bilateral Liver 3
18 Sardi and cols. (32) 1992 53/M Papillary Hematuria R (12) Lungs 7
19 Marino and cols. (33) 1991 -/ F Follicular 201T , 123I scan R – 26
20 Johnson and cols. (34) 1982 66/F Follicular Hematuria L Lungs 37
21 Davis and Corson (35) 1979 49/F Follicular – Bilateral (R: 3.5; L: 4.4) – 18
22 Takayasu and cols. (36) 1968 44/F Follicular IVU Bilateral Bone 3
M: male; F: female; P/F: follicular variant of papillary thyroid cancer; years: years after detection of primary tumor; 131I-WBS: 131I-whole body scintigraphy; CT: computed tomography; MRI: magnetic
resonance imaging; 131I-SPECT/CT: single-photon emission computed tomography/computed tomography. IVP: intravenous pyelogram; IVU: International Vegetarian Union.
tomatic and most are less than 45 years old, as seen in our cases, also suggesting that avid 131I metastatic foci
of renal metastasis could be detected at an early stage by 131I-SPECT/CT scan.
Due to dedifferentiation, about 20-50% of metastat-ic DTC have no ability to take up 131I. The deinitive
role of 18F-FDG-PET/CT in DTC patients with serum
Tg levels and negative 131I-WBS has been consistently
demonstrated (38). The discrepancy between the two imaging tools is attributable to the lip-lop phenome-non of 131I and 18F-FDG (39). Three patients with three
lesions did not accumulate 131I after 131I treatment.
Among them, two DTC patients had renal metastases discovered on 18F-FDG-FET/CT (originally done to
evaluate elevated Tg). Moreover, Borde and cols. also described renal metastases that had no uptake of 131I
but were detected by 18F-FDG-FET/CT in a
56-year-old male PTC patient (16). Tumors with 131I
Cop
yright
© ABE&M t
odos os dir
eit
os r
eser
vados
.
imaging scans without clinical symptoms or clinical sus-picion prior to the initiation of various therapies. For example, because of lower back pain and hematuria, a 51-year-old female patient with no avid 131I was found
to have a left renal metastasis from DTC by CT com-bined with biopsy in our study.
Renal metastatic foci from DTC (regardless of 131I
avidity) can be accurately localized with 131I-SPECT/
CT or 18F-FDG-FET/CT; however, renal lesions less
than 1.0 cm are too small for detection by CT scans. Moreover, Blum and cols. (40) reported a sixty-three-year-old woman (with a history of PTC) treated with surgery and then ablation with 100 mCi of 131I.
Post-treatment WBS demonstrated an equivocal signal in the upper right abdomen that 131I-SPECT/CT later
conirmed as 131I accumulation within a benign renal
cyst. These are strong reminders that 131I-SPECT/CT
and 18F-FDG-FET/CT images are valuable in inding,
but not completely in diagnosing, rare renal metasta-ses from DTC. Thus, other imaging modalities need to be applied for inding renal metastases when metastatic foci are positive in 131I-SPECT or 18F-FDG-FET, but
negative or equivocal in CT scans in the follow-up of DTC. These other modalities, including US, enhanced CT, and MRI, are especially useful tools to detect small (< 1 cm) or cryptic renal lesions unseen on CT scans. Of the 14 patients here, four were further identiied by MRI scan, four by US, one by enhanced CT, and one by biopsy. Therefore, multimodality imaging is essen-tial to accurately assess the extent of renal metastases from DTC to guide treatment, prevent tumor progres-sion, and improve survival.
Due to the rare occurrence of renal metastases from DTC, the best management for this condition is un-clear. Since most cases are associated with metastases at other sites, surgical excision, with its risks and limited eficacy, is not a practical solution. Although external beam radiotherapy can provide local tumor control in a high percentage of cases, its eficacy is transient and dose-dependent. To obtain a longer lasting eficacy, a high dose of irradiation may be required and adverse effects must be considered. In addition, it is usually ap-plied to treat a single metastasis and is unsuitable for the treatment of multiple metastases.
Sorafenib is a multikinase inhibitor that targets sev-eral molecular signals involved in the pathogenesis of DTC, and that has been used in the treatment of ad-vanced or metastatic 131I-refractory DTC (41).
How-ever, it has only been reported as an anti-cancer drug
for DTC with distant metastases, but not avid 131I lung
metastases, in recent years. Therefore, these treatments have not been applied in this group of patients. Cur-rently, 131I therapy is the treatment of choice for most
DTC patients with distant metastases after thyroidec-tomy. If renal metastases from DTC have excellent 131I
uptake, they can be differentiated from other malignant neoplasms based on this feature, and be treated with
131I. However, there are no data showing the eficacy
of 131I for the treatment of renal metastases from DTC
due to their rarity. Here, the therapeutic effects of 131I
therapy on renal metastases from DTC were evaluat-ed basevaluat-ed on changes in serum Tg and alterations in anatomical imaging of metastatic renal lesions. In our study, among the 14 DTC patents with renal metasta-ses, 11 patients showed avidity for 131I.
Serum Tg is a highly sensitive and speciic marker of DTC metastasis and recurrence, which also relects tumor burden. Serum Tg is usually signiicantly ele-vated in DTC patients with distant metastases. Thus, the pronounced reduction in Tg (at roughly the same TSH level) indicates that 131I therapy can eliminate
some tumor cells after multiple treatments (4). In our study, serum Tg levels in 81.82% (9/11) patients showed a gradual decline and 18.18% (2/11) patients showed a signiicant elevation, suggesting that 131I is
partly effective for the treatment of DTC patients with renal metastases. Because the detection of Tg may be disturbed by TgAbs, we measured serum levels of Tg and TgAbs simultaneously in all patients. In only one patient in this study, serum TgAb levels increased to a certain extent (> 100 ng/mL) but Tg levels were nor-mal and stabilized at about 2.56 and 9.3 ng/mL. After
131I therapy, serum levels of TgAbs decreased markedly.
After 131I therapy, MRI examinations revealed
sta-tistically signiicant shrinking of metastatic renal lesions in only one patient. This improvement may be due to small lesions or those that were at an early stage. The anatomical imaging of renal metastases with excellent avidity for 131I showed insigniicant changes in eight
patients (72.73%), indicating that those lesions were stable. Though renal metastatic foci accumulated 131I,
US still showed PD in a patient, suggesting renal me-tastasis in this DTC patient may exhibit dedifferentia-tion (42). Renal metastatic foci in the remaining three patients gradually increased without 131I uptake after 131I treatment. Therefore, 131I treatment is ineffective
Cop
yright
© ABE&M t
odos os dir
eit
os r
eser
vados
.
CONCLUSION
In summary, renal metastasis is an extremely rare pattern of invasion from DTC with an incidence of 0.47%. 131I-SPECT/CT, combined with other
imag-ing modalities after 131I-WBS, can contribute to the
early detection of renal metastases and is essential to accurately assess the extent of renal metastases from DTC to guide treatment and prevent tumor progres-sion. 131I therapy can signiicantly decrease serum Tg,
and shrink or stabilize renal metastatic lesions with ex-cellent avidity for 131I.
Conlict of interest disclosure: Zhong-Ling Qiu and Yan-Li Xue contributed equally to this work. This study was sponsored by the National Natural Science Foundation of China (No: 81201115).
REFERENCES
1. Jemal A, Siegel R, Xu J, Ward E. Cancer statistics. CA Cancer J Clin. 2010;60:277-300.
2. Schlumberger MJ. Papillary and follicular thyroid carcinoma. N Engl J Med. 1998;338:297-306.
3. Zanotti-Fregonara P, Rubello D, Hindié E. Bone metastases of di-fferentiated thyroid cancer: the importance of early diagnosis and 131I therapy on prognosis. J Nucl Med. 2008,49:1902-3. 4. Qiu ZL, Song HJ, Xu YH, Luo QY. Eficacy and survival analysis
of 131I therapy for bone metastases from differentiated thyroid cancer. J Clin Endocrinol Metab. 2011;96:3078-86.
5. Nixon IJ, Whitcher MM, Palmer FL, Tuttle RM, Shaha AR, Shah JP, et al. The impact of distant metastases at presentation on progno-sis in patients with differentiated carcinoma of the thyroid gland. Thyroid. 2012;22(9):884-9.
6. Schlumberger M, Challeton C, De Vathaire F, Travagli JP, Gardet P, Lumbroso JD, et al. Radioactive iodine treatment and external radiotherapy for lung and bone metastases from thyroid carcino-ma. J Nucl Med. 1996;37:598-605.
7. Ahmed M, Aslam M, Ahmed J, Faraz HA, Almahfouz A, Al Arii A, et al. Renal metastases from thyroid cancer masquerading as renal angiomyolipoma on ultrasonography. J Ultrasound Med. 2006;25:1459-64.
8. Schmidt D, Szikszai A, Linke R, Bautz W, Kuwert T. Impact of 131I SPECT/spiral CT on nodal staging of differentiated thyroid carci-noma at the irst radioablation. J Nucl Med. 2009;50:18-23. 9. Grewal RK, Tuttle RM, Fox J, Borkar S, Chou JF, Gonen M, et al.
The effect of posttherapy 131I SPECT/CT on risk classiication and management of patients with differentiated thyroid cancer. J Nucl Med. 2010;51:1361-7.
10. Shammas A, Degirmenci B, Mountz JM, McCook BM, Branstetter B, Bencherif B, et al. 18F-FDG PET/CT in patients with suspected recurrent or metastatic well-differentiated thyroid cancer. J Nucl Med. 2007;48:221-6.
11. Quon A, Fischbein NJ, McDougall IR, Le QT, Loo BW Jr, Pinto H, et al. Clinical role of 18F-FDG PET/CT in the management of squa-mous cell carcinoma of the head and neck and thyroid carcinoma. J Nucl Med. 2007;48 Suppl 1:58S-67S.
12. Shaha AR, Ferlito A, Rinaldo A. Distant metastases from thyroid and parathyroid cancer. ORL J Otorhinolaryngol Relat Spec. 2001;63:243-9.
13. Lundgren CI, Hall P, Dickman PW, Zedenius J. Clinically signiicant prognostic factors for differentiated thyroid carcinoma: a popu-lation-based, nested case-control study. Cancer. 2006;106:524-31. 14. McKenna SRJ, Murphy GP. Cancer surgery. Philadelphia, PA: JB
Lippincott CO; 1994. p. 485.
15. Heitz P, Moster H, Staub JJ. Thyroid cancer: a study of 573 thyroid tumors and 161 autopsy cases observed over a thirty-year period. Cancer. 1976;37:2329-37.
16. Borde C, Basu S, Kand P, Arya S, Shet T. Bilateral renal metastases from papillary thyroid carcinoma on post 131I treatment scan: lip-lop sign, radioiodine SPET, 18F-FDG PET, ECT and histopa-thological correlation. Hell J Nucl Med. 2011;14:72-3.
17. Malhotra G, Upadhye TS, Sridhar E, Asopa RV, Garde PS, Gawde S, et al. Unusual case of adrenal and renal metastases from pa-pillary carcinoma of thyroid. Clin Nucl Med. 2010;35:731-6. 18. Djekidel M, Gordon M, Shah RB, Gross MD, Avram A. Renal
me-tastasis from Hurthle cell thyroid carcinoma and its evaluation with hybrid imaging. Thyroid. 2010;20:429-33.
19. Luo Q, Luo QY, Sheng SW, Chen LB, Yu YL, Lu HK, et al. Locali-zation of concomitant metastases to kidney and erector spinae from papillary thyroid carcinoma using (131)I-SPECT and CT. Thyroid. 2008;18:663-4.
20. von Falck C, Beer G, Gratz KF, Galanski M. Renal metastases from follicular thyroid cancer on SPECT/CT. Clin Nucl Med. 2007;32:751-2.
21. Kumar A, Nadig M, Patra V, Srivastava DN, Verma K, Bal CS. Adre-nal and reAdre-nal metastases from follicular thyroid cancer. Br J Ra-diol. 2005;78:1038-41.
22. Iwai H, Ohno Y, Ito H, Kiyokawa T, Aoki N. Renal rupture asso-ciated with a poorly differentiated follicular thyroid carcinoma metastasizing to the thigh muscle, lung and kidney. Intern Med. 2005;44:848-52.
23. Liou MJ, Lin JD, Chung MH, Liau CT, Hsueh C. Renal metasta-sis from papillary thyroid microcarcinoma. Acta Otolaryngol. 2005;125:438-42.
24. Inahara M, Mikami K, Tobe T, Suzuki H, Itou H. [A case of thyroid cancer metastasizing to the bilateral kidneys]. Hinyokika Kiyo. 2002;48:315-7.
25. Smallridge RC, Castro MR, Morris JC, Young PR, Reynolds JC, Merino MJ, et al. Renal metastases from thyroid papillary car-cinoma: study of sodium iodide symporter expression. Thyroid. 2001;11:795-804.
26. Garcia-Sanchis L, Lopez-Aznar D, Oltra A, Rivas A, Alonso J, Mon-talar J, et al. Metastatic follicular thyroid carcinoma to the kidney: a case report. Clin Nucl Med. 1999;24:48-50.
27. Benchekroun A, Lachkar A, Alami M, Iken A, Soumana A, Farih MH, et al. Thyroid cancer metastasizing to the kidney. Report of a case. Ann Urol (Paris). 1999;33:51-4.
28. Lam KY, Ng WK. Follicular carcinoma of the thyroid appearing as a solitary renal mass. Nephron. 1996;73:323-4.
29. Graham LD, Roe SM. Metastatic papillary thyroid carcinoma pre-senting as a primary renal neoplasm. Am Surg. 1995;61:732-4. 30. Ro HJ, Ha HK, Kim HS, Shinn KS. Renal metastasis from thyroid
carcinoma visible as a hyperdense lesion on unenhanced CT. AJR Am J Roentgenol. 1995;165:1018.
31. Tur GE, Asanuma Y, Sato T, Kotanagi H, Sageshima M, Yong-Jie Z, et al. Resection of metastatic thyroid carcinomas to the liver and the kidney: report of a case. Surg Today. 1994;24:844-8.
32. Sardi A, Agnone CM, Pellegrini A. Renal metastases from papilla-ry thyroid carcinoma. J La State Med Soc. 1992;144:416-20. 33. Marino G, Cocimano V, Taraglio S, Testori O. Metastasis of thyroid
Cop
yright
© ABE&M t
odos os dir
eit
os r
eser
vados
.
34. Johnson MW, Morettin LB, Sarles HE, Zaharopoulos P. Follicular carcinoma of the thyroid metastatic to the kidney 37 years after resection of the primary tumor. J Urol. 1982;127:114-6.
35. Davis RI, Corson JM. Renal metastasis from well differentiated follicular thyroid carcinoma. Cancer. 1979;43:265-8.
36. Takayasu H, Kumamoto Y, Terawaki Y, Ueno A. A case of bilateral metastatic renal tumor originating from a thyroid carcinoma. J Urol. 1968;100:717-9.
37. Avram AM. Radioiodine scintigraphy with SPECT/CT: an impor-tant diagnostic tool for thyroid cancer staging and risk stratiica-tion. J Nucl Med. 2012;53:754-64.
38. Feine U, Lietzenmayer R, Hanke JP, Held J, Wöhrle H, Müller--Schauenburg W. Fluorine-18-FDG and iodine-131 uptake in thyroid cancer. J Nucl Med. 1996;37:1468-72.
39. Fletcher JW, Djulbegovic B, Soares HP, Siegel BA, Lowe VJ, Ly-man GH, et al. Recommendations on the use of 18F-FDG PET in oncology. J Nucl Med. 2008;49:480-508.
40. Blum M, Tiu S, Chu M, Goel S, Friedman K. I-131 SPECT/CT elu-cidates cryptic indings on planar whole-body scans and can re-duce needless therapy with I-131 in post-thyroidectomy thyroid cancer patients. Thyroid. 2011;21:1235-47.
41. Cabanillas ME, Waguespack SG, Bronstein Y, Williams MD, Feng L, Hernandez M, et al. Treatment with tyrosine kinase inhibitors for patients with differentiated thyroid cancer: the M. D. Ander-son experience. J Clin Endocrinol Metab. 2010;95:2588-95. 42. Qiu ZL, Luo QY. Coexistant iodine-negative pleura metastasis