Rev. esc. enferm. USP vol.49 número6
Texto
Imagem
Documentos relacionados
All patients were assessed at baseline and 2, 4, 8 and 12 weeks after injection for Modified Ashworth Score, time walking 10 meters, and the Functional Independence Measure
Method: Twenty patients with chronic craniofacial pain and PD ( CFP group ) and 20 patients with PD ( PD group ) were assessed before and after periodontal treatment (baseline,
Method: Sixty five out of sixty seven consecutive patients with CD were assessed with two instruments: Short-form Health Survey with 36 questions (SF-36) and Toronto
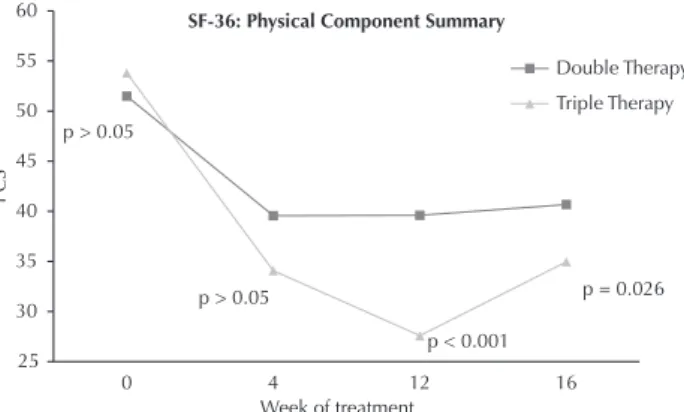
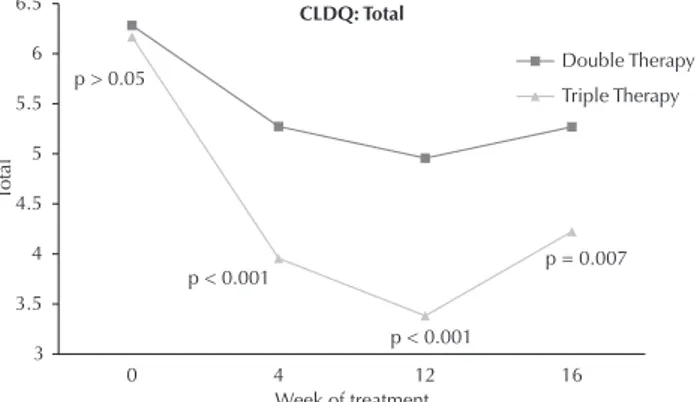
The assessment of fatigue and its effects in patients with liver disease has traditionally been performed using general questionnaires and Short Form Health Survey (SF-36) (28) ,
his study has found that, in the perception of nurses, the main factors that negatively inluence the quality of CPR in adult inpatient units are: high number of
Knowledge and attitudes of nurses towards alcohol and related problems: the impact of an educational intervention.. Rev Esc Enferm
Knowledge and attitudes of nurses towards alcohol and related prob- lems: the impact of an educational intervention.. Rev Esc Enferm
Thus, the study aimed to analyze the APR markers at different times of the disease, which were applied to patients of a reference center for infectious and contagious diseases
