Q U A L I T Y O F L I F E I N S Y S T E M I C L U P U S
E R Y T H E M A T O S U S P A T I E N T S I N N O R T H E A S T E R N
B R A Z I L
:
I S H E A L T H-
R E L A T E D Q U A L I T Y O F L I F E AP R E D I C T O R O F S U R V I V A L F O R T H E S E P A T I E N T S ?
Eutilia Freire,
*,****Adriana Bruscato,
**Rozana Ciconelli
***,****de pacientes com lupus eritematoso sistêmico (LES).
Métodos: Sessenta e três pacientes com
diagnósti-co de LES foram selecionados no nosso serviço mé-dico, avaliados em 1999 e revistos em 2005. Nas duas avaliações nós utilizamos um protocolo para obter dados sociais, demográficos e clínicos, índi-ces de atividade e dano e a qualidade de vida atra-vés do SF-36. Todos os testes estatísticos foram exe-cutados usando um nível de significância de 5%.
Resultados: Dos 63 pacientes examinados em 1999,
seis morreram, quatro foram perdidos o contato e o protocolo precedente foi aplicado outra vez aos 53 pacientes restantes. Os seis pacientes que mor-reram apresentaram os piores índices de qualida-de qualida-de vida, em todos os aspectos. O factor predic-tivo observado mais importante foi a baixa pon-tuação no domínio emocional do componente mental do SF-36 (p< 0.01).
Conclusão: A qualidade de vida relacionada com a
saúde pode ser usada como possível fator prediti-vo de mortalidade entre pacientes com LES.
Palavras-chaves: Lupus; Predictor; Qualidade de
Vida Relacionada a Saúde; Sobrevida; SF-36.
Introduction
Systemic lupus erythematosus (SLE) is a chronic autoimmune disease with a mortality rate 1.5 to 5
times greater than the general population.1Many
demographic predictors of survival have been iden-tified in previous studies, such as age at disease
on-set, sex, ethnicity and socioeconomic status.1
Fac-tors relating to renal disease, central nervous sys-tem disease, serositis, hemolytic anaemia and
thrombocytopenia have also been identified.1
However, there is some disagreement among pre-vious studies with regard to ethnicity and
socioe-*Department of Internal Medicine, Federal University of Paraíba (UFPB); PhD student at the Federal University of São Paulo (UNIFESP);
**Professor at IBMEC, São Paulo; PhD student at the University of São Paulo
***Assistant Professor of Rheumatology in the Federal University of São Paulo (UNIFESP)
****Pronuclear project of the Brazilian Society of Rheumatology
Abstract
Objective: To identify social, demographic and
cli-nical characteristics that influence survival of pa-tients with systemic lupus erythematosus (SLE).
Methods: Sixty-three patients with a diagnosis of
SLE were studied at our medical services in 1999 and then reviewed in 2005. We utilized a protocol to obtain demographic and clinical traits, activity and damage indices, and health-related quality of life via the SF-36. All statistical tests were performed using a significance level of 5%.
Results: Out of the 63 patients examined in 1999, six
died, four were lost for the follow-up and the previous protocol was applied to the remaining 53 patients. The six patients who died presented the worst recor-ded health-related quality of life, in all aspects. The most important observed predictor of death was a mean lower score in the Role-Emotional Domain of the mental health component of the SF-36 (p<0.01).
Conclusion: Health-related quality of life may be
used as possible predictive factor of mortality among patients with SLE.
Keywords: Lupus; Predictor; Health-related Quality
of Life; Survival; SF-36.
Resumo
Objetivo: Identificar as características sociais,
I S Q U A L I T Y O F L I F E A P R E D I C T O R F O R SLE?
conomic status.2It is now recognized that a more
comprehensive evaluation of this disease also re-quires the characterization of parameters that pa-tients themselves report, such as health-related
quality of life (QOL) as an independent variable.3-7
This topic has been quite well reported in previous studies on SLE, but this variable has not been used as a predictor for mortality due to this disease. The present study was conducted over a five-year pe-riod and evaluates QOL using the ‘Medical Outco-mes Survey Short Form 36’ questionnaire (SF-36) and also sociodemographic and clinical variables, in an attempt to identify predictors of survival for this disease.
Patients and Methods
For this observational cohort study, 63 patients seen at the rheumatology clinic of the university hospital of the Federal University of Paraíba, in the State of Paraíba, northeastern Brazil, in 1999 were included. These patients were diagnosed with SLE, using the classification criteria recommended by
the American College of Rheumatology (ACR).8
In accordance with the protocol adopted in the present study, each patient was investigated with respect to age, duration of disease, ethnicity, gen-der, income, length of schooling, clinical manifes-tations, activity, as assessed by the systemic lupus
erythematosus activity index (SLEDAI 2K)9,
irrever-sible damage, as assessed by the Systemic Lupus International Collaborative Clinics/ACR damage
index (SLICC/ACR-DI)10, and health-related QOL,
as assessed by Brazilian validated version of the SF-36.11
In 2005 these patients were again recruited. Pa-tients who did not attend our call were invited through their relatives, by letter or phone call. Their
medical files were also reviewed. Six patients had died and four had abandoned follow-up. The pa-tients’ survival was calculated as the period from the date of baseline evaluation to their death.
Statistical analysis
Pearson’s chi-square method was used to analyze associations between deaths due to SLE and the so-ciodemographic variables, ACR criteria, SLEDAI 2K, and SLICC/ACR-DI. The means for deaths due to SLE and for patients who did not die were com-pared and analyzed with regard to the SF-36 doma-ins, using the Student t and Mann-Whitney tests. All statistical tests were performed using a signifi-cance level of 5% (p<0.05).
The survival curve was analyzed using the Ka-plan-Meier method, with a 95% confidence inter-val, over the time period from June 1999 to Decem-ber 2005.
Results
The patient assessments carried out in 1999 resul-ted in a cross-sectional descriptive study of a po-pulation in northeastern Brazil, and these patients’ demographic and clinic characteristics are presen-ted in Table I. At the second assessment, in 2005, four patients were lost for follow-up, because they had changed residency. Six patients had died, two from generalized infection after the use of immu-nossupressors for SLE activity control, two from renal complications of SLE and two from nervous system complications of SLE.
On the survival curve in Figure 1 it can be seen that 89% of the patients survived for more than 79 months, e.g. 6.5 years, with a mean Kaplan-Meier survival of 73 months (95% confidence interval from 69 to 77 months). The mean SLEDAI 2K sco-re was 2.5 for the 63 patients originally examined, and ten patients presented very active disease (SLEDAI 2K > 8) at the first assessment. There was no difference between deceased and survivors (p=0.41). Twenty patients presented irreversible damage, with SLICC/ACR-DI scores ranging from 1 to 5 (mean of 1.5). The damage observed in the-se 20 patients and the respective numbers of pa-tients affected were: renal (three), ocular (four), neurological (five), pulmonary (three), cardiovas-cular (two), peripheral cardiovascardiovas-cular (three), and
Table I. Means and standard deviations (SD) of the demographic characteristics of the 63 patients with SLE at baseline evaluation
Demographic characteristics Mean (SD)
Age (years) 39.9 (15,0)
Mean income per month 300 (220)
(dollars per family of four people)
Schooling (years) 5.4 (5.2)
E U T I L I A F R E I R E , E C O L.
Mean disease duration among the patients who died was shorter, but without statistical significan-ce at the nonparametric tests (Table II).
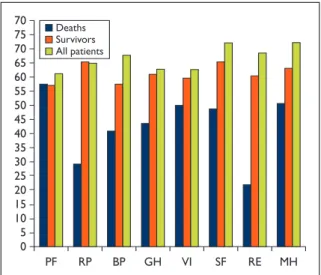
With regard to health-related QOL, the mean scores in the SF-36 domains are shown in Table II. A low level of QOL was observed for the study po-pulation at the first assessment and the six patients who died presented the worst QOL scores, in ge-neral (Figure 2). They presented significant diffe-rences regarding scores in Role-emotional (p<0.01), general health (p=0.05) and Role-physi-cal (p=0.03) domains and had worse mental-health summary component scores (p<0.001) in compa-rison with the survivors (Table II).
Discussion
In our previous study, we reported that SLE pa-tients in northeastern Brazil presented lower QOL
than did the general population.12However, no
re-lationship with patients’ activities or any other cli-nical aspect of the disease was established in that study, although there was a significant correlation with disease duration and chronic damage, which
yielded worse QOL scores.12In the present study,
the same patients were reevaluated five years later chronic alopecia and tissue loss in the face (one).
Three of these 20 patients presented damage at more than one organ system. The patients who died had renal, neuropsychiatric, pulmonary and cutaneous damage and yielded higher mean SLICC/ACR-DI scores than survivors at baseline measurement (p=0.07). .00 010 Time (months) Cum sur vival Survival Funcion 1.00 .60 .80 .40 .20 20 30 40 50 60 70 80 Censored Survival function
Figure 1. Kaplan-Meier estimated survival curve for 63
patients with SLE.
Table II. Means and standard deviations (SD) of patients' characteristics and p-values from the Student t and Mann-Whitney tests at second evaluation.
Mean (SD)
Patients Patients
All patients who survived who died Student t test Mann-Whitney
Characteristics n=63 n=53 n=6 p-value p-value
Disease duration 6.8 (6.2) 6.9 (7.0) 4.0 (1.4) 0.01 0.61 SLEDAI 2Ka 2.5 (2.9) 2.6 (3.1) 1.4 (1.9) 0.31 0.41 SLICC/ACR-DIb 1.5 (4) 1.0 (2) 2.5 (2) 0.05 0.07 PFc 59 (27) 59 (28) 60 (20) 0.94 0.91 RPd 60 (38) 64 (36) 29 (42) 0.02 0.03 BPe 61 (25) 63 (24) 50 (32) 0.22 0.26 GHf 59 (21) 60 (21) 45 (13) 0.02 0.05 VIg 61 (23) 62 (24) 49 (19) 0.14 0.10 SFh 67 (27) 69 (27) 50 (18) 0.03 0.06 REi 59 (37) 64 (35) 19 (18) < 0.01 < 0.01 MHj 66 (25) 68 (25) 51 (19) 0.06 0.049 PHSk 41.4 41.9 39.6 0.53 0.48 MHSl 48.4 46.8 35.6 0.001 0.001
aSLEDAI 2K: Systemic Lupus Erythematosus Disease Activity Index,bSLICC/ACR-DI: Damage Index,cPF: Physical function,dRP- Role-physical,eBP: Bodily pain,
and, for the first time, we were able to show that the emotional aspects of patients’ QOL are related to survival at 5 years. This was mainly with regard to limitations due to emotional aspects of QOL (Role Emotion domain of SF-36), and there was a signi-ficant difference between deceased and survivors (p<0.01). This observation confirms that this para-meter is an important predictor that should be eva-luated in cases of this disease, since the survivors we reexamined did not show any difference be-tween the assessments in 1999 and 2005.
We acknowledge the fact that this was not ne-cessarily a representative, significant sample of all patients with SLE. Nonetheless, the number of pa-tients involved was representative of the daily at-tendance at our rheumatology clinic over a one--year period.
The main gain from the present work was the evaluation of health-related QOL issues among pa-tients with worse evolution who died. This was achieved by reevaluating the survivors, who gene-rally presented the same best QOL indices, same disease-related damage scores (SLICC/ACR-DI) and low SLEDAI scores, possibly reflecting a stable disease overtime. Therefore, these variables had discriminatory value for comparing survivors and deceased.
Similar studies have been carried out in relation
to cancer,13,14hypertension,15cardiac
insufficien-I S Q U A L insufficien-I T Y O F L insufficien-I F E A P R E D insufficien-I C T O R F O R SLE?
cy,16 acquired immunodeficiency syndrome
(AIDS)17and the elderly.18In these studies, the
au-thors clearly reported that patients who yielded worse scores in health-related QOL questionnaires had worse prognosis and higher mortality.
Effica-ce et al. (2006)19reported that in metastatic
colo-rectal cancer cases, a 10-point gain in score of the social function QOL domain of European Organi-zation for Research and Treatment of Cancer (EORTC) QOL Questionnaire – Core -30, would de-crease the risk of death by 9%. Jacobson et al.
(2003)17reported that, for patients with acquired
immunodeficiency syndrome (AIDS), in the physi-cal condition domain of QOL questionnaire speci-fic for patient with AIDS, each one-point gain from the baseline score would reduce the chance of death by 4% and the risks of cytomegalovirus
in-fection and treatment dropout by 2%.16Using the
SF-36 questionnaire in an investigation on
rheu-matic diseases, Singh et al. (2005)20reported that
18,464 veterans with rheumatoid arthritis yielded lower scores in the physical condition QOL doma-in and that this doma-increased their chance of hospita-lization and death.
There have not been any reports in this respect from SLE patients. However, there are many impor-tant studies dealing with health-related QOL is-sues, in which the presence of comorbidities and
damage were important predictors of mortality.21
SF-36 has also been used as a predictor of
depres-sion among such patients.18
In summary, this study presented a health-rela-ted QOL evaluation of SLE patients and, in parti-cular, it was found that the emotional aspects of QOL might provide a means of assessing patients’ prognosis and survival. However, further studies with longer observation periods and larger num-bers of patients would be highly recommendable.
Correspondence to
Eutilia Andrade Medeiros Freire Avenida Cabo Branco 3524/501 B Cabo Branco, João Pessoa – Paraíba Brazil
CEP: 58045-010 Tel: 55 8399836101
E-mail address: [email protected]
References
1. Kasitanon N, Magder LS, Petri M. Predictors of survi-val in systemic lupus erythematosus. Medicine (Bal-timore) 2006;85:147-156
2. Alarcon GS. Is rheumatoid arthritis in African des-cendants from North and South America the same?
0 30 35 40 70 70 65 60 55 75 50 45 10 15 5 20 25 PF RP BP GH VI SF RE MH Deaths Survivors All patients
Figure 2. Mean quality-of-life characteristics among SLE
patients.
PF: Physical function, RP: Role-physical, BP: Bodily pain, GH: General health,VI:Vitality, SF: Social function, RE: Role-emotional, MH: Mental health.
Semin Arthritis Rheum 2001;31:143-145
3. Panopalis P, Petri M, Manzi S et al. The systemic lu-pus erythematosus tri-nation study: longitudinal changes in physical and mental well-being. Rheuma-tology (Oxford) 2005;44:751-755
4. Fortin P R, Abrahamowicz M, Neville C et al. Impact of disease activity and cumulative damage on the he-alth of lupus patients. Lupus 1998;7:101-107
5. Gilboe IM, Kvien TK, Husby G. Disease course in systemic lupus erythematosus: changes in health sta-tus, disease activity, and organ damage after 2 years. J Rheumatol 2001;28:266-274
6. Jolly M, Utset TO. Can disease specific measures for systemic lupus erythematosus predict patients’ he-alth related quality of life? Lupus 2004;13:924-926 7. Stoll T, Kauer Y, Büchi S, Klaghofer R, Sensky T, Villiger
PM. Prediction of depression in systemic lupus erythematosus patients using SF-36 Mental Health scores. Rheumatology (Oxford) 2001;40:695-698 8. Tan EM, Cohen AS, Fries JF et al. The 1982 revised
cri-teria for the classification of systemic lupus erythe-matosus. Arthritis Rheum 1982;25:1271-1277 9. Gladman, DD, Ibanez D, Urowitz MB. Systemic lupus
erythematosus disease activity index 2000. J Rheu-matol 2002;29:288-291
10. Gladman DD, Goldsmith CH, Urowitz MB et al. The Systemic Lupus International Collaborating Cli-nics/American College of Rheumatology (SLICC/ACR) Damage Index for Systemic Lupus Erythematosus International Comparison. J Rheu-matol 2000;27:373-376
11. Ciconelli R, Ferraz M et al. Tradução par a lingua por-tuguesa e validação do questionário genérico de ava-liação de qualidade de vida SF-36 (Brasil SF-36). Rev Bras Reumatol 1999;39:143-150
12. Freire EA, Maia IO, Nepomuceno JC, Ciconelli RM . Damage index assessment and quality of life in syste-mic lupus erythematosus patients (with long-term disease) in Northeastern Brazil. Clin Rheumatol 2007;26:423-428
E U T I L I A F R E I R E , E C O L.
13. Maisey NR, Norman A, Watson M, Allen MJ, Hill ME, Cunningham D. Baseline quality of life predicts survi-val in patients with advanced colorectal cancer. Eur J Cancer 2002;38:1351-1357
14. Chau I, Norman AR, Cunningham D, Waters JS, Oates J, Ross PJ. Multivariate prognostic factor analysis in locally advanced and metastatic esophago-gastric cancer-pooled analysis from three multicenter, ran-domized, controlled trials using individual patient data. J Clin Oncol 2004;22:2395-2403.
15. Ried LD, Tueth MJ, Taylor MD, Sauer BC, Lopez LM, Pepine CJ. Depressive symptoms in coronary artery disease patients after hypertension treatment. Ann Pharmacother 2006;40:597-604
16. Rodriguez-Artalejo F, Guallar-Castillon P, Pascual CR et al. Health-related quality of life as a predictor of hospital readmission and death among patients with heart failure. Arch Intern Med 2005;165:1274-1279 17. Jacobson DL, Wu AW, Feinberg J et al. Health-related
quality of life predicts survival, cytomegalovirus dise-ase, and study retention in clinical trial participants with advanced HIV disease. J Clin Epidemiol 2003;56:874-879
18. Dorr DA, Jones SS, Burns L. Use of health-related, quality-of-life metrics to predict mortality and hospi-talizations in community-dwelling seniors. J Am Geri-atr Soc 2006;54:667-673
19. Efficace F, Bottomley A, Coens C et al. Does a patient’s self-reported health-related quality of life predict sur-vival beyond key biomedical data in advanced colo-rectal cancer? Eur J Cancer 2006;42:42-49
20. Singh JA, Nelson DB, Fink HA et al. Health-related quality of life predicts future health care utilization and mortality in veterans with self-reported physici-an-diagnosed arthritis: the veterans arthritis quality of life study. Semin Arthritis Rheum 2005;34:755-765 21. Ward M M, Pajevic S, J Dreyfuss et al. Short-term
pre-diction of mortality in patients with systemic lupus erythematosus: classification of outcomes using ran-dom forests. Arthritis Rheum 2006;55:74-80.