1. Rheumatology Department, Centro Hospitalar e Universitário de Coimbra EPE; UICISA:E, Nursing School of Coimbra
2. Department of Rheumatology & Clinical Immunology, University Medical Center, Utrecht
3. Rheumatology Department, AP-HP, Pitié Salpêtrière Hospital; Sorbonne Université, UPMC Paris 06 University, GRC-UPMC 08 4. Centre for Rheumatology & MRC Centre for Neuromuscular Diseases, University College London
5. Centre for Health and Clinical Research, Department of Nursing and Midwifery, University of the West of England
6. Rheumatology department, Leiden University Medical Centre 7. Coimbra Institute for Clinical and Biomedical Research (iCBR) – Faculty of Medicine – University of Coimbra, Portugal;
Rheumatology Department - Centro Hospitalar e Universitário de Coimbra, Portugal
all mutually exclusive, and (iv) 3v-remission (TJC28≤1, SJC28≤1, CRP≤1). Likelihood ratios will be used to de-scriptively compare whether meeting the 3v and 4v-re-mission criteria in a single visit (at 6 or 12 months) pre-dicts good outcome in the second year (1-2y). Differences in the predictive value of PGA in the defini-tion of remission will be assessed by comparing the three mutually exclusive disease states using logistic regres-sion analysis. Good outcome is defined primarily by ra-diographic damage (no deterioration in rara-diographic scores, whatever the instrument used in each trial), and secondarily by functional disability (Health Assessment Questionnaire consistently ≤0.5 and no deterioration), and their combination (“overall good outcome”). Addi-tional analyses will consider longer periods over which to (concurrently) define remission status and outcome (between 1-5y and 1-10y), different cut-offs to define good radiographic outcome (change ≤0.5, ≤3 and ≤5 in radiographic score), sustained remission and the influ-ence of treatment and other clinical factors.
Discussion: If 4v-remission and 4v-near-remission are associated with a similar probability of good outcomes, particularly regarding structural damage, the 3v-re-mission (excluding PGA) could be adopted as the tar-get for immunosuppressive therapy. Patients’ perspec-tives would remain essential, but assessed separately from disease activity, using instruments adequate to guide adjunctive therapies.
Systematic review registration: PROSPERO, CRD42 017057099.
Keywords: Rheumatoid arthritis; Outcome research; Patient global assessment; PaPatient reported outcomes; Di -sease activity; Remission; Near-remission; Radiogra phic damage; Function; Individual patient data meta-analysis.
The impact of patient global assessment in the definition
of remission as a predictor of long-term radiographic
damage in patients with rheumatoid arthritis: protocol
for an individual patient data meta-analysis
Ferreira RJO1, Welsing PMJ2, Gossec L3, Jacobs JWG2, Machado PM4, Ndosi M5, van der Heijde D6, da Silva JAP7
ACTA REUMATOL PORT. 2018;43:52-60
AbstrAct
Background: Remission is the target for management of rheumatoid arthritis (RA) and intensification of im-munosuppressive therapy is recommended for those that do not achieve this status. Patient global assessment (PGA) is the single patient reported outcome consi dered in the American College of Rheumatology/European League Against Rheumatism remission criteria, but its use as target has been questioned. The primary aim of this study is to assess whether excluding PGA from the definition of disease remission changes the association of disease remission with longterm radiographic da -mage and physical function in patients with RA. Methods: Individual patient data meta-analysis using data from randomized controlled trials of biological and targeted synthetic agents, identified through Clinical-Trials.gov and PubMed. Different remission states will be defined: (i) 4v-remission [tender (TJC28) and swollen (SJC28) 28-joint counts both≤1, C-reactive protein (CRP)≤1 (mg/dl), and PGA≤1 (0-10 scale)], (ii) 4v-near-remission (TJC28≤1, SJC28≤1, CRP≤1, and PGA>1), (iii) non-remission (TJC28>1 or SJC28>1 or CRP>1),
IntroductIon
Disease remission or low disease activity is now a rea -listic therapeutic target in patients with rheumatoid arthritis (RA)1,2. The American College of Rheumato
-logy (ACR) and the European League Against Rheuma-tism (EULAR) proposed two alternative definitions of remission3: one based in Boolean criteria and another
on the Simplified Disease Activity Index (SDAI). The Boolean-based definition requires that tender 28-joint count (TJC28), swollen 28-joint count (SJC28), C-Reacti ve Protein (CRP, in mg/dl), and patient glo bal asses sment (PGA, 0–10 scale) are all ≤1. The SDAI crite rion requires that the sum of SJC28, TJC28, PGA, CRP and physician/observer global assessment [PhGA] is ≤3.3. These definitions have been recommended for use in daily care of RA2.
PGA is the sole patient reported outcome (PRO) in-cluded in the recommended definitions of remission, having the same weight as other criteria1-3. Its inclusion
was justified because it represents the patient’s pers -pective and because it proved to discriminate between active and control intervention in clinical trials3.
How-ever, several studies4-13have shown that PGA is not
solely influenced by RA disease activity, but also by sociodemographic features, geographic area, and cultu -ral and ethnic aspects, reflecting the fact that PGA scores can be influenced by physical and psychologi-cal factors (including disease perception), comorbidi-ties and fibromyalgia, among others12.
Patients that fail only one of the four Boolean criteria have been called “near-misses”14or “nearremission” (de
-signation applied when PGA is the solely criteria >1)13.
Previous studies4,13-15demonstrated that the
propor-tion of near-remission patients could vary from 14.4% up to 38.2%13, which can represent up to four times
the proportion of patients in remission13. Following
current treatment guidelines1,2 this state of
nearremission would justify intensification of immuno -suppressive treatment if based on a shared decision between patient and rheumatologist, taking structural damage, comorbidities or contraindications into account (Overarching Principles A and B)2.
The importance of incorporating PROs in the ove -rall management plan is indisputable. However, whether PGA conveys information that should be ta -ken into account when considering changing immunosuppressive regimens in patients that have other -wise achieved a remission state based on TJC, SJC and CRP remains unclear. A recent study from our group12
showed that PGA was weakly correlated with “more” objective disease activity measures (SJC28, TJC28, CRP) but the correlations were strong with pain, fatigue, function, comorbidities, depression and anxie -ty, and were also significant with other dimensions such as happiness and personality dimensions (weak correlations). Furthermore, it was shown that PGA cor-relations differ according to disease activity state, with pain, function and joint counts having stronger corre-lation with PGA when patients are in non-remission.
Immunosuppressive therapy, including biologic di -sease modifying antirheumatic drugs (bDMARDs), has been shown to improve PGA as disease activity evolves towards remission. However, in cases where PGA is being mainly driven by factors not related to RA, immu nosuppressive therapy may not be able to lower PGA ≤1, despite SCJ28, TJC28 and CRP scores ≤1 hav-ing already been achieved. From this stage onwards, PGA is not dependent on disease activity and the in-ability to improve it further should not be interpreted as a failure of the immunosuppressive therapy.
Progression of joint damage is one of the most im-portant outcome measures in RA, because it reflects historic disease activity, is associated with decline of physical function over time, and can be reliably asses -sed16. A recent systematic literature review (SLR)17
inves tigated the clinical predictors of radiographic pro-gression in RA, including disease activity indices and their individual components. Regarding the individual components, only SJC and acute phase reactants were associated with radiographic progression. Regarding PGA, the authors concluded that “published data for GH [patient’s general health], PGA and EGA [evalua-tor’s global assessment] are limited and do not support their use as unique tools related to progression of joint damage”17. The data analysed included two rando
-mized controlled trials (RCTs) and two prospective co-horts, with 1 to 3 years of follow-up, including pa-tients receiving conventional synthetic (cs)DMARDS. However, radiographic progression may be different in patients receiving bDMARDs. A subsequent obser-vational study18with 527 patients with early RA,
follow ed for 8 years, demonstrated that 31% of pa-tients reaching remission according to the ACR/EU-LAR Boolean criteria, at 1, 2, 5, and 8 years (sustained remission) had radiographic progression (>1 unit/ /year). There was no significant contribution of PGA to the prediction of radiographic progression18.
These observations suggest that the concept of “disea se remission” should not include PGA for the
necrosis factor (TNF) inhibitors; Interleukin (IL) inhi -bitors; B-cell inhi-bitors; and T-cell inhibitors] or tsDMARD [janus kinase (JAK) inhibitors] will be in-cluded. All routes of drug administration will be con-sidered. Studies testing DMARDs dose spacing or sus-pension will be excluded.
Types of assessments
As a minimum, studies will need to have assessed SJC28, TJC28, CRP, and PGA (in order to determine the Boolean-based criteria) at baseline and at 6 and 12 months and the radiographic damage assessment and physical function at baseline, 12 and 24 months.
IdEntIfyInG studIEs
Studies of interest were searched by one researcher (RF), between November and December of 2016, from the ClinicalTrials.gov registry. The following search strategy was used, without limits: “Rheumatoid arthri-tis” AND (“radiographic damage” OR “radiographic progression” OR “joint damage”). A second search was also performed in PubMed MEDLINE, for the same time-period, using also the pharmacological names of bDMARDs and tsDMARD as search terms. Additional-ly, local medical contacts of pharmaceutical companies were approached in order to identify possible pu -blished studies missed in previous searches and how to get access to their IPD. A summary table with the re-sults of this search is presented in Appendix 2.
study sElEctIon ProcEss
Full papers of the identified studies were obtained and checked against the inclusion criteria by two re-searchers (RF and JAPS) independently.
dAtA collEctIon ProcEssEs
Not all published studies have IPD available, which can be the case if patients did not give permission for broa -der research than the original study. The timing of data availability after study publication may also vary accor -ding to data holder policy22: while some companies
make the data available immediately after the first pu -blication, others only do it after the investigational product has been approved for use in both the United States and European Union. Thus, after study selection (Appendix 2) a research proposal was submitted to all sponsors of those trials, asking for IPD access.
dAtA ItEMs
In addition to the radiographic damage score and purposes of guiding immunosuppressive therapy. Such
a definition of remission, i.e. excluding PGA from ACR/ /EULAR Boolean definition, might be designated as “re-mission 3 variables” or “3v-re“re-mission”. Long-term lon-gitudinal studies, looking at more objective outcomes are required to support this change in the definition of remission.
The primary aim of this study is to assess whether excluding PGA from the definition of disease remission changes the association of disease remission with long-term radiographic damage and physical function in pa-tients with RA.
MEtHods/dEsIGn
This is an individual patient data (IPD) meta-analysis of published RCTs selected from a systematic literature search.
Protocol And rEGIstrAtIon
This study protocol was registered in PROSPERO with the number CRD4201705709919. The results will be
reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses of Individual Participant Data (PRISMA-IPD), and this checklist (Appendix 1) also served as guidance for writing this protocol.
Ethical approval to this study was granted by the Centro Hospitalar e Universitário de Coimbra Ethics Committee (CHUC-047-17).
ElIGIbIlIty crItErIA Type of studies
This study will include recently published RCTs, and their long-term extensions (≥ 2 years), which evaluate the efficacy of csDMARDs, bDMARDs or targeted syn-thetic (ts) DMARD on radiographic damage in patients with RA.
All RCTs assessing radiographic damage assess also physical function as a secondary outcome. Studies with less than two years of follow-up will be excluded. Participants
Both men and women with diagnosis of RA, and ful-filling the 1987 ACR criteria or the 2010 ACR-EULAR criteria for RA20,21, will be included.
Types of interventions
physi cal function (outcomes), and to SJC28, TJC28, CRP, and PGA (for remission definition) the following varia bles will be extracted from the trials: (i) patient characteristics – gender, age at baseline; (ii) clinical characteristics – disease duration at baseline, rheuma-toid factor (RF) status, anti-citrullinated peptide antibo dy (ACPA) status, and treatment arm (iii) trial/vi -sit information variables, namely anonymised patient identification (ID) code, visit number or sequence, and visit date. Appen dix 3 provides a list off all essential variables that will be extracted from each trial.
IPd IntEGrIty
Any important issues identified when checking IPD, such as data plausibility, consistency, completeness or baseline imbalance will be reported and summarised using a PRISMA-IPD flow diagram.
rIsk of bIAs AssEssMEnt of IndIvIduAl studIEs
The quality and potential bias of included studies will be assessed using the guidelines for assessing quality in prognostic studies, assigning an overall quality score per study of between 0 and 6 points according to Hay-den et al.23The six topics assessed are: study
participa-tion, study attriparticipa-tion, prognostic factor measurement, outcome measurement, confounding measurement and account, and analysis. Of particular relevance for this study will be the assessment of radiographic dama -ge. A list of ten possible biases in the assessment of ra-diographic data was described by van der Heijde24and
this information will be collected separately for quali-ty assessment of the radiographic outcome, but will not be used as the basis for including/excluding studies.
sPEcIfIcAtIon of outcoMEs And EffEct MEAsurEs
For the purposes of this study the methodology adopt-ed by the ACR/EULAR group3to define good outcome
in radiographic damage and function (separately and combined) will be adopted. Using the same definitions will allow direct comparisons of the results/conclusion. However, in the present study different definitions of “good radiographic outcome” will be evaluated (for more details please see “Exploration in variation effects (sensitivity analyses)” section).
Primary outcome:
a) Percentage of individuals with a good radiographic outcome during the second year of the trial (i.e.
be-tween month 12 and month 24).
“Good radiographic outcome” is defined as stable radiographic scores (change ≤0 in Sharp25or modified
Sharp scores26-28during the second year of the trial).
Secondary outcomes:
b) Percentage of individuals with a good functional out-come during the second year of the trial.
“Good physical function outcome” is defined as sta-ble and low scores of Health Assessment Questionnaire (HAQ)29(change ≤0 and HAQ score consistently ≤0.5
during the second year of the trial).
c) Percentage of individuals with overall good outcome during the second year of the trial.
“Overall good outcome”is considered the combi-nation of “good radiographic outcome” and “good physical function outcome”.
Additional secondary outcomes:
The above-mentioned outcomes assessed the stabili ty between 1 and 2 years. Additional secondary outcomes will assess stability between 1 and 5 years and between 1 and 10 years after baseline for a), b) and c), in trials with such long follow-up.
Measures of association:
The principal effect measure for all outcomes will be the positive (LR+) and negative likelihood ratios (LR-).
coMPArIsons: dEfInItIons of rEMIssIon
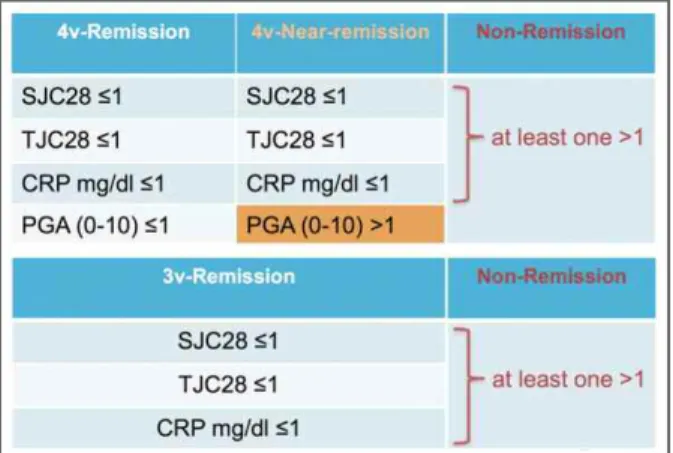
Analyses will be based on the definition of different re-mission states (Figure 1), assessed at 6 months and 12 months, following the methodology adopted by the ACR/EULAR committee3, as follows:
a) ACR/EULAR Boolean-based remission3, also
de-signed in this project as “4v-Remission” (i.e., TJC28≤1, SJC28≤1, CRP mg/dl ≤1, and PGA≤1/10) b) “4v-near-remission”13,14, defined as TJC28≤1,
SJC28≤1, CRP mg/dl ≤1, and PGA>1.
c) “Non-remission” defined as TJC28>1 or SJC28>1 or CRP mg/dl >1.
The above three definitions are mutually exclusive, i.e. each patient will be categorized in one group only. d) “3v-remission” defined as TJC28≤1, SJC28≤1, CRP
mg/dl ≤1.
All remission definitions are considered to be satis-fied when they are satissatis-fied either at 6 or 12 months follow-up.
The LR for good outcome associated with 4v and 3v--remission states will be descriptively compared. Then,
e.g. when they satisfy both the remission and 4v--near-remission definitions at two consecutive visits, or have both a ConRew score >25thpercentile based on
4v-remission and 4v-near remission, they are assigned to the 4v-remission category.
dAtA AnAlysIs And syntHEsIs Data analysis
To guarantee privacy and security of IPD, the platforms in which the data is available require that statistics be performed via remote and secure online platforms, which impedes data download. All platforms com-monly allow the use of SAS software, which will be used within each platform. For data synthesis, Stata software version 14 will be used. Thus, the same pro-cedures will need to be performed in each platform.
Means and standard deviations (SD) will be used to describe normally distributed continuous data, medians and interquartile ranges to describe continuous data that are not normally distributed, and frequencies and percentages will be used for categorical data. Data will be described using 95% confidence intervals (95% CI).
The number of true positive (TP), true negative (TN), false negative (FN) and false positive (FP) statis-tics will be extracted for each dataset. Then, sensitivi-ty, specificisensitivi-ty, positive and negative predictive value (PPV and NPV) will be determined for being in (sus-tained) remission (by 3v and 4v-remission) to predict good radiographic outcome at 2-years after baseline. The LR+ and LR- will then be calculated by the for-mulas: sensitivity/(1-specificity) and (1sensitivity)/specificity, respectively. All analyses will be repeated for se -condary outcomes: good function, and overall good outcome.
LRs, calculated as above, will be descriptively com-pared. In a second phase, participants in non-remission will be excluded from analyses and LRs for good radio-graphic outcome will be calculated for “4v-remission” versus “4v-near-remission”, as a means to assess the pre-dictive impact of PGA (Appendix 4, image C).
To additionally test the predictive value of PGA in the definition of remission, logistic regression will be used with the outcome of interest - radiographic sta-bility - as dependent variable. The independent vari-ables will include remission (a categorical variable in-dicating whether a patient is in “4v-remission”, “4v-near-remission”, or not satisfying any of these def-initions, i.e. “non-remission”) (Appendix 4, images D and E). The regression coefficient/odds ratio (OR) (and 95% CI) comparing the “4v-near-remission” category an analysis will be performed for evaluating the (lack
of) additional predictive value of PGA in the definition of remission, using the mutually exclusive categories (“4vremission”, “4vnearremission” and “nonre -mission”) (for more details please see “data analyses” section and Appendix 4).
dEfInItIons of sustAInEd rEMIssIon
Sensitivity analyses will assess the influence of sus-tained remission, i.e. remission in more than a single time-point (6 or 12 months), in the prediction of good outcomes in RA. Because there is no currently uniform definition of sustained remission, the following will be tested: (i) remission at 6 and 12 months, (ii) remission at two consecutive visits among all time-points consis-tently available during the first year in all trials, ideal-ly separated by 3 months (i.e. 3, 6, 9, and 12 months), as suggested by Konijn et al.30, (iii) having or not ≥50%
of visits in remission, and (iv) using the “Continuity Reward” (ConRew) score proposed by Boers et al.31,
which gives 1 point for a period in remission and a bonus (1 point more) if the subsequent period is also remission or if it is the last observation period. Because ConRew is a continuous score and the distributions are expected to be strongly right skewed31, the 25th
per-centile will be considered as cut-off to dichotomize sus-tained versus non-sussus-tained remission. Definitions (iii) and (iv) will consider the visits from the beginning to the end of the follow-up under consideration, i.e. not only the first year of the trial and patients will be clas-sified to the ‘highest category’ for definitions ii and iv,
fIGurE 1. Definitions of Boolean remission considered for this study, adapted from the ACR/EULAR Boolean definition CRP: C-reactive protein, PGA: patient global assessment; SJC28: swollen 28-joint counts; TJC28: tender 28-joint counts
with the “4v-remission” category will indicate whether there is any relevant difference between these groups and, thus, whether PGA has any additional predictive value for outcome.
Missing data will not be submitted to any method of data imputation, based on the comparable results of imputed and nonimimputed data shown by a similar analy -sis30. The number and percentage of patients with
miss-ing values for each variable will be reported per trial. Measures to adjust for confounders
In order to adjust for important covariates (gender, age at baseline, disease duration at baseline, RF, ACPA, ra-diographic damage at baseline, treatment arm), logistic regression (as above) will be used in individual studies. Data synthesis
A two-step approach will be followed in this IPD meta--analysis. Thus, the TP, TN, FN, and FP results obtained for each trial in a first step (described above) will be used to synthetize the data in a second step. To consider the results from the mutually exclusive definitions of re-mission and to take into account the influence of the covariates, the OR and its standard error (SE) resulting from the logistic regression will also be synthesized, using appropriate fixed-effect and random-effects approa ches, as suggested by Chang and Hoaglin32.
As the definitions of remission will be the same over all studies as well as the definition of the outcome (as they are calculated by the authors), a Bivariate hierar-chical model with random effect will be used to sum-marize the diagnostic association measure33.
The I2of Higgins and Thompson will be calculated
to quantify heterogeneity34,35.
ExPlorAtIon In vArIAtIon EffEcts (sEnsItIvIty AnAlysEs)
In recent years a statistically significant reduction in ra-diographic progression during clinical studies in pa-tients with RA has become difficult to detect due to ear-ly-escape study designs and to declining rates of progression in control-group patients36. For this
rea-son, and also to be consistent with the methodology used by ACR and EULAR to establish the current defi -nition of remission, a strict defi-nition of good outcome was adopted for this study, i.e, a change ≤0 in radiogra phic progression. However, the majority of recent stu -dies consider a cut-off ≤0.5 to define radiographic sta-bility, to allow for a maximum change of 1 unit by one of the two readers. Therefore, a sensitivity analysis will
consider change ≤0.5 units as cut-off for radiographic da mage progression. Also, in order to account for in-ter and intra-rain-ter variation of the radiographic score30,37,38 and to provide information on the
magni-tude of structural damage, two additional cut-offs to define good radiographic outcome will be considered: ≤3 and ≤5 units of the radiographic score. It is also ar-gued that the number of years of follow-up could affect the results of radiographic outcomes18. Thus, in
addi-tion to the main analysis of the 2-year outcome (the most frequently reported), outcomes at 5 and 10 years after baseline will also be assessed, i.e, 4 and 9 years’ stabili ty after 12 months.
The definition of “sustained” remission (and non--remission) based on only 1 time point or even 2 con-secutive time points may not fully capture all relevant information31. Thus we will explore whether multiple
remission and relapse periods are related to long-term radiographic progression and compare the perfor-mance of 3v and 4v-remission definitions, namely using the ConRew score31, as explained above.
We will, finally, evaluate whether the relationship between the definition of remission and outcome is af-fected by treatment (mono versus combined), disease duration (early versus established), and history of previous DMARD treatments (naive versus failure/nonres -ponders).
dIscussIon
This study will evaluate whether the predictive value of 3v and 4v-remission states regarding the development of structural damage are comparable. If confirmed, the inclusion of PGA in the definition of remission as treat-ment target should be revised (to 3v-remission), thus helping to avoid unnecessary immunosuppressive treatment escalation and associated risks. Given that more patients attain 3v than 4v-remission, it is expected that the value (long term benefit) of available the -rapies will be reassessed and probably recognized as higher than previously acknowledged.
If no relevant difference is observed by including or excluding PGA from the definition, the proposal to-wards the adoption of two separate targets for the treat-ment of RA (control of the disease process and control of its impact upon the patient’s life) will be strongly supported. Disease impact will continue to be core to the assessment and management of the disea se but it will be better served by instruments that allow the
health professionals to understand the reasons dri ving a high-perceived impact of the disease. Once di sease control is achieved, adjunctive pharmacological and non-pharmacological therapies of different nature may be considered, based on the understanding of disea se impact in the individual patient12,13.
In case the results demonstrate that including PGA in the ACR/EULAR Boolean-based definition increases its predictive value of good outcomes, the current defi -nition of remission is supported. This would not in-validate the need to consider a separate patient impact target39,40. We would argue, in any case, following
availa ble evidence, that the formulation of PGA should be standardized41,42and that patients should have a
dedicated debriefing about this measure in order to im-prove its reliability43.
An IPD meta-analysis is adequate for this study be-cause it allows calculating a new definition of remission in RA: the 3vremission, which includes the same varia -bles used to assess remission by current definitions. Be-ing “new”, this definition has never been published, thus not accessible through a conventional meta-analy sis.
This type of meta-analysis has many advantages but also some limitations44-46. The main advantages of this
specific study include access: (i) to large datasets of pa-tients, (ii) with long-term outcome assessment, and (iii) rigorous data collection. The potential limitations are mainly related with the different designs of the RCTs in-cluded, namely: different inclusion criteria (e.g. pa-tients naive versus non-responders to MTX), different treatments (e.g. patient in mono versus combined DMARD therapy), different time point assessments within the same period, or variation in radiographic scoring. To face these limitations different sub-group and sensitivity analyses are planned, that will allow guaranteeing the rigor and generalizability of the re-sults. The inclusion of highly experienced experts in radiographic outcome assessment and in RCT design, development, and statistical analyses in this interna-tional consortium of researchers will also contribute to overcome possible difficulties. All the authors will be engaged in close critical appraisal in every step of the analyses to ensure the validity of the results and con-clusions of this study. To guarantee quality control and reproducibility of the procedures the analysis’s syntax will be recorded.
Two important decisions that were taken during study design are important to highlight. The first deci-sion was regarding the number of studies to include. Usually, turning large amounts of data into actionable
information allows better contributions in epidemiolo -gy47. The authors agreed that there was no need to
in-clude all existing RCTs testing biological and targeted synthetic agents, but including data from different data--holders would strengthen this study. The second de-cision was related with the fact that this study is ques-tioning the current ACR/EULAR Boolean-based definition of remission and how strictly should this study reproduce their methodological decisions. It was decided to reproduce their analysis but performing fur-ther sensitivity analysis using ofur-ther methodological options. An example was the additional cut-off for the definition of good radiographic outcomes. Another example was the definition of sustained remission: al-though ACR/EULAR committee3have used a single
point in time (6 or 12 months) to define remission and despite the nonexistence of a uniform definition of sustai ned remission30, this study will also use four addi
-tional definitions.
The present study considers radiographic score as primary endpoints and function (HAQ) and overall out-comes as secondary endpoints. This decision was based on the fact that HAQ: (i) is not only an outcome mea-sure (cumulative functional deterioration over time) but also a disease activity-related measure (impact of current disease activity on function a specific point in time)48,
and (ii) is subjective49,50, i.e. does not measure
func-tioning of patients, but assesses their opinion on their functioning. So, the factors underlying an unjustifiably high PGA would be expected to have a similar effect upon HAQ, confounding the argument.
At the time of submission of this manuscript, all the five pharmaceutical companies (MSD/JANSSEN, Pfi -zer, Abbvie, Roche and UCB) contacted had already granted us access to their RCTs, which demonstrates the perceived value of this research project. These posi -tive answers also assure that structural damage and functional outcomes after 5 and 10-years of DMARD initiation will also be possible to be compared.
AcknowlEdGMEnts
We wish to thank Cátia Duarte and Eduardo Santos (Centro Hos-pitalar e Universitário de Coimbra, Coimbra, Portugal) for critical-ly revising the manuscripts for its intellectual content.
corrEsPondEncE to
José António Pereira da Silva
Centro Hospitalar Universitário de Coimbra, EPE. Serviço de Reumatologia, Piso 7.
Praceta Professor Mota Pinto 3000-075 Coimbra. Portugal E-mail: [email protected]
alistic outcome measure in clinical trials with early inflamma-tory arthritis? Clin Exp Rheumatol 2003; 21: S37-41. 17. Navarro-Compan V, Gherghe AM, Smolen JS, Aletaha D,
Lan-dewe R, van der Heijde D. Relationship between disease acti vity indices and their individual components and radiographic pro-gression in RA: a systematic literature review. Rheumatology (Oxford) 2015; 54: 994-1007.
18. Svensson B, Andersson ML, Bala SV, Forslind K, Hafstrom I. Long-term sustained remission in a cohort study of patients with rheumatoid arthritis: choice of remission criteria. BMJ open 2013; 3: e003554.
19. Ferreira RJO, Machado PM, Gossec L, et al. Long-term predic-tive value of including patient global assessment in Boolean re-mission regarding radiographic damage and physical function in patients with rheumatoid arthritis: protocol for an individu-al patient data meta-anindividu-alysis PROSPERO2017 http://www. crd.york.ac.uk/PROSPERO/display_record.php?ID=CRD42017 057099. Accessed in October 25th 2017.
20. Arnett FC, Edworthy SM, Bloch DA, et al. The American Rheumatism Association 1987 revised criteria for the classifi-cation of rheumatoid arthritis. Arthritis Rheum 1988; 31: 315--324.
21. Aletaha D, Neogi T, Silman AJ, et al. 2010 rheumatoid arthritis classification criteria: an American College of Rheumatolo-gy/European League Against Rheumatism collaborative initia-tive. Ann Rheum Dis 2010; 69: 1580-1588.
22. Committee on Strategies for Responsible Sharing of Clinical Tri-al; Data Board on Health Sciences Policy; Institute of Medicine. Discussion Framework for Clinical Trial Data Sharing: Guiding Principles, Elements, and Activities. Washington (DC): National Academies Press (US); 2014.
23. Hayden JA, Cote P, Bombardier C. Evaluation of the quality of prognosis studies in systematic reviews. Ann Intern Med 2006; 144: 427-437.
24. van der Heijde D. Structural damage in rheumatoid arthritis as visualized through radiographs. Arthritis Res 2002; 4 Suppl 2: S29-33.
25. Sharp JT, Lidsky MD, Collins LC, Moreland J. Methods of scor-ing the progression of radiologic changes in rheumatoid arthritis. Correlation of radiologic, clinical and laboratory abnormali -ties. Arthritis Rheum 1971; 14: 706-720.
26. Ory PA. Interpreting radiographic data in rheumatoid arthritis. Ann Rheum Dis 2003; 62: 597-604.
27. van der Heijde D. How to read radiographs according to the Sharp/van der Heijde method. J Rheumatol 2000; 27: 261-263. 28. van der Heijde DM, van Riel PL, Nuver-Zwart IH, Gribnau FW, vad de Putte LB. Effects of hydroxychloroquine and sul-phasalazine on progression of joint damage in rheumatoid arthritis. Lancet 1989; 1: 1036-1038.
29. Fries JF, Spitz P, Kraines RG, Holman HR. Measurement of pa-tient outcome in arthritis. Arthritis Rheum 1980; 23: 137-145. 30. Konijn NPC, van Tuyl LHD, Boers M, et al. Do Short and Sus-tained Periods of American College of Rheumatology/European League Against Rheumatism Remission Predict Functional and Radiographic Outcome in Early Rheumatoid Arthritis Patients With Low Overall Damage Progression? Arthritis Care Res (Hoboken) 2017; 69: 989-996.
31. Boers M, Berkhof J, Twisk JW, et al. A new graph and scoring sys-tem simplified analysis of changing states: disease remissions in a rheumatoid arthritis clinical trial. J Clin Epidemiol 2010; 63: 633-637.
rEfErEncEs
1. Smolen JS, Breedveld FC, Burmester GR, et al. Treating rheuma-toid arthritis to target: 2014 update of the recommendations of an international task force. Ann Rheum Dis 2015; 75: 3-15. 2. Smolen JS, Landewe R, Bijlsma J, et al. EULAR
recommenda-tions for the management of rheumatoid arthritis with syntheti c and biological disease-modifying antirheumatic drugs: 2016 update. Ann Rheum Dis 2017; 76: 960-977.
3. Felson DT, Smolen JS, Wells G, et al. American College of Rheumatology/European League Against Rheumatism provi-sional definition of remission in rheumatoid arthritis for clini-cal trials. Arthritis Rheum 2011; 63: 573-586.
4. Vermeer M, Kuper HH, van der Bijl AE, et al. The provisional ACR/EULAR definition of remission in RA: a comment on the patient global assessment criterion. Rheumatology (Oxford) 2012; 51: 1076-1080.
5. Khan NA, Spencer HJ, Abda E, et al. Determinants of discor-dance in patients’ and physicians’ rating of rheumatoid arthri-tis disease activity. Arthriarthri-tis Care Res (Hoboken) 2012; 64: 206--214.
6. Ward MM, Guthrie LC, Alba MI. Measures of arthritis activity associated with patient-reported improvement in rheumatoid arthritis when assessed prospectively versus retrospectively. Arthritis Care Res (Hoboken) 2015; 67: 776-781.
7. Egsmose EL, Madsen OR. Interplay between patient global assessment, pain, and fatigue and influence of other clinical di sease activity measures in patients with active rheumatoid arthri-tis. Clin Rheumatol 2015; 34: 1187-1194.
8. Sokka T, Kautiainen H, Pincus T, et al. Disparities in rheumatoid arthritis disease activity according to gross domestic pro -duct in 25 countries in the QUEST-RA database. Ann Rheum Dis 2009; 68: 1666-1672.
9. Masri KR, Shaver TS, Shahouri SH, et al. Validity and reliabili-ty problems with patient global as a component of the ACR/EU-LAR remission criteria as used in clinical practice. J Rheumatol 2012; 39: 1139-1145.
10. Studenic P, Radner H, Smolen JS, Aletaha D. Discrepancies be-tween patients and physicians in their perceptions of rheuma-toid arthritis disease activity. Arthritis Rheum 2012; 64: 2814--2823.
11. Inanc N, Yilmaz-Oner S, Can M, Sokka T, Direskeneli H. The role of depression, anxiety, fatigue, and fibromyalgia on the eva -luation of the remission status in patients with rheumatoid arthritis. J Rheumatol 2014; 41: 1755-1760.
12. Ferreira RJO, Duarte C, Ndosi M, de Wit M, Gossec L, da Silva JAP. Suppressing inflammation in rheumatoid arthritis: Does patient global assessment blur the target? A practice–based 2018; 70(3):369-378.
13. Ferreira RJO, Dougados M, Kirwan J, et al. Drivers of patient global assessment in patients with rheumatoid arthritis who are close to remission: an analysis of 1588 patients. Rheumatology (Oxford) 2017; 56: 1573-1578.
14. Studenic P, Smolen JS, Aletaha D. Near misses of ACR/EULAR criteria for remission: effects of patient global assessment in Boolean and index-based definitions. Ann Rheum Dis 2012; 71: 1702-1705.
15. Balogh E, Dias JM, Orr C, et al. Comparison of remission crite-ria in a tumour necrosis factor inhibitor treated rheumatoid arthritis longitudinal cohort: patient global health is a con-founder. Arthritis Res Ther 2013; 15: R221.
re-32. Chang BH, Hoaglin DC. Meta-Analysis of Odds Ratios: Current Good Practices. Med Care 2017; 55: 328-335.
33. Macaskill P, Gatsonis C, Deeks JJ, Harbord RM, Takwoingi Y. Chapter 10 Analysing and Presenting Results. In: Deeks JJ, Bossuyt PM, Gatsonis C, editors. Cochrane Handbook for Sys-tematic Reviews of Diagnostic Test Accuracy Version 10: The Cochrane Collaboration, 2010. http://srdta.cochrane.org/ Ac-cessed in October 25th 2017.
34. Moayyedi P. Meta-analysis: Can we mix apples and oranges? Am J Gastroenterol 2004; 99: 2297-2301.
35. Higgins JP, Thompson SG. Quantifying heterogeneity in a meta--analysis. Stat Med 2002; 21: 1539-1558.
36. Landewe RB, Connell CA, Bradley JD, et al. Is radiographic pro-gression in modern rheumatoid arthritis trials still a robust out-come? Experience from tofacitinib clinical trials. Arthritis Res Ther 2016; 18: 212.
37. van der Heijde D, Tanaka Y, Fleischmann R, et al. Tofacitinib (CP-690,550) in patients with rheumatoid arthritis receiving methotrexate: twelve-month data from a twenty-four-month phase III randomized radiographic study. Arthritis Rheum 2013; 65: 559-570.
38. Fleischmann RM, Huizinga TW, Kavanaugh AF, et al. Efficacy of tofacitinib monotherapy in methotrexate-naive patients with early or established rheumatoid arthritis. RMD open 2016; 2: e000262.
39. van Tuyl LHD, Boers M. Rheumatoid arthritis: Remission - keep-ing the patient experience front and centre. Nat Rev Rheuma-tol 2017; 13: 573-574.
40. Ferreira RJO, Duarte C, Ndosi M, de Wit M, Gossec L, da Silva JAP. The controversy of using PGA to define remission in RA. Nat Rev Rheumatol 2018; 14: 245.
41. Nikiphorou E, Radner H, Chatzidionysiou K, et al. Patient glo -bal assessment in measuring disease activity in rheumatoid arthritis: a review of the literature. Arthritis Res Ther 2016; 18: 251.
42. Ferreira RJO, Eugenio G, Ndosi M, Silva C, Medeiros C, Duarte C, da Silva JAP. Influence of the different "patient global assess-ment" formulations on disease activity score by different indices in rheumatoid arthritis. Clin Rheumatol. Online First: 10 March 2018. doi:10.1007/s10067-018-4063-9
43. Henriques M, Duarte C, Ndosi M, Marques A, Silva da Silva JAP, Ferreira RJO. “It can’t be zero”: a qualitative study of patients’ perspective on patient global assessment in rheumatoid arthri-tis [abstract]. Ann Rheum Dis 2017; 76(Suppl 2): 112-112. 44. Riley RD, Lambert PC, Abo-Zaid G. Meta-analysis of indivi dual
participant data: rationale, conduct, and reporting. BMJ 2010; 340: c221.
45. Stewart LA, Tierney JF. To IPD or not to IPD? Advantages and disadvantages of systematic reviews using individual patient data. Eval Health Prof 2002; 25: 76-97.
46. Stewart LA, Tierney JF. Reviews of individual patient data. 2011. In: Cochrane Handbook for Systematic Reviews of Interven-tions. Chichester: John Wiley & Sons Ltd.
47. European Commission. Directorate-General for Health and Consumers. Unit D3 eHealth and Health Technology Assess-ment. The Use of Big Data in Public Health Policy and Research: Background information document. Brussels, 2014.
48. Welsing PM, van Gestel AM, Swinkels HL, Kiemeney LA, van Riel PL. The relationship between disease activity, joint des -truction, and functional capacity over the course of rheumatoid arthritis. Arthritis Rheum 2001; 44: 2009-2017.
49. Wolfe F. A reappraisal of HAQ disability in rheumatoid arthri-tis. Arthritis Rheum 2000; 43: 2751-2761.
50. van den Ende CH, Hazes JM, Le Cessie S, Breedveld FC, Dijk-mans BA. Discordance between objective and subjective as-sessment of functional ability of patients with rheumatoid arthri-tis. Br J Rheumatol 1995; 34: 951-955.
APPEndIx 1. systEMAtIc rEvIEws And MEtA-AnAlysEs of IndIvIduAl PArtIcIPAnt dAtA (PrIsMA-IPd) P r Is M A -I P d c H Ec k lI st o f It EM s to In cl u d E w H En r EP o r tI n G A s y st EM A tI c r Ev IE w A n d M Et A -A n A ly sI s o f In d Iv Id u A l P A r tI cI P A n t d A tA ( IP d ) P R IS M A -I P D It em R ep o rt ed S ec ti o n /t o p ic N o C h ec k li st i te m o n p ag e T it le T it le 1 Id en ti fy t h e re p o rt a s a sy st em at ic r ev ie w a n d m et a-an al y si s o f in d iv id u al p ar ti ci p an t d at a. A b st ra ct S tr u ct u re d 2 P ro v id e a st ru ct u re d s u m m ar y i n cl u d in g a s ap p li ca b le : su m m ar y B ac k g ro u n d : st at e re se ar ch q u es ti o n a n d m ai n o b je ct iv es , w it h i n fo rm at io n o n p ar ti ci p an ts , in te rv en ti o n s, co m p ar at o rs a n d o u tc o m es . M et h o d s: r ep o rt e li g ib il it y c ri te ri a; d at a so u rc es i n cl u d in g d at es o f la st b ib li o g ra p h ic s ea rc h o r el ic it at io n , n o ti n g th at I P D w er e so u g h t; m et h o d s o f as se ss in g r is k o f b ia s. R es u lt s: p ro v id e n u m b er a n d t y p e o f st u d ie s an d p ar ti ci p an ts i d en ti fi ed a n d n u m b er ( % ) o b ta in ed ; su m m ar y e ff ec t es ti m at es f o r m ai n o u tc o m es ( b en ef it s an d h ar m s) w it h c o n fi d en ce i n te rv al s an d m ea su re s o f st at is ti ca l h et er o g en ei ty . D es cr ib e th e d ir ec ti o n a n d s iz e o f su m m ar y e ff ec ts i n t er m s m ea n in g fu l to t h o se w h o w o u ld p u t fi n d in g s in to p ra ct ic e. D is cu ss io n : st at e m ai n s tr en g th s an d l im it at io n s o f th e ev id en ce , g en er al i n te rp re ta ti o n o f th e re su lt s an d a n y im p o rt an t im p li ca ti o n s. O th er : re p o rt p ri m ar y f u n d in g s o u rc e, r eg is tr at io n n u m b er a n d r eg is tr y n am e fo r th e sy st em at ic r ev ie w a n d I P D m et a-an al y si s. In tr o d u ct io n R at io n al e 3 D es cr ib e th e ra ti o n al e fo r th e re v ie w i n t h e co n te x t o f w h at i s al re ad y k n o w n . O b je ct iv es 4 P ro v id e an e x p li ci t st at em en t o f th e q u es ti o n s b ei n g a d d re ss ed w it h r ef er en ce , as a p p li ca b le , to p ar ti ci p an ts , in te rv en ti o n s, c o m p ar is o n s, o u tc o m es a n d s tu d y d es ig n ( P IC O S ). I n cl u d e an y h y p o th es es t h at r el at e to p ar ti cu la r ty p es o f p ar ti ci p an t-le v el s u b g ro u p s. M et h o d s P ro to co l an d 5 In d ic at e if a p ro to co l ex is ts a n d w h er e it c an b e ac ce ss ed . I f av ai la b le , p ro v id e re g is tr at io n i n fo rm at io n i n cl u d in g re g is tr at io n re g is tr at io n n u m b er a n d r eg is tr y n am e. P ro v id e p u b li ca ti o n d et ai ls , if a p p li ca b le . E li g ib il it y 6 Sp ec if y i n cl u si o n a n d e x cl u si o n c ri te ri a in cl u d in g t h o se r el at in g t o p ar ti ci p an ts , in te rv en ti o n s, c o m p ar is o n s, o u tc o m es , cr it er ia st u d y d es ig n a n d c h ar ac te ri st ic s (e .g . y ea rs w h en c o n d u ct ed , re q u ir ed m in im u m f o ll o w -u p ). N o te w h et h er t h es e w er e ap p li ed a t th e st u d y o r in d iv id u al l ev el i .e . w h et h er e li g ib le p ar ti ci p an ts w er e in cl u d ed ( an d i n el ig ib le p ar ti ci p an ts ex cl u d ed ) fr o m a s tu d y t h at i n cl u d ed a w id er p o p u la ti o n t h an s p ec if ie d b y t h e re v ie w i n cl u si o n c ri te ri a. T h e ra ti o n al e fo r cr it er ia s h o u ld b e st at ed . Id en ti fy in g 7 D es cr ib e al l m et h o d s o f id en ti fy in g p u b li sh ed a n d u n p u b li sh ed s tu d ie s in cl u d in g , as a p p li ca b le : w h ic h b ib li o g ra p h ic st u d ie s – d at ab as es w er e se ar ch ed w it h d at es o f co v er ag e; d et ai ls o f an y h an d s ea rc h in g i n cl u d in g o f co n fe re n ce p ro ce ed in g s; in fo rm at io n u se o f st u d y r eg is te rs a n d a g en cy o r co m p an y d at ab as es ; co n ta ct w it h t h e o ri g in al r es ea rc h t ea m a n d e x p er ts so u rc es in t h e fi el d ; o p en a d v er ts a n d s u rv ey s. G iv e th e d at e o f la st s ea rc h o r el ic it at io n . co n ti n u es o n t h e n ex t p a ge
co n tI n u A tI o n P R IS M A -I P D It em R ep o rt ed S ec ti o n /t o p ic N o C h ec k li st i te m o n p ag e Id en ti fy in g 8 P re se n t th e fu ll e le ct ro n ic s ea rc h s tr at eg y f o r at l ea st o n e d at ab as e, i n cl u d in g a n y l im it s u se d , su ch t h at i t st u d ie s – se ar ch co u ld b e re p ea te d . St u d y se le ct io n 9 S ta te t h e p ro ce ss f o r d et er m in in g w h ic h s tu d ie s w er e el ig ib le f o r in cl u si o n . p ro ce ss es D at a co ll ec ti o n 1 0 D es cr ib e h o w I P D w er e re q u es te d , co ll ec te d a n d m an ag ed , in cl u d in g an y p ro ce ss es f o r q u er yi n g an d c o n fi rm in g d at a w it h p ro ce ss es in v es ti g at o rs . I f IP D w er e n o t so u g h t fr o m a n y e li g ib le s tu d y, t h e re as o n f o r th is s h o u ld b e st at ed ( fo r ea ch s u ch s tu d y ). If a p p li ca b le , d es cr ib e h o w a n y s tu d ie s fo r w h ic h I P D w er e n o t av ai la b le w er e d ea lt w it h . T h is s h o u ld i n cl u d e w h et h er , h o w a n d w h at a g g re g at e d at a w er e so u g h t o r ex tr ac te d f ro m s tu d y r ep o rt s an d p u b li ca ti o n s (s u ch a s ex tr ac ti n g d at a in d ep en d en tl y i n d u p li ca te ) an d a n y p ro ce ss es f o r o b ta in in g a n d c o n fi rm in g t h es e d at a w it h i n v es ti g at o rs . D at a it em s 1 1 D es cr ib e h o w t h e in fo rm at io n a n d v ar ia b le s to b e co ll ec te d w er e ch o se n . L is t an d d ef in e al l st u d y l ev el a n d p ar ti ci p an t le v el d at a th at w er e so u g h t, i n cl u d in g b as el in e an d f o ll o w -u p i n fo rm at io n . If a p p li ca b le , d es cr ib e m et h o d s o f st an d ar d is in g o r tr an sl at in g v ar ia b le s w it h in t h e IP D d at as et s to e n su re c o m m o n s ca le s o r m ea su re m en ts a cr o ss s tu d ie s. IP D i n te g ri ty A 1 D es cr ib e w h at a sp ec ts o f IP D w er e su b je ct t o d at a ch ec k in g ( su ch a s se q u en ce g en er at io n , d at a co n si st en cy a n d c o m p le te n es s, b as el in e im b al an ce ) an d h o w t h is w as d o n e. R is k o f b ia s 1 2 D es cr ib e m et h o d s u se d t o a ss es s ri sk o f b ia s in t h e in d iv id u al s tu d ie s an d w h et h er t h is w as a p p li ed s ep ar at el y f o r as se ss m en t in ea ch o u tc o m e. I f ap p li ca b le , d es cr ib e h o w f in d in g s o f IP D c h ec k in g w er e u se d t o i n fo rm t h e as se ss m en t. in d iv id u al R ep o rt i f an d h o w r is k o f b ia s as se ss m en t w as u se d i n a n y d at a sy n th es is . st u d ie s. S p ec if ic at io n 1 3 S ta te a ll t re at m en t co m p ar is o n s o f in te re st s. S ta te a ll o u tc o m es a d d re ss ed a n d d ef in e th em i n d et ai l. o f o u tc o m es S ta te w h et h er t h ey w er e p re -s p ec if ie d f o r th e re v ie w a n d , if a p p li ca b le , w h et h er t h ey w er e p ri m ar y /m ai n o r an d e ff ec t se co n d ar y /a d d it io n al o u tc o m es . G iv e th e p ri n ci p al m ea su re s o f ef fe ct ( su ch a s ri sk r at io , h az ar d r at io , d if fe re n ce m ea su re s in m ea n s) u se d f o r ea ch o u tc o m e. S y n th es is 1 4 D es cr ib e th e m et a-an al y si s m et h o d s u se d t o s y n th es is e IP D . S p ec if y a n y s ta ti st ic al m et h o d s an d m o d el s u se d . m et h o d s Is su es s h o u ld i n cl u d e (b u t ar e n o t re st ri ct ed t o ): • U se o f a o n e-st ag e o r tw o -s ta g e ap p ro ac h . • H o w e ff ec t es ti m at es w er e g en er at ed s ep ar at el y w it h in e ac h s tu d y a n d c o m b in ed a cr o ss s tu d ie s (w h er e ap p li ca b le ). • S p ec if ic at io n o f o n e-st ag e m o d el s (w h er e ap p li ca b le ) in cl u d in g h o w c lu st er in g o f p at ie n ts w it h in s tu d ie s w as a cc o u n te d f o r. • U se o f fi x ed o r ra n d o m e ff ec ts m o d el s an d a n y o th er m o d el a ss u m p ti o n s, s u ch a s p ro p o rt io n al h az ar d s. • H o w ( su m m ar y ) su rv iv al c u rv es w er e g en er at ed ( w h er e ap p li ca b le ). • M et h o d s fo r q u an ti fy in g s ta ti st ic al h et er o g en ei ty ( su ch a s I2 a n d τ 2 ). • H o w s tu d ie s p ro v id in g I P D a n d n o t p ro v id in g I P D w er e an al y se d t o g et h er ( w h er e ap p li ca b le ). • H o w m is si n g d at a w it h in t h e IP D w er e d ea lt w it h ( w h er e ap p li ca b le ). co n ti n u es o n t h e n ex t p a ge
co n tI n u A tI o n P R IS M A -I P D It em R ep o rt ed S ec ti o n /t o p ic N o C h ec k li st i te m o n p ag e E x p lo ra ti o n o f A 2 If a p p li ca b le , d es cr ib e an y m et h o d s u se d t o e x p lo re v ar ia ti o n i n e ff ec ts b y s tu d y o r p ar ti ci p an t le v el c h ar ac te ri st ic s (s u ch v ar ia ti o n i n as e st im at io n o f in te ra ct io n s b et w ee n e ff ec t an d c o v ar ia te s) . S ta te a ll p ar ti ci p an t-le v el c h ar ac te ri st ic s th at w er e an al y se d ef fe ct s as p o te n ti al e ff ec t m o d if ie rs , an d w h et h er t h es e w er e p re -s p ec if ie d . R is k o f b ia s 1 5 S p ec if y a n y a ss es sm en t o f ri sk o f b ia s re la ti n g t o t h e ac cu m u la te d b o d y o f ev id en ce , in cl u d in g a n y p er ta in in g t o n o t o b ta in in g ac ro ss s tu d ie s IP D f o r p ar ti cu la r st u d ie s, o u tc o m es o r o th er v ar ia b le s. A d d it io n al 1 6 D es cr ib e m et h o d s o f an y a d d it io n al a n al y se s, i n cl u d in g s en si ti v it y a n al y se s. S ta te w h ic h o f th es e w er e p re -s p ec if ie d . an al y se s R es u lt s S tu d y s el ec ti o n 1 7 G iv e n u m b er s o f st u d ie s sc re en ed , as se ss ed f o r el ig ib il it y, a n d i n cl u d ed i n t h e sy st em at ic r ev ie w w it h r ea so n s fo r ex cl u si o n s an d I P D at e ac h s ta g e. I n d ic at e th e n u m b er o f st u d ie s an d p ar ti ci p an ts f o r w h ic h I P D w er e so u g h t an d f o r w h ic h I P D w er e o b ta in ed . o b ta in ed F o r th o se s tu d ie s w h er e IP D w er e n o t av ai la b le , g iv e th e n u m b er s o f st u d ie s an d p ar ti ci p an ts f o r w h ic h a g g re g at e d at a w er e av ai la b le . R ep o rt r ea so n s fo r n o n -a v ai la b il it y o f IP D . In cl u d e a fl o w d ia g ra m . S tu d y 1 8 F o r ea ch s tu d y, p re se n t in fo rm at io n o n k ey s tu d y a n d p ar ti ci p an t ch ar ac te ri st ic s (s u ch a s d es cr ip ti o n o f in te rv en ti o n s, ch ar ac te ri st ic s n u m b er s o f p ar ti ci p an ts , d em o g ra p h ic d at a, u n av ai la b il it y o f o u tc o m es , fu n d in g s o u rc e, a n d i f ap p li ca b le d u ra ti o n o f fo ll o w -u p ). P ro v id e (m ai n ) ci ta ti o n s fo r ea ch s tu d y. W h er e ap p li ca b le , al so r ep o rt s im il ar s tu d y c h ar ac te ri st ic s fo r an y s tu d ie s n o t p ro v id in g I P D . IP D i n te g ri ty A 3 R ep o rt a n y i m p o rt an t is su es i d en ti fi ed i n c h ec k in g I P D o r st at e th at t h er e w er e n o n e. R is k o f b ia s 1 9 P re se n t d at a o n r is k o f b ia s as se ss m en ts . If a p p li ca b le , d es cr ib e w h et h er d at a ch ec k in g l ed t o t h e u p -w ei g h ti n g o r w it h in s tu d ie s d o w n -w ei g h ti n g o f th es e as se ss m en ts . C o n si d er h o w a n y p o te n ti al b ia s im p ac ts o n t h e ro b u st n es s o f m et a-an al y si s co n cl u si o n s. R es u lt s o f 2 0 F o r ea ch c o m p ar is o n a n d f o r ea ch m ai n o u tc o m e (b en ef it o r h ar m ), f o r ea ch i n d iv id u al s tu d y r ep o rt t h e n u m b er o f el ig ib le in d iv id u al p ar ti ci p an ts f o r w h ic h d at a w er e o b ta in ed a n d s h o w s im p le s u m m ar y d at a fo r ea ch i n te rv en ti o n g ro u p ( in cl u d in g , w h er e st u d ie s ap p li ca b le , th e n u m b er o f ev en ts ), e ff ec t es ti m at es a n d c o n fi d en ce i n te rv al s. T h es e m ay b e ta b u la te d o r in cl u d ed o n a f o re st p lo t. R es u lt s o f 2 1 P re se n t su m m ar y e ff ec ts f o r ea ch m et a-an al y si s u n d er ta k en , in cl u d in g c o n fi d en ce i n te rv al s an d m ea su re s o f st at is ti ca l sy n th es es h et er o g en ei ty . S ta te w h et h er t h e an al y si s w as p re -s p ec if ie d , an d r ep o rt t h e n u m b er s o f st u d ie s an d p ar ti ci p an ts a n d , w h er e ap p li ca b le , th e n u m b er o f ev en ts o n w h ic h i t is b as ed . W h en e x p lo ri n g v ar ia ti o n i n e ff ec ts d u e to p at ie n t o r st u d y c h ar ac te ri st ic s, p re se n t su m m ar y i n te ra ct io n e st im at es f o r ea ch ch ar ac te ri st ic e x am in ed , in cl u d in g c o n fi d en ce i n te rv al s an d m ea su re s o f st at is ti ca l h et er o g en ei ty . S ta te w h et h er t h e an al y si s w as p re -s p ec if ie d . S ta te w h et h er a n y i n te ra ct io n i s co n si st en t ac ro ss t ri al s. P ro v id e a d es cr ip ti o n o f th e d ir ec ti o n a n d s iz e o f ef fe ct i n t er m s m ea n in g fu l to t h o se w h o w o u ld p u t fi n d in g s in to p ra ct ic e. R is k o f b ia s 2 2 P re se n t re su lt s o f an y a ss es sm en t o f ri sk o f b ia s re la ti n g t o t h e ac cu m u la te d b o d y o f ev id en ce , in cl u d in g a n y p er ta in in g t o ac ro ss s tu d ie s th e av ai la b il it y a n d r ep re se n ta ti v en es s o f av ai la b le s tu d ie s, o u tc o m es o r o th er v ar ia b le s. co n ti n u es o n t h e n ex t p a ge
co n tI n u A tI o n P R IS M A -I P D It em R ep o rt ed S ec ti o n /t o p ic N o C h ec k li st i te m o n p ag e A d d it io n al 2 3 G iv e re su lt s o f an y a d d it io n al a n al y se s (e .g . se n si ti v it y a n al y se s) . If a p p li ca b le , th is s h o u ld a ls o i n cl u d e an y a n al y se s th at an al y se s in co rp o ra te a g g re g at e d at a fo r st u d ie s th at d o n o t h av e IP D . If a p p li ca b le , su m m ar is e th e m ai n m et a-an al y si s re su lt s fo ll o w in g th e in cl u si o n o r ex cl u si o n o f st u d ie s fo r w h ic h I P D w er e n o t av ai la b le . D is cu ss io n S u m m ar y o f 2 4 S u m m ar is e th e m ai n f in d in g s, i n cl u d in g t h e st re n g th o f ev id en ce f o r ea ch m ai n o u tc o m e. ev id en ce S tr en g th s an d 2 5 D is cu ss a n y i m p o rt an t st re n g th s an d l im it at io n s o f th e ev id en ce i n cl u d in g t h e b en ef it s o f ac ce ss t o I P D a n d a n y l im it at io n s li m it at io n s ar is in g f ro m I P D t h at w er e n o t av ai la b le . C o n cl u si o n s 2 6 P ro v id e a g en er al i n te rp re ta ti o n o f th e fi n d in g s in t h e co n te x t o f o th er e v id en ce . Im p li ca ti o n s A 4 C o n si d er r el ev an ce t o k ey g ro u p s (s u ch a s p o li cy m ak er s, s er v ic e p ro v id er s an d s er v ic e u se rs ). C o n si d er i m p li ca ti o n s fo r fu tu re r es ea rc h . F u n d in g F u n d in g 2 7 D es cr ib e so u rc es o f fu n d in g a n d o th er s u p p o rt ( su ch a s su p p ly o f IP D ), a n d t h e ro le i n t h e sy st em at ic r ev ie w o f th o se p ro v id in g s u ch s u p p o rt . A 1 – A 3 d en o te n ew i te m s th at a re a d d it io n al t o s ta n d ar d P R IS M A i te m s. A 4 h as b ee n c re at ed a s a re su lt o f re -a rr an g in g c o n te n t o f th e st an d ar d P R IS M A s ta te m en t to s u it t h e w ay t h at s y st em at ic r ev ie w I P D m et a-an al y se s ar e re p o rt ed . © R ep ro d u ce d w it h p er m is si o n o f th e P R IS M A I P D G ro u p , w h ic h e n co u ra g es s h ar in g a n d r eu se f o r n o n -c o m m er ci al p u rp o se
APPEndIx 2. suMMAry tAblE of ElIGIblE studIEs for tHIs IPd MEtA-AnAlysIs AlrEAdy IdEntIfIEd F o ll o w -U p T ri al n am e – T ri al r eg is tr y D ru g – C o m p an y S am p le D u ra ti o n D am ag e F u n ct io n P o p u la ti o n P R E M IE R N C T 0 0 1 9 5 6 6 3 A d al im u m ab A b b v ie 7 9 9 / 6 9 7 / 4 5 2 1 0 y m T S S H A Q N aï v e M T X D E 0 1 9 N C T 0 0 1 9 5 7 0 2 A d al im u m ab A b b v ie 6 1 9 / 2 0 2 / 3 2 7 1 0 y m T S S H A Q N o n -r es p o n d er s M T X T E A R N C T 0 0 2 5 9 6 1 0 E ta n er ce p t - P fi ze r 7 5 5 /4 7 6 2 y m T S S m H A Q N o n -r es p o n d er s M T X C O M E T N C T 0 0 1 9 5 4 9 4 E ta n er ce p t - P fi ze r 5 4 2 /3 9 8 2 y m T S S H A Q N aï v e M T X C A M E O N C T 0 0 6 5 4 3 6 8 E ta n er ce p t - P fi ze r 2 0 5 2 Y m T S S H A Q N o n -r es p o n d er s M T X P R IZ E N C T 0 0 9 1 3 4 5 8 E ta n er ce p t - P fi ze r 1 9 3 /1 3 1 1 ,5 /2 y m T S S H A Q N aï v e M T X T E M P O N C T 0 0 3 9 3 4 7 1 E ta n er ce p t - P fi ze r 6 8 2 3 y m T S S H A Q F ai le d D M A R D ( n o t M T X ) P R E S E R V E N C T 0 0 5 6 5 4 0 9 E ta n er ce p t - P fi ze r 6 0 0 2 y ( 8 8 w ) m T S S H A Q N o n -r es p o n d er s M T X E R A N C T 0 0 3 5 6 5 9 0 E ta n er ce p t - P fi ze r 6 3 2 /5 1 2 2 y S h ar p H A Q N aï v e M T X ~ 3 0 0 2 + 3 y G O B E F O R E N C T 0 0 2 6 4 5 3 7 G o li m u m ab M S D 6 3 7 /4 2 2 2 + 3 Y m T S S H A Q N aï v e M T X G O F O R W A R D N C T 0 0 2 6 4 5 5 0 G o li m u m ab M S D 4 4 4 /3 1 3 5 Y m T S S H A Q N o n -r es p o n d er s M T X G O F U R T H E R N C T 0 0 9 7 3 4 7 9 G o li m u m ab M S D 5 9 2 /4 8 6 2 Y ( 1 0 0 w ) m T S S H A Q N o n -r es p o n d er s M T X A T T R A C T N C T 0 0 2 6 9 8 6 7 In fl ix im ab M S D 4 2 8 /3 4 0 2 y ( 1 0 2 w ) m T S S H A Q N o n -r es p o n d er s M T X A S P IR E N C T 0 0 2 3 6 0 2 8 In fl ix im ab - M S D 1 0 4 9 1 y m T S S H A Q N o n -r es p o n d er s M T X L IT H E N C T 0 0 1 0 6 5 3 5 T o ci li zu m ab R o ch e 1 1 9 0 / 1 1 4 9 5 y G m T S S H A Q N o n -r es p o n d er s M T X F U N C T IO N N C T 0 1 0 0 7 4 3 5 T o ci li zu m ab R o ch e 1 1 5 7 2 y m T S S H A Q N o n -r es p o n d er s M T X B R E V A C T A N C T 0 1 2 3 2 5 6 9 T o ci li zu m ab R o ch e 6 5 6 / 3 1 4 2 Y m T S S H A Q N o n -r es p o n d er s M T X A C T -R A Y N C T 0 0 8 1 0 1 9 9 T o ci li zu m ab R o ch e 5 1 2 /4 2 3 2 Y G m T S S H A Q N o n -r es p o n d er s M T X S A M U R A I - N C T 0 0 1 4 4 5 0 8 T o ci li zu m ab R o ch e 3 0 6 /2 4 1 1 y m T S S m H A Q N o n -r es p o n d er s M T X 3 y S U R P R IS E N C T 0 1 1 2 0 3 6 6 T o ci li zu m ab R o ch e 2 2 6 2 Y m T S S H A Q N o n -r es p o n d er s M T X R E F L E X N C T 0 0 4 6 8 5 4 6 / R it u x im ab - R o ch e 5 1 7 2 Y G m T S S H A Q In ad eq u at e re sp o n se t o N C T 0 2 0 9 7 7 4 5 1 8 4 5 Y an ti -T N F IM A G E N C T 0 0 2 9 9 1 0 4 R it u x im ab R o ch e 7 7 6 /6 0 6 2 Y G m T S S H A Q N aï v e M T X R A P ID 1 N C T 0 0 1 5 2 3 8 6 C er to li zu m ab U C B 9 8 2 /8 4 7 3 y ( 1 4 8 w ) m T S S H A Q N o n -r es p o n d er s M T X R A P ID 2 N C T 0 0 1 6 0 6 0 2 / C er to li zu m ab U C B 6 1 9 /5 6 7 2 ,5 y ( 1 2 8 w ) m T S S H A Q N o n -r es p o n d er s M T X N C T 0 0 1 7 5 8 7 7 C -O P E R A N C T 0 1 4 5 1 2 0 3 C er to li zu m ab U C B 3 1 6 /1 8 4 1 y 1 3 1 2 y m T S S H A Q N aï v e M T X O R A L S T A R T N C T 0 1 0 3 9 6 8 8 T o fa ci ti n ib P fi ze r 9 5 8 /9 5 6 2 y m T S S H A Q N aï v e M T X O R A L S C A N N C T 0 0 8 4 7 6 1 3 T o fa ci ti n ib P fi ze r 7 9 7 2 y m T S S H A Q N o n -r es p o n d er s M T X D M A R D d is ea se -m o d if y in g a n ti rh eu m at ic d ru g s; G m T S S G en an t-m o d if ie d T o ta l S h ar p S co re ; H A Q H ea lt h A ss es sm en t Q u es ti o n n ai re ; m H A Q – m o d if ie d H ea lt h A ss es sm en t q u es ti o n n ai re ; m T S S m o d if ie d T o ta l S h ar p S co re ; M T X M et o tr ex at e; T N F t u m o r n ec ro si s fa ct o r
APPEndIx 3. lIst of vArIAblEs rEquIrEd And dEsIrAblE for AnAlysEs
• Remission definition data (minimum at baseline, 6 and 12 months; desired also at 3 and 9 months, 2 years, others) – SJC28
– TJC28
– CRP (in mg/dl or mg/L, but clearly indicated) – PGA
• Outcome data (minimum at baseline, 12 and 24 months; desired 5 and 10 years) – Radiographic score
– HAQ
• Patient characteristics (all at baseline only) – gender
– age at baseline
• Clinical characteristics (all at baseline only) – disease duration at baseline
– RF
– ACPA (not essential) – Treatment arm • Trial/visit information
– anonymised patient ID code (at baseline only) – visit number or sequence
– visit date
APPEndIx 4. ExAMPlEs of PAtIEnt's clAssIfIcAtIon In dIffErEnt rEMIssIon stAtE dEfInItIons (dIcHotoMIc And cAtEGorIcAl) And consIdErInG sInGlE or MultIPlE tIME