w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
Autoantibodies
in
systemic
sclerosis
and
their
clinical
correlation
in
patients
from
a
Midwestern
region
of
Brazil
Alex
Magno
Coelho
Horimoto
a,∗,
Izaias
Pereira
da
Costa
a,baUniversidadeFederaldeMatoGrossodoSul,CampoGrande,MS,Brazil bUniversidadedeSãoPaulo,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received28March2014 Accepted21September2014 Availableonline6January2015
Keywords:
Autoantibodies Systemicsclerosis Anti-topoisomeraseI Anti-centromere Anti-RNApolymeraseIII
a
b
s
t
r
a
c
t
Introduction:Systemicsclerosis(SSc)isaconnectivetissuediseaseofautoimmunenature characterizedbythetriadofvascularinjury,autoimmunity(cellularandhumoral)and tis-sue fibrosis.Autoantibodiesdonot seemtobesimplyepiphenomena,but areinvolved indiseasepathogenesis.Itisbelieved thattheSSc-specificautoantibodiesare responsi-blebothforamplifyingimmuneresponseandtargetingcelltypesthatarerelevantinthe pathophysiologyofSSc.
Objectives: Tocorrelatetheprofileofthefollowingspecificautoantibodies:anti-centromere (ACA),anti-topoisomeraseI(topoI)andanti-RNApolymeraseIII(RNAPIII)withclinicaland laboratorymanifestationswereobservedin46patientswithSScintheMidwestregionof Brazil.
Methods:Theoccurrenceofspecificautoantibodiesin46patientswithSScwasinvestigated, correlatingthetypeofautoantibodywithclinicalandlaboratorymanifestationsfound.
Results:Amongallpatientsevaluated,wefoundapredominanceoffemales(97.8%),mean age 50.21 yearsold, Caucasian (50%),limited cutaneous SSc (47.8%), time ofdiagnosis between5and10years(50%),anddiseasedurationof9.38years.Accordingtothespecific autoantibodyprofile,24patientswereACA-positive(52.2%),15werepositiveforanti-topo I(32.6%),and7showedpositiveanti-RNAPIII(15.2%).Theanti-topoIautoantibody cor-related withdiffusescleroderma,withgreaterdiseaseseverityandactivity,withworse qualityoflifemeasuredbytheSHAQindex,witha higherprevalenceofobjective Ray-naud’sphenomenonanddigitalpittingscarsoffingertips.TheACAcorrelatedwithlimited scleroderma,withearlieronsetofdisease,aswellashigherprevalenceoftelangiectasias. Theanti-RNAPIIIcorrelatedwithdiffusescleroderma,withahigheroccurrenceof subjec-tiveRaynaud’sphenomenonandmuscleatrophy.Therewasnoassociationbetweenthe positivityforanti-topoI,ACAandanti-RNAPIIIantibodiesandothervariablesrelatedto laboratoryabnormalities,aswellasRodnanskinscoreandskin,vascular,musculoskeletal, gastrointestinal,cardiopulmonaryandrenalmanifestations.
∗ Correspondingauthor.
E-mail:[email protected](A.M.C.Horimoto).
http://dx.doi.org/10.1016/j.rbre.2014.09.009
Conclusions:TheclinicalsubtypeofthediseaseandsomeclinicalmanifestationsinSScmay correlatepositivelywiththepresenceofspecificautoantibodies.
©2014ElsevierEditoraLtda.Allrightsreserved.
Autoanticorpos
em
esclerose
sistêmica
e
sua
correlac¸ão
com
as
manifestac¸ões
clínicas
da
doenc¸a
em
pacientes
do
Centro-Oeste
do
Brasil
Palavras-chave:
Autoanticorpos Esclerosesistêmica AntitopoisomeraseI Anticentrômero Anti-RNApolimeraseIII
r
e
s
u
m
o
Introduc¸ão: aesclerosesistêmica(ES)éumaenfermidadedotecidoconjuntivodecaráter autoimunecaracterizadapelatríadedeinjúriavascular,autoimunidade(celularehumoral) efibrosetecidual.Osautoanticorposnãoparecemsersimplesmenteepifenômenos,massim estaremenvolvidosnapatogênesedadoenc¸a.Acredita-sequeosautoanticorposespecíficos daESsãoresponsáveistantopelaamplificac¸ãodarespostaimunequantoporalvejarostipos celularesquesãorelevantesnafisiopatologiadaES.
Objetivos: correlacionaroperfildeautoanticorposespecíficos(anti-SCL70,ACA,anti-POL3) comasmanifestac¸õesclínicaselaboratoriaisobservadasem46pacientescomESdaregião Centro-OestedoBrasil.
Métodos: pesquisou-seaocorrênciadeautoanticorposespecíficosem 46pacientescom diagnósticodeESecorrelacionou-seotipodeautoanticorpocomasmanifestac¸õesclínicas elaboratoriaisencontradas.
Resultados: dentretodosospacientesavaliados,encontrou-sepredomíniofeminino(97,8%), idademédiade50,21anos,corbranca(50%),formalimitadadadoenc¸a(47,8%),tempode diagnósticoentrecincoe10anos(50%)etempodeevoluc¸ãodadoenc¸ade9,38anos.De acordocomoautoanticorpoespecífico,24pacientesapresentavamACApositivo(52,2%), 15apresentavampositividadeparaanti-SCL70(32,6%)eseteapresentavamanti-POL3 pos-itivo(15,2%).Oautoanticorpoanti-SCL70secorrelacionoucomaformadifusadadoenc¸a, commaiorgravidadeeatividadedadoenc¸a,compiorqualidadedevidamedidapeloíndice HAQ,commaiorprevalênciadefenômenodeRaynaudobjetivoemicrocicatrizesdepolpas digitais.OACAsecorrelacionoucomaformalimitadadadoenc¸a,comoiníciomais pre-cocedaenfermidade,bemcomocommaiorprevalênciadetelangiectasiasnospacientes. Já oanti-POL3secorrelacionou coma forma difusada doenc¸a, commaiorocorrência defenômenodeRaynaudsubjetivoedeatrofiamuscular.Paraasdemaisvariáveis rela-cionadasàsalterac¸õeslaboratoriais,bemcomoemrelac¸ãoaoescorecutâneodeRodnane àsmanifestac¸õescutâneas,vasculares,musculoesqueléticas,gastrintestinais, cardiopul-monares erenais,nãohouveassociac¸ãoentreelaseapositividade paraos anticorpos anti-SCL70,ACAeanti-POL3.
Conclusões: aformaclínicadadoenc¸aealgumasmanifestac¸õesclínicasnaESpodemse correlacionarpositivamentecomapresenc¸adeautoanticorposespecíficos.
©2014ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Systemic sclerosis (SSc) is a connective tissue disease of autoimmune nature, extremely heterogeneous in its clin-ical presentation, with involvement of multiple systems, and followinga variable andunpredictable course.1 Its
eti-ology remains unknown, witha multifactorial cause being suggested,possiblytriggeredbyenvironmentalfactors ina geneticallypredisposedindividual.2
Thehallmark ofSSc ismicrovasculopathy, activation of fibroblastsandexcessivecollagenproduction.3Itisaunique
disease as it has features of three distinct pathophysiolo-gical processes; it consists of the triad of vascular injury, autoimmunity (cellular and humoral) and tissue fibrosis,
leadingtoinvolvementofskin,inadditiontoseveral inter-nalorganssuchaslungs,heart,gastrointestinaltract,among others.3,4
Itisbelievedthatthelinkbetweeninitialvascular involve-mentandthefinalconsequenceofthedisease(tissuefibrosis) couldberepresentedbyautoimmunity.Circulatingantibodies, alteration of immune mediators and infiltration of mono-nuclearcellsinaffectedorgansrepresentapositiveargument forthe hypothesisthatdysfunction ofthe immunesystem leadstoillness.5,6
It is described that highly specific antibodies can be detected in the sera of virtually all patients with SSc.7 A
involvementofthehumoralimmunesysteminthegenesis ofSSc.8 These autoantibodieshavefundamental
character-istics ofaresponse triggeredbythe antigen, beingmainly representedby:centromereantibodies(ACA),anti-DNA topo-isomeraseI(anti-topoI),andanti-RNAantibodiespolymerase III(anti-RNAPIII).9–12
Recent studies highlight the pathogenic potential of autoantibodiesinSScpatients,suggestingthatspecific anti-bodiesagainstfibroblasts,endothelialcellsandreceptorsfor platelet-derivedgrowthfactor(PDGF)candirectlycause acti-vationoffibroblastsandendothelialcells andcontributeto tissuedamage.1,13,14
Thereisevidencetosupporttheideathatthecomplexityof theSScseemstorepresentanothercollectionofphenotypes comparedtoasinglediseaseentity.Thus,thesegenetic asso-ciationsmayactuallyberelatedtodistinctphenotypesinthe SScbasedonapatternofautoantibodies.15
The region of the HLA genes is a clear example of genetic polymorphism in the development of SSc.15
HLA association studies were very inconsistent when patients were grouped by race or ethnicity.15,16
How-ever, when patients with SSc were grouped according to the autoantibody profile, the findings were consistent across the different ethnic groups.15 For example,
HLA-DRB1*01–DQB1*0501 are more common in patients with ACA-positiveSScwhilehaplotypesHLA-DRB1*11–DQB1*0301 have been associated with the positivity of anti-topo I antibodies.16
The mechanisms postulated for the development of autoantibodiesinSSc patients include:molecular mimicry, chronic hyper-reactivity of B lymphocytes from intrinsic abnormalities of the cell and increased expression, or alteredsubcellularlocalizationofpotentially auto-antigenic peptides.1 Some antibodies do not appear to be simply
epiphenomena,buttobeinvolvedindiseasepathogenesis,17
possiblybyamplifyingthe immuneresponseand targeting cell types that are relevant in the pathophysiology of the disease.18
TheimportanceofthestudyofautoantibodiesinSScliesin thefactthatsomeofthemhaveassociationwiththedisease andparticipateinthecriteriaproposedbyLeRoyandMedsger forearlydiagnosis ofthecondition,whichgivesthem con-siderablediagnosticvalue.9,10,19Moreover,theyareassociated
withcertainphenotypictraitsofthedisease,andareusedto aidintheclassificationandcharacterizationoftwomajor dis-easesubtypes:diffusecutaneousSScandlimitedcutaneous SSc.10,20Also,acloserelationshipbetweenlevelsofanti-topoI
andseverityofskininvolvementandglobaldiseaseactivityin SScwasobserved,revealingapossibleprognosticrole.10,21In
addition,significantcorrelationsbetweenthepatternof anti-bodyprofilepresentedandthetherapeuticresponsehavebeen reported.22
Objectives
Tocorrelatetheprofileofspecificautoantibodies(ACA, anti-topoIandanti-RNAPIII)withclinicalmanifestationsobserved in46patientswithSScfollowedinauniversitycenterfromthe MidwestregionofBrazil.
Methods
Thisisanobservationalstudyofcross-sectionaldesign,with prospectiveanalysisofpatientdata.
Arandomselectionof46patientswascarriedoutfroma surveyofthemedicalrecordsoftheDepartmentof Rheuma-tologyoftheUniversityHospitaloftheSchoolofMedicineof theFederalUniversityofMatoGrossodoSul(FMUFMS).
Thepatientsweredividedintothreegroups,accordingto thepositivityofoneofthespecificautoantibodies(ACA, anti-topoIandanti-RNAPIII).
Patientsshouldmeetthefollowinginclusioncriteria:
• Meetthe2013newclassificationCriteriaforSSc;23
• Incasesofabsenceofskinthickening,theyshouldmeetthe 2001LeRoyandMedsger’scriteriaofearlySSc;24
• They should have signed a Consent Form previously approvedbytheResearchEthicsCommitteeofUFMS.
• Patients who presentedwith other associated infectious diseasesormalignancieswereexcluded.
The socio-demographic and clinical information was obtainedfromthepatientmedicalrecordsandcomplemented withtwointerviews,withinatimeintervalof6months.In thefirstappointment,demographicandclinicaldatawere col-lected,includingdiseaseduration,yearofdiagnosis,modified Rodnan skin score,25 autoantibodies test, thorough clinical
examinationandcurrenttreatment.
Diseasedurationwasdividedintotwo:totaltimeinyears ofRaynaud’sphenomenon(RP)beforediagnosisofthedisease (RPtime)andtotaltimeinyearsofclinicalmanifestationsof thediseaseafterdiagnosis,notconsideringRP(timewithout RP).
Specific data about Medsger’s Severity Criteria26 and
Valentini’sCriteriaofActivity27werecollectedonspecific
for-mularies at baseline assessment and after 6 months. The SclerodermaHealthAssessmentQuestionnaire(SHAQ)28was
alsocollectedintheinitialpatientassessmentandonsecond assessment.
SHAQisameasureoffunctioninSSc,beingahelpfultool fortheassessmentofphysicalfunctionaldisability29andthe
impactofthediseaseonpatient’sphysicalandmental well-being.30Theobjectivewastocorrelateiftherateofdisability
measuredbySHAQwouldbehigherinoneofthethreegroups ofpatientswithspecificautoantibodies(ACA,anti-topoIand anti-RNAPIII).
Seraproperlyfrozenat−50◦CandstoredattheLaboratory
oftheUniversityHospitalofUFMSfrompreviouslyselected patientswasusedforperformingtheresearch.
(a) Fortheexaminationofanti-centromere(ACA)–weused theindirect immunofluorescence techniqueand having HEp2 cells as substrate according tothe criteria of the IIBrazilianConsensusofantinuclearantibodyinHep-2 (2003)cells,31fortheinterpretationofresults.
(b) Fortheexaminationofanti-DNAtopoisomerase1 (anti-topo I) – enzyme immunoassaytechnique was used,21
andstronglypositiveif>80units.AspecifickitQUANTA LiteTMScl-70wasusedfromLaboratoryINOVA(INOVA Diagnostics,Inc.,SanDiego,CA,USA),followingthe man-ufacturer’sspecifications.
(c) Anti-RNA polymerase III (anti-RNAP III) antibody – examinations were performedin duplicateusing ELISA technique, as previously described.32 Values <20 units
wereconsidered negative,weaklypositiveifbetween20 and 39 units, moderatelypositiveif between40and 80 unitsandstronglypositiveif>80units.
Statisticalanalysis
Comparisonofpatientswithpositiveanti-topoIantibody,ACA oranti-RNAPIIIinrelationtothequantitativevariables eval-uatedinthisstudywasperformedbyone-wayANOVA.
Thechi-square test was used toassess the association betweentheresultsfortheantibodies(ACA,anti-topoIand anti-RNAP III), with qualitative variables measured in this study.Theresultsoftheother variables were presentedin theformofdescriptivestatisticsorintheformoftablesand graphs.Statistical analysiswasperformed usingSPSS soft-ware,version20.0,consideringasignificancelevelof5%.
Results
Ofthe 46patients included, 45 werewomen (97.8%)and 1 was a man (2.2%), with a mean age of 50.21±3.55 years (mean±standarderror).
Theraceofthepatientswasasfollows:23patientswere classifiedas Caucasians(50.0%), 21as mixed(45.7%)and 2 patients,black(4.3%).
Regarding the diagnosis, 42 diagnosedpatients met the 2013ACR/EULAR classificationCriteria forSSc (91.3%). The 4 patients (8.7%) who did not meet these criteria met LeRoy/Medsger’scriteriaforearlySSc.
Regardingtheclinicalsubtypesofthedisease,22patients hadlimitedcutaneousSSc(47.8%),16patientshadthediffuse cutaneousSSc(34.8%),3patientshadtheearlyform(6.5%), 5patientshad overlapform(10.9%)and nonehad theSine Sclerodermaform.TheseresultsareshowninFig.1.
Regardingtimesincediagnosis,12patientswerediagnosed formorethan 10years(26.1%), 23patientswere diagnosed between5and10years(50.0%)and11patientswerediagnosed forlessthan5years(23.9%).
Thetimefordiseaseprogressionofpatientsingeneralwas 9.38±3.08years.
Amongall patients, 24 showed positive ACA(52.2%), 15 werepositiveforanti-topo I(32.6%)and7werepositivefor anti-RNAPIII(15.2%).
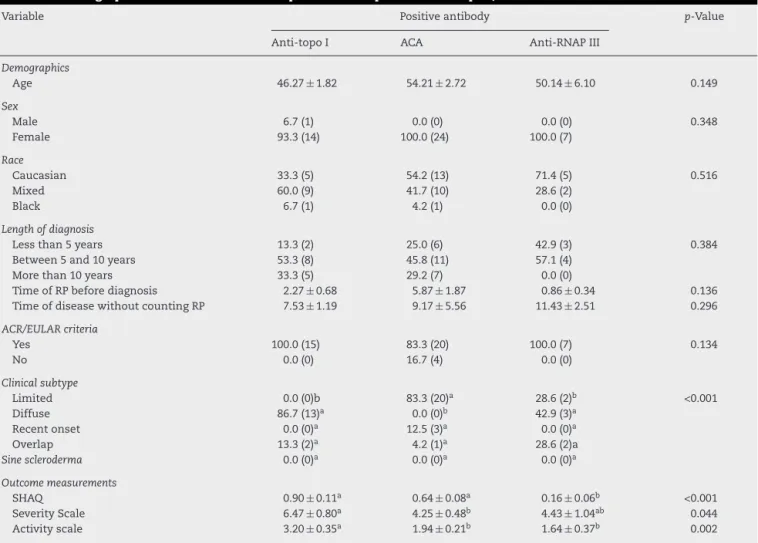
Resultsregardingsocio-demographicandclinical parame-tersinpatientswithpositiveACA,anti-topoIoranti-RNAPIII, arepresentedinTable1.
Therewasnosignificantdifferencebetweenpatientswith positiveanti-topoI,ACAoranti-RNAPIIIantibodiesinrelation tothequantitativevariablesage,durationofRPbefore diag-nosis,anddurationofillnesswithoutcountingRP.Moreover, SHAQofpatientswithpositiveanti-topo Iwassignificantly higherthanthatforpatientswithpositiveACAoranti-RNAP
0.0% n = 0
86.7% n = 13
0.0% n = 0
13.3% n = 2 83.3%
n = 20
0.0 n=0
12.5% n = 3
4.2% n = 1 28.6%
n = 2
42.9% n = 3
0.0% n = 0
28.6% n = 2
0.0 10.0 20.0 30.0 40.0 50.0 60.0 70.0 80.0 90.0 100.0 Overlap Recent onset Diffuse Limited
Percentage of patients (%)
Clinical subtype anti-SCL70 ACA anti-POL3
*
**
Positive antibodyFig.1–Percentageofpatientswithpositiveantibodyto anti-topoI,ACAandanti-RNAPIIIamongpatientswith differentclinicalsubtypesofthedisease.Eachcolumn representsthepercentofpatients.*Significantdifference comparedtopatientswithpositiveanti-topoIand anti-RNAPIII,inlimitedscleroderma.**Significant differencecomparedtopatientswithpositiveACA,in diffusescleroderma(chi-squaretest;p<0.050).
IIIantibody(p<0.05).Thesameresultwasobservedinrelation tothescaleofactivity.Moreover,SHAQamongpatientswith positiveACAoranti-topoIwashigherthanthatforpatients withpositiveanti-RNAPIIIantibody(p<0.05).
Forthescaleofseverity,thescoreamongpatientswith pos-itive anti-topoIantibodywashigherthan thatforpatients withpositiveACAantibody(p<0.05),butwithnodifference for patients with positive anti-RNAP III antibody (p>0.05). Therewasnofurtherassociationbetweenpositiveanti-topo I, ACA or anti-RNAP III antibodies and nominal or ordinal qualitativevariablesofgender,race,timesincediagnosisand 2013ACR/EULARclassificationcriteriaforSSc.However,there wasanassociationbetweenpositiveanti-topoI,ACAor anti-RNAPIII antibodiesand the clinicalsubtypeofthe disease (p<0.001),withthe percentageofpatientswithlimited dis-easeamongpatientswithpositiveACAantibody(83,3%,n=20) beingsignificantlyhigherthanthatamongpatientswith pos-itive anti-topo Iand anti-RNAPIIIantibody(0.0%,n=0and 28.6%,n=2,respectively).Ontheotherhand,thepercentage ofpatients withdiffusedisease,among patientswith pos-itive anti-topo I andanti-RNAP III(86.7%, n=13 and42.9%,
n=3),respectively,wassignificantlyhigherthanthatamong patientswithpositiveACA(0.0%,n=0)antibody.
Table2showstheresultsfortheskin,vascularand
mus-culoskeletalmanifestationsinpatientswithapositiveresult foranti-topoI,ACAandanti-RNAPIIIantibodies.Inthis eval-uation,itwasobservedthatthepercentageofpatientswith positiveanti-topoIantibody,whichhadobjectiveRP(93.3%,
Table1–Demographicandclinicalfeaturesofpatientswithpositiveanti-topoI,ACAoranti-RNAPIIIantibodies.
Variable Positiveantibody p-Value
Anti-topoI ACA Anti-RNAPIII
Demographics
Age 46.27±1.82 54.21±2.72 50.14±6.10 0.149
Sex
Male 6.7(1) 0.0(0) 0.0(0) 0.348
Female 93.3(14) 100.0(24) 100.0(7)
Race
Caucasian 33.3(5) 54.2(13) 71.4(5) 0.516
Mixed 60.0(9) 41.7(10) 28.6(2)
Black 6.7(1) 4.2(1) 0.0(0)
Lengthofdiagnosis
Lessthan5years 13.3(2) 25.0(6) 42.9(3) 0.384
Between5and10years 53.3(8) 45.8(11) 57.1(4)
Morethan10years 33.3(5) 29.2(7) 0.0(0)
TimeofRPbeforediagnosis 2.27±0.68 5.87±1.87 0.86±0.34 0.136 TimeofdiseasewithoutcountingRP 7.53±1.19 9.17±5.56 11.43±2.51 0.296
ACR/EULARcriteria
Yes 100.0(15) 83.3(20) 100.0(7) 0.134
No 0.0(0) 16.7(4) 0.0(0)
Clinicalsubtype
Limited 0.0(0)b 83.3(20)a 28.6(2)b <0.001
Diffuse 86.7(13)a 0.0(0)b 42.9(3)a
Recentonset 0.0(0)a 12.5(3)a 0.0(0)a
Overlap 13.3(2)a 4.2(1)a 28.6(2)a
Sinescleroderma 0.0(0)a 0.0(0)a 0.0(0)a
Outcomemeasurements
SHAQ 0.90±0.11a 0.64±0.08a 0.16±0.06b <0.001
SeverityScale 6.47±0.80a 4.25±0.48b 4.43±1.04ab 0.044
Activityscale 3.20±0.35a 1.94±0.21b 1.64±0.37b 0.002
Theresultsarepresentedasmean±standarderrorofthemeanorrelativefrequency(absolutefrequency).
p-Valueinone-wayANOVAorchi-squaretest.
Differentletteronlinesindicatesignificantdifferenceamongantibodies.
ACA,anticentromereantibodies;anti-topoI,anti-DNAtopoisomeraseIantibodies;anti-RNAPIII,antiRNApolymeraseIIIantibodies;RP, Ray-naud’sphenomenon;ACR,AmericanCollegeofRheumatology;EULAR,EuropeanLeagueAgainstRheumatism;SHAQ,SclerodermaHealth AssessmentQuestionnaire.
patientswithpositiveanti-topoIantibody,whichalsoshowed subjectiveRP(6.7%,n=1).
Patientswithpositiveanti-topoIantibodyshowedmore digitalpittingscarsoffingertipsthanpatientswithpositive ACAantibody(p<0.05).Furthermore,patientswithpositive ACA antibody had more telangiectasia than patients with positiveanti-topoIantibody(p<0.050).Furthermore,patients withpositiveanti-RNAPIIIantibodyhadmoremuscle atro-phythanpatientswithpositiveACAantibody(p<0.050).These resultsarepresentedinFig.2.Fortheothervariablesrelatedto skin,vascularandmusculoskeletalmanifestations,therewas noassociationbetweenthemandthepositivityforanti-topo I,ACAandanti-RNAPIIIantibodies.There wasalsono sig-nificantdifferencebetweenpatientswithpositivityforthese threeantibodiesinrelationtoskinscore(p=0.065).
Theresults relatedto gastrointestinal,cardiopulmonary andrenalmanifestationsinpatientswithpositiveanti-topo I,ACAoranti-RNAPIIIarepresentedinTable3.Therewasno associationbetweenthepresenceofautoantibodiesspecific forSScandthevariablesstudied.
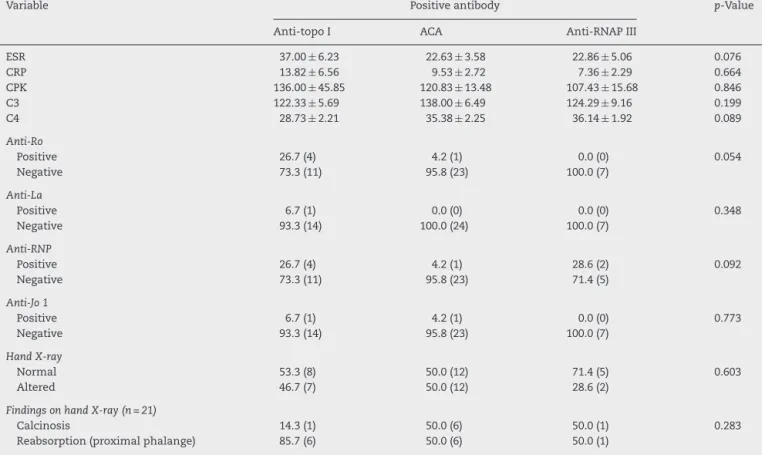
Theresultsofthe laboratorytests(ESR,CRP,CPK, creat-inine, C3andC4),antibodytests(anti-Ro,anti-La,anti-Sm, anti-RNPandantiJo-1)andchangesobservedonhand radio-graphs in patients with positive anti-topo I, ACA and/or anti-RNAPIIIantibodiesareshowninTable4,wherealack ofstatisticalsignificanceforallthestudiedparameterscanbe seen.
Discussion
Inourstudy,aunique samplewasdefinedthatwas repre-sentativeoftheMidwestregionofBrazil,characterizedbya heterogeneousgroupofpatientswithvarious spectrumsof disease and differentstages ofclinical manifestations and diseaseactivity,butthatisverysimilartootherpatient popu-lationsinthecountryandevenfromotherlocations.33–38
Table2–Distributionofpatientsaccordingtotheskin,vascularandmusculoskeletalmanifestationsinpatientswith positiveanti-topoI,ACAoranti-RNAPIIIantibodies.
Variable Positiveantibody p-Value
Anti-topoI ACA Anti-RNAPIII
Skinmanifestations
Calcinosis
Yes 20.0(3) 25.0(6) 14.3(1) 0.817
No 80.0(12) 75.0(18) 85.7(6)
Hands
Nochanges 13.3(2) 20.8(5) 28.6(2) 0.685
Withchanges 86.7(13) 79.2(19) 71.4(5)
Findingsonhands(n=37)
Edematousphase 15.4(2) 36.8(7) 20.0(1) 0.735
Indurativephase 46.2(6) 31.6(6) 40.0(2)
Atrophicphase 38.5(5) 31.6(6) 40.0(2)
Skinscore(Rodnanmodified) 16.33±2.03 10.79±1.30 13.86±2.80 0.065
Vascularmanifestations
RP
Objective 93.3(14)a 66.7(16)ab 42.9(3)b 0.036
Subjective 6.7(1)b 33.3(8)ab 57.1(4)a
Absent 0.0(0) 0.0(0) 0.0(0)
Digitalpittingscarsoffingertips
Yes 53.3(8)a 16.7(4)b 14.3(1)ab 0.031
No 46.7(7)b 83.3(20)a 85.7(6)ab
Activeulcers
Yes 20.0(3) 8.3(2) 0.0(0) 0.316
No 80.0(12) 91.7(22) 100.0(7)
Necrosisoramputation
Yes 13.3(2) 12.5(3) 0.0(0) 0.602
No 86.7(13) 87.5(21) 100.0(7)
Telangiectasias
Yes 53.3(8)b 87.5(21)a 57.1(4)ab 0.045
No 46.7(7)a 12.5(3)b 42.9(3)ab
Musculoskeletalmanifestations
Arthritis/synovitis
Yes 40.0(6) 37.5(9) 0.0(0) 0.134
No 60.0(9) 62.5(15) 100.0(7)
Flexioncontracture
Yes 26.7(4) 8.3(2) 14.3(1) 0.300
No 73.3(11) 91.7(22) 85.7(6)
Tendonfrictionrubs
Yes 6.7(1) 4.2(1) 0.0(0) 0.773
No 93.3(14) 95.8(23) 100.0(7)
Muscleweakness
Yes 20.0(3) 8.3(2) 28.6(2) 0.347
No 80.0(12) 91.7(22) 71.4(5)
Atrophy
Yes 6.7(1)ab 4.2(1)b 42.9(3)a 0.012
No 93.3(14)ab 95.8(23)a 57.1(4)b
Theresultsarepresentedasmean±standarderrorofthemeanorrelativefrequency(absolutefrequency).
p-Valueinone-wayANOVAorchi-squaretest.
Differentletteronlinesindicatesignificantdifferenceamongantibodies.
Table3–Distributionofpatientsaccordingtogastrointestinal,cardiopulmonaryandrenalmanifestationsinpatients withpositiveanti-SCL70,ACAoranti-POL3.
Variable Positiveantibody p-Value
Anti-topoI ACA Anti-RNAPIII
Gastrointestinalmanifestations
Esophagusinvolvement
Yes 73.3(11) 70.8(17) 57.1(4) 0.730
No 26.7(4) 29.2(7) 42.9(3)
OtherGImanifestations
GERD 26.7(4) 16.7(4) 0.0(0) 0.304
Esophagitis 20.0(3) 16.7(4) 42.9(3) 0.329
Gastritis 13.3(2) 20.8(5) 14.3(1) 0.812
Esophagichypotonia 20.0(3) 25.0(6) 0.0(0) 0.340
Esophagealdilation 6.7(1) 4.2(1) 14.3(1) 0.634
Cardiopulmonarymanifestations
VFC 76.27±3.27 86.50±2.56 83.71±4.47 0.054
VFC–classification
>80% 40.0(6) 70.8(17) 42.9(3) 0.282
Between70and80% 40.0(6) 20.8(5) 57.1(4)
Between50and69% 13.3(2) 8.3(2) 0.0(0)
<50% 6.7(1) 0.0(0) 0.0(0)
ChestCT
Normal 26.7(4) 62.5(15) 42.9(3) 0.089
Altered 73.3(11) 37.5(9) 57.1(4)
FindingsonCT(n=24)
Fibrosis 72.7(8) 66.7(6) 75.0(3) 0.938
“Ground-glass”pattern 27.3(3) 33.3(3) 25.0(1)
EchoPSAP 32.50±5.50 37.25±3.64 32.67±12.25 0.882
Echocardiogram(n=26)
Normal 40.0(6) 54.2(13) 14.3(1) 0.164
Altered 60.0(9) 45.8(11) 85.7(6)
Findingsonechocardiogram
Valvulopathy 33.3(5) 25.0(6) 28.6(2) 0.854
ConcentricLVH 20.0(3) 12.5(3) 28.6(2) 0.583
LVdiastolicdysfunction 6.7(1) 16.7(4) 28.6(2) 0.395
MildormoderatePAH 6.7(1) 8.3(2) 28.6(2) 0.260
Pericarditis 13.3(2) 12.5(3) 0.0(0) 0.602
Renalmanifestations
Renalcrisis
Yes 0.0(0) 0.0(0) 0.0(0) –
No 100.0(15) 100.0(24) 100.0(7)
Theresultsarepresentedasmean±standarderrorofthemeanorrelativefrequency(absolutefrequency).
p-Valueinone-wayANOVAorchi-squaretest.
ACA,anticentromereantibodies;anti-topoI,anti-DNAtopoisomeraseIantibodies;anti-RNAPIII,anti-RNApolymeraseIIIantibodies;GI, gas-trointestinal;GERD,gastroesophagealrefluxdisease;VFC,vitalfunctionalcapacity;CT,computedtomography;EchoPSAP,pulmonaryartery estimatedpressurebytransthoracicechocardiogram;LVH,leftventriclehypertrophy;LV,leftventricle;PAH,pulmonaryarteryhypertension.
otherpopulations,ourpatientsweremostlyfemale(97.83%) andwithlimitedscleroderma(47.8%),withameanageof50 yearsandcaucasian(50.0%).In65%ofthepatients,RPwasthe firstdiseasemanifestationbeforediagnosis,timesince diag-nosisoccurredmainlybetween5and10years(50.0%),mean disease duration of9 years,and average modified Rodnan skinscoreof13.66.Regardingspecificantibodies,52.2%ofthe patientshadpositiveACA,32.6%werepositiveforanti-topoI and15.2%werepositiveforanti-RNAPIII.
InBrazil,recentlytwodifferentgroupsofresearchersinthe southernregion described theoccurrenceofmajor specific
autoantibodiesinpatientswithSScandbothauthors high-lightedtheimportanceofautoantibodiesintheevaluationof patientswithSSc.33,34
ThefirstgroupfromHospitalEvangélicodeCuritiba(HUEC) found, in66 SScpatients, theprevalenceofACA,anti-topo I and anti-U1-RNP, respectively in 33.3%,17.8% and 11.8% ofpatients.33Althoughthepercentageofeachautoantibody
Table4–Distributionofpatientsaccordingtothelaboratorytestsinpatientswithanti-topoI,ACAoranti-RNAPIII positive.
Variable Positiveantibody p-Value
Anti-topoI ACA Anti-RNAPIII
ESR 37.00±6.23 22.63±3.58 22.86±5.06 0.076
CRP 13.82±6.56 9.53±2.72 7.36±2.29 0.664
CPK 136.00±45.85 120.83±13.48 107.43±15.68 0.846
C3 122.33±5.69 138.00±6.49 124.29±9.16 0.199
C4 28.73±2.21 35.38±2.25 36.14±1.92 0.089
Anti-Ro
Positive 26.7(4) 4.2(1) 0.0(0) 0.054
Negative 73.3(11) 95.8(23) 100.0(7)
Anti-La
Positive 6.7(1) 0.0(0) 0.0(0) 0.348
Negative 93.3(14) 100.0(24) 100.0(7)
Anti-RNP
Positive 26.7(4) 4.2(1) 28.6(2) 0.092
Negative 73.3(11) 95.8(23) 71.4(5)
Anti-Jo1
Positive 6.7(1) 4.2(1) 0.0(0) 0.773
Negative 93.3(14) 95.8(23) 100.0(7)
HandX-ray
Normal 53.3(8) 50.0(12) 71.4(5) 0.603
Altered 46.7(7) 50.0(12) 28.6(2)
FindingsonhandX-ray(n=21)
Calcinosis 14.3(1) 50.0(6) 50.0(1) 0.283
Reabsorption(proximalphalange) 85.7(6) 50.0(6) 50.0(1)
Theresultsarepresentedasmean±standarderrorofthemeanorrelativefrequency(absolutefrequency).
p-Valueinone-wayANOVAorchi-squaretest.
ACA,anticentromereantibodies;anti-topoI,anti-DNAtopoisomeraseIantibodies;anti-RNAPIII,antiRNApolymeraseIIIantibodies;ESR, erythrocytesedimentationrate;CRP,C-reactiveprotein;CPK,creatinephosphokinase;C3,C3complementcomponent;C4,C4complement component.
fingertips;however,theyfoundanassociationbetweenthis autoantibodyandthepresenceofcardiomyopathy.Unlikeour study,ACAwasprotectiveforcardiomyopathiesand anti-U1-RNPwasmorecommoninoverlapforms.33
Thesecond groupfrom Hospitalde Clínicas ofthe Fed-eralUniversityofthestateofParaná(HC-UFPR)investigated the prevalenceofanti-RNAP III, anti-topo I and ACA in85 SScpatientsandfoundtheirpresencein41.18%;31.76%and 30.59%ofpatients,respectively.34Althoughitwasnotedthat
thelimitedformwasthemostprevalentamongpatients,this study foundveryhigh prevalenceofpositiveanti-RNAPIII, whichisrelatedtodiffusecutaneousSSc.Ourstudyhas val-idated the same clinical featuresobserved inthe group of patientsfromHC-UFPRwhowereanti-topoI-positive,suchas associationwithdiffusescleroderma,thepresenceofactive diseaseanddigitalulcers.However,thegroupfromHC-UFPR foundanassociationbetweensynovitisandpositivityfor anti-RNAPIII,andgreaterprevalenceofsystemichypertensionand cardiacconductionblockinpatientswithpositiveACA.34
In the present work, ACA was mainly correlated with limitedcutaneousSSc,withearlieronsetofdisease,aswellas higherprevalenceoftelangiectasias.ACAwasfoundin52.2% ofpatientsand,intheliterature,ACAswereobservedinabout 20–30%ofpatientswithSSc10,12andin55–80%ofpatientswith
thelimitedform9,althoughitcanvaryamongdifferentethnic
populations.10,12ACAshavepredictivevalueforfuture
devel-opmentofSScinpatientswithRPandare associatedwith limitedcutaneousinvolvement,peripheralvasculardamage and calcinosis.10,12 However,nogreaterprevalenceof
calci-nosisinourpatientswiththelimitedformwasobserved.The presenceofACAgenerallyprovidesabetterprognosisthan thatseenwithotherantibodies,sincetheyarelessfrequently associatedwithinterstitiallungfibrosis,10,12asobservedinour
study,althoughnotachievingstatisticalsignificance. Inthisstudy,theanti-topoIautoantibodywasmainly cor-relatedwiththediffusecutaneousSSc,withgreaterdisease severityandactivity,withworsequalityoflifeasmeasured by SHAQ index, a higher prevalence of objective RP, and digital pitting scars of fingertips. We found anti-topo I in 32.6% ofpatients, in accordancewith the literature,which describesthisantibodyin40%ofpatientswithSSc,12inabout
28–70%patientswiththediffusecutaneousSSc9,10,12andin
less than 10% ofpatients withlimited scleroderma.9–11 As
observed inour patients, it isdescribed that ethnic differ-ences significantlyaffectthe prevalenceofanti-topo I, and it is observed to a lesser extent in Caucasians. Anti-topo I, when determined byimmunodiffusion,is virtuallynever seeninhealthyindividuals,inotherdiseasesofthe connec-tivetissue,orinpatientswithprimaryRP.10,12Itspresenceis
0 10 20 30 40 50 60 70 80 90 100
Muscle atrophy Telangiectasias
Digital pitting scars of fingertips
Percentage of patients (%)
Clinical feature
anti-SCL70
ACA anti-POL3 Antibody
positive
*
**
***
Fig.2–Percentageofpatientswithclinicalmanifestations suchasdigitalpittingscarsoffingertips,telangiectasias andmuscleatrophy,amongpatientswithpositive
anti-topoI,ACAandanti-RNAPIII.Eachcolumnrepresents thepercentofpatients.*Significantdifferencecomparedto patientswithpositiveACAandanti-RNAPIII.**Significant differencecomparedtopatientswithpositiveanti-topoI andanti-RNAPIII.***Significantdifferencecomparedto patientswithpositiveanti-topoIandACA(chi-squaretest;
p<0.050).
severity of skin involvement, interstitial lung disease and cardiac involvement.9,10,12,39–41 However, cardiopulmonary
manifestationswerenotmoreprevalentormoresevereinthis study.
However,inthiswork,theanti-RNAPIIIwasprimarily cor-related with diffusescleroderma, since other two patients withinflammatorymyopathy-associatedpositiveanti-RNAP III had diffuse cutaneous involvement. Interestingly, both patientswithoverlapwerenotpositiveforanti-Jo1antibody. Moreover,weobservedahigher frequencyofsubjective RP andmuscleatrophyinourpatients.Wefoundanti-RNAPIII in15.2% ofpatients, but other published studiesdescribes aprevalenceofthisantibodyatdifferentfrequencies, prob-ablyrelatedtogeneticandracialdifferences.Itsprevalence rangedfrom4to9.4%inFrench,12%inEnglish,6%inJapanese, 19.4%inCanadian,and25%inAmericanpatients.9,42
Autoan-tibodiesagainstRNApolymerase1and3usuallycoexist in aprevalenceof20%,and this pattern ishighlyspecific for SSc.9,10,12Anti-RNAPIIIalsohasaprognosticrole,sinceitwas
relatedtodiffuseskininvolvement,tendonfrictionrubs,and kidneyinvolvement,9,42,43butnosclerodermarenalcrisiswas
observedinour patients. Besides myositisobservedinour patients,studiespublishedintheliteraturehighlightsother significantassociationsbetweenthepositivityofanti-RNAPIII withtheoccurrenceofsynovitisandsystemichypertension, aswellasapossiblerelationtomalignancies,predominantly solidorgancancer.42,43
Unlikesystemiclupuserythematosus(SLE),theproduction ofaspecificautoantibodyisuniqueinpatientswithSSc,so theoccurrenceofmorethanonetypeofantibodyinapatient israre,exceptforantibodies againstRNApolymerase.9,10,12
Thecoexistenceofanti-topoIandACAinSScisuncommon (0.5–5.5%), although some authors have previously consid-ereditmutuallyexclusive.44Althoughthecorrelationbetween
antibodiesthatdefinesubtypesofSScisunusual,the coexis-tenceofACAoranti-topoIwithanti-histoneantibodies,ACA withanti-mitochondrialantibodies,anti-topoIwith anticardi-olipinantibodies,ACAoranti-topoIwithRo(SSA)antibodies, orantiRNPswithantiTh/Toantibodieswasdescribed.45Our
studyobservedthecoexistenceofpositiveanti-topoIand anti-RNAPIIIinapatientwithdiffusescleroderma.
BasedonSHAQ,thisstudyobservedhigherscoresof dis-abilityamongpatientswithpositivityofanti-topoI,similar tothosedescribedinotherpopulationsofpatientswiththe diffuseformofSSc.29,46Comparatively,Moritaandcolleagues
reportedthatpatientswiththediffuseformofSSchadhigher rates of disability on the SHAQ, also higher than those of patientswithRA,SLEand otherautoimmune diseases.46 It
wasalsoobservedthatSScpatientswitharticularinvolvement hadhigherscoresonSHAQthanpatientswithpsoriatic arthri-tis,whilethepain domainwashigherinSSc patientsthan inRApatients.47 Unpublished dataofourpatientsconfirm
thegreaterdisabilityinthesubgroupofpatientswith arthri-tis.RecentlyIudiciand colleaguesfoundthatpatientswith earlyformofSSc,despitehavingonlyRP,hadalready expe-riencedanimpairmentofqualityoflifeinbothphysicaland mentaldomains.48Accordingly,our3patientswiththeearly
formshowedadisabilityindexmeasuredbytheSHAQthat wascomparabletoothergroups.TheusefulnessofSHAQin theevaluationofpatientswithSSchasbeendemonstratedby studiesthatreportedthatitcanpredicttheevolutionand sur-vivalinthesepatients.29,49Inthiswork,therewasasignificant
positivelinearcorrelationbetweenSHAQanddisease activ-ityasmeasuredbythePearsontest.Medsgerandcolleagues foundthattheratesofdisabilitymeasuredbySHAQshowed strongcorrelationwithskinthickening,cardiacinvolvement, digitalcontractures,tendonfrictionrubs,andrenal involve-mentin1000patientswithSSc.26
Inconclusion, thisstudy confirmsthe importantroleof specificautoantibodiesintheevaluationofpatientswithSSc. Itispossibletocorrelatetheantibodyprofileofthisnational populationwithsomedistinctclinicalmanifestationsofthe disease.
Conclusions
Wehighlight,inagreementwiththeliterature,thatthe clin-icalsubtypeofthediseaseandsomeclinicalmanifestations inSScmaycorrelatepositivelywiththepresenceofspecific autoantibodies.
ThepresenceofACAwasobserved,particularlyintheearly formsofthedisease,limitedscleroderma,andoverlap syn-drome,withabsenceinthediffusescleroderma.Theanti-topo Iwasmainlyobservedinthediffuseandoverlapforms,being absentinthelimiteddisease.
Patientswithpositiveanti-topoIhavehigherdisease activ-ityandseverity,andimpairmentinqualityoflifeasmeasured bySHAQindex.
moretelangiectasiaandpatientswithpositiveanti-RNAPIII antibodyhadmoremuscleatrophy.
Thespecificautoantibodiesmaydirectlycontributetothe patient’sevolutionandprognosis.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
Theauthors thanktheircolleaguesDrLuisEduardo Coelho AndradeandDr.CristianeKayserforhelpinginthe perfor-manceofanti-RNAPolymeraseIIItests,andtoDr.Natalino Yoshinariforhisgreatincentivetotheirresearch.
r
e
f
e
r
e
n
c
e
s
1. VargaJ,AbrahamD.Systemicsclerosis:aprototypic
multisystemfibroticdisorder.JClinInvest.2007;117:557–67.
2. HerrickAL,WorthingtonJ.Geneticepidemiologysystemic
sclerosis.ArthritisRes.2002;4:165–8.
3. Coral-AlvaradoP,PardoAL,Casta ˜no-RodriguezN,
Rojas-VillarragaA,AnayaJM.Systemicsclerosis:aworldwide
globalanalysis.ClinRheumatol.2009;28:757–65.
4. BeyerC,SchettG,GayS,DistlerO,DistlerJHW.Hypoxiainthe
pathogenesisofsystemicsclerosis.ArthritisResTher.
2009;11:220.
5. AbrahamDJ,KriegT,DistlerJ,DistlerO.Overviewof
pathogenesisofsystemicsclerosis.Rheumatology.
2009;48:iii3–7.
6. LafyatisR,YorkM.Innateimmunityandinflammationin
systemicsclerosis.CurrOpinRheumatol.2009;21:617–22.
7. KraaijMD,VanLaarJM.TheroleofBcellsinsystemic
sclerosis.Biologics.2008;2:389–95.
8. ZimmermannAF,PizzichiniMMM.Atualizac¸ãona
etiopatogênesedaesclerosesistêmica.RevBrasReumatol.
2013;53:516–24.
9. AndradeLEC,LeserPG.Autoanticorposnaesclerose
sistêmica(ES).RevBrasReumatol.2004;44:215–23.
10.HoKT,ReveilleJD.Theclinicalrelevanceofautoantibodiesin
scleroderma.ArthritisResTher.2003;5:80–93.
11.MouthonL,Pe ˜na-LefebvrePGL,ChanseaudY,TambyMC,
BoissierMC,GluillevinL.Sclérodermie(1repartie).AnnMed
Interne.2002;153:167–78.
12.HamaguchiY.Autoantibodyprofilesinsystemicsclerosis:
predictivevalueforclinicalevaluationandprognosis.J
Dermatol.2010;37:42–53.
13.SalojinKV,TonquèzeML,SarauxA,NassonovEL,DueymesM,
PietteJC,etal.Antiendothelialcellantibodies:usefulmarkers
ofsystemicsclerosis.AmJMed.1997;102:178–85.
14.BaroniSS,SantilloM,BevilacquaF,LuchettiM,SpadoniT,
ManciniM,etal.StimulatoryautoantibodiestothePDGF
receptorinsystemicsclerosis.NEnglJMed.2006;354:2667–76.
15.MayersMD,TrojanowskaM.Geneticfactorsinsystemic sclerosis.ArthritisResTher.2007;9(2):S5,
http://dx.doi.org/10.1186/ar2189.
16.RomanoE,ManettiM,GuiducciS,CeccarelliC,AllanoreY,
Matucci-CerinicM.Thegeneticsofsystemicsclerosis:an
update.ClinExpRheumatol.2011;29:S75–86.
17.Feghali-BostwickCA,WilkesDS.Autoimmunityinidiopathic
pulmonarfibrosis.Arecirculatingautoantibodiespathogenic
orepiphenomena?AmJRespCritCareMed.2011;183:692–3.
18.GabrielliA,SvegliatiS,MoronciniG,AvvedimentoEV.
Pathogenicautoantibodiesinsystemicsclerosis.CurrOpin
Immunol.2007;19:640–5.
19.VilasAP,VeigaMZ,AbecasisP.Esclerosesistémica–
perspectivasactuais.MedInterna.2002;9:111–20.
20.FreireEAM,CiconelliRM,Sampaio-BarrosPD.Análisedos
critériosdiagnósticos,declassificac¸ão,atividadeegravidade
dedoenc¸anaesclerosesistêmica.RevBrasReumatol.
2004;44:40–5.
21.SatoS,HamaguchiY,HasegawaM,TakeharaK.Clinical
significanceofanti-topoisomeraseIantibodylevels
determinedbyElisainsystemicsclerosis.Rheumatology.
2001;40:1135–40.
22.SharpGC,IrvinWS,LaRoqueRL,VelezC,DalyV,KaiserAD,
etal.Associationofautoantibodiestodifferentnuclear
antigenswithclinicalpatternsofrheumaticdiseaseand
responsivenesstotherapy.JClinInvest.1971;50:350–9.
23.HoogenF,KhannaD,FransenJ,JohnsonSR,BaronM,Tyndall
A,etal.2013classificationcriteriaforsystemicsclerosis:an
AmericanCollegeofRheumatology/EuropeanLeagueAgainst
Rheumatismcollaborativeinitiative.AnnRheumDis.
2013;72:1747–55.
24.LeRoyEC,MedsgerTAJr.Criteriafortheclassificationofearly
systemicsclerosis.JRheumatol.2001;28:1573–6.
25.ValentiniG,D’AngeloS,RossaAD,BencivelliW,Bombardieri
S.EuropeanSclerodermaStudyGrouptodefinedisease
activitycriteriaforsystemicsclerosis.IV.Assessmentofskin
thickeningbymodifiedRodnanskinscore.AnnRheumDis.
2003;62:904–5.
26.MedsgerTAJr.Naturalhistoryofsystemicsclerosisandthe
assessmentofdiseaseactivity,severity,functionalstatus,and
psychologicwell-being.RheumDisClinNAm.2003;29:
255–73.
27.ValentiniG,SilmanAJ,VealeD.Assessmentofdisease
activity.ClinExpRheumatol.2003;21:S39–41.
28.RannouF,PoiraudeauS,BereznéA,BaubetT,Le-GuernV,
CabaneJ,etal.Assessingdisabilityandqualityoflifein
systemicsclerosis:constructvaliditiesoftheCochinhand
functionscale,healthassessmentquestionnaire(HAQ),
systemicsclerosisHAQ,andmedicaloutcomesstudy36-item
shortformhealthsurvey.ArthritisRheum.2007;57:
94–102.
29.GeorgesC,ChassanyO,MouthonL,TievK,ToledanoC,Meyer
O,etal.ValidationofFrenchversionoftheScleroderma
HealthAssessmentQuestionnaire(SScHAQ).ClinRheumatol.
2005;24:3–10.
30.XinyiNG,ThumbooJ,LowAHL.Validationofthescleroderma
healthassessmentquestionnaireandqualityoflifeinEnglish
andChinese-speakingpatientswithsystemicsclerosis.IntJ
RheumDis.2012;15:268–76.
31.DellavanceA,GabrielAJr,CintraAFU,XimenesAC,Nuccitelli
B,TabilertiBH,etal.IIConsensoBrasileirodeFator
AntinuclearemcélulasHep-2.RevBrasReumatol.
2003;43:129–40.
32.CodulloV,MorozziG,BardoniA,SalviniR,DeleonardiG,Pità
O,etal.Validationofanewimmunoenzymaticmethodto
detectantibodiestoRNApolymeraseIIIinsystemicsclerosis.
ClinExpRheumatol.2007;25:373–7.
33.SkareTL,LucianoAC,FonsecaAE,AzevedoPM.
Autoanticorposemesclerodermiaesuaassociac¸ãoaoperfil
clínicodadoenc¸a.Estudoem66pacientesdosuldoBrasil.An
BrasDermatol.2011;86:1075–81.
34.MüllerCS,PaivaES,AzevedoVF,RadominskiSC,LimaFilho
JHC.Perfildeautoanticorposecorrelac¸ãoclínicaemum
grupodepacientescomesclerosesistêmicanaregiãoSuldo
Brasil.RevBrasReumatol.2011;51:319–24.
35.HunzelmannN,GenthE,KriegT,LehmacherW,MelchersI,
systemicscleroderma:frequencyofdiseasesubsetsand
patternsoforganinvolvement.Rheumatology.
2008;47:1185–92.
36.FerriC,ValentiniG,CozziF,SebastianiM,MichelassiC,La
MontagnaG,etal.Systemicsclerosis:demographic,clinical,
andserologicfeaturesandsurvivalin1012Italianpatients.
Medicine(Baltimore).2002;81:139–53.
37.Sampaio-BarrosPD,BortoluzzoAB,MarangoniRG,RochaLF,
DelRioAPT,SamaraAM,etal.Survival,causesofdeath,and
prognosticfactorsinsystemicsclerosis:analysisof947
Brazilianpatients.JRheumatol.2012;39:1971–8.
38.GuidolimF,EsmanhottoL,MagroCE,SilvaMB,SkareTL.
Prevalênciadeachadoscutâneosemportadoresdeesclerose
sistêmica–Experiênciadeumhospitaluniversitário.AnBras
Dermatol.2005;80:481–6.
39.HuPQ,FertigN,MedsgerTJr,WrightTM.Correlationof
serumanti-DNAtopoisomeraseIantibodylevelswithdisease
severityandactivityinsystemicsclerosis.ArthritisRheum.
2003;48:1363–73.
40.HénaultJ,RobitailleG,SenécalJL,RaymondY.DNA
topoisomeraseIbindingtofibroblastosinducesmonocyte
adhesionandactivationinthepresenceof
anti-topoisomeraseIautoantibodiesfromsystemicsclerosis
patients.ArthritisRheum.2006;54:963–73.
41.HuPQ,HurwitzAA,OppenheimJJ.ImmunizationwithDNA
topoisomeraseIinducesautoimmuneresponsesbutnot
scleroderma-likepathologiesinmice.JRheumatol.
2007;34:2243–52.
42.NikpourM,HissariaP,ByronJ,SahharJ,MicallefM, PaspaliarisW,etal.Prevalence,correlatesandclinical usefulnessofantibodiestoRNApolymeraseIIIinsystemic sclerosis:across-sectionalanalysisofdatafroman
Australiancohort.ArthritisResTher.2011;13:R211
http://arthritis-research.com/content/13/6/R211
43.VanthuyneM,SmithV,DeLangheE,PraetJV,AratS,
DepresseuxG,etal.TheBelgiansystemicsclerosiscohort:
correlationsbetweendiseaseseveritysclores,cutaneous
subsets,andautoantibodyprofile.JRheumatol.
2012;39:2127–33.
44.RascoRG,PalmaMJC,HernándezFJG,RománJS.Coexistencia
deanticuerposanti-topoisomeraseIyanticentrômeroemla
esclerodermia.MedClín(Barc).2010;135:430–1.
45.DickT,MierauR,Bartz-BazzanellaP,AlaviM,
Stoyanova-ScholzM,KindlerJ,etal.Coexistenceof
anti-topoisomeraseIandanticentromereantibodiesin
patientswithsystemicsclerosis.AnnRheumDis.
2002;61:121–7.
46.MoritaY,MuroY,SugiuraK,TomitaY,TamakoshiK.Results
oftheHealthAssessmentQuestionnaireforJapanese
patientswithsystemicsclerosis–Measuringfunctional
impairmentinsystemicsclerosisversusotherconnective
tissuediseases.ClinExpRheumatol.2007;25:367–72.
47.PopeJ.Measuresofsystemicsclerosis(Scleroderma).Arthritis
CareRes.2011;63(S11):S98–111.
48.IudiciM,CuomoG,VettoriS,AvellinoM,ValentiniG.Quality oflifeasmeasuredbytheshort-form36(SF-36)questionnaire inpatientswithearlysystemicsclerosisandundifferentiated connectivetissuedisease.HealthQualLifeOut.2013;11:23
http://www.hqlo.com/content/11/1/23
49.DanieliE,AiròP,BettoniL,CinquiniM,AntonioliCM,
CavazzanaI,etal.Health-relatedqualityoflifemeasuredby
theShortForm36(SF-36)insystemicsclerosis:correlations
withindexesofdiseaseactivityandseverity,disability,and