w w w . r e u m a t o l o g i a . c o m . b r
REVISTA
BRASILEIRA
DE
REUMATOLOGIA
Original
article
Overlap
between
systemic
sclerosis
and
rheumatoid
arthritis:
a
distinct
clinical
entity?
Alex
Magno
Coelho
Horimoto
a,∗,
Izaias
Pereira
da
Costa
a,b aUniversidadeFederaldeMatoGrossodoSul,CampoGrande,MS,BrazilbUniversidadedeSãoPaulo,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received24May2014
Accepted23December2014
Availableonline13July2015
Keywords:
Systemicsclerosis
Rheumatoidarthritis
Overlap Anticitrulin
Rheumatoidfactor
a
b
s
t
r
a
c
t
Introduction:Systemicsclerosis(SSc)isanautoimmunediseaseoftheconnectivetissue
char-acterizedbythetriadofvascularinjury,autoimmunity(cellularandhumoral)andtissue
fibrosis.Itisestimatedthatmusculoskeletalpainisacommoncomplaintofpatientswith
SSc,rangingfrom40to80%,andmainlyinpatientswithearlydiffusedisease.Arthritis,
clinicallyobserved,maybeafeatureseeninthepresentationofSSc,oftenleadingtoearly
diagnosticerrorswithrheumatoidarthritis(RA).Inthecourseofthedisease,arthritisis
observedin24–97%ofpatientswithSSc.
Objectives: TocorrelatetheoccurrenceornonoccurrenceofarthritisinpatientswithSScof
theMidwestregionofBrazilwithpossibledistinctclinicalandlaboratorymanifestations
observedinthreegroupsofpatients.Toreportthefrequencyoftrueassociationbetween
systemicsclerosisandrheumatoidarthritisinpatientswithclinicallyandradiologically
observedsynovitis.
Methods:Sixty-oneSScpatientsweresubsequentlyassessedevery3monthswithin1year,
inordertoclinicallyobservetheoccurrenceofsynovitisanditspatternsofprogression.
Patientsweredividedinto3groups:41patientswithSScwithoutarthritis,16SScpatients
witharthritisand4patientswithoverlapofSScandRA.Allpatientsunderwentaradiological
examinationofthehandsattheendofthestudy.
Results:Amongallpatientsevaluated,wefoundafemalepredominance(98.7%),meanage
of50.94years,whitecolor(49.2%),limitedformofthedisease(47.6%),timeofdiagnosis
between5and10years(47.6%)anddurationofthediseaseof8.30years.Amongallpatients,
14(22.9%)hadpositiverheumatoidfactor(RF),whileamongthosewithpositiveRF,only
10patientshadarthritisduringone-yearfollow-up.Theantibodyanticitrulline(anti-CCP)
testwasperformedin24patients,beingpositivein4ofthem(16.7%),withpositivitybeing
observedonlyinpatientswithSSc/RAoverlap.Comparingtheclinicalmanifestationsamong
thegroupsofpatients,therewasahigherincidenceofgastritisandcardiacvalvulopathyin
patientswithSScandarthritis,butnotintheothers.InthegroupofpatientswithSSc/RA
overlapandinpatientswithSScandarthritisasignificantreductioninqualityoflifewas
observed,measuredbyHAQindex,especiallyinpatientswitharthritispresentduring
clin-icalevaluation.Wefoundradiographicchangesin42.6%ofpatientswithSSc.However,
inpatientswithsynovitis,radiologicalchangesconsistentwithrheumatoidarthritiswere
foundin50%ofpatients.
∗ Correspondingauthor.
E-mails:[email protected],[email protected](A.M.C.Horimoto).
http://dx.doi.org/10.1016/j.rbre.2014.12.011
2255-5021/©2015ElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense(http://creativecommons.org/
Conclusions: Whilethefrequencyofclinicalarthritisobservedinpatientswithsystemic
sclerosiswas32.8%,thetrueoverlapbetweenofSScandRAwas6.6%inthisstudy.We
alsoobservedthefrequencyofpositiveanti-CCPin20%ofpatientswitharthritisversusno
patientswithSScwithoutarthritis.
©2015ElsevierEditoraLtda.ThisisanopenaccessarticleundertheCCBY-NC-NDlicense
(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Sobreposic¸ão
de
esclerose
sistêmica
e
artrite
reumatoide:
uma
entidade
clínica
distinta?
Palavras-chave:
Esclerosesistêmica
Artritereumatoide
Sobreposic¸ão/overlap Anticitrulina
Fatorreumatoide
r
e
s
u
m
o
Introduc¸ão: Aesclerosesistêmica(ES)éumaenfermidadedotecidoconjuntivodecaráter
autoimunecaracterizadapelatríadedeinjúriavascular,autoimunidade(celularehumoral)
efibrosetecidual.Estima-sequeadormusculoesqueléticasejaumaqueixafrequentedos
pacientescomES,oscilandoentre40a80%eprincipalmenteempacientescomdoenc¸a
difusaprecoce.Aartrite,clinicamenteobservada,podeserumacaracterísticaobservada
naapresentac¸ãodaES,frequentementelevandoaerrosdiagnósticosiniciaiscomartrite
reumatoide(AR).Nocursodaenfermidade,aartriteéobservadaem24a97%dospacientes
comES.
Objetivos:CorrelacionaraocorrênciaounãodeartriteempacientescomESdaregiãoCentro
OestedoBrasilcompossíveismanifestac¸õesclínicaselaboratoriaisdistintasobservadas
emtrêsgruposdepacientes.Relatarafrequênciadeverdadeiraassociac¸ãoentre
escle-rosesistêmicaeartritereumatoideempacientescomsinoviteclínicaeradiologicamente
observada.
Métodos: 61pacientesportadoresdeESforamavaliadossubsequentementeacada3meses
duranteoperíododeumano,parafinsdeseconstatarclinicamenteaocorrênciadesinovite
epadrõesdeevoluc¸ão.Ospacientesforamdivididosem3grupos:41pacientescomESsem
artrite,16pacientescomEScomartritee4pacientescomsobreposic¸ãoentreESeAR.Todos
ospacientesforamsubmetidosaexameradiológicodasmãosnofinaldoestudo.
Resultados:Dentretodosospacientesavaliados,encontrou-sepredomíniofeminino(98,7%),
idademédiade50,94anos,corbranca(49,2%),formalimitadadadoenc¸a(47,6%),tempode
diagnósticoentre5a10anos(47,6%)etempodeevoluc¸ãodadoenc¸ade8,30anos.Entretodos
ospacientes,14(22,9%)apresentavamfatorreumatoide(FR)positivo,emboraentreaqueles
comFRpositivo,apenas10pacientesapresentaramartriteduranteoseguimentodeum
ano.Oanticorpoanticitrulina(antiCCP)foirealizadoem24pacientes,compositividadeem
4deles(16,7%),sendoapositividadeobservadasomentenospacientescomsobreposic¸ão
ES/AR.Comparando-seasmanifestac¸õesclínicasentreosgruposdepacientes,observou-se
amaiorocorrênciadegastriteevalvulopatiacardíacaempacientescomESeartrite,mas
nãonosdemaisgrupos.NogrupodepacientescomoverlapES/ARenospacientescomES
eartriteobservou-sereduc¸ãoimportantedequalidadedevida,medidopeloíndiceHAQ,
sobretudonospacientescomartritepresentenomomentoda avaliac¸ãoclínica.
Encon-tramosalterac¸õesradiográficasem42,6%dospacientescomES.Contudo,nospacientes
comsinovite,encontrou-sealterac¸õesradiológicascompatíveiscomartritereumatoideem
50%dospacientes.
Conclusões: Enquantoafrequênciadeartriteclínicaobservadaempacientescomesclerose
sistêmicafoide32,8%,averdadeirasobreposic¸ãoentreESeARfoide6,6%nesteestudo.
Observou-seaindaafrequênciadeantiCCPpositivoem20%dos pacientescomartrite
contranenhumpacientecomESsemartrite.
©2015ElsevierEditoraLtda.Este ´eumartigoOpenAccesssobumalicenc¸aCC
BY-NC-ND(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Systemicsclerosis(SSc)isanautoimmunediseaseofthe
con-nectivetissuethatisextremelyheterogeneousinitsclinical
presentation,withinvolvementofmultiplesystems,
follow-ingavariableandunpredictablecourse.1Itsetiologyremains
unknown,withamultifactorialcausebeingsuggested,
pos-sibly triggered by environmental factors in a genetically
predisposedindividual.2
SScismainlycharacterizedbymicrovasculopathy,
activa-tion offibroblastsand excessivecollagenproduction.3 This
isaunique conditionas ithascharacteristics ofthree
dis-tinctpathophysiologicalprocesses:itconsistsofthetriadof
tissue fibrosis, leading to involvement of skin and several
internalorganslikelungs,heart,gastrointestinaltract,aswell
asmusculoskeletalmanifestations.3,4
Itisestimatedthatmusculoskeletal(ME)painisafrequent
complaintofSScpatients,rangingfrom40to80%and
espe-ciallyinpatients withearlydiffusedisease.5 ThemainME
symptomsshownaremovementlimitations,jointpainand/or
swelling.6Arthritis,clinicallyobserved,maybeafeatureinthe
initialpresentationofSSc,oftenleadingtoinitialdiagnostic
errorswithrheumatoidarthritis(RA).7,8 Inaseriesofcases
describedbyRodnanMedsger,Jr.,in41%ofpatients,arthritis
orpolyarthralgiawasthefirstsymptom,ordevelopedwithin
thefirstyearaftertheonsetofRaynaud’sphenomenon.8In
thecourseofthedisease,arthritisisobservedin24–97%of
patientswithSSc.6
Joint lesions,ranging from periarticular osteopenia and
joint space narrowing to apparent erosions, have been
reported in the metacarpophalangeal, proximal
interpha-langealand distalinterphalangeal joints,aswell as inthe
wrists.5,6 AccordingtoRodnan,themostcommon
radiolog-icalabnormalityseeninthebonesandjointsofpatientswith
SScwastheresorptionoftheterminalphalanges
(acroosteoly-sis),whichwasoftenfollowedbysubcutaneouscalcinosis.8In
fact,afterprogressiongreaterthan7yearsofSSc,boneerosion
wasobserved,especiallyinthehands,in4–57%ofpatients,
whilejointspacereductionwasobservedin16–92%ofcases.5
Althoughmanyradiographicchangeshavebeenidentifiedin
thejointsofpatientswithSSc,importanterosivearthropathy
isconsideredunusual.9
SynovialbiopsiesofthejointsofpatientswithSScshowed
evidenceof varyingseverity ofinflammation, and in most
cases, an infiltrate of lymphocytes and plasma cells
dis-tributed diffusely in the tissue or collected in small focal
aggregates was observed.8 Unlike the findings observed in
patientswithRA,littleornotendencytotheformationof
pan-nusandintensesynovialfibrosislaterinthediseasecourse
wasreportedinSScpatients.8
There are isolated reports of erosive arthritis affecting
wristsandhands,withradiologicalandserologicalfeatures
thatareindistinguishablefromthoseobservedinRA.10
How-ever,itisstillunderdiscussionwhethererosivearthritisispart
ofSSc,ifitcouldbeamanifestationofanoverlapsyndrome,
or the manifestationof a different independent disease.11
Whetherrheumatoid arthritisand systemicsclerosis could
coexistinthe same patienthasalsobeen subjectofmuch
controversy.6 Whilesomestudiesassociateerosivearthritis
withthepresenceofrheumatoidfactor,suggestingan
associ-ationbetweenthetwodiseases,7,12othershavenotconfirmed
thesedata.10,11,13
Thisstudywasexpectedtoconfirmtheoccurrenceof
typi-calclinicalandlaboratorymanifestationsinasubgroupofSSc
patientswithclinicallyandradiologicallyobservedarthritis,
assuggestedbypreviousstudies.
Objectives
Tocorrelatetheoccurrenceornonoccurrenceofarthritisin
SScpatientsfromtheMidwestregionofBrazilwithpossible
distinct clinical and laboratory manifestationsobserved in
threegroupsofpatients.
Toreportthetruefrequencyofassociationbetween
sys-temic sclerosis and rheumatoid arthritis in patients with
clinicallyandradiologicallyobservedsynovitis.
Methods
Thisisanobservational,analytical,andcross-sectionalstudy.
Therandomselectionof61patientswasperformedbased
onasurveyofmedicalrecordsfromtheRheumatologyService
ofthe UniversityHospital atthe SchoolofMedicineofthe
FederalUniversityofMatoGrossodoSul(FMUFMS).
Forcomparison,thepatientsweredividedinto3groups:
- 41SScpatientswithoutarthritis;
- 16SScpatientswitharthritis;
- 4patientswithoverlapofSScandRA.
Thepatientstobeselectedshouldmeetthefollowing
crite-ria:
- Meetthenew2013classificationcriteriaforSSc14;
- Inthecaseoflackofskinthickening,theyshouldmeetthe
criteriaofearlySScbyLeRoyandMedsger200115;
- Forthediagnosisoftrueoverlapwithrheumatoidarthritis,
theRAclassificationcriteriaofthe2010ACR/EULARwere
used,16 andalsothemandatorypresenceofanticitrulline
antibody(anti-CCP)and/ortypicalradiological
manifesta-tionsofthedisease;
- Patientswho had other associatedinfectious diseases or
malignancieswereexcluded.
Theinformationrequiredforsociodemographicand
clin-icalcharacterizationofthediseasewasobtainedfromeach
patient’s chartsofmedical records,and they were
supple-mented with patient interviews. In the first consultation,
demographic and clinical data were collected, including
disease duration, year of diagnosis, skin score of
modi-fiedRodnan,17presenceofautoantibodies,thoroughclinical
examination and current treatment. Patients were
subse-quently assessed every 3 months during the first year, to
clinicallyobservetheoccurrenceofsynovitisanditspatterns
ofprogression.Allpatientsunderwentaradiological
exami-nationofthehandsattheendofthestudy.
Specific data on the Medsger’s severity scale,18
Valen-tini’s activity criteria of the disease19 and the Scleroderma
Health Assessment Questionnaire (sHAQ)20 were collected in
the patient’s initial assessmentand alsoin asecond
eval-uation, only in those who presented clinical evidence of
synovitis.
Regarding serum samples,serafrom patientspreviously
selectedandwhichwerefrozenat−50◦Candproperlystored
intheLaboratoryoftheUniversityHospitalofUFMSwereused
fortheresearch.
a. AntinuclearAntibodies(ANA)
Indirectimmunofluorescent techniquewas usedfor the
technique)and usingthecriteriaoftheIIBrazilian
con-sensusofantinuclearantibodiesinHep-2cells(2003),21for
theinterpretationoftheresults.
Serawereconsideredpositiveifthetitlewasgreaterthan
orequalto160anddiluteduntilfluorescencebecame
neg-ative.
b. Anti-Sm,anti-RNP,anti-Jo1,anti-Ro(SSA)andanti-La(SSB)
tests–enzymeimmunoassay(ELISA)techniquewasused
as previously described by McClain,22 using
substrate-specific kits for each test, following the manufacturer’s
specifications(Hemagen Diagnostics,Inc.). Thetestwas
consideredpositivewhenthevaluefoundwas3timesor
morehigherthancut-off.
c. Rheumatoidfactorresearch–atechniqueofnephelometry
wasusedandit wasconsidered positiveifthe titlewas
greaterthan40IU/ml.
d. Anti-CCP test – enzyme-linked immunosorbent assay
(ELISA)techniquewasused,followingthemanufacturer’s
specifications (INOVA QUANTA LiteTM CCP3.1 IgG/IgA
ELISA). The test was considered negative if <20 units,
weaklyreactivebetween20and39units,moderately
reac-tivebetween40 and 60 units, and highlyreactive (high
values)if>60units.
e. For the anti-centromere research – indirect
immuno-fluorescence technique was used, having HEp2 cells as
substrateaccordingtothecriteriaoftheIIBrazilian
con-sensusofantinuclearantibodiesinHep-2cells(2003),21for
theinterpretationofresults.
f. For anti-DNA topoisomerase 1 (anti-Scl70) test –
immunoassay technique was used,23 using a
spe-cific kit QUANTA Lite TM Scl-70 from the laboratory
INOVA (INOVA Diagnostics, Inc., San Diego, CA, USA)
following the manufacturer’s specifications. It was
considered nonreactive if <20 units, weakly reactive
between 20 and 39 units, moderately reactive between
40 and 80 units, and highly reactive (high values) if
>80units.
g. Anti-RNA polymerase III – ELISA technique was used
as previously described,24 using a specific kit QUANTA
Lite RNA POL III ELISA from INOVA laboratory (INOVA
Diagnostics, Inc., San Diego, CA, USA) following the
manufacturer’s specifications. It was considered
neg-ative if values <20 units, weakly reactive if between
20 and 39 units, moderately reactive between 40
and 80 units, and strongly reactive (higher values) if
>80units.
Statistical
analysis
Thecomparisonbetweenpatientswithandwithoutarthritis
inrelationtothequantitativevariablesevaluatedinthisstudy
wasperformedusingtheStudentt-test.Thechi-squaretest
wasusedtoexaminetheassociationbetweenpresenceand
absenceofarthritiswithqualitativevariablesmeasuredinthis
study.Theresultsoftheothervariablesevaluatedinthisstudy
werepresentedindescriptiveformorintheformoftables
and graphs. Statistical analysis was performed using the
softwareSPSS,version20.0,consideringasignificancelevel
of5%.
Results
Atotalof61patients,with60(98.7%)beingwomenand1(1.6%)
aman,withameanageof50.94±2.40years(mean±standard
errorofthemean),wasfound.
Of all patients, 30 (49.2%) patients were reported to be
white,28(45.9%)patientswerereportedhavingbrowncolor
and3(4.9%)werereportedbeingblack.
Regardingthediagnosis,58(95.1%)patientsdiagnosedmet
thecriteriaforclassificationof2013ACR/EULARforSSc.The3
(4.9%)patientswhodidnotmeetthesecriteria,metthecriteria
byLeroy/MedsgerforearlySSc.
Regarding the clinical forms of the disease, 29 (47.6%)
patients had the limited form,20 (32.8%) patients had the
diffuseform,3(4.9%)patientshadtheearlyform,8(13.1%)
patientshad theoverlap form(1.6%)and 1patienthad the
formsinescleroderma.
Regardingthetimefordiagnosis,16(26.2%)patientswere
diagnosedmorethan10yearsbefore,29(47.6%)patientswere
diagnosed between 5 and 10 years before, and 16 (26.2%)
patients werediagnosed lessthan 5yearsbefore. The
pro-gressionofthediseaseinpatientsingeneralwas8.30±1.01
years.
Amongallpatients,14(22.9%)werepositivefor
rheuma-toidfactor.Thepositivityofrheumatoidfactor was9.8%in
patients withSScwithout arthritis,37.5% intheSSc group
with arthritis, and 100% in the group with SSc/RA
over-lap. The anticitrulline antibody (anti-CCP) was performed
in 24 patients, being positive in 4 (16.7%) of these, with
positivitybeingobservedonlyinpatientswithSSc/RA
asso-ciation.AmongpatientswithtrueSSc/RA overlap,halfwas
oflimitedform(n=2–50.0%),onepatientwasofdiffuseform
(n=1–25.0%) and one patient had association with Sjögren
syndrome(n=1–25.0%).
The results regarding the epidemiological data and the
monitoringindexinSScpatientswithoutarthritis,SScwith
arthritis,andoverlapSSc/RAareshowninTable1.Therewas
nosignificantdifferencebetweenpatientswithSScwithout
arthritis, SSc with arthritisand SSc/RA overlap inrelation
to the quantitative variables age, time of Raynaud’s
phe-nomenon(RP)beforediagnosis,diseasedurationnotcounting
RPand monitoring indices(one-way ANOVA,pvalues
ran-gingbetween0.046and0.872;HQ2:Student’st-test,p=0.071).
Likewise, there was no association between the different
experimentalgroupsandthenominalorordinalqualitative
variables gender, color, timeofdiagnosis and clinicalform
(chi-squaretest,pvaluerangingfrom.758to.941).
Table2shows thedistributionofthe patientsevaluated
inthisstudyandresultsregardingskin,vascularand
muscu-loskeletaldisorders,inSScpatientswithoutarthritis,SScwith
arthritis,andoverlapofSSc/RA.Overall,therewasno
asso-ciation betweentheexperimentalgroupsand the variables
relatedtoskin,vascularandmusculoskeletalmanifestations
observedinthepatientsevaluatedinthisstudy(chi-square
test, pvalues rangingfrom 0.145 to0.630). There wasalso
nodifferencebetweenpatientswithandwithoutarthritisin
relationtoskinscore(One-wayANOVAtest,p=0.513).
Except for gastritis (p=0.016) and valvar heart disease
Table1–DemographicaspectsandmonitoringindexesinpatientswithSScwithoutarthritis,SScwitharthritisand
SSc/RAoverlap.
Variable Group pvalue
SScwithoutarthritis SScwitharthritis SSc/RAoverlap
Epidemiologicaldata
Age 50.83±1.96 50.31±3.04 54.00±8.18 0.872
Gender
Male 1(2.4) 0(0.0) 0(0.0) 0.780
Female 40(97.6) 16(100.0) 4(100.0)
Color
White 20(48.8) 9(56.2) 1(25.0) 0.758
Brown 19(46.3) 6(37.5) 3(75.0)
Black 2(4.9) 1(6.2) 0(0.0)
Timeofdiagnosis
Lessthan5years 11(26.8) 4(26.7) 1(25.0) 0.595
Between5and10years 17(41.5) 8(53.3) 3(75.0) Morethan10years 13(31.7) 3(20.0) 0(0.0)
TimeofRPbeforediagnosis 2.68±0.84 5.56±2.16 6.50±4.57 0.235 TimeofdiseasewithoutcountingRP 9.41±1.05 7.44±1.20 6.25±1.03 0.396
Clinicalform
Limited 18(43.9) 9(52.6) 2(50.0) 0.941
Diffuse 14(34.1) 5(31.2) 1(25.0)
Recentonset 3(7.3) 0(0.0) 0(0.0)
Overlap 5(12.2) 2(12.5) 1(25.0)
Sine 1(2.4) 0(0.0) 0(0.0)
Monitoringindexes
sHAQ1(n=61) 0.59±0.07 0.71±0.08 0.97±0.17 0.163
sHAQ2(n=20) – 0.75±0.08a 1.09±0.14a 0.071a
Severityscale 5.29±0.49 4.00±0.53 4.50±1.04 0.300
Activityscale 2.29±0.21 2.50±0.34 2.50±0.68 0.854
SSc:systemicsclerosis,RA:rheumatoidarthritis,RP:Raynaud’sphenomenon,sHAQ:SclerodermaHealthAssessmentQuestionnaire. Theresultsarepresentedinmedian±standarderrorofthemedianorabsolutefrequency(relativefrequency).pvalueonone-wayANOVAtest. EquallettersonlineindicatethatthereisnosignificantdifferenceamongthegroupsafterTukey’stest.
a pvalueonStudent’st-test.
n=7–43.8%, valvar disease: n=7–100.0%) showed a higher
percentofcaseswhencomparedwiththosewithSSc
with-outarthritis(gastritis:n=5–12.2%;valvulopathy:n=11–26.8%),
therewasnoassociationbetweentheexperimentalgroupsof
SScwithoutarthritis,SScwitharthritisandSSc/RAoverlap
with variables related to other gastrointestinal,
cardiopul-monaryand renal manifestationsobserved inthe patients
evaluated in this study (chi-square test, p values ranging
from 0.088 to 0.924). There was no significant difference
between the experimentalgroups in relationto the
quan-titative variable pulmonary functional vital capacity (FVC)
(One-wayANOVAtest,p=0.313).Moreover,itwasnot
possi-bletocomparepatientswithSScwithoutarthritis,SScwith
arthritis, and SSc/RA overlap, regardingthe estimated
pul-monaryarterypressurebyechocardiography(EcoPSAP)asout
ofthe16SScpatientswitharthritis,thismeasurewasonly
per-formedinonepatientandwasnotperformedinanypatient
withSSc/RAoverlap.TheseresultsareshowninTable3.
Theresultsofthe laboratorytests inSScpatients
with-outarthritis,SScwitharthritisandSSc/RAoverlapareshown
inTable4. There wasno difference betweenpatients with
and without arthritis regarding erythrocyte sedimentation
rate,C-reactiveprotein,creatinephosphokinase,C3and C4
complements(one-wayANOVA,pvaluerangingfromp=0.467
top=0.952).Moreover,inrelationtotheresultsofthe
labora-torytests,therewasnoassociationbetweentheexperimental
groupsandtheresultforanti-Ro,anti-La,anti-Sm,anti-RNP,
anti-Jo1,anti-Scl70,anticentromereandanti-RNAPol3,
nei-therwiththeresultregardinggeneralchangesinradiography
(X-ray)ofhands(chi-squaretest,valuerangingfrom0.073to
0.816). Onthe other hand,the percentageof patientswith
overlapping SSc/RAwho hadareductioninthejoint space
orsubchondralerosionsinthehandsX-ray,orpositive
anti-CCP(n=4–100.0%)wasgreaterthanthatofpatientswithSSc
withandwithoutarthritis(n=0–0.0%).Furthermore,the
per-centageofpatientswithSScwitharthritisandSSc/RAoverlap
whohadpositiverheumatoidfactor(n=6–37.5%n=4–100.0%,
respectively)wassignificantlyhigherthanthatofSScpatients
withoutarthritis,whoalsoshowedpositiverheumatoidfactor
(n=4–9.8%;chi-squaretest,p<0.05).Theseresultsareshown
inFig.1.
Among the patients with arthritis(n=20) the most
fre-quently prescribed drugs were methotrexate (n=9–45.0%),
azathioprine (n=7–35.0%), prednisone (n=6–30.0%),
chloro-quine diphosphate (n=6–30.0%), and leflunomide (n=
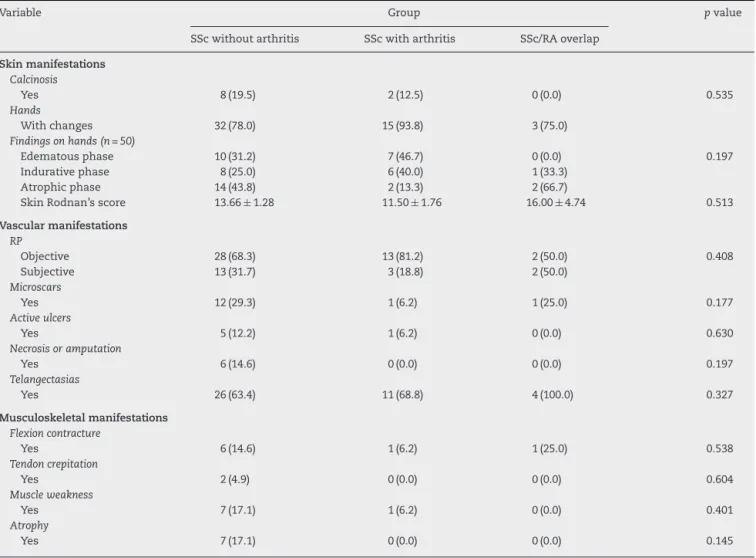
Table2–Skin,vascular,andmusculoskeletalmanifestations,inpatientswithSScwithoutarthritis,SScwitharthritis
andSSc/RAoverlap.
Variable Group pvalue
SScwithoutarthritis SScwitharthritis SSc/RAoverlap
Skinmanifestations Calcinosis
Yes 8(19.5) 2(12.5) 0(0.0) 0.535
Hands
Withchanges 32(78.0) 15(93.8) 3(75.0)
Findingsonhands(n=50)
Edematousphase 10(31.2) 7(46.7) 0(0.0) 0.197
Indurativephase 8(25.0) 6(40.0) 1(33.3) Atrophicphase 14(43.8) 2(13.3) 2(66.7)
SkinRodnan’sscore 13.66±1.28 11.50±1.76 16.00±4.74 0.513
Vascularmanifestations RP
Objective 28(68.3) 13(81.2) 2(50.0) 0.408
Subjective 13(31.7) 3(18.8) 2(50.0)
Microscars
Yes 12(29.3) 1(6.2) 1(25.0) 0.177
Activeulcers
Yes 5(12.2) 1(6.2) 0(0.0) 0.630
Necrosisoramputation
Yes 6(14.6) 0(0.0) 0(0.0) 0.197
Telangectasias
Yes 26(63.4) 11(68.8) 4(100.0) 0.327
Musculoskeletalmanifestations Flexioncontracture
Yes 6(14.6) 1(6.2) 1(25.0) 0.538
Tendoncrepitation
Yes 2(4.9) 0(0.0) 0(0.0) 0.604
Muscleweakness
Yes 7(17.1) 1(6.2) 0(0.0) 0.401
Atrophy
Yes 7(17.1) 0(0.0) 0(0.0) 0.145
SSc:systemicsclerosis,RA:rheumatoidarthritis,RP:Raynaud’sphenomenon.
Theresultsarepresentedinmedian±standarderrorofthemedianorabsolutefrequency(relativefrequency).pvalueonone-wayANOVAtest.
Discussion
Jointinvolvementwithseveresynovitisisrelatively uncom-moninpatientswithsystemicsclerosis(SSc).25About11%of
SScpatientspresentwitharthritisattheonsetofthedisease,
usuallycharacterizedbymono-oroligoarthritis,responsiveto
corticosteroidtherapy.However,somepatientswithSSchave
moreaggressiveerosivearthritis,mimickingclassic
rheuma-toidarthritis(RA).25
Arate of6.6%of overlap withRAwas observed inthis
studyin61patientswithSScandmusculoskeletalsymptoms
wereveryprevalentinthesepatientswithorwithout
associ-ationbetweenthediseases,mainlyrepresentedbyarthritis
inalmost a thirdofthem. Other studies inBrazil found a
higherprevalenceofosteoarticularmanifestations(47.7%),26
witharthralgiarangingfrom70.5%to84.5%,10,27,28inaddition
toarthritisdescribedin17.6–44.4%ofpatients.10,27 However,
theprevalenceoftrueoverlapwithRAhasbeendescribedas
beingof4.3–5.2%inotherstudieswithpatientswithSSc.6,11,12
Animportantaspectobservedinourpatientswasthatthe
presenceofarthritiscontributedalottothefunctionaldeficit
andlowerqualityoflifemeasuredbysHAQ.WithsHAQ,much
higherdisabilityscoreswereobservedinthesecondclinical
evaluationinpatientswitharthritis,althoughadirect
compar-isonwithpatientswithoutarthritiswasnotpossible.Morita
andcolleaguesreportedthatpatientswithdiffuseSSchadthe
highestratesofdisabilityinHAQ,higherthanthoseofpatients
withRA,SLEand othercollagenvasculardiseases.29Itwas
alsoobservedthatpatientswithSScandjointinvolvement
hadhigherscoresinHAQthanpatientswithpsoriaticarthritis,
whilethepaindomainwashigherinSScpatientsthaninthose
withRA.30AnassociationbetweenHAQandfunctionaldeficit
causedbyhandsinvolvementhasalreadybeendescribed.31
Inaddition,itwasdescribedthatthedisabilitycausedbythe
involvementofthehandsinSScpatientswhodidnothave
RPatthetimeofevaluationwasassevereasthatobserved
inapopulationofpatientswithRAwithcomparabledisease
duration of10years.20 TheusefulnessofHAQinthe
evalu-ationofpatientswithSScwasdemonstratedbystudiesthat
reportedthatitcanpredicttheprogressandsurvivalinthese
patients.32,33Inthiswork,therewasasignificantpositive
lin-earcorrelationbetweensHAQinpatientswitharthritisand
diseaseactivityasmeasuredbythePearsontest.Medsgerand
Table3–Gastrointestinal,cardiopulmonaryandrenalmanifestations,inpatientswithSScwithoutarthritis,SScwith
arthritisandSSc/RAoverlap.
Variable Group pvalue
SScwithoutarthritis SScwitharthritis SSc/RAoverlap
Gastrointestinalmanifestations Involvementofesophagus
Yes 30(73.2) 9(56.2) 3(75.0) 0.447
Gastrointestinalsymptoms
GERD 9(22.0) 5(31.3) 2(50.0) 0.414
Esophagitis 11(26.8) 2(12.5) 1(25.0) 0.510
Gastritis 5(12.2)b 7(43.8)a 0(0.0)ab 0.016
Esophagealhypotonia 6(14.6) 1(6.3) 2(50.0) 0.088
Esophagealdilation 2(4.9) 1(6.3) 0(0.0) 0.875
Cardiopulmonarymanifestations
FVC 81.83±2.32 88.31±3.47 85.00±4.74 0.313
FVC–classification
>80% 22(53.7) 11(68.8) 3(75.0) 0.887
Between70and80% 13(31.7) 4(25.0) 1(25.0) Between50and69% 4(9.8) 1(6.2) 0(0.0)
<50% 2(4.9) 0(0.0) 0(0.0)
ChestTC
Altered 19(46.3) 9(56.2) 1(25.0)
Tomographyfindings(n=29)
Fibrosis 14(73.7) 5(55.6) 1(100.0) 0.496
“Groundglass”pattern 5(26.3) 4(44.4) 0(0.0)
EchoPASP 31.23±3.19(n=13) 42.00(n=1) – –
Resultonechocardiogram
Altered 26(63.4) 7(43.8) 1(25.0)
Findingsonechocardiogram(n=34)
Valvulopathy 11(26.8)b 7(100.0)a 0(0.0)ab 0.014
ConcentricLVH 9(22.0) 0(0.0) 1(100.0) 0.189
LVdiastolicdysfunction 6(14.6) 2(28.6) 0(0.0) 0.924 MildormoderatePAH 5(12.2) 1(14.3) 0(0.0) 0.668
Pericarditis 4(9.8) 2(28.6) 0(0.0) 0.665
Renalmanifestations Renalcrisis
Yes 1(2.4) 0(0.0) 0(0.0) 0.780
SSc:systemicsclerosis,RA:rheumatoidarthritis,GERD:gastroesophagicalrefluxdisease,FVC:pulmonaryfunctionalvitalcapacity,EchoPASP: estimatedpressureonpulmonaryarteryonechocardiogram,LVH:leftventricularhypertrophy,PAH:pulmonaryarteryhypertension. Theresultsarepresentedinmedian±standarderrorofthemedianorabsolutefrequency(relativefrequency).pvalueonone-wayANOVAtest. EquallettersonlineindicatesignificantdifferenceamongthegroupsafterTukey’stest.
correlationwithskinthickening,cardiac involvement, digi-talcontractures,tendon crepitation,andrenal involvement in1000patientswithSSc.18
Theobjective wastostudy,inthis heterogeneous
popu-lation ofpatients in the Midwest of Brazil,the correlation
between the presence of clinical and radiological proven
arthritis and the clinical and laboratory manifestations
observed inpatients with SSc. Patients with arthritis who
were observedduringthe study periodtotaled32.8% ofall
patients, with the majority presenting a pattern of
mono-oroligoarthritiswithremissionafterbeginningthestandard
treatmentforsystemicsclerosis.However,ofthe20patients
withdemonstratedarthritis,6hadapatternofsymmetrical
andadditivepolyarthritisaffectinglargeandsmalljointswith
prolongedmorningstiffness,requiringtheuseofleflunomide
withorwithouttheuseofmethotrexate,amongother
medica-tions.Ofthese6patientswithpersistentarthritis,4ofthem
showedpositivecycliccitrullinatedantipeptid(anti-CCP),as
wellasjointspacenarrowingand/orsubchondralerosionsin
theradiographsofhands,leadingtotheconclusionthatthere
isclearlyanoverlapwithrheumatoidarthritis,anditwas
nec-essarytocombinerituximabtothetherapeuticregimenoftwo
patientstobettercontrolofcompositeindicesofjointactivity.
There are isolated reports of erosive arthritis affecting
wristsandhands,withradiologicalandserologicalfeatures
thatareindistinguishablefromthoseobservedinRA.10
How-ever,whethererosivearthritisispartofSSc,whetheritcould
be a manifestation of an overlap syndrome or the
mani-festation of a different independent disease is still under
discussion.11 Whether rheumatoid arthritis and systemic
sclerosiscouldcoexistinthesamepatienthasalsobeenthe
subjectofmuchcontroversy.6Whilesomestudiesassociate
erosivearthritiswiththepresenceofrheumatoidfactor,
sug-gestinganoverlapbetweenthetwodiseases,7,12othershave
notconfirmedthesedata.10,11,13Inourpatients,althoughthe
presenceofrheumatoidfactorwasrelatedtotheoccurrenceof
arthritisinpatients,onlyanti-CCPwasundoubtedlyrelatedto
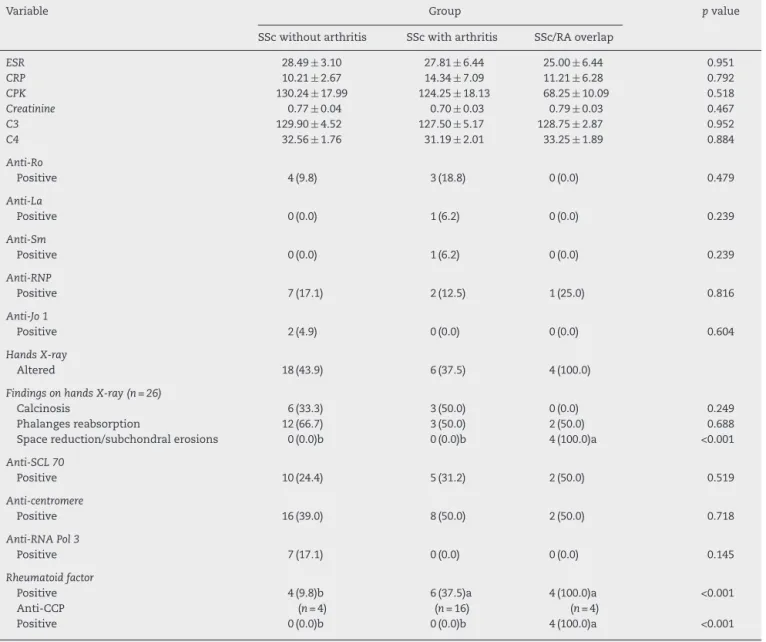
Table4–LaboratorytestsandradiographsofhandsofpatientswithSScwithoutarthritis,SScwitharthritisandSSc/RA overlap.
Variable Group pvalue
SScwithoutarthritis SScwitharthritis SSc/RAoverlap
ESR 28.49±3.10 27.81±6.44 25.00±6.44 0.951
CRP 10.21±2.67 14.34±7.09 11.21±6.28 0.792
CPK 130.24±17.99 124.25±18.13 68.25±10.09 0.518
Creatinine 0.77±0.04 0.70±0.03 0.79±0.03 0.467
C3 129.90±4.52 127.50±5.17 128.75±2.87 0.952
C4 32.56±1.76 31.19±2.01 33.25±1.89 0.884
Anti-Ro
Positive 4(9.8) 3(18.8) 0(0.0) 0.479
Anti-La
Positive 0(0.0) 1(6.2) 0(0.0) 0.239
Anti-Sm
Positive 0(0.0) 1(6.2) 0(0.0) 0.239
Anti-RNP
Positive 7(17.1) 2(12.5) 1(25.0) 0.816
Anti-Jo1
Positive 2(4.9) 0(0.0) 0(0.0) 0.604
HandsX-ray
Altered 18(43.9) 6(37.5) 4(100.0)
FindingsonhandsX-ray(n=26)
Calcinosis 6(33.3) 3(50.0) 0(0.0) 0.249
Phalangesreabsorption 12(66.7) 3(50.0) 2(50.0) 0.688 Spacereduction/subchondralerosions 0(0.0)b 0(0.0)b 4(100.0)a <0.001
Anti-SCL70
Positive 10(24.4) 5(31.2) 2(50.0) 0.519
Anti-centromere
Positive 16(39.0) 8(50.0) 2(50.0) 0.718
Anti-RNAPol3
Positive 7(17.1) 0(0.0) 0(0.0) 0.145
Rheumatoidfactor
Positive 4(9.8)b 6(37.5)a 4(100.0)a <0.001
Anti-CCP (n=4) (n=16) (n=4)
Positive 0(0.0)b 0(0.0)b 4(100.0)a <0.001
SSc:systemicsclerosis,RA:rheumatoidarthritis,ESR:erythrocytesedimentationrate;CRP:C-reactiveprotein;CPK:creatinephosphokinase; C3:C3complementfraction;C4:C4complementfraction;X-ray:radiograph.
Theresultsarepresentedinmedian±standarderrorofthemedianorabsolutefrequency(relativefrequency).pvalueonone-wayANOVAtest. EquallettersonlineindicatesignificantdifferenceamongthegroupsafterTukey’stest.
asthefindingofreductionofthejointspaceandsubchondral erosionsonradiographsofthehandsofthesepatients.
TheprevalenceofanassociationbetweenSSc/RAvaries from4.3to5.2%amongpatientswithsystemicsclerosis.6,11,12
Inaddition,ahigherincidenceofRAinpatientswithSScthan
inthegeneralpopulationwasfound.34Itwassuggestedthat
thisSSc/RAoverlapisadistinctentityaccordingtothe
dif-ferentgeneticbackgroundofpatients:significantlyincreased
frequencies of HLA-DR3 and HLA-DR11 were observed in
SSc/RAcomparedwithRApatientsandhealthyindividuals;
also,allelefrequenciesofHLA-DR1andHLA-DR4(shared
epi-topes)were significantlyhigher inSSc/RA and RAthan in
patientswithSScorcontrols.12However,theresultsobtained
inalargecohortofEuropeanCaucasianpatientswithSScdid
notsupporttheinvolvementofgenes(CCL21,CD244,CDK6)
recentlyidentifiedasofsusceptibilitytoRAinthesepatients.13
Anyway, thegeneticlinkisthe bestexplanation forthe
occurrenceofSSc/RAoverlap.35 Severalstudieshaveshown
thatautoimmunediseasesaregroupedinfamiliesofpatients
with SSc.36–39 In a population with 719 patients with SSc,
RA was the second most prevalent disease in a study of
polyautoimmunity(21%)and themostcommonlyobserved
infamilialautoimmunity(18%).34Thissupportstheconcept
thatthesediseasescanariseinasharedgeneticbasis
under-lyingvariousautoimmunephenotypes,withoverlapbetween
SSc/RAbeingonlyoneofthesephenotypes.
Szücs et al.described,inpatientswithoverlap between
SSc/RA, a combination ofcharacteristic clinical
manifesta-tions, both for SSc and RA, with erosive polyarthritis in
82%,pulmonaryfibrosisin77%,esophagealinvolvementin
55%,andcardiovascularmanifestations,whilekidney
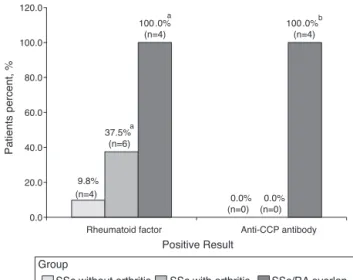
9.8%
(n=4) 0.0%
(n=0) (n=6)
0.0% (n=0)
(n=4) (n=4)
0.0 20.0 40.0 60.0 80.0 100.0 120.0
Rheumatoid factor Anti-CCP antibody
Patients percent, %
Positive Result
SSc without arthritis SSc with arthritis Group
SSc/RA overlap
100.0%a
37.5%a
100.0%b
Fig.1–Graphshowingthepercentageofpatientswith rheumatoidfactororpositiveornegativeanti-CCP antibody,amongSScpatientswithoutarthritis,SScwith arthritis,andoverlappingSSc/RA.Eachcolumnrepresents thepercentageofpatients.aSignificantdifferencein relationtoSScpatientswithoutarthritis(chi-squaretest, p<0.001).bSignificantdifferenceinrelationtoSScpatients withoutarthritisandSScwitharthritis(chi-squaretest, p<0.001).SSc:systemicsclerosis,RA:rheumatoidarthritis.
serologicalpatternwasalsoreported,sincemostpatientswith
overlapwere those oflimitedform,withpositivityof
anti-topoisomerasein23%ofpatientsbutpositiveanti-centromere
inonly9%.12However,inthisstudywefoundinpatientswith
SSc/RAoverlapanequalproportionofpatientswithlimited
anddiffuseforms,and50%ofpositivityofthetopoisomerase
andtheanticentromere.Moreover,whencomparingthe
clini-calmanifestationsofpatientsofthegroupwitharthritis,even
theSSc/RAoverlapsubgroup,tothegroupofSScpatients
with-outarthritis,wecouldnotconfirmthattheSSc/RAoverlapis
anentityclinicallydistinctfrommereassociationofSScand
RA.
Thepresenceofrheumatoidfactor(RF)hasbeenobserved
inup to25% ofpatientswithSSc,6 in agreementwiththe
presentstudy,which foundapositivityrate ofRFof22.9%
Table5–Mostfrequentlyuseddrugsinpatientswith
arthritis.
Drugs(amongpatientswitharthritis–n=20) (n)%
Non-steroidalanti-inflammatories 13(65.0)
Methotrexate 9(45.0)
Azathioprine 7(35.0)
Prednisone 6(30.0)
Chloroquinediphosphate 6(30.0)
Leflunomide 6(30.0)
Rituximab 2(10.0)
Theresultsarepresentedinabsolutefrequency(relativefrequency).
among61patients.Inourcase,thepresenceofarthritis cor-relatedsignificantlywithFRpositivity.Misraetal.foundRF positivityin80%ofpatientswithdegenerativearthritis com-pared with 13% positivity inother patients with SSc.6 We
foundpositiveFRin50%ofpatientswitharthritisandin100%
ofpatientswithdegenerativearthritisrelatedtoradiographic
changes,against9.8%ofpatientswithSScwithoutarthritis.
Inthelattergroupofpatients,rheumatoidfactorwas
prob-ablyrelatedtotheoverlapsyndrome,sincethe4patientsin
thisgroupwithpositiveRFhadanassociationwithSjögren’s
syndrome.
Recently,throughtheavailabilityofthecycliccitrullinated
antipeptide tests (anti-CCP), the percentage of association
with positive anti-CCP RA has been reported in 1–15% of
patients with SSc.5 A statistically significant correlation
betweentheanti-CCP positivityandthe presenceof
arthri-tiswithmarginalerosionsinpatientswithSScisdescribed,
whichcouldaidinthediagnosisofoverlapofSScandRA,and
enableappropriatetreatment.9However,anti-CCPantibodies
bythemselvesdonotdefinerheumatoidarthritis,sincethe
frequencyofpositivityoftheseantibodies inpatientswith
SScwithoutarthritisisnotknown.5Wefoundanti-CCP
posi-tivityin20%ofSScpatientswitharthritisandpresentin100%
ofpatientswithdegenerativearthritisrelatedtoradiographic
changes,versusnoSScpatientswithoutarthritis.
Radiographic changes were found in 42.6% of the SSc
patients,particularlycharacterizedbyresorptionofthe
dis-tal phalanges (65.4%)and calcinosis(34.6%)inbothgroups
withandwithoutarthritis.However,inpatientswithsynovitis
presentingchangesonradiographsofthehands,radiological
changescompatiblewithrheumatoidarthritiswereobserved
in50%ofthesepatients,characterizedbyjointspace
narrow-ingand/orsubchondralerosions.TheseRA-likechangeswere
onlyfound in4patients withdiagnosis ofSSc/RA overlap.
However,bothinpatientswithSScandarthritisorpatients
withSSc/RAoverlap,thepresenceofresorptionofthedistal
phalangesandcalcinosiswasseen,butthesepathognomonic
changesofSScwereobservedlesscommonlyinthesecond
group. Meanwhile, Allali et al.found radiographic changes
in80%of46patientswithSScwhohad arthritis,including
joint spacenarrowing in37%and erosions in43%ofthese
patients.9Thesameresearcherfoundthatthemostcommon
sitesofoccurrenceoferosions weretheproximal
interpha-langeal and radiocarpal joints.9 In a cohort of58 patients
with SSc, Schmeiser et al. found signs of arthritis in 31%
of patients, with 19% being clinical and 26% radiological.
Inameta-analysisofsevenstudies,wefoundaprevalence
of26%ofradiologicallydetectablearthritisinpatientswith
SSc.11
Thehigherincidenceofgastritisandcardiacvalvulopathy
observedonlyinpatientswithSScandarthritis,butnotinthe
othergroups,canbeexplainedbythemoresustaineduse,and
ingreateramounts,ofnon-steroidanti-inflammatorydrugs
(NSAIDs) forjointpain. Thegroup ofpatientswith SSc/RA
overlap, despite apersistent arthritis, promptly began
tak-ingdisease-modifyinganti-rheumaticdrugs(DMARDs)rather
thanusingNSAIDs.Theblockadeofcyclooxygenasecaused
bytheuse ofNSAIDsreducesthe productionof
inflamma-toryprostaglandins,altering the balance ofvasoconstrictor
bloodpressure,leadingtodecompensationofheartfailureand
valvulopathies.40,41StudypatientswithSScandarthritishad
ahigherassociationwithsystemichypertension(unpublished
data)andthetwostudypatientswithSScandarthritis,who
had valvulopathies,showedno associationwith rheumatic
fever,systemiclupuserythematosusorantiphospholipid
syn-drome.
RegardingtheuseofDMARDs,theliteratureisscarceabout
theuseofleflunomide(LFD)insystemicsclerosis.Sebastiani
etal.observedthatLFDwasabletoimprovearthritisrelated
toSScin3patients.Moreover,organinvolvementremained
stablein2cases,whileskinsclerosisimprovedintheother
patient.25
The efficacy of rituximab (RTX) as a modifying drug
in patients with rheumatoid arthritis is well documented.
In patients with SSc its use appears to be safe and well
tolerated.42–44AcontrolledstudypriortoRTXindicatedthat
it can improve lung function in patients with SSc,42 and
a skin improvement was described with the use of
mod-ified Rodnan score42–44 or histological methods,42,44 which
couldsuggestapotentialroleofdisease-modificationinthe
pathophysiological process offibrosis in SSc byB
lympho-cytedepletion.InRA,theeffectiveclinicalresponsewasnot
necessarilycorrelatedwiththedegreeofB-cellinfiltrationin
synovialtissuesbeforetreatment.43Butsincethelocal
infil-trationof Bcells is animportant component ofthe mode
ofactionofRTX, Lafyatiset al. highlight thatthis therapy
may be moreeffective when the target tissues show
infil-tratesfullofBcells,suchaspulmonaryfibrosisassociatedwith
SSc.43
Biologicalblockersoftumornecrosisfactor(anti-TNF)were
notused in our patients, althoughthey proved to be
use-fulandeffectiveinthetreatmentofarthritisassociatedwith
inflammatorySSc.45–48Boselloetal.suggestedthattheuseof
anti-TNFinmedium-termcouldalsobebeneficialtoreduce
theprogressionoffibroticdiseaseandcontrolofulcerations,46
butotherstudiesdidnotobserveanyimprovementintheskin
scoreandinthepulmonaryfunctionwiththerapy.45,47
More-over,Omairetal.reportedmalignancies(breastcancer,basal
cellcarcinomaandleukemia)inathirdofpatientsreceiving
anti-TNFtherapy47 andnowtheEuropeangroupofexperts
onthesclerodermaandsystemicsclerosistrialsandresearch
(EUSTAR)doesnotrecommendtheroutineuse.48
Regarding theuse ofotherbiologicals inSSc,theywere
notnecessary in ourpatients with arthritisdue toa good
response with the use of rituximab, although the EUSTAR
groupconcludedinanobservationalstudythattocilizumab
andabataceptappearedtobesafeandeffectiveinthe
treat-mentofrefractorypolyarthritisinpatientswithSSc,butthere
werenosignificant changesinlungorskinfibrosisinboth
groups.49
Theweaknessofthestudywastheheterogeneityofthe
study population,patients withlong clinicalstagingofthe
disease,andalsothesmallnumberofpatientsintheSSc/RA
overlapgroup.Therelevanceofthisstudyisthatitdescribed,
forthe firsttimeinthe country,the clinicallaboratory
fea-turesofthisoverlapinpatientswithSSc.Moreover,thisstudy
confirmstheimportantroleofradiographsofthehands,of
rheumatoidfactor,andanti-CCPintheevaluationof
arthri-tis inpatients with SSc,and it is possibleto correlatethe
positivityofbothantibodieswiththe occurrenceof
associ-ationbetweenSScandRA.
Conclusions
Whilethefrequencyofclinicalarthritisobservedinpatients
withsclerodermawas32.8%,thetrueoverlap between
sys-temic sclerosis and rheumatoid arthritis was 6.6% in this
study.
Exceptforahigherincidenceofgastritisandheartvalve
disease, there were no distinct clinical manifestations in
patientswithSScandpresenceofarthritiscomparedwitha
groupofpatientswithoutarthritis.
However,thepercentageofpatientswitharthritiswhohad
radiographic changes, and positive rheumatoid factor, was
significantly higherthan those oftheSSc patients without
arthritis.Wealsoobservedthefrequencyofpositiveanti-CCP
in20%ofpatientswitharthritisversusnopatientswithSSc
withoutarthritis.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.VargaJ,AbrahamD.Systemicsclerosis:aprototypic
multisystemfibroticdisorder.JClinInvest.2007;117(3):557–67.
2.HerrickAL,WorthingtonJ.Geneticepidemiology:systemic sclerosis.ArthritisRes.2002;4(3):165–8.
3.Coral-AlvaradoP,PardoAL,Casta ˜no-RodriguezN,
Rojas-VillarragaA,AnayaJM.Systemicsclerosis:aworldwide globalanalysis.ClinRheumatol.2009;28:757–65.
4.BeyerC,SchettG,GayS,DistlerO,DistlerJHW.Hypoxiainthe pathogenesisofsystemicsclerosis.ArthritisResTher. 2009;11:220–9.
5.ClementsPJ,AllanoreY,KhannaD,SinghM,FurstDE. Arthritisinsystemicsclerosis:systematicreviewofthe literatureandsuggestionsfortheperformanceoffuture clinicaltrialsinsystemicsclerosisarthritis.SeminArthritis Rheum.2012;41:801–14.
6.MisraR,DartonK,JewkesRF,BlackCM,MainiRN.Arthritisin scleroderma.BrJRheumatol.1995;34:831–7.
7.CatoggioLJ,EvisonG,HarknessJAL,MaddisonPJ.The arthropathyofsystemicsclerosis(scleroderma);comparison withmixedconnectivetissuedisease.ClinExpRheumatol. 1983;1:101–12.
8.RodnanGP,MedsgerTAJr.Therheumaticmanifestationsof progressivesystemicsclerosis(scleroderma).ClinOrthopRel Res.1968;57:81–92.
9.AllaliF,TahiriL,SenjariA,AbouqalR,Hajjaj-HassouniN. Erosivearthropathyinsystemicsclerosis.BMCPublicHealth. 2007;7:260.
10.FernandesSEM,MarquesNetoJF,FinettiRMI,SamaraAM. Manifestac¸õesosteoarticularesnaesclerosesistêmica.Rev BrasReumatol.1988;28(3):65–9.
11.SchmeiserT,Pons-KühnemannJ,ÖzdenF,Müller-LadnerU, DinserR.Arthritisinpatientswithsystemicsclerosis.EurJ InternMed.2012;23:25–9.
distinctgenetic,serologicalandclinicalentity.Rheumatology. 2007;46:989–93.
13.CoustetB,DieudeP,WipffJ,AvouacJ,HachullaE,DiotE,etal. Associationstudyof3rheumatoidarthritisrisklociin systemicsclerosisinaEuropeancaucasianpopulation.Clin ExpRheumatol.2011;29(65):S6–9.
14.HoogenF,KhannaD,FransenJ,JohnsonSR,BaronM,Tyndall A,etal.2013classificationcriteriaforsystemicsclerosis:an Americancollegeofrheumatology/Europeanleagueagainst rheumatismcollaborativeinitiative.AnnRheumDis. 2013;72:1747–55.
15.LeRoyEC,MedsgerTAJr.Criteriafortheclassificationofearly systemicsclerosis.JRheumatol.2001;28(7):1573–6.
16.AletahaD,NeogiT,SilmanAJ,FunovitsJ,FelsonDT,Bingham COIII,etal.2010Rheumatoidarthritisclassificationcriteria. AnAmericanCollegeofRheumatology/EuropeanLeague AgainstRheumatismcollaborativeinitiative.Arthritis Rheum.2010;62(9):2569–81.
17.ValentiniG,D’AngeloS,RossaAD,BencivelliW,Bombardieri S.EuropeanSclerodermaStudyGrouptodefinedisease activitycriteriaforsystemicsclerosis.IV.Assessmentofskin thickeningbymodifiedRodnanskinscore.AnnRheumDis. 2003;62:904–5.
18.MedsgerTAJr.Naturalhistoryofsystemicsclerosisandthe assessmentofdiseaseactivity,severity,functionalstatus,and psychologicwell-being.RheumDisClinNorthAm.
2003;29:255–73.
19.ValentiniG,SilmanAJ,VealeD.Assessmentofdisease activity.ClinExpRheumatol.2003;21(S29):S39–41.
20.RannouF,PoiraudeauS,BereznéA,BaubetT,Le-GuernV, CabaneJ,etal.Assessingdisabilityandqualityoflifein systemicsclerosis:constructvaliditiesoftheCochinhand functionscale,healthassessmentquestionnaire(HAQ), systemicsclerosisHAQ,andmedicaloutcomesstudy36-item shortformhealthsurvey.ArthritisRheum.2007;57(1):94–102.
21.DellavanceA,GabrielAJr,CintraAFU,XimenesAC,Nuccitelli B,TabilertiBH,etal.IIConsensoBrasileirodeFator
AntinuclearemcélulasHep-2.RevBrasReumatol. 2003;43(3):129–40.
22.McClainMT,RamslandPA,KaufmanKM,JamesJA.Anti-Sm autoantibodiesinsystemiclupustargethighlybasicsurface structuresofcomplexedspliceosomalautoantigens.J Immunol.2002;168:2054–62.
23.SatoS,HamaguchiY,HasegawaM,TakeharaK.Clinical significanceofanti-topoisomeraseIantibodylevels determinedbyElisainsystemicsclerosis.Rheumatology. 2001;40:1135–40.
24.CodulloV,MorozziG,BardoniA,SalviniR,DeleonardiG,Pità O,etal.Validationofanewimmunoenzymaticmethodto detectantibodiestoRNApolymeraseIIIinsystemicsclerosis. ClinExpRheumatol.2007;25:373–7.
25.SebastianiM,GiuggioliD,VespriniE,CarusoA,FerriC. Successfultreatmentwithleflunomideofarthritisin systemicsclerosispatients.Rheumatology.2006;45:1175–6.
26.Sampaio-BarrosPD,BortoluzzoAB,MarangoniRG,RochaLF, DelRioAPT,SamaraAM,etal.Survival,causesofdeath,and prognosticfactorsinsystemicsclerosis:analysisof947 Brazilianpatients.JRheumatol.2012;39:1971–8.
27.SkareTL,LucianoAC,FonsecaAE,AzevedoPM.
Autoanticorposemesclerodermiaesuaassociac¸ãoaoperfil clínicodadoenc¸a.Estudoem66pacientesdosuldoBrasil.An BrasDermatol.2011;86(6):1075–81.
28.JezlerSFO,SantiagoMB,AndradeTL,AraujoNetoC,BragaH, CruzAA.Comprometimentodointerstíciopulmonarem portadoresdeesclerosesistêmicaprogressiva.Estudodeuma sériede58casos.JBrasPneumol.2005;31(4):300–6.
29.MoritaY,MuroY,SugiuraK,TomitaY,TamakoshiK.Results oftheHealthAssessmentQuestionnaireforJapanese
patientswithsystemicsclerosis–measuringfunctional impairmentinsystemicsclerosisversusotherconnective tissuediseases.ClinExpRheumatol.2007;25:367–72.
30.PopeJ.Measuresofsystemicsclerosis(Scleroderma).Arthritis CareRes.2011;63(S11):S98–111.
31.MerkelPA,HerlynK,MartinRW,AndersonJJ,MayesMD,Bell P,etal.Measuringdiseaseactivityandfunctionalstatusin patientswithsclerodermaandRaynaud’sphenomenon. ArthritisRheum.2002;46(9):2410–20.
32.GeorgesC,ChassanyO,MouthonL,TievK,ToledanoC,Meyer O,etal.ValidationofFrenchversionoftheScleroderma HealthAssessmentQuestionnaire(SScHAQ).ClinRheumatol. 2005;24:3–10.
33.DanieliE,AiròP,BettoniL,CinquiniM,AntonioliCM, CavazzanaI,etal.Health-relatedqualityoflifemeasuredby theShortForm36(SF-36)insystemicsclerosis:correlations withindexesofdiseaseactivityandseverity,disability,and depressivesymptoms.ClinRheumatol.2005;24:48–54.
34.HudsonM,Rojas-VillarragaA,Coral-AlvaradoP, López-GuzmánS,MantillaRD,ChalemP,etal.
Polyautoimmunityandfamilialautoimmunityinsystemic sclerosis.JAutoimmun.2008;31:156–9.
35.AgarwalSK,TanFK,ArnettFC.Geneticsandgenomicstudies inscleroderma(systemicsclerosis).RheumDisClinNorth Am.2008;34(1):17–40.
36.KoumakisE,DieudéP,AvouacJ,KahanA,AllanoreY.Familial autoimmunityinsystemicsclerosis–resultsofa
French-basedcase–controlfamilystudy.JRheumatol. 2012;39:532–8.
37.HemminkiK,LiX,SundquistJ,SundquistK.Familial associationsofrheumatoidarthritiswithautoimmune diseasesandrelatedconditions.ArthritisRheum. 2009;60(3):661–8.
38.JawaheerD,SeldinMF,AmosCI,ChenWV,ShigetaR, MonteiroJ,etal.Agenomewidescreeninmultiplex rheumatoidarthritisfamiliessuggestsgeneticoverlapwith otherautoimunediseases.AmJHumGenet.2001;68:927–36.
39.CaramaschiP,BiasiD,VolpeA,CarlettoA,CecchettoM, BambaraLM.Coexistenceofsystemicsclerosiswithother autoimmunediseases.RheumatolInt.2007;27:407–10.
40.McGettiganP,HenryD.Currentproblemswithnon-specific COXinhibitors.CurrPharmDes.2000;6(17):1693–724.
41.BrooksPM,KeanWF,KassamY,BuchananWW.Problemsof antiarthritictherapyintheelderly.JAmGeriatrSoc. 1984;32(3):229–34.
42.DaoussisD,LiossisSNC,TsamandasAC,KalogeropoulouC, KazantziA,SirinianC,etal.Experiencewithrituximabin scleroderma:resultsfroma1-year,proof-of-principlestudy. Rheumatology.2010;49:271–80.
43.LafyatisR,KissinE,YorkM,FarinaG,VigerK,FritzlerMJ,etal. Bcelldepletionwithrituximabinpatientswithdiffuse cutaneoussystemicsclerosis.ArthritisRheum. 2009;60(2):578–83.
44.SmithV,PraetJTV,VandoorenB,DerCruyssenBV,Naeyaert JM,DecumanS,etal.Rituximabindiffusecutaneous systemicsclerosis:anopen-labelclinicaland
histopathologicalstudy.AnnRheumDis.2010;69:193–7.
45.PhumethumV,JamalS,JohnsonSR.Biologictherapyfor systemicsclerosis:asystematicreview.JRheumatol. 2011;38:289–96.
46.BoselloS,DeSantisM,TolussoB,ZoliA,FerraccioliG.Tumor necrosisfator-␣inhibitortherapyinerosivepolyarthritis
secondarytosystemicsclerosis.AnnInternMed. 2005;143(12):918–20.
48.DistlerJHW,JordanS,AiròP,Alegre-SanchoJJ,AllanoreY, GurmanAB,etal.IstherearoleforTNF-␣antagonistsinthe
treatmentofSSc?EUSTARexpertconsensusdevelopment usingtheDelphitechnique.ClinExpRheumatol.
2011;29(65):S40–5.