O
r
IG
IN
A
l
A
r
T
IC
lE
ABSTRACT
HepatitisBandCareimportantcausesofmorbidityandmortalityworldwide.InBrazil,according totheMinistryofHealth,about15%ofpopulationisinfectedbyhepatitisBvirus(HBV)andless than1%byhepatitisCvirus(HCV).Nevertheless,theage-specificprevalenceofHBVandHCV markersremainsunknown.ThisstudyaimedtodeterminetheseroprevalenceofHBVandHCV markersofinfectionandimmunityinchildrenandadolescentsbetween10to16yearsoldwholive inthemetropolitanareaofFlorianópolis,stateofSantaCatarina,SouthofBrazil.Threehundred andeightyfourindividualswereenrolledinthisstudy.SerologicalmarkersforHBVandHCV(HB- sAg,totalanti-HBc,anti-HBcIgM,anti-HBsandanti-HCV)weredeterminedthroughMicropar-ticleEnzymeImmunosorbantAssay(MEIA)-AxSYMSystem®-byusingcommercialdiagnostic kits(AbbottLaboratories,AbbottPark,Illinois,USA).All384adolescents(100%)werenegativefor HBsAgandanti-HBcIgM.Onlytwo(0.52%)werepositivefortotalanti-HBc.Amongthestudied individuals,226(58.85%)presentedtitersofanti-HBs≥10.0mIU/mL,121(31.51%)presentedanti HBs<10.0mIU/mL,and37(9.64%)didnotpresenttitersofanti-HBs.Regardingtoanti-HCV,all 384adolescents(100%)presentednegativeresultsforthismarker.Inconclusion,thisstudyshowed alowprevalenceofHBVandHCVinfections.Inaddition,itwasverifiedagreatnumberofchildren andadolescents(89.84%)whowerepositivefortheimmunitymarkeranti-HBs,implyingthatthe NationalImmunizationProgramProtocolforhepatitisBhasbeeneffectiveinthestudiedregion. Keywords:HBV,HCV,HBsAg,anti-HBs,anti-HBc,anti-HCV,seroprevalence.
[Braz J Infect Dis 2010;14(1):60-65]©ElsevierEditoraLtda. Authors
AndréiaRoyerVoigt1
MiguelStrazerNeto2
CelsoSpada1
ArícioTreitinger1 1ClinicalAnalysis
Department,Health SciencesCenter, UniversidadeFederal deSantaCatarina, Florianópolis,Santa Catarina,Brazil
2HospitalofUniversidade
FederaldeSantaCatarina, Florianópolis,Santa Catarina,Brazil
Submittedon:08/14/2009 Approvedon:11/30/2009
Correspondence to:
Dr.ArícioTreitinger UniversidadeFederalde SantaCatarina,Health ScienceCenter,Clinical AnalysisDepartment, CampusUniversitário Trindade
Florianópolis–SC88010-970–Brazil.
Phone:+55(48)37219712. Fax:+55(48)37219542 E-mail:[email protected]
Wedeclarenoconflict ofinterest.
Seroprevalence of hepatitis B and hepatitis C markers
among children and adolescents in the south brazilian
region - metropolitan area of Florianópolis, Santa Catarina
INTRODUCTION
HepatitisBvirus(HBV)andhepatitisCvirus (HCV)infectionsarethemostcommoncauses of liver disease worldwide.1 Both viruses can
betransmittedparenterally,sexuallyandperi-natally,withperinatalandsexualtransmission beingmorecommonforHBV2,3thanforHCV.4
Despiteprogressonprophylaxis,diagnosticand treatmentoftheseinfections,theystillareone of the major causes of chronicle liver disease, suchcirrhosisorhepatocellularcarcinoma.5,6
AccordingtotheWorldHealthOrganiza-tion (WHO) it is estimated that, currently, morethan2billionoftheglobalpopulation had been infected with HBV. Out of these, approximately360millionarechronicallyin-fectedandatriskofseriousillnessanddeath fromlivercirrhosisandlivercancer,diseases thatareestimatedtocause500,000to700,000 deathseachyearworldwide.7
Also according to WHO estimates, about 170millionpeople,3%oftheworld’spopula-tion,areinfectedwithHCVandareatriskof developinglivercirrhosisand/orlivercancer.8
InBrazil,theMinistryofHealthestimates that15%ofthepopulationhavebeenincon- tactwithHBVandnotlessthan1%ofthepop-ulationhaschronicdisease.9However,thereare notmanystudiesrevealingtherealprevalence of HCV among Brazilians.10 Data obtained from blood donor banks, in 2002, showed a differentdistributionoftheillnessamongBra-zilianregions.IntheNorthregionwasfound anincidenceof0.62%,intheNortheast0.55%, in the West-Center 0.28%, in the Southeast 0.43%andintheSouth0.46%.11
DuetoBrazilian’sterritorialextensionand its economic and cultural differences, hepati-tisBandCinfectionratesaredifferentineach region.11 Epidemiologic studies regarding to
uncommon.Ingeneral,suchstudiesfocustheincidence ratherthanprevalence,likeinthestudyofCharleset al., which demonstrated the incidence of hepatitis B in the SouthregionofBrazilfromtheyearof1997to1999.12
The main reason for the predominance of incidence studies rest in the way how the data are collected. The termincidencereferstothenumberofnewcasesofin-fection, emerged in a certain population, at determined intervaloftime.Therefore,incidencestudiesdonotneed deal with population directly, because this information is obtained from health public organization, like Epide-miologicVigilance.Ontheotherhand,theprevalenceis established by the total number of positive cases of in-fection, in a certain population at specific time.And to gettheprevalencerates,testswithpopulationareneeded. In fact, the difficulty in gathering the needful number of blood samples among the ordinary population is the mainreasonforthislackofprevalencestudies.13So,these studies are almost always performed in specific groups, likeblooddonors14-17orHIV-seropositivepatients.18,19
HepatitisBandCareimportantdiseasesandhaveseri- ousconsequences.Preventionisthebestalternativetocon-troltheirspreading.ForhepatitisCthereisnotavaccine, anditspreventionisreachedonlybyeducationalprograms, butforhepatitisBvaccinationexistsandisessential.The preventionofhepatitisBbyvaccinationisoneofthemost efficienttoolstoavoidthetransmissionofthevirus.
In1989,thevaccinationagainsthepatitisBbeganin some regions of Brazil, for specific groups. Some years later, it was enlarged to more regions and to children youngerthanoneyearold,aswellastohighriskpopu- lations.Afterwards,thecoverageofthevaccinewasam-plified for health students and militaries, and then, for adolescentsupto15yearsoldinsomeFederalStates.Re-garding specifically to Santa Catarina state, in 1993 the vaccinationwasrecommendedtochildrenyoungerthan fouryearsold,andin1996,tochildrenuptofifteenyears old. In 2001 the immunization was extended to whole Brazilianterritory,comprehendingthepopulationupto nineteenyearsold.11
ThisstudyaimedtodeterminetheprevalenceofHBV andHCVinfectionsinchildrenandadolescentsbetween 10and16yearsoldwholiveinthemetropolitanareaof Florianópolis, state of Santa Catarina, in South of Bra-zil. For this purpose, serological assays of hepatitis B surface antigen (HBsAg), antibodies to hepatitis B core antigen(totalanti-HBcandanti-HBcIgM),andhepatitis C antibody (anti-HCV) were performed. Moreover, one pretends to determine the prevalence of the marker for immunity to hepatitis B in the same population, using antibodytohepatitisBsurfaceantigen(anti-HBs),allow- ingoneevaluatestheeffectivenessoftheNationalImmu-nizationProgramProtocolforhepatitisB.
MATERIAL AND METHODS
The studied group was formed by children and adoles- centsbetween10to16yearsold,residentsinthemetro-
politanareaofFlorianópolis,whosebloodwastested,re-gardlessthereason,intheClinicalAnalysisLaboratories ofthesameregion.Anadditionalamountofbloodwas drawnfromthesamevenouspuncturesiteusedtocollect theoriginalsampleforthetestingassignedtothepatient at the Clinical Analysis Laboratory. The blood samples wereobtainedbetweenMay2007andAugust2008in14 ClinicalAnalysisLaboratoriesdistributedaroundthere-gionofinterest.
The study was approved by the Ethical Committees of the Federal University of Santa Catarina (Project nº 351/2006). A written informed consent was obtained from the legal responsible persons of each participant since all subjects were under the legal majority age (18 yearsold).
Theminimumnumberofsamplesnwasdefinedby20
whereα is the confidence interval,z is the corresponding valueofαatnormalcurve,pistheprobabilityoffindingthe studiedphenomenon,q (q = 1-p)isthecomplementarypart ofprobability,andEistheadmissibleerror.Inthisstudya confidenceintervalof95%wasadopted.Thus,α =0.05and
z = 1.96. Unknown prevalence markers at studied popu-lation makes p equals 50% (p = 0.5) and, consequently,
q equals 0.5. The admissible error was bounded in 5% (E =0.05).Usingsuchcriteriatheminimumsamplenumber wasdefinedas384,numberreachedattheendofthestudy.
Thecollectedbloodsampleswerecentrifugedtosepa-ratetheserum,whichwasforwardedthentolaboratorial analysis.SerologicalmarkersforHBVandHCV(HBsAg, total anti-HBc, anti-HBc IgM, anti-HBs and anti-HCV) were determined through Microparticle Enzyme Im-munosorbantAssay(MEIA)-AxSYMSystem®,byusing commercialdiagnostickits(AbbottLaboratories,Abbott Park, Illinois, USA) and following the instructions pro-vided by the producer. All laboratory assays were per-formedattheClinicalAnalysisLaboratoryofUniversity HospitalofFederalUniversityofSantaCatarina,inFlori-anópolis.Then,prevalenceofeachserologicalmarkerwas establishedaccordingtosex.
RESULTS
Table 1. Demographic study population
Adolescents
Sex (n = 384)
male 163 (42.45%)
female 221 (57.55%)
Age at enrollment (years; mean ± D) 12.59 ± 2.02
residential location
Florianópolis 241 (62.76%)
Metropolitan area 143 (37.24%)
Table 2. Prevalence of HBsAg according to sex
Sex HBsAg (+) HBsAg (-)
male 0 (0%) 163 (42.45%)
female 0 (0%) 221 (57.55%)
Total 0 (0%) 384 (100%)
*HBsAg: hepatitis B surface antigen
Table 3. Prevalence of anti-HBc IgM according to sex
Sex anti-HBc IgM (+) anti-HBc IgM (-)
male 0 (0%) 163 (42.45%)
female 0 (0%) 221 (57.55%)
Total 0 (0%) 384 (100%)
*Anti-HBc IgM: antibody (immunoglobulin M) to hepatitis B core antigen
Table 4. Prevalence of total anti-HBc according to sex
Sex total anti-HBc (+) total anti-HBc (-) Total
male 2 (0.52%) 161 (41.93%) 163 (42.45%)
female 0 (0%) 221 (57.55%) 221 (57.55%)
Total 2 (0.52%) 382 (99.48%) 384 (100%)
*Total anti-HBc: antibodies (immunoglobulin M and G) to hepatitis B core antigen
Table 7. Prevalence of anti-HCV according to sex
Sex anti-HCV (+) anti-HCV (-)
male 0 (0%) 163 (42.45%)
female 0 (0%) 221 (57.55%)
Total 0 (0%) 384 (100%)
*Anti-HCV: hepatitis C antibody
Table 5. Prevalence of anti-HBs according to sex
Sex anti-HBs = 0.0 mIU/mL 0.0 > anti-HBs < 10.0mIU/mL anti-HBs ≥ 10.0mIU/mL Total
male 17 (4.43%) 50 (13.02%) 96 (25%) 163 (42.45%)
female 20 (5.21%) 71 (18.49%) 130 (33.85%) 221 (57.55%)
Total 37 (9.64%) 121 (31.51%) 226 (58.85%) 384 (100%)
* Anti-HBs: antibody to hepatitis B surface antigen
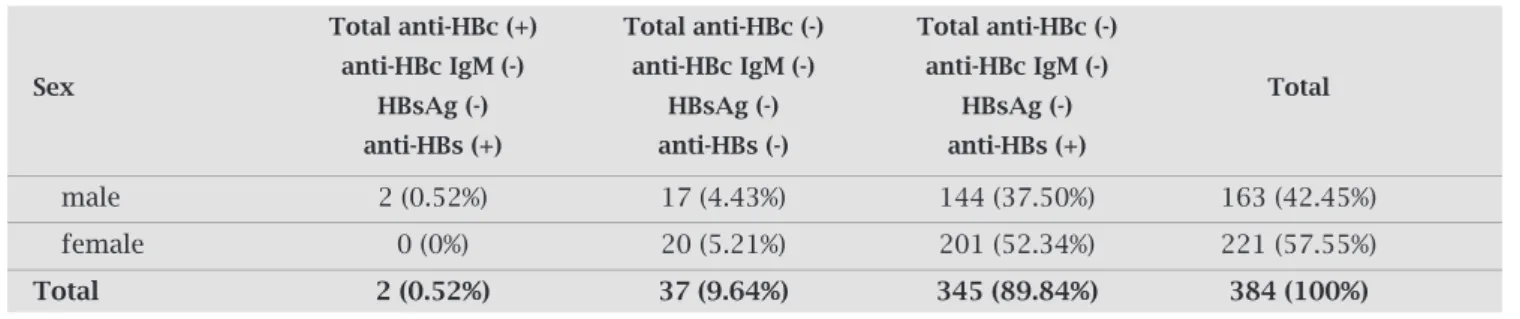
Table 6. Comparison of HBV markers prevalence according to sex
Total anti-HBc (+) Total anti-HBc (-) Total anti-HBc (-)
Sex anti-HBc IgM (-) anti-HBc IgM (-) anti-HBc IgM (-) Total
HBsAg (-) HBsAg (-) HBsAg (-)
anti-HBs (+) anti-HBs (-) anti-HBs (+)
male 2 (0.52%) 17 (4.43%) 144 (37.50%) 163 (42.45%)
female 0 (0%) 20 (5.21%) 201 (52.34%) 221 (57.55%)
Total 2 (0.52%) 37 (9.64%) 345 (89.84%) 384 (100%)
*Total anti-HBc: antibodies (immunoglobulin M and G) to hepatitis B core antigen; *anti-HBc IgM: antibody (immunoglobulin M) to hepatitis B core antigen; *HBsAg: hepatitis B surface antigen; *anti-HBs: antibody to hepatitis B surface antigen
DISCUSSION
According to the Ministry of Health, the South of Brazil isconsideredalowprevalenceregionofhepatitisBinfec-tion (less than 2% of populaisconsideredalowprevalenceregionofhepatitisBinfec-tion is positive for HBsAg). Nevertheless, there are exception for the west region of Santa Catarina, classified as a moderate prevalence region (between 2% and 7% of HBsAg positive) and the west of Paraná,whichpresentshighprevalencelevels(higherthan 7% of HBsAg positive) of hepatitis B infection.11 The few
prevalencestudiesinBrazilhaveshowedlownumbersfor itsinfectionmarkers.13-15,17Mirandaet al.13 establishedprev-alence of hepatitis B serological markers among 632 indi-vidualssubmittedtobloodtestsinhealthcentersofRibeirão Preto,SãoPaulo.Suchdatawerecollectedbetween1994and 1995.Theyfound0.3%ofprevalenceforHBsAg,specifically foundintwoindividualsagedmorethan60years.Regard- ingtoanti-HBc,itwasfoundaprevalenceof13.9%.How-ever,therewasnocaseofpositiveanti-HBcintheage-group of10to19yearsold.
Furthermore,prevalenceofHBVinfectionmarkershas beendecreasinginlastyears.14,17,21Silveiraet al.,21inastudy ofhepatitisBseroprevalenceinLatinAmerica,carriedout in1994to1997,describedawiderangeofseroprevalences inthedifferentregionsofBrazil,withahighrateinMan- aus(21%),followedbyPortoAlegre(7.5%),RiodeJanei-ro (5.5%), and Fortaleza (1.2%). Rosiniet al.17 estimated prevalenceofserologicalmarkersforHBVinfectionamong blooddonorsinSantaCatarinaintheyearsof1999,2000 and2001.TheyfoundHBsAgprevalenceof0.98%(1999), 0.84%(2000)and0.64%(2001),andanti-HBcprevalence of8.83%(1999),7.09%(2000)and5.35%(2001).
Recently, the Brazilian Ministry of Health, with some Universities’help,hadrealizedaseroprevalencestudyabout viralhepatitis,inthecapitalofeachstate.Someresultswere alreadypresented.22Accordingtothisinquiry,intheSouth region,ananti-HBcprevalenceof1.18%wasfoundforado-lescentsbetween10and19yearsold,and11.2%foradults between20and69yearsold.Foranti-HBs,theprevalence were0.12%foradolescents,and0.5%foradults.
TheresultsrepresentprevalenceofhepatitisBinurban population,andinthiscaseattentionisneeded,sinceitis factthathigherprevalenceusuallyisfoundincountryside, especiallyAmazonregion,southofEspíritoSanto,westof ParanáandSantaCatarina,regionsnotcontemplatedatthe study.22
Inthepresentstudy,averylowprevalenceofHBVinfec-tionwasfound,likeinthestudiespresentedbefore.Onlytwo individuals(0.52%)presentedaninfectionmarkerofhepati-tisB(totalanti-HBc)positive.Furthermore,theypresented negativeresultsforanti-HBcIgMandHBsAg.Theanti-HBc IgM negative means that contact was not recent, whereas the HBsAg negative means that virus was depurated of the organism.Suchresultscharacterizeapastcuredinfection.
Regarding to immunity, the majority of the studied populationinthiswork(58.85%)presentedtitersofanti-HBs≥ 10.0mIU/mL,criterionadoptedtoestablishprotec-tiveconcentrations.23-25Moreover,31.51%oftheindividuals presented anti HBs < 10.0mIU/mL. The remainder 9.64% didnotpresenttitersofanti-HBs.
Theanti-HBsisresponsiblefortheimmunityagainst HBV. In addition to cured infections, it is generally ac-quired through vaccination. Primary vaccination with a three-dose series of hepatitis B vaccine results in sero-protection (defined as the development of anti-HBs at a concentration greater than 10 mille International Units per milliliter [mIU/mL]) in > 95% of vaccinated infants and children.23-25 However, following completion of the primary series, anti-HBs concentrations decline and may fallbelow10.0mIU/mLafterseveralyears.Despitethecri-terion adopted to establish protective concentrations of anti-HBs(≥ 10.0mIU/mL),recentstudiesarguetheimmu-nologicmemorywouldbecapableofpreventingchronic orsymptomaticinfectionsevenafteranti-HBsdeclinesto undetectableconcentrationsinvaccinatedones.26-34
Basedonpreviousdiscussion,oneconcludesthatallin-dividualsinthisstudy,whopresentedpositivetitersofanti HBsandwerenegativeforinfectionmarkers(89.84%),may havebeenvaccinated(Table6).However,thesamplewasnot randomandisnotpopulation-based,soitcouldnotberep- resentativeofthepopulation.ConcerningtoBrazilianIm-munizationProgram,thevaccinationcoverageforhepatitis BinthestateofSantaCatarinahasreached95%inthelast years,forinfantsunderoneyearold.Ontheotherhand,the rangeofvaccinationcoverageforchildrenandadolescentsis notavailableforthispopulation.35
TheSecretariatofEpidemiologicVigilance,department subordinate to the Brazilian Ministry of Health, does not haveadatabasereferenttothevaccinationprogram.Perti-nentinformationsuchaswhowasvaccinated,whetherthe vaccinationschedulewascompletedandwhenitwasaccom-plishedcanbeobtainedjustthroughvaccinationcards.Since themajorityoftheadolescentsenrolledinthisstudydidnot presentthevaccinationcards,itisnotknowifindividuals withouttitersofanti-HBs(9.64%)representnot-vaccinated individuals,iftheywerevaccineprimarynonrespondersor if their antibodies titers declined over time. Even though thevaccinationcardswereavailable,itwouldnotbepossi-bletohavesureaboutthisinformation,becauseSecretariat ofHealthdoesnothavecontrolintheexpeditionofthese cards,anditiscommonpeoplehavemorethanone.
infectionmarkers,onlyonechildpresentedanti-HBcposi-tiveintheItalianstudy,31comparedtotwofoundinours.In bothstudies,therewasnocaseofHBsAgpositive.
Regarding to HCV infection, in the present study, all 384adolescents(100%)werenegativeforthismarker(an-ti-HCV), which means none infection case in the studied population.SuchresultwasnotsurprisingduetotheHCV modes of transmission and the age-group of the studied population.Infact,oneofthefewBrazilian’sstudiesabout hepatitis C prevalence, carried out in São Paulo, demon-stratedanestimatedHCVprevalenceof1.42%.Thisspecific infectionoccurredmorefrequentlyamongadults30years ofageorolder,withtheprevalencereachingapeakof3.80% amongthegroupaged50to59years.36Inaddition,Rosini et al.17 estimatedtheanti-HCVprevalenceamongblooddo-norsinSantaCatarina,intheyearsof1999,2000and2001. Theyfoundaprevalenceof0.41%inFlorianópolisregion; numberalittlebithigherthanfoundinthestateofSanta Catarinaasawhole(0.35%).
ThelackofdatarelativetochildandadolescentsinBra-zilmakesdifficultadeepcomparisonoftheresultsobtained inthisstudy.Mostofstudiesdealwithspecificgroups.The prevalencefoundinstudieswithblooddonors,forexample, referstoanage-grouphigherthantheobjectofthepresent study,sincetheminimumageforblooddonoris18years old. On the other hand, HIV seropositive groups are not good representatives for a population in general because theyrefertoagroupofindividualswithahighriskofHBV andHCVinfectionduetothecommonmodesoftransmis- sionbetweensuchdiseases.Hence,morestudieswithchil- drenandadolescentsareneededtoconfirmtheresultsob-servedinthepresentstudy.
However,therecentMinistryofHealth’sinquirybrings someinformationregardingtoanti-HCV.Aprevalenceof 1.63%foradolescentsbetween10and19yearsold,andof 1.98%foradultsbetween20and69yearsoldwerefound. For HCV, there are not studies revealing differences on prevalenceincountrysidecomparedtocitieslocatedatbig urbancenters.24
Despite the uncertainties, the results observed in this studyrevealagoodperspectiveforthefuture.Alowpreva-lence of HBV and HCV infection and a high prevastudyrevealagoodperspectiveforthefuture.Alowpreva-lence of HBV immunity among children and adolescents show progresstowardsthecontrolofhepatitisBandCinfections inBrazil.However,itisimportanttokeeporevenimprove educationalprograms,especiallybecausethereisnotavac-cine for the HCV prevention.As a matter of fact, diseases which have the same mode of transmission, like hepatitis B, hepatitis C andAIDS, could share the same prevention campaigns.
CONCLUSION
In conclusion, this study showed a low seroprevalence of HBVandHCVinfectionsamongchildrenandadolescents in the metropolitan area of Florianópolis, Santa Catarina, SouthofBrazil.Inaddition,alargenumberofindividuals
presentedtitersoftheseroprotectionmarkeranti-HBs,im-plying that National Immunization Program Protocol for hepatitisBhasbeeneffectiveinthestudiedregion.Besides low prevalence of HBV and HCV infections, prevention campaigns are important to remind children and adoles-centshowtheseinfectionscanbeprevented,mainlyHCV, whichdoesnothaveavaccineforitsprevention.
REFERENCES
1.
RehermannB,NascimbeniM.ImmunologyofhepatitisBvi-rusandhepatitisCvirusinfection.NatRevImmunnol2005; 5:215-29.
2. BondWW,PetersenNJ,FaveroMS.ViralhepatitisB:aspects ofenvironmentalcontrol.HealthLabSci1977;14:235-52. 3.
AlterMJ,MargolisHS.TheemergenceofhepatitisBasasexu- allytransmitteddisease.MedClinNorthAm1990;74:1529-41.
4. Tahan V, Karaca C, Yildirim Bet al. Sexual transmission of
HCVbetweenspouses.AmJGastroenterol2005;100:821-24. 5.
ParkinDM,BrayF,FerlayJ,PisaniP.Estimatingtheworldcan-cerburden:Globocan2000.IntJCancer2001;94:153-6. 6. FattovichG,StroffoliniT,ZagniI&DonatoF.Hepatocellular
carcinomaincirrhosis:incidenceandriskfactors.Gastroen-terology2004;127:(suppl)S35-S50.
7. WorldHealthOrganization.Programmesandprojects-Im-munization service delivery and accelerated disease control –Newvaccinesandtechnologies-HepatitisB.2008.(http:// www.who.int/immunization_delivery/new_vaccines/hepb/ en/index.html).
8. WorldHealthOrganization.Programmesandprojects–Me-diacentre-Factsheetn°164-HepatitisC.2000.(http://www. who.int/mediacentre/factsheets/fs164/en/).
9. HepatiteB:Glossáriodedoenças.ProgramaNacionaldeHep-atites Virais.
(http://portal.saude.gov.br/portal/saude/visuali-zar_texto.cfm?idtxt=27151)(in portuguese).
10. HepatiteC:Glossáriodedoenças.ProgramaNacionaldeHep-atites Virais.
(http://portal.saude.gov.br/portal/saude/visuali-zar_texto.cfm?idtxt=27220)(in portuguese).
11. Brasil.MinistériodaSaúde.SecretariadeVigilânciaemSaúde. Materialinstrucionalparacapacitaçãoemvigilânciaepidemi-ológicadashepatitesvirais.Brasília,DF:MinistériodaSaúde,
2008(in portuguese).
12. ChávezJH,CampanaSG,HaasP.PanoramadehepatiteBno BrasilenoEstadodeSantaCatarina.RevPanamSaludPublica 2003;14(2):91-6.
13. MirandaLVG,PassosADC,FigueiredoJFCet al.Marcadores
sorológicosdehepatiteBemindivíduossubmetidosaexames de sangue em unidades de saúde. Journal of Public Health 2000,34(3):286-91.
14. Andrade AFB, Silva MO, Silva SGCet al. Seroprevalence of
hepatitisBandCvirusmarkersamongblooddonorsinRio deJaneiro,Brazil,1998-2005.MemInstOswaldoCruz2006, 101(6):673-6.
15. Nascimento MC, Mayaud P, Sabino ECet al. Prevalence of
hepatitisBandCserologicalmarkersamongfirst-timeblood donorsinBrazil:amulti-centerserosurvey.JMedVirol2008; 80:53-7.
16. Treitinger A, Spada C, Ferreira LAPet al. Hepatitis B and
17. Rosini N, Mousse D, Spada C. Treitinger A. Seroprevalence ofHBsAg,anti-HBcandanti-HCVinSouthernBrazil,1999-2001.BrazJInfectDis2003;7(4):262-7.
18. TreitingerA, Spada C, Silva ELet al. Prevalence of serologic
markersofHBVandHCVinfectioninHIV-1seropositivepa-tientsinFlorianópolis-Brazil.BrazJInfectDis1999;3(1):1-5. 19. PereiraRARA,MussiADH,SilvaVCA,SoutoFJD.HepatitisB
virusinfectioninHIV-positivepopulationinBrazil:resultsof asurveyinthestateofMatoGrossoandacomparativeanaly-siswithotherregionsofBrazil.BMCInfectDis2006;6:34. 20. MottaVT,WagnerMB.Bioestatística.CaxiasdoSul,RS:Educs;
SãoPaulo,SP:RobeEditorial,2003.(in portuguese).
21. SilveiraTR,FonsecaJC,RiveraLet al
.HepatitisBseropreva- lenceinLatinAmerica.PanAmJPublicHealth1999;6(6):378-83.
22.
Inquéritonacionaldehepatitesvirais.2009.(http://www.hep-to.com)(in portuguese).
23. CentersforDiseaseControl.RecommendationoftheImmu-nization PracticesAdvisory Committee (ACIP). Recommen-dations for protection against viral hepatitis. Morb Mortal WklyRep1985;34:313-24,329-35.
24. CentersforDiseaseControl.RecommendationsoftheImmu-nizationPracticesAdvisoryCommittee.UpdateonhepatitisB prevention.MorbMortalWklyRep1987;38:353-60,366. 25. InternationalGroup.ImmunizationagainsthepatitisB.Lancet
1988;1:875-876.
26. WestDJ,CalandraGB.Vaccineinducedimmunologicmem-oryforhepatitisBsurfaceantigen:implicationsforpolicyon boostervaccination.Vaccine1996;14(11):1019-27.
27. Banatvala J, Van Damme P, Oehen S. Lifelong protection againsthepatitisB:theroleofvaccineimmunogenicityinim-munememory.Vaccine2001;19:877-85.
28. WangRX,BolandGJ,HattumJV,DeGastGC.Longtermper- sistenceofTcellmemorytoHBsAgafterhepatitisBvaccina-tion.WorldJGastroenterol2004;10(2):260-3.
29. McMahonBJ,BrudenDL,PetersenKMet al.Antibodylevels
and protection after hepatitis B vaccination: results of a 15-yearfollow-up.AnnInternMed2005;142:333-41.
30. Dentinger CM, McMahon BJ, Butler JCet al. Persistence of
antibody to hepatitis B and protection from disease among Alaskanativesimmunizedatbirth.PediatrInfectDisJ2005; 24:786-92.
31. ZanettiAR,MarianoA,RomanòLet al
.Long-termimmuno-genicityofhepatitisBvaccinationandpolicyforbooster:an Italianmulticentrestudy.Lancet2005;366:1379-84.
32. FerreiraCT,SilveiraTR.Viralhepatitispreventionbyimmuni-zation.J.Pediatr2006;82(3)suppl:S55-S66.
33. GiambiC,BellaA,BaraleAet al.Acohortstudytoevaluate
persistence of hepatitis B immunogenicity after administra-tionofhexavalentvaccines.BMCInfectDis2008;8:100. 34. Bialek SR, Bower WA, Novak R. Persistence of protection
against hepatitis B virus infection among adolescents vacci-natedwithrecombinanthepatitisbvaccinebeginningatbirth: a15-yearfollow-upstudy.PediatrInfectDisJ2008;27:881-5. 35. Brasil.MinistériodaSaúde.SecretariadeVigilânciaemSaúde.
Sistemanacionaldevigilânciaemsaúde:relatóriodesituação
-SantaCatarina.Brasília,DF:MinistériodaSaúde,2007(in
portuguese).
36. FocacciaR,ConceiçãoOJ,SetteHJet al.Estimatedprevalence