169
Original Article
REVISTA PAULISTA DE MEDICIN AHypomagne se mia in short
bowe l syndrome patie nts
Division of Clinical Nutrition, Department of Internal Medicine, Hospital das Clínicas,
Faculdade de Medicina de Ribeirão Preto, Universidade de São Paulo, Ribeirão Preto, Brazil
a b s t r a c t
CO N TEX T: Mag nesium suppo rt to small bo wel resectio n patients.
O BJECTIVE: Incidence and treatment o f hypo mag nesemia in patients with extensive small bo wel resectio n.
DESIGN : Retro spective study.
SETTIN G: Metabo lic Unit o f the University Ho spital Medical Scho o l o f Ribeirão Preto , University o f São Paulo , Braz il.
PATIEN TS: Fifteen patients with extensive small bo wel resectio n who develo ped sho rt bo wel syndro me.
M AIN M EASUREM EN TS: Serum mag nesium co ntro l o f patients with bo wel resectio n. Replacement o f mag nesium when lo w values were fo und.
RESULTS: Initial serum mag nesium values were o btained 2 1 to 1 8 0 days after surg ery. Hypo mag nesemia [serum mag nesium belo w 1 .5 mEq/ l (SD 0 .4 3 )] was detected in 4 0 % o f the patients [1 ,1 9 mEq/ l (SD 0 .2 2 )]. During the fo llo w-up perio d, 6 6 % o f the patients pre-sented a t lea st two va lues b elo w referenc e (1 .5 0 mEq / l). 4 0 % increased their serum values after mag nesium therapy.
CO N CLUSIO N : Metabo lic co ntro l o f serum mag nesium sho uld be fo llo wed up after extensive small bo wel resectio n. Hypo mag nesemia may be fo und and sho uld be co ntro lled.
KEY W O RDS: Hypo mag nesemia. Small g ut syndro me. Intestine. N utritio n suppo rt.
• Simo ne Chaves Miranda • Michelle Liz z y Bandeira Ribeiro • Eduardo Ferrio lli • Júlio Sérg io Marchini
INTRODUCTION
Magnesium is the fo urth mo st abundant catio n in the blo o d. Its existence in animals was detected aro und 1859. Magnesium deficiency was described in the early 1930s. Magnesium depletio n has been fo und in alc o h o lic s an d o th e r p atie n ts afte r lo n g ho spitalizatio n.1,2,3 The human bo dy has 25 to 30 grams
o f magnesium, but values o f up to 40 g have been described. It is co ncentrated in bo nes, which co ntain abo ut 24 g (50 to 60% intracellular); 1% o f the to tal bo dy magnesium po o l is fo und in the blo o d plasma (50% free and 1/3 bo und to albumin).1
The Reco mmended Dietary Allo wance (RDA) fo r magnesium ranges fro m 280 to 350 mg o r 23 to 30 mEq /day.4
Magnesium ab so rptio n o ccurs all o ver the entire gastro intestinal tract, b ut mainly in the ileum and co lo n. There is evidence to suppo rt the secretio n o f this io n b y the duo denum. Cellular mag-nesium transpo rt o ccurs thro ugh active and passive mechanisms and is inhib ited b y calcium, alco ho l, pho sphate, phytates and fat, and stimulated b y vita-min D. Renal excretio n is inversely pro po rtio nal to extracellular co ncentratio n.2,5 The impo rtant ro le o f
magnesium in human metab o lism can b e reco gnized thro ugh its functio ns as a stab ilizer o f ATP-depen-dent enzymatic reactio ns, as a co facto r o f circa 300 enzymes, as a mo dulato r in neuro muscular transmis-sio n and as an essential io n in cardiac phytransmis-sio lo gy.2,6
Its ac tio n o n the m yo c ard ium d uring is c he m ic episo des and reperfusio n injury after acute myo car-dium infarctio n have b een sho wn in studies such as the Seco nd Leicester Intraveno us Magnesium
170
ventio n Trial (LIMIT-2).7 It has also b een sho wn to
have b eneficial effects in the treatment o f cardiac arrythmia.8,9 A link b etween hypo magnesemia and
sudden death has b een stro ngly suggested and also
its co rrelatio n with higher numb ers o f ischemic epi-so des o r higher intake o f nitrates in ischemic pa-tie nts.8,9 The re is an inve rse re latio nship b e twe e n
m agne se m ia, d e aths and ho sp ital c are fo llo wing vascular o r co ro nary disease10,11,12. Magnesium
defi-ciency can also lead to premenstrual tensio n syn-d ro m e ansyn-d syn-d e p re ssio n as a re sult o f syn-d im inishe syn-d do pamine synthesis. It is o ne o f the micro nutrients related to fetal malfo rmatio n in lab o rato ry animals, either as an excess o r deficiency.2,6 Hypo magnesemia
is co mmo n amo ng patients who need intensive care and in the general po pulatio n.3,6
Magnesium administratio n must be do ne care-fully fo r patients with severe atrio ventricular blo ck and re nal insufficie ncy, as high le ve ls o f this io n m ay decrease the cardiac rate.7 Fo o d so urces o f
magne-sium are vegetables, ro o ts, seafo o d, nuts, cereals and milk pro ducts. Drinking water o ffers 1 - 16 ppm. This catio n is part o f chlo ro phyll and so is present in all green plants. Magnesium may be lo st during co o king. To retain this micro nutrient o ne sho uld co o k fo o d in small amo unts o f water and fo r the sho rtest time po ssible.1,5
This study had the aim o f e xam ining hypo -magnesemia incidence amo ng patients with extensive small bo wel resectio n, and fo llo wing up these patients during their ho spitalizatio n and treatment o f their deficiency.
METHODS
Fifteen patients fro m the Metabo lic Unit o f the University Ho spital o f the Medical Scho o l o f Ribeirão Preto Universidade de São Paulo , Brazil, were retro -sp e c tive ly re vie we d c o nc e rning the ir m agne sium status. All were submitted to extensive small bo wel resectio n (> 2 meters) and their small bo wel transit time was less than ten minutes. No ne o f the studied patients had any do cumented intestinal disease be-fo re surgery. The cause o f enterecto my in all patients was intestinal ischemia, either thro mbo sis o r embo li. Amo ng these 15 patients, 7 also had co lecto my, at least o f the ascending co lo n. The mo st extensive resectio n was o f the asce nding co lo n and transve rse co lo n. Values o f their first magnesium serum levels after s u rg e ry, th e fo llo w- u p o f s e ru m d ata d u rin g ho spitalizatio n and treatment o f the deficiency were analyzed. To treat the deficiency, at least twice the RDA value s (23 to 30 m Eq ) we re give n b y intrave no us infusio n, i.e. 10 ml o f magnesium sulfate 20%. The serum level o f magnesium fo r eutro phic subjects is 1.5 to 2.5 mEq/l.2
Sao Paulo Med J/Rev Paul Med 2000; 118(6):169-72. First and last dosages
Ma
gnesemia - mg/dl
Figure 3. Evolution of magnesemia in all patients. Initial value = 1.59 mEq/l (SD 0.43). End value = 1.72 mEq/l (SD 0.33).
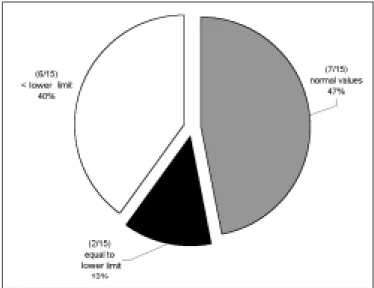
Figure 1. Percentage incidence of hypomagnesemia in the first magnesium determination after surgery.
First and last dosages
Ma
gnesemia - mg/dl
171
RESULTS
Initial plasma magnesium values [mean 1.59 mEq /l (SD 0.43)] were o b tained fro m 21 to 180 days after surgery, 45 days o n average. Magnesemia in the first co llectio n varied fro m 0.85 to 2.17 mEq /l and was lo w in 6 (40%, 1.19 mEq /l SD 0.22) patients o ut o f 15. Two patients (13.3%) had magnesium plasma levels at the lo wer limit (Figures 1, 2 and 3). There was no relatio nship b etween resectio n o f the co lo n and hypo magnesemia. Patients with no rmal magnesemia were o n average mo nito red o n the twentieth po st-o perative day, i.e. earlier than the st-o thers. Of thst-o se eight patients who had magnesemia eq ual to o r less than the lo wer do sage limit, o nly two received supple-ments when diagno sis was kno wn. During ho spital-izatio n with nutritio nal suppo rt therapy, 10 o ut o f the 15 patients fo llo wed sho wed serum magnesium b e-lo w the e-lo wer limit, o n at least two o ccasio ns. Fro m these, o nly fo ur received specific treatment fo r hy-p o m a g n e s e m ia . N o hy-p a tie n t hy-p re s e n te d hypermagnesemia.
DISCUSSION
The status o f se rum m agne sium afte r large b o wel resectio n surgery may affect patients’ treat-ment and fo llo w-up. Hypo magnesemia can b e fo und just after surgery o r during fo llo w-up o f such patients. A seq uence o f lo w values o f serum magnesium was fo und in 10 o ut o f o ur 15 patients, under o ur co n-tinuo us lo ng term study pro gram o f these patients. It is impo rtant to reco gnize that pro lo nged parenteral nutritio n alo ne wo uld no t explain the fall o f magne-sium levels, as the patient received the reco mmended daily allo wances.4 Magnesium nutritio n co ntro l has
Sao Paulo Med J/Rev Paul Med 2000; 118(6):169-72.
1. Dutra-de-Oliveira JE, Marchini JS. Ciências Nutricio nais. São Paulo : Sarvier; 1998.
2. Shils ME, Olso n JA, Shike M. Mo dern Nutritio n in: Health and Disease, 8th ed. Philadelphia: USA; 1994.
3. Britto n J, Pavo rd I, Richards K, et al. Dietary magnesium, lung functio n, wheezing, and hyper-reactivity in a rando m adult po pulatio n sample. Lancet 1994;344:357-62.
4. Natio nal Research Co uncil. Fo o d and Nutritio n Bo ard. Reco mmended Dietary Allo wances: 10th revised Editio n. Washingto n, DC: Natio nal
Academy o f Sciences; 1989.
REFERENCES
5. Mahan LK, Arlin MT. Krause Alimento s, Nutrição e Dieto terapia, 8th
ed. São Paulo : Ro ca; 1995.
6. McLean RM. Magnesium and its therapeutic uses: a review. Am J Med 1994;96:63-76.
7. Wo o d s KL, Fle tc he r S. Lo ng - te rm o utc o m e afte r intrave no us magnesium sulfate in suspected acute myo cardial-infarctio n - The Seco nd Leicester Intraveno us Magnesium Interventio n Trial (LIMIT-2). Lancet 1994;343:816-9.
8. Eisenberg MJ. Magnesium deficiency and sudden death (edito rial). Am Heart J 1992;124:544-9.
b een sho wn to b e inadeq uate, causing patients to fa c e m ic ro n u trie n t im b a la n c e a n d s u ffe r its co nse q ue nce s. In spite o f pro b le ms in co rre lating b lo o d m ag n e s iu m le ve ls to th e ir in trac e llu lar amo unts, plasma values co uld help to detect o r at least suggest b o dy magnesium deficiency and the need fo r treatment.
Our pre se nt and sugge ste d m agne sium tre at-m e nt fo r the se p atie nts is: a) whe n se ruat-m le ve ls range fro m 1.2 to 1.5 m Eq /l the y sho uld re ce ive a to tal infusio n o f 66 m Eq /day, 20 m illilite rs o f m ag-ne sium sulfate 20% plus daily allo wance s, dilute d in 100 o r 200 m l saline o r gluco se so lutio n, de pe nd-ing o n the patie nt’s liq uid re strictio ns; b ) patie nts with lo we r m agne sium le ve ls (< 1.2 m Eq /l), sho uld re ce ive an infusio n o f 99 m Eq pe r day plus allo w-ance s, ke e ping the dilutio n as de scrib e d ab o ve .
Infusio n sho uld b e at a lo w rate like 5 m Eq p e r ho ur (sid e e ffe c ts have b e e n re p o rte d whe n m a g n e s i u m s u l fa t e i s i n fu s e d ra p i d l y i . e . p a re s t h e s i a , n a u s e a , vo m i t i n g , m a l a i s e a n d hyp o te nsio n). In o ur unit, we c he c k m agne sium b lo o d le ve ls 24 ho urs afte r re p o sitio n, and a we e k late r if the pro ce dure was e fficie nt. Afte r the patie nt has b e e n stab ilize d , we c o ntinue c he c king it e ve ry 15 d ays d uring ho sp italizatio n and m o nthly, whe n the p atie nt is at ho m e .
172
r e s u m o
CO N TEX TO : Supo rte nutricio nal de mag nésio em pacientes co m ressecção de intestino curto .
O BJETIVO : Analisar a incidência e tratamento de hipo mag nesemia em pacientes co m pequena ressecção extensiva do intestino .
TIPO DE ESTUDO : Estudo retro spectivo .
LO CAL: Unidade Metabó lica Ho spital das Clínicas da Faculdade de Medicina de Ribeirão Preto - Universidade de São Paulo .
PACIEN TES: 1 5 pacientes pó s g rande enterecto mia evo luindo co m Síndro me do Intestino Curto .
VARIÁVEIS ESTUDADAS: Co ntro le sérico de mag nésio de pacientes co m ressecção intestinal. Repo sição de mag nésio quando valo res baixo s fo ram enco ntrado s.
RESULTADO S: Valo res sérico s de mag nésio iniciais [1 ,5 9 mEq/ l (SD 0 , 4 3 )] fo ra m o b tid o s 2 1 a 1 8 0 d ia s a p ó s a c irurg ia . Hipo mag nesemia (mag nésio sérico meno r do que 1 ,5 mEq/ l) fo i detectada em 4 0 % do s pacientes [1 ,1 9 mEq/ l (SD 0 ,2 2 )]. Durante o perío do de seg uimento , 6 6 % do s pacientes apresentaram pelo me no s d o is va lo re s a b a ixo d o s limite s d e re fe rê nc ia . 4 0 % aumentaram seus valo res apó s terapia co m mag nésio .
CO N CLUSÃO : O co ntro le metabó lico do mag nésio sérico deve ser fe ito a p ó s e nte re c to mia e xte nsa . Hip o ma g ne se mia p o d e se r enco ntrada e deve ser co ntro lada.
PALAVRAS-CHAVE: Hipo mag nesemia. Síndro me do Intestino Curto . Intestino . Supo rte N utricio nal.
Simone Chave s Miranda, MD. Divisio n o f Clinical Nutritio n, Department o f Internal Medicine, Ho spital das Clínicas, Faculty o f Medicine o f Ribeirão Preto , University o f São Paulo , Ribeirão Preto , Brazil.
Miche lle Lizzy Bande ira Ribe iro, RD. Divisio n o f Clinical Nutritio n, Department o f Internal Medicine, Ho spital das Clínicas, Faculty o f Medicine o f Ribeirão Preto , University o f São Paulo , Ribeirão Preto , Brazil.
Eduardo Fe rriolli, MD. Divisio n o f Clinical Nutritio n, Department o f Internal Medicine, Ho spital das Clínicas, Faculty o f Medicine o f Ribeirão Preto , University o f São Paulo , Ribeirão Preto , Brazil.
Júlio Sé rgio Marchini, MD. Asso ciate Pro fesso r, Divisio n o f Clinical Nutritio n, Department o f Internal Medicine, Ho spital das Clínicas, Faculty o f Medicine o f Ribeirão Preto , University o f São Paulo , Ribeirão Preto , Brazil.
Source s of funding: No t declared
Conflict of inte re st: No t declared
Last re ce ive d: 06 April 2000
Acce pte d: 20 June 2000
Addre ss for corre sponde nce :
Júlio Sérgio Marchini
Divisão de Nutrição Clínica da Faculdade de Medicina de Ribeirão Preto , Universidade de São Paulo
Avenida Bandeirantes, 3.900
Ribeirão Preto /SP - Brasil - CEP 14049-900 Telefo ne: (16) 602 3375 / 633 0436 Fax: (16) 633 6695
E-mail: jsmarchi@ fmrp.usp.br
p u b lis hin g in fo r m a t io n
Sao Paulo Med J/Rev Paul Med 2000; 118(6):169-72.
9. Lasserre B, Spo erri M, Mo ullet V, Theubet MP. Sho uld magnesium therapy be co nsidered fo r the treatment o f co ro nary heart disease? II. Epidemio lo gical evidence in o utpatients with and witho ut co ro nary heart disease. Magnes Res 1994;7:145-53.
10. Bernardi D, Dini FL, Azzarelli A, Giaco ni A, Vo lterrani C, Lunardi M. Sudden cardiac death rate in an area characterized by high incidence o f c o ro nary arte ry d ise ase and lo w hard ne ss o f d rinking wate r. Angio lo gy 1995;46:145-9.
11. Gartside PS, Glueck CJ. The impo rtant ro le o f mo difiable dietary and behavio ral characteristics in the causatio n and preventio n o f co ro nary heart disease ho spitalizatio n and mo rtality: the pro spective NHANES I fo llo w-up study. J Am Co ll Nutr 1995;14:71-9.
12. Altura BM, Zhang A, Altura BT. Magne sium, hype rte nsive vascular dise ase s, athe ro ge ne sis, sub ce llular co mpartme ntatio n o f Ca2+ and
M g2 + a n d va s c u l a r c o n tra c ti l i ty. M i n e r El e c tro l yte M e ta b