Gender and other factors
associated with the use of hearing
protection devices at work
I Programa de Pós-Graduação em Saúde
Coletiva. Instituto de Saúde Coletiva. Universidade Federal da Bahia. Salvador, BA, Brasil
II Programa Integrado em Saúde Ambiental e
do Trabalhador. Instituto de Saúde Coletiva. Universidade Federal da Bahia. Salvador, BA, Brasil
III Departamento de Fonoaudiologia. Instituto
de Ciências da Saúde. Universidade Federal da Bahia. Salvador, BA, Brasil
Correspondence: Silvia Ferrite
Av. Reitor Miguel Calmon, s/n Vale do Canela 40110-902 Salvador, BA, Brasil
E-mail: [email protected] Received: 7/7/2014 Approved: 1/11/2015
ABSTRACT
OBJECTIVE: To analyze whether sociodemographic, occupational, and health-related data are associated with the use of hearing protection devices at work, according to gender.
METHODS: A cross-sectional study was conducted in 2006, using a random sample of 2,429 workers, aged between 18 and 65 years old, from residential sub-areas in Salvador, BA, Northeastern Brazil. Questionnaires were used to obtain sociodemographic, occupational, and health-related data. Workers who reported that they worked in places where they needed to shout in order to be heard were considered to be exposed to noise. Exposed workers were asked whether they used hearing protection devices, and if so, how frequently. Analyses were conducted according to gender, with estimates made about prevalence of the use of hearing protection devices, prevalence ratios, and
their respective 95% conidence intervals.
RESULTS: Twelve percent (12.3%) of study subjects reported that they were exposed to noise while working. Prevalence of the use of hearing protection devices was 59.3% for men and 21.4% for women. Men from higher socioeconomic levels (PR = 1.47; 95%CI 1.14;1.90) and who had previous audiometric tests (PR = 1.47; 95%CI 1.15;1.88) were more likely to use hearing protection devices. For women, greater perceived safety was associated with the use of protection devices (PR = 2.92; 95%CI 1.34;6.34).
This perception was speciically related to the presence of supervisors
committed to safety (PR = 2.09; 95%CI 1.04;4.21), the existence of clear rules to prevent workplace injuries (PR = 2.81; 95%CI 1.41;5.59), and whether they were informed about workplace safety (PR = 2.42; 95%CI 1.23;4.76).
CONCLUSIONS: There is a gender bias regarding the use of hearing protection devices that is less favorable to women. The use of such devices among women is positively influenced by their perception of a safe workplace, suggesting that gender should be considered as a factor in hearing conservation programs.
DESCRIPTORS: Ear Protective Devices, utilization. Hearing Loss, prevention & control. Occupational Risks. Gender and Health. Cross-Sectional Studies.
Tatiane Costa MeiraI
Vilma Sousa SantanaII
Noise is one of the most common risk factors in
work environments. It is the main modiiable cause
of hearing loss in adults,5 and ranks third among
the occupational hazards that generate the greatest number of years lived with disability.a In 2010, in
the European Union, 29.0% of workers were exposed to noise for at least a quarter of their daily working hours,b while in the United States, between 1999 and
2004, 17.2% were exposed to noise over their entire work shift.18
Protecting workers from exposure to noise has been the target of international recommendations, such as ISO-1999c and speciic country regulations. Such
recommendations consider factors ranging from the
deinition of acceptable noise limits to hearing conser -vation programs, which include the use of hearing protection devices (HPD).d,e
The World Health Organization (WHO) estimates that noise-induced hearing loss (NIHL) leading to irreversible cochlear damage accounts for 19.0% of all years lived with disability related to all work-related diseases and illnesses worldwide.3
NIHL can be prevented through collective measures, such as the modification or replacement of machines and equipment, and the use of acoustical barriers, silencers and enclosure, which are recognized as the best and most effective protection measures.d
When these are not technically feasible, while they are being installed, or used on an emergency basis, individual prevention measures are utilized to reduce the intensity of workers’ exposure to noise.d,f These
procedures reduce the risk of NIHL and other poten-tially adverse effects, such as insomnia, irritability, and increased heart rate and blood pressure.12 In
Brazil, Regulatory Norm NR-6f establishes the
mandatory use of HPD when sound pressure levels INTRODUCTION
exceed those defined by NR-15,d i.e., 85 dB(A) for
eight hours a day, or the equivalent.
Although HPD are mandatory, the prevalence of the use of these devices by workers exposed to noise is low: 42.2% of workers in Brazilg and 65.7% in the United
States.18 HPD use is positively associated with certain
factors, such as increased noise levels in the work-place,16,17 being young,17 being inluenced by peers and
supervisors,9,10 and, particularly, being male, regardless
of occupation.17,18
Women’s participation in the labor market has increased, especially in economic sectors and occu-pations traditionally considered to be predominantly male,h,i which may have resulted in increased
preva-lence and/or intensity of exposure to noise. A study of women’s working and health conditions using data from the European Unionh showed that noise
levels in women’s work environments are either neglected or poorly monitored, and prevention is not usually targeted by training and information. Such neglect arises from factors related to gender bias and because it occurs in non-industrial activities, such as services – particularly education, accommodation, food and beverage, among others.h The WHOj
recom-mended that studies investigate noise exposure and its distinct effects on men and women, since this is rarely addressed in the literature. Studies on HPD use have not considered gender differences when identifying associated factors. The creation of proper hearing conservation programs cannot disregard information regarding the reasons for HPD use and should take gender differences into account.
This study aimed to analyze whether sociodemographic, occupational, and health-related data are associated with the use of hearing protection devices at work, according to gender.
a World Health Organization. Global health risks: mortality and burden of disease attributable to selected major risks. Geneva; 2009
[cited 2014 Jun 18]. Available from: http://www.who.int/healthinfo/global_burden_disease/GlobalHealthRisks_report_ full.pdf
b The European Foundation for the Improvement of Living and Working Conditions. Fifth European Working Conditions Surveys. Luxembourg;
2012 [cited 2015 Apr 30]. Available from: http://www.eurofound.europa.eu/sites/default/files/ef_files/pubdocs/2011/82/en/1/EF1182EN.pdf
c International Organization for Standardization. Determination of occupational noise exposure and estimation of noise-induced
hearing impairment - ISO 1990:1999. 2.ed. Geneva; 1990 [cited 2015 Apr 30]. Available from: http://www.iso.org/iso/catalogue_detail. htm?csnumber=6759
d Ministério do Trabalho e Emprego. Norma Regulamentadora nº 15: atividades e operações insalubres. Brasília (DF); 1978 [cited 2015 Apr
28]. Available from: http://portal.mte.gov.br/data/files/8A7C816A47594D040147D14EAE840951/NR-15%20(atualizada%202014).pdf
e National Institute for Occupational Safety and Health. Criteria for a Recommended Standard: occupational noise exposure: revised criteria
1998. Cincinnati: NIOSH; CDC; 1998 [cited 2014 Jun 18]. Available from: http://www.cdc.gov/niosh/docs/98-126/pdfs/98-126.pdf
f Ministério do Trabalho e Emprego. Norma Regulamentadora Nº 6: Equipamento de Proteção Individual – EPI. Brasília (DF); 1978 [cited 2015
Apr 28]. Available from: http://portal.mte.gov.br/data/files/FF8080814CD7273D014D34C6B18C79C6/NR-06%20(atualizada)%202015.pdf
g Ferrite S. Epidemiologia da perda auditiva em adultos trabalhadores [thesis]. Salvador (BA): Instituto de Saúde Coletiva da Universidade
Federal da Bahia; 2009 [cited 2015 Apr 28]. Available from: https://repositorio.ufba.br/ri/handle/ri/10892
h European Agency for Safety and Health at Work. New risks and trends in the safety and health of women at work. Luxembourg: Publications
Office for the European Union; 2013. DOI:10.2802/69206
i Messing K, Östlin P. Gender equality, work and health: a review of the evidence. Geneva: World Health organization; 2006 [cited 2014 Jun
18] Available from: http://www.who.int/gender/documents/Genderworkhealth.pdf?ua=
jConcha-Barrientos M, Campbell-Lendrum D, Steenland NK. Occupational noise: assessing the burden of disease from work-related hearing
METHODS
This is a cross-sectional study based on data from a survey on working and health conditions, which used a sample of Salvador, BA, Northeastern Brazil, residents. The city has 2,675,656 residents (2010 census), making it the third most populated in the country. In 2010, it had a Human Development Index (HDI) of 0.759.k
The original study is a population-based prospective cohort study, which began in 2000, with visits repeated every two years until 2008. The data analyzed came from the fourth phase of the study, which was conducted in 2006, when data on hearing health and noise expo-sure were obtained. Cluster sampling was conducted in a single stage, with the selection of sub-areas, out of
which each family was identiied and recruited for the research. Trained ield workers used individual ques -tionnaires for interviews during home visits, in order to collect data related to sociodemography, lifestyle, working conditions, and health.
The study population comprises all subjects aged between 18 and 65 years old, who reported having a paid job and being exposed to noise in the work-place – 299 people in total. Noise exposure was defined by positive responses to two questions: “Have you ever worked in a very noisy environ-ment, where you had to shout so that a colleague one meter away could hear you?”, which suggests noise exceeding 85 dB(A);14 and “Over the last 12
months, have you worked in an environment with that level of noise?”.
The outcome variable was the use of hearing protec-tion devices when exposed to workplace noise (yes: regular or frequent use; no: seldom or never). The predictor variables were: 1) sociodemographic: age, ethnicity, marital status, education level, socioeco-nomic level (based on family assets: low - zero to two items; medium or high - three to nine items); occupational: occupational exposure to noise (in years), average hours of exposure per day, employ-ment relationship (formal, when registered in the worker’s Employment Registration Book, or informal, when not), and perceived workplace safety; 3) hearing-related: self-reported hearing loss; tinnitus; previous audiometric tests; and 4) Self-reported health
status, which was deined through a response to the
question, “Between 0 and 10, what score would you give your health?” (score < 8 = poor, fair, or good; score ≥ 8 = great or excellent).
Regarding perceived workplace safety, responses to the following six questions were analyzed both
separately and together: 1) “Are the health and safety of workers sufficiently protected in your workplace?”; 2) “Do your supervisors or bosses encourage you to protect yourself and prevent injuries?”; 3) “Do company owners spend money (invest) to make your workplace safe?”; 4) “Are clear rules established about what you should do to prevent workplace injuries?”; 5) “Is safety more important than production in the company where you work?”; 6) “Are you provided with informa-tion on workplace safety?” (adapted from the form used by Garcia et al,7 2004). Answers “never”,
“seldom”, and “sometimes” were taken as “no”, and “frequently” and “always”, as “yes”. The composite variable regarding perceived workplace safety corre-sponded to the total sum of scores, counting one point for each “yes” response and zero for each “no”, where each answer had the same weight. Categories for analysis were based on tertiles: 0 = poor; 1 to 4 = good; and 5 to 6 = very good.
Overall and specific prevalence of HPD use were estimated according to variable categories. Analyses were carried out separately by gender. The association measure was prevalence ratio (PR), to which 95%
conidence intervals based on the Mantel-Haenszel
method were used for statistical inference. Analyses were performed using SAS 9.2 statistical software.
The research was approved by the Ethics in Research Committee of the Hospital das Clínicas at the Universidade Federal daBahia (Protocol 49, June 1st,
2000). All subjects signed informed consent forms.
RESULTS
The study comprised 299 workers exposed to workplace noise out of the total cohort subjects (n = 2,429). Study subjects were more commonly young (76.6%), black (65.4%), in formal jobs (61.4%), male (60.9%) adults with at least high school education (67.6%). The majority had been exposed to occupational noise for
at least ive years (60.2%), eight hours a day or less
(78.9%). Women exposed to occupational noise were less likely to be black (p = 0.0029), had more schooling (p = 0.0004), and were less likely to report previous audiometric tests (p < 0.0001). Men and women perceived workplace safety differently: 45.4% of the women considered their workplace safety to be “poor”, whereas only 20.5% men (p < 0.0001) expressed this opinion. There were no gender differences for the remaining variables.
Prevalence for use of HPD by workers exposed to noise was 44.5% (95%CI 38.9;50.1). Patterns of HPD use differed between genders; 59.3% of men
k Instituto Brasileiro de Geografia e Estatística. Cidades. Brasília (DF); 2014 [cited 2014 Jun 18]. Available from: http://www.cidades.ibge.gov.
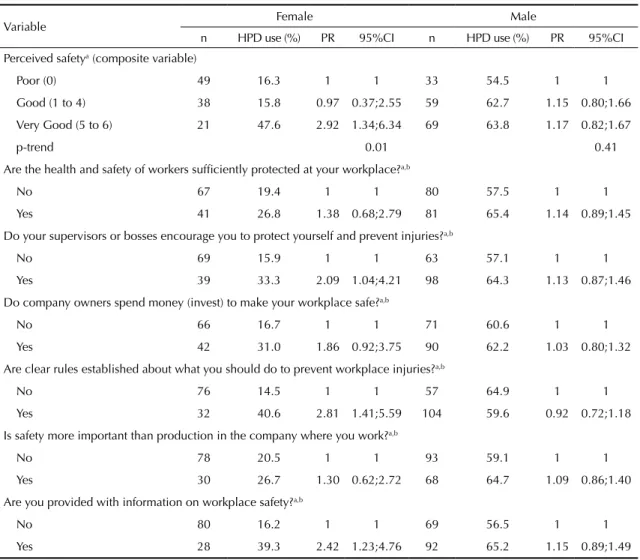
and 21.4% of women reported HPD use (PR = 2.78; 95%CI 1.92;4.01). Regarding sociodemographic factors (Table 1), HPD use was associated with medium/high socioeconomic levels (compared to low) and with having had previous audiometric tests (compared to no tests) for men (Table 2). For women who perceived workplace safety as “very good” the prevalence of HPD use was three times greater than for those who reported working under “poor” safety
conditions (Table 3). The inluence of supervisors in
preventing workplace injuries, the existence of clear rules to prevent them, and being informed about workplace safety were positively associated with HPD use in women.
DISCUSSION
Less than half of the workers exposed to noise used HPD; this was almost three times more common among men than women. The perceived degree of safety was associated with HPD use among women, with greater use related to greater perception of an unsafe work envi-ronment. Use of HPD was more likely to be reported by women who mentioned that they had committed supervisors, clearly stated safety rules, and access to
safety information. Among men, medium or high socio-economic levels and previous audiometric tests were associated factors.
Our estimated prevalence of HPD use is close to the finding of 41.4% from a study in the United States, based on data from 1981 to 1983, by the National Institute for Occupational Safety and Health (NIOSH).4 From 1999 to 2004, results from the
National Health and Nutrition Examination Survey (NHANES) showed a prevalence of 65.7%.18 Despite
evidence of a positive trend in the use of hearing protection in the United States, these results still indi-cate that one out of three workers exposed to noise did not use HPD.
Less HPD use by women – even when exposed to workplace noise – demonstrates that they are less protected, and more vulnerable, with increased risk of NIHL, compared with men. This gender
bias merits attention. This inding conirms results
from European studies, which found negligence in monitoring and prevention that demonstrated the invisibility of occupational noise exposure among women. Women have taken up jobs in industries that,
Table 1. Prevalence (%) and prevalence ratio (PR) for the association between sociodemographic variables and use of hearing protection devices (HPD) in a population of workers exposed to workplace noise. Salvador, BA, Northeastern Brazil, 2006. (N = 299)
Variable Female Male
n HPD use (%) PR 95%CI n HPD use (%) PR 95%CI
Total 117 21.4 1 13.9;28.8 182 59.3 1 52.2;66.5
Age (years)
18 to 28 29 20.7 1.50 0.47;4.76 59 61.0 1.09 0.78;1.53
29 to 46 59 25.4 1.84 0.67;5.06 82 59.8 1.07 0.77;1.47
> 46 29 13.8 1 1 41 56.1 1 1
Ethnicitya
Black/Mixed race 64 21.9 1 1 129 59.7 1 1
Non-black 52 21.1 0.97 0.48;1.95 50 56.0 0.94 0.71;1.25
Marital status
Single 61 23.0 1 1 82 54.9 1 1
Married/Cohabiting 56 19.6 0.86 0.42;1.73 100 63.0 1.15 0.90;1.47 Education level
Completed elementary school or less 24 12.5 1 1 73 58.9 1 1 Completed high school or above 93 23.7 1.89 0.62;5.80 109 59.6 1.01 0.79;1.29 Socioeconomic levelb
Low 49 26.5 1 1 85 48.2 1 1
Medium/High 63 17.5 0.66 0.32;1.34 90 71.1 1.47 1.14;1.90
Type of employment relationshipc
Informal 52 15.4 1 1 63 55.6 1 1
Formal 65 26.2 1.70 0.80;3.62 118 61.9 1.11 0.86;1.45
although less obviously linked to NIHL risk factors, have been found to have high noise levels.h This
has been observed in countries with more advanced health regulations concerning labor-related health: in the United States, HPD use among women exposed to noise was 50.7%, compared with 68.9% among men.18 The more frequent use of hearing protection
by men may be related to the job tasks and industries most frequently performed by men, in which high noise exposure levels are common, such as mining, construction, and manufacturing.3 Future analyses
must consider speciic occupations and industries,
since these are important factors in noise exposure. This was not possible here, due to a small study sample composed of a general worker population.
In our study, factors associated with HPD use differed according to gender. Higher socioeconomic levels and having previous audiometric tests seem to favor the use of individual protection among men; among women, however, correlated factors were how their workplace was organized, namely their perception that it had a safety climate. Work in Brazil’s manufac-turing industry is relatively well paid, and is known to have high levels of exposure to loud noises.2 This
association may arise from a more hazardous work
environment for NIHL, a more extensive adoption of protection measures, closer supervision of HPD use or compliance with legal regulations to protect workers’ health.
Previous audiometric testing seems to favor the use of HPD among men, which may also indicate better compliance to regulations, given presumably greater workplace noise. In Brazil, audiometric tests are manda-tory for workers exposed to noise levels that exceed the legally permitted limits. Workers are also required to join hearing conservation programs.l However,
Lusk et al11 and Kim et al10 did not ind that HPD use
was associated with previous audiometric tests in the United States and South Korea, respectively.
The association between the positive aspects of perceived workplace safety and HPD use among
women corroborates the indings of Edelson et al6 for
workers of both genders. Women are more inclined towards sociability, which also applies to their
workplaces, and are more inluenced by recommen -dations to protect their health. Further, they are more likely to report health problems and more committed to healthy behavior, such as checkups, treatment compliance and other recommendations that promote Table 2. Prevalence (%) and prevalence ratio (PR) for the association between study variables and use of hearing protection devices (HPD) in a population of workers exposed to workplace noise. Salvador, BA, Northeastern Brazil, 2006. (N = 299)
Variable Female Male
n HPD use (%) PR 95%CI n HPD use (%) PR 95%CI Length of occupational exposure to noise
< 5 years 48 27.1 1 1 71 59.2 1 1
≥ 5 years 69 17.4 0.64 0.32;1.28 111 59.5 1.00 0.79;1.29
Average hours of exposure per day
≤ 8 hours/day 92 19.6 1 1 144 60.4 1 1
> 8 hours/day 25 28.0 1.43 0.67;3.04 38 55.3 0.91 0.67;1.25 Self-reported hearing loss
No 78 21.8 1 1 137 61.3 1 1
Yes 39 20.5 0.94 0.45;1.99 45 53.3 0.87 0.64;1.18
Tinnitus
No 103 21.4 1 1 168 58.9 1 1
Yes 14 21.4 1.00 0.34;2.92 14 64.3 1.09 0.72;1.64
Previous audiometric tests
No 90 17.8 1 1 95 48.4 1 1
Yes 27 33.3 1.88 0.94;3.75 87 71.3 1.47 1.15;1.88
Self-reported health status (scale of 0 to 10)
Poor/Fair/Good (0 to 7) 33 12.1 1 1 36 44.4 1 1
Great/Excellent (≥ 8) 84 25.0 2.06 0.77;5.55 146 63.0 1.42 0.96;2.09
l Ministério do Trabalho e Emprego, Secretaria de Saúde e Segurança no Trabalho. Portaria nº 19 de 9 de abril de 1998. Diretrizes e
their health.13 This may arise from behavioral and
cultural patterns, as well as from awareness and commitment to their role as caregiver, particularly of children.8 It may also be a result of speciic charac
-teristics related to jobs and industries where women are usually engaged, which may have affected our
indings. However, the small numbers in this study
did not allow for further analysis.
The differences between men and women must be understood from a gender perspective. Women are affected by discrimination at work, earn lower wages than men (even when occupying similar jobs), face obstacles which limit their prospects of promotion, are less likely to be union members, and have less visibility and political capital in decision-making.i Women are
gradually achieving jobs in traditionally male areas, and have thus become increasingly involved in new
Table 3. Prevalence (%) and prevalence ratio (PR) for the association between variables regarding perceived safety and use of hearing protection devices (HPD) in a population of workers exposed to workplace noise. Salvador, BA, Northeastern Brazil, 2006. (N = 299)
Variable Female Male
n HPD use (%) PR 95%CI n HPD use (%) PR 95%CI Perceived safetya (composite variable)
Poor (0) 49 16.3 1 1 33 54.5 1 1
Good (1 to 4) 38 15.8 0.97 0.37;2.55 59 62.7 1.15 0.80;1.66 Very Good (5 to 6) 21 47.6 2.92 1.34;6.34 69 63.8 1.17 0.82;1.67
p-trend 0.01 0.41
Are the health and safety of workers sufficiently protected at your workplace?a,b
No 67 19.4 1 1 80 57.5 1 1
Yes 41 26.8 1.38 0.68;2.79 81 65.4 1.14 0.89;1.45
Do your supervisors or bosses encourage you to protect yourself and prevent injuries?a,b
No 69 15.9 1 1 63 57.1 1 1
Yes 39 33.3 2.09 1.04;4.21 98 64.3 1.13 0.87;1.46
Do company owners spend money (invest) to make your workplace safe?a,b
No 66 16.7 1 1 71 60.6 1 1
Yes 42 31.0 1.86 0.92;3.75 90 62.2 1.03 0.80;1.32
Are clear rules established about what you should do to prevent workplace injuries?a,b
No 76 14.5 1 1 57 64.9 1 1
Yes 32 40.6 2.81 1.41;5.59 104 59.6 0.92 0.72;1.18
Is safety more important than production in the company where you work?a,b
No 78 20.5 1 1 93 59.1 1 1
Yes 30 26.7 1.30 0.62;2.72 68 64.7 1.09 0.86;1.40
Are you provided with information on workplace safety?a,b
No 80 16.2 1 1 69 56.5 1 1
Yes 28 39.3 2.42 1.23;4.76 92 65.2 1.15 0.89;1.49
a No data for thirty subjects.
b No = never, seldom, sometimes; Yes = frequently, always.
production spaces.i However, exposure to workplace
hazards and preventive programs tend to be framed and analyzed from a male perspective. Hazards and their control are therefore frequently neglected or forgotten when they affect women.h A European Union review
of women’s working conditionsh demonstrated noise
exposure in job posts not traditionally recognized as “hazardous” for men, such as education, health care and hospitality. It was also noted that women usually receive less training and fewer recommendations regarding HPD use than men.
Although age,11,16,17 education,9 and self-reported
hearing loss16 have been found in association with HPD
As a tool for occupational noise control, the use of HPD is limited and not very effective, compared with collective interventions, which work independently of individual discretion or access to equipment for worker protection, and do not cause the discomfort or annoyance associated with anatomical or ergo-nomic adjustment difficulties. More appropriate recommendations are the control of noise emissions at their principal sources and of noise propagation in the workplace, and the implementation of actions to reduce worker exposure.15 However, such initiatives
are not always feasible, causing the widespread use of HPD, given their low cost, reasonable effectiveness, and easy access.10
This research presents limitations related to statis-tical power, because of its small sample size. This is aggravated by a need to take into account gender,
although it did enable the identiication of distinct
occupational factors between men and women. Given the few observations, it was not possible to include multinomial variables in the analysis, such as jobs or industries, nor to perform a more in-depth treatment
of potential confounding variables or effect modiiers.
Furthermore, our data comes from a study carried out with a different aim, thus reducing the scope of the available descriptor variables and other impor-tant causal factors, such as exposure intensity level. The HPD use did not take into account duration, or
quality of adjustment, comfort, and level of protec-tion. The advantages of this study include its relevance for prevention and its originality, because it did not merely describe the occurrence of clinical diagnoses in populations. Rather it focused on popularity, access, and compliance to a protection recommended against one of the most common labor-related illnesses,
NIHL, which is responsible for a signiicant number
of sensory disability cases worldwide. Since HPD use is mandatory for workers exposed to noise, the results of this study also demonstrate the extent of regula-tory compliance. Organizational factors regarding risk management in work environments, such as the perceived safety investigated in this study, have not
been suficiently explored.
There is gender bias regarding protection against exposure to noise, namely in HPD use, which is less favorable to women than men. Gender, therefore, must be considered in hearing conservation programs. Although perceived safety and some of its components have only been associated with use of HPD among women, interventions based on these results may also contribute to the more frequent use of hearing protection devices by men, once such interventions are adjusted for male characteristics. Contributions can therefore be made to prevent the onset or worsening of NIHL, while better conditions for workers’ hearing health can be promoted.
1. Alli BO. Fundamental principles of occupational health and satefy. 2.ed. Geneva: ILO; 2008.
2. Cavalcante F, Ferrite S, Meira TC. Exposição ao ruído na indústria de transformação no Brasil. Rev CEFAC. 2013;15(5):1364-70. DOI:10.1590/S1516-18462013005000021
3. Concha-Barrientos M, Nelson DI, Driscoll T, Steenland NK, Punnett L, Fingerhut M, et al. Selected occupational risk factors. In: Ezzati M, Lopez AD, Rodgers A, Murray CJL, editors. Comparative quantification of health risks: global and regional burden of disease attributable to selected major risk factors. Geneva: World Health Organization; 2004. p.1651-801.
4. Davis RR, Sieber WK. Hearing protector use in noise-exposed workers: a retrospective look at 1983. AIHA J. 2002;63(2):199-204. DOI:10.1080/15428110208984705
5. Dobie RA. The burdens of age-related and occupational noise-induced hearing loss in the United States. Ear Hear. 2008;29(4):565-77. DOI:10.1097/AUD.0b013e 31817349ec
6. Edelson J, Neitzel R, Meischke H, Daniell W, Sheppard L, Stover B, et al. Predictors of hearing protection use in construction workers. Ann Occup Hyg. 2009;53(6):605-15. DOI:10.1093/annhyg/mep039
7. Garcia AM, Boix P, Canosa C. Why do workers behave unsafely at work? Determinants of safe work practices in industrial workers. Occup Environ Med. 2004;61(3):239-46. DOI:10.1136/oem.2002.005629 8. Gustafson PE. Gender differences in risk
perception: theoretical and methodological perspectives. Risk Anal. 1998;18(6):805-11. DOI:10.1111/j.1539-6924.1998.tb01123.x
9. Kerr MJ, Lusk SL, Ronis DL. Explaining Mexican American workers’ hearing protection use with the health promotion model. Nurs Res. 2002;51(2):100-9. DOI:10.1097/00006199-200203000-00006
10. Kim Y, Jeong I, Hong O. Predictors of hearing protection behavior among power plant workers. Asian Nurs Res. 2010;4(1):10-8. DOI:10.1016/S1976-1317(10)60002-3
11. Lusk SL, Hong OS, Ronis DL, Eakin BL, Kerr M, Early MR. Effectiveness of an intervention to increase construction workers’ use of hearing protection. Hum Factors. 1999;41(3):487-94. DOI:10.1518/001872099779610969
12. Lusk SL, Hagerty BM, Gillespie B, Caruso CC. Chronic effects of workplace noise on blood pressure and heart rate. Arch Environ Health. 2002;57(4):273-81. DOI:10.1080/00039890209601410
13. Machin R, Couto MT, Silva GSN, Schraiber LB, Gomes R, Figueiredo WS, et al. Concepções de gênero, masculinidade e cuidados em saúde: estudo com profissionais de saúde da atenção primária. Cienc Saude Coletiva. 2011;16(11):4503-12. DOI:10.1590/S1413-81232011001200023
14. Neitzel R, Daniell W, Sheppard L, Davies H, Seixas N. Comparison of perceived and quantitative measures of occupational noise exposure. Ann Occup Hyg. 2008;53(1):41-54. DOI:10.1093/annhyg/men071 15. Nelson DI, Nelson RY, Concha-Barrientos M, Fingerhut
M. The global burden of occupational noise-induced hearing loss. Am J Ind Med. 2005;48(6):446-58. DOI:10.1002/ajim.20223
16. Raymond DM, Hong O, Lusk SL, Ronis DL. Predictors of hearing protection use for Hispanic and non-Hispanic White factory workers. Res Theory Nurs Pract. 2006;20(2):127-40. DOI:10.1891/rtnp.20.2.127
17. Sbihi H, Teschke K, MacNab YC, Davies HW. Determinants of use of hearing protection devices in Canadian lumber mill workers. Ann Occup Hyg. 2010;54(3):319-28. DOI:10.1093/annhyg/mep043 18. Tak S, Davis RR, Calvert GM. Exposure to
hazardous workplace noise and use of hearing protection devices among US workers - NHANES, 1999–2004. Am J Ind Med. 2009;52(5):358-71. DOI:10.1002/ajim.20690
Research supported by the Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq – Research Production Grant – Process 304108/2011-1 and Research Grant – Process 487341/2012-0), by the Programa de Apoio a Projetos Institucionais com a Participação de Recém-Doutores (PRODOC – Project 3038/2011), and the Fundação de Amparo à Pesquisa do Estado da Bahia (FAPESB – Undergraduate Research Grant – Process 4973/2011).
Based on master dissertation of Tatiane Costa Meira, titled: “Gênero e fatores associados ao uso de equipamento de proteção auditiva no trabalho”, presented to the Graduate Program in Collective Health at the Universidade Federal da Bahia, in 2015. A partial version of this study was presented at the 21st Speech-Language-Hearing Sciences Congress, in Porto de Galinhas, PE, on September 24, 2013.