BrazJOtorhinolaryngol.2016;82(2):223---231
www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
REVIEW
ARTICLE
Systematic
review:
the
influence
of
nasal
obstruction
on
sleep
apnea
夽
Debora
Petrungaro
Migueis
a,
Luiz
Claudio
Santos
Thuler
a,b,
Lucas
Neves
de
Andrade
Lemes
c,
Chirlene
Santos
Souza
Moreira
a,
Lucia
Joffily
d,
Maria
Helena
de
Araujo-Melo
a,d,∗aPostgraduatePrograminNeurology,UniversidadeFederaldoEstadodoRiodeJaneiro(UNIRIO),RiodeJaneiro,RJ,Brazil bClinicalInvestigationDivision,InstitutoNacionaldeCâncer(INCA),RiodeJaneiro,RJ,Brazil
cUniversidadedoEstadodoRiodeJaneiro(UERJ),RiodeJaneiro,RJ,Brazil
dUniversidadeFederaldoEstadodoRiodeJaneiro(UNIRIO),RiodeJaneiro,RJ,Brazil
Received8May2015;accepted18May2015
Availableonline7January2016
KEYWORDS
Nasalobstruction; Obstructivesleep apnea;
Sleepfragmentation; Polysomnography; Treatmentoutcome
Abstract
Introduction:Obstructivesleepapneasyndrome(OSAS)isacommondisorderthatcanleadto cardiovascularmorbidityandmortality,aswellastometabolic,neurological,andbehavioral consequences.Itiscurrentlybelievedthatnasalobstructioncompromisesthequalityofsleep whenitresultsinbreathingdisordersandfragmentationofsleep.However,recentstudieshave failedtoobjectivelyassociatesleepqualityandnasalobstruction.
Objective: Theaimofthissystematicreviewistoevaluatetheinfluenceofnasalobstruction onOSASandpolysomnographicindicesassociatedwithrespiratoryevents.
Methods:Elevenoriginalarticlespublishedfrom2003to2013wereselected,whichaddressed surgicalandnon-surgicaltreatmentfornasalobstruction,performingpolysomnographytype1 beforeandaftertheintervention.
Results/conclusions: Inmosttrials,nasalobstructionwasnotrelatedtotheapnea---hypopnea index(AHI),indicatingnoimprovementinOSASwithreductioninnasalresistance.However, fewresearchersevaluatedotherpolysomnographyindices,suchasthearousalindexandrapid eye movement(REM)sleeppercentage.These couldchangewithnasalobstruction, sinceit ispossiblethatthenasal obstructiondoesnotcompletely blocktheupperairways,butcan increasenegativeintrathoracicpressure,leadingtosleepfragmentation.
© 2015 Associac¸ão Brasileira de Otorrinolaringologia e Cirurgia Cérvico-Facial. Published by Elsevier Editora Ltda. This is an open access article under the CC BY license (https://creativecommons.org/licenses/by/4.0/).
夽 Pleasecitethisarticleas:MigueisDP,ThulerLCS,deAndradeLemesLN,MoreiraCSS,JoffilyL,deAraujo-MeloMH.Systematicreview: theinfluenceofnasalobstructiononsleepapnea.BrazJOtorhinolaryngol.2016;82:223---31.
∗Correspondingauthor.
E-mails:[email protected],[email protected](M.H.deAraujo-Melo). http://dx.doi.org/10.1016/j.bjorl.2015.05.018
PALAVRAS-CHAVE
Obstruc¸ãonasal; Apneiaobstrutivado sono;
Fragmentac¸ãodo sono;
Polissonografia; Resultadodo tratamento
Revisãosistemática:influênciadaobstruc¸ãonasalnaapneiadosono
Resumo
Introduc¸ão:Asíndromedaapneiaobstrutivadosono(SAOS)éumdistúrbiomuitoprevalente que pode ocasionarmorbi-mortalidade cardiovascular, alémde consequências metabólicas, neurológicasecomportamentais.Atualmente,acredita-sequeaobstruc¸ãonasalcomprometa aqualidadedosono,devidoadistúrbiosrespiratóriosefragmentac¸ãodosono.Entretanto,até omomentoestudos recentesnão conseguemrelacionarobjetivamente qualidadedosonoe obstruc¸ãonasal.
Objetivo:Oobjetivo principaldesta revisão sistemáticaéavaliarainfluênciadaobstruc¸ão nasalnaSAOSeemíndicespolissonográficosassociadosaeventosrespiratórios.
Método: Foramselecionadosumtotalde11artigosoriginaisde2003a2013comtratamentos cirúrgicosenão cirúrgicosdaobstruc¸ãonasal,realizandoapolissonografiadotipo1antese apósaintervenc¸ão.
Resultados/conclusões: Namaioriadosensaios,aobstruc¸ãonasalnãoserelacionouaoíndice deapneia-hipopneia,indicando ausênciademelhoradaSAOS comareduc¸ão daresistência nasal.Entretanto,poucospesquisadoresavaliaramíndicespolissonográficoscomooíndicede despertareseopercentualdosonoREM(movimentorápidodosolhos)quepoderiamvir alter-ados,uma vezqueaobstruc¸ãonasal possivelmentenãoobstruicompletamente aviaaérea superior,masaumentaapressãonegativaintratorácica,levandoàfragmentac¸ãodosono. © 2015 Associac¸ão Brasileira de Otorrinolaringologia e Cirurgia Cérvico-Facial. Publi-cado por Elsevier Editora Ltda. Este é um artigo Open Access sob a licença CC BY (https://creativecommons.org/licenses/by/4.0/deed.pt).
Introduction
Obstructivesleepapneasyndrome(OSAS)isaveryprevalent
disorder,whichmayresultincardiovascularmorbidityand
mortality,aswellasmetabolic,neurological,andbehavioral
consequences.IntheBrazilianpopulation,thissyndromeis
apublichealthproblem,affecting32.8%ofthepopulation.1
OSASisananatomicalandfunctionalabnormalityresulting
frompartialor totalneuromuscular collapseof theupper
airways(UA)during sleep,mainlywithnegativepressures
duringinspiration.Thisobstructioncausessleep
fragmenta-tionandintermittenthypoxia.Themainareasofobstruction
arethenose,palate,andtongue,buttheobstructionmaybe
multifactorial.2Currently,itisbelievedthatnasal
obstruc-tionimpairsthequalityofsleepinrespiratorydisorders,and
alsoadverselyaffectstheadoptionandadherenceto
con-tinuouspositiveairwaypressure(CPAP),thegold standard
for OSAStreatment.3 However,recent studies have failed
to objectively associate the quality of sleep with nasal
obstruction.4
According to the European Position Paper on
Rhinos-inusitis and Nasal Polyps (EPOS 2012), nasal obstruction
canbe caused by several typesof chronic (CRS) or acute
rhinosinusitis.5 Somestudiessuggest thatsleepcomplaints
inpatientswithCRSarecommonandcanevenaffecttheir
quality of life, but there is little information about this
association.6Thelastreviewonthesubject,carriedoutin
2013by Meenetal., showedthat drugand surgicalnasal
interventionsdid not improve the apnea---hypopnea index
(AHI), or OSAS,but improved subjective symptomsof the
disorder,suchasexcessivedaytimesleepinessandqualityof
life.4Thisandothermorerecentsystematicreviews,
how-ever,didnotevaluatethearousalindex,RERA(respiratory
effort-relatedarousals),andthesleep-disorderedbreathing
index.
The main objective of this systematic review was to
evaluate the influence of nasal obstruction on OSAS and
other polysomnographyindicesassociatedwithrespiratory
events,overthelastdecade.
Methods
Articles selected were prospective studies, consisting of
controlled clinical trials, and cohort studies, in which
patients underwent type 1 polysomnography (supervised
by the technician in the sleep laboratory), performed as
a complete overnightstudy beforeandafter conservative
orsurgicalinterventionstoimprovenasalbreathingduring
sleep.Tworeviewersselectedtherelevantliterature
pub-lished between2003 and2013 fromMEDLINE(BIREME and
PubMed),inEnglishorPortugueselanguages,onthe
associ-ationbetweennasalobstructionandOSAS.Relatedarticles
andreferenceswerealsoincludedinthisreview.Only
origi-nalstudieswithsurgicalandnon-surgicaltreatmentofnasal
obstructionthatperformedtype1polysomnographybefore
and after the intervention were selected. The following
wereexcluded:letterstotheEditor,caseseries(with less
thantenpatients),review articles,basicresearchstudies,
andstudieswithoutinterventionorwithouttype1
polyso-mnographyperformedthroughouttheentirenight.Studies
thatincludedpatientswithneuropathy,heartdisease,age
<18years,andmultilevelsurgeryorothernon-nasal
surger-iesatthesametimewerealsoexcluded.
The assessed interventions were: use of medications
(nasaldecongestantsandtopicalcorticosteroids),nasal
Systematicreview:theinfluenceofnasalobstructiononsleepapnea 225
withoutturbinectomy,functionalendoscopicsinussurgery).
Inthissystematicreview,treatmentsuccesswasevaluated
according tosubjective improvementin nasal obstruction
and/orimprovementinnasalresistance.Additionally,
poly-somnographyindicesrelatedtorespiratoryeventsandpre
andpost-interventionEEGindiceswerecomparedtoassess
theinfluenceofnasalobstructiononOSAS.
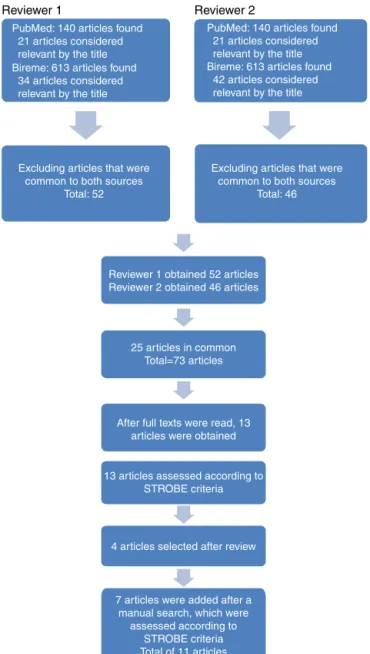
The search in PubMed wascarried out in August 2014
using the terms ‘‘Nasal Obstruction’’ [MeSH] AND ‘‘Sleep
Apnea, Obstructive’’ [MeSH], resultingin 140 articles. In
theVirtualHealthLibrary,usingtheterms ‘‘nasal
obstruc-tionand Obstructive SleepApnea’’, the authors obtained
613articles.Afterareviewoftitlesandabstracts,thefirst
reviewer obtained 21 articles from PubMed and 33 from
BIREME.Afterexcludingarticlesthatwererepeatedinboth
sources,52studiesremained.Afterreviewingthetitlesand
abstracts, the second reviewer selected 21 articles from
PubMedand42fromBIREME.Aftereliminatingtherepeated
articles,46remained.
Amongthearticlesselectedbybothreviewers,25were
repeated,andafterassessingboththetitlesandabstracts,
73articlesremainedtobereadinfullandfinallyselected.In
additiontothese,otherarticleswerealsoincludedthrough
manualsearchoftheevaluatedreferences(Fig.1).
Thelevelofsignificancewassetat5%(˛=0.05)toreject
thenullhypothesis.Thevaluesareshownwiththe
respec-tive95%confidenceintervals(95%CI),whichexpresseswith
95%certaintytherangeofvalueswithinwhichthetruevalue
isfoundinthepopulation.7Medianageandbodymassindex
(BMI)werecalculatedasacentraltendencymeasure.
Addi-tionally, all selected articles met the criteria established
byStrengtheningtheReportingofObservationalStudiesin
Epidemiology(STROBE)appliedtocohortstudies.8
Results
Afterselectingthefullarticlesandevaluatingthe
methodol-ogy,p-value,confidenceinterval,absenceofbias,andthe
presence of allcriteriaestablished by theSTROBE
check-list,11 articleswere selected for this systematic review.
Patientswithnasalobstructionunderwentclinicaland
sur-gical interventionstoimprovenasal breathing,comparing
pre-andpostoperativepolysomnographyindices.Excessive
daytimesleepinesswasassessedbytheEpworthSleepiness
Scale(ESS)9andclinicalimprovement.
The followingpolysomnographic parameterswere
eval-uated: AHI, sleep-disordered breathing index (SDBI),
presenceofdesaturationandsnoring,arousal index,sleep
architecture,REM(rapid eye movement) sleep,and
slow-wave sleep (previously known as N3+N4 sleep stage)
accordingtothecriteriaoftheAmericanAcademyofSleep
Medicine(AAMS)Manual.10
A totalof 297patients wereevaluated, withamedian
ageof46yearsandameanBMIof27.9kg/m2.
Of the three trials with drug treatment (Table 1), all
patients obtained a reduction in nasal resistance and
improved subjective sleep quality, without changing the
snoring. After conservative treatment, the AHI and the
desaturation index only showed a significant reductionin
study by Kielyet al.11 Two trialsusing decongestants12,13
demonstrated no improvement in excessive daytime
Reviewer 1 Reviewer 2
PubMed: 140 articles found 21 articles considered relevant by the title Bireme: 613 articles found 34 articles considered relevant by the title
Excluding articles that were common to both sources
Total: 52
Excluding articles that were common to both sources
Total: 46 PubMed: 140 articles found 21 articles considered relevant by the title Bireme: 613 articles found 42 articles considered relevant by the title
Reviewer 1 obtained 52 articles Reviewer 2 obtained 46 articles
25 articles in common Total=73 articles
After full texts were read, 13 articles were obtained
13 articles assessed according to STROBE criteria
4 articles selected after review
7 articles were added after a manual search, which were
assessed according to STROBE criteria Total of 11 articles
Figure 1 Literature review process. The articles were
obtainedbyusing thekeywordsinBIREMEandPubMed.Each
reviewerinitiallyassessed753articles.Afterexclusionof
arti-cles repeated between sources, titles, and abstracts were
evaluated together, which resulted in 73 articles that were
assessed in full. There were 25 articles in common and 13
wereevaluatedaccordingtotheSTROBE criteria.Inaddition
tothese,sevenarticleswereincludedthroughmanualsearch
oftheanalyzedreferences.
sleepinessaccordingtotheEpworthSleepinessScale(ESS).
In two studies with clinical interventions,11,12 there was
a significant increase in slow-wave sleep, and only Lean
etal.12foundalowerarousalindex,highersleepefficiency,
andincreasedpercentageofREMsleepandslow-wavesleep
(Table2).
Among the eight studies withsurgical intervention14---21
(Table 1),allachievedsignificant reductionin nasal
resis-tance.Only one trial with surgical intervention15 did not
achieve significant change in the ESS, while the others
showeda reductionin excessivedaytimesleepiness.
Migueis
DP
et
al.
Table1 Totalnumberofstudieswithclinicalandsurgicalintervention. Authorsandyear
ofpublication
Follow-up period
Studydesign Patients(n) Males(%) Meanage MeanBMI Nasalintervention AMMSmanual
Kielyetal.112004 2months Clinicaltrial 23 82.6 46 27.9 Fluticasonespray100mcg2×/dayfora
monthandplaceboforamonth.Crossover
design.
1999
Leanetal.122005 2PSGwitha
one-day interval
betweenthem
Clinicaltrial 10 90 46.5 27 Nasaldecongestant1hbeforelights-out
andnasaldilator.Crossoverdesign.
1999
Clarenbach
etal.132008
3weeks Clinicaltrial 12 83.3 49.1 30.7 PatientswithEDS,OSAS,andnasal
complaintsintworandomizedgroups:one
withtopicalxylometazolineandanother
withplaceboforsevendays.Crossover
design.
1992
Nakataetal.14
2005
PSGpreand
post-op
Clinicaltrial 12 100 54.2 27 Inferiorturbinectomyandseptoplasty.
Sinusotomyinonepatient.CPAPuse
pre-andpostoperatively.
1999
Virkkulaetal.15
2006
2---6months Prospective
study
40 100 44.2 27.9 Septoplastywith(2)orwithoutpartial
inferiorturbinectomyandrhinoseptoplasty
(twopatients).
1999
Koutsourelakis
etal.162008
PSGpreand
post-op
Clinicaltrial 49 75.5 38.3 30.15 27septoplastieswith(18)orwithoutpartial
inferiorturbinectomy,22shamsurgeries.
1999
Lietal.172008 3months Clinicaltrial 51 98 39 26 Septoplastyandsinusectomy. 1999
Tosunetal.182009 3months Clinicaltrial 27 81.5 40.37 23.87 FESSinpatientswithsinonasalpolyposis
(obstruction≥50%ofeachnasalpassage).
1999
Bicanetal.192010 4months Prospective
study
20 100 47.5 31 Rhinoseptoplasty,withemphasisonthe
nasalvalve,improvementandCPAPpreand
post-op.
1999
Choietal.202011 3months Prospective
study
22 100 41.3 25.5 Aftertheuseoftopicalsteroidswithout
nasalobstructionimprovement,theywere
submittedtonasalsurgery(5endoscopic,
17septoplastieswithturbinectomy).
2007
Sufio˘gluetal.21
2012
3months Prospective
study
31 83.9 53 30.3 Surgeries:(1)threeseptoplasties,(2)two
rhinoseptoplasties,(3)eighteen
septoplastiesandturbinectomies,(4)four
sinusectomies,septoplastiesand
turbinectomies(5)fourbilateralinferior
turbinectomies.
2007
Systematicreview:theinfluenceofnasalobstructiononsleepapnea 227
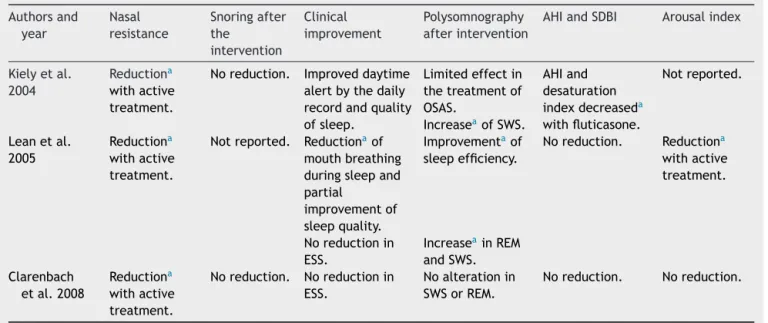
Table2 Changeswithclinicaltreatment. Authorsand
year
Nasal resistance
Snoringafter the
intervention
Clinical improvement
Polysomnography afterintervention
AHIandSDBI Arousalindex
Kielyetal. 2004
Reductiona
withactive
treatment.
Noreduction. Improveddaytime
alertbythedaily
recordandquality
ofsleep.
Limitedeffectin
thetreatmentof
OSAS.
AHIand
desaturation
indexdecreaseda
withfluticasone.
Notreported.
IncreaseaofSWS.
Leanetal.
2005
Reductiona
withactive
treatment.
Notreported. Reductionaof
mouthbreathing
duringsleepand
partial
improvementof
sleepquality.
Improvementaof
sleepefficiency.
Noreduction. Reductiona
withactive
treatment.
Noreductionin
ESS.
IncreaseainREM
andSWS.
Clarenbach
etal.2008
Reductiona
withactive
treatment.
Noreduction. Noreductionin
ESS.
Noalterationin
SWSorREM.
Noreduction. Noreduction.
AHI,apneaandhypopneaindex;SDBI,sleep-disorderedbreathingindex;ESS,EpworthSleepinessScale;SWS,slow-wavesleep;CPAP, continuouspositiveairwaypressure;desaturationindex,numberofdesaturations≥4%perhourofsleep.
a Statisticallysignificantdifference.
etal.19 andSufio˘gluetal.21)showedsignificantreduction
inAHIandCPAPpressure.AftersurgeryandtheuseofCPAP,
Nakataetal.14showeddecreaseinCPAPpressure,without
reductionintheAHI.
Fourstudies17,18,20,21 showedareductionofsnoring,and
Sufio˘gluetal.21reportedthatthisimprovementwas
subjec-tive.Onlytwostudies14,19 showedincreaseintheminimum
nocturnal oxygen saturation postoperatively. In addition,
Bicanetal.19 andChoietal.20 showedanincreaseintotal
sleep timeand increase in the percentage of REM sleep.
Onlyonestudy21showedanincreaseinN3+N4sleep
(slow-wavesleep).Nostudywithsurgicalinterventionassessedor
demonstratedanychangesinthearousalindex(Table3).
Discussion
Sleep-disordered breathing (SDB), according to the Third
InternationalClassificationofSleepDisorders(ICSD-3),22 is
characterizedbyventilationabnormalitiesduringsleepand,
sometimesmaybepresentduringwakefulness.Itcomprises
four categories: OSAS, central sleepapnea, sleep-related
hypoventilation/hypoxemia, and upper-airway resistance
syndrome (UARS); individuals can display more than one
condition.Thisreviewshowsaseriesof297cases,inwhich
patients with different causes of nasal obstruction were
submittedtoclinical andsurgical interventions,and were
evaluatedforpolysomnographyindicesandclinical
improve-ment.
OSAS wasthe best-studiedandmost accepteddisorder
inthemedicalcommunity.Itischaracterizedbypartialor
totalobstructionoftheupperairways,calledhypopneaand
apnea,withepisodicdropsinoxyhemoglobinsaturationand
recurrentawakenings.10Inadditiontotheseevents,
respi-ratory effort-related arousals (RERA) may occur, without
apneaorhypopnea,maintainingoxyhemoglobinlevels
sta-bleduringsleep.Theseawakeningshaveconsequences,such
assleepfragmentation and excessive daytimesleepiness,
andare related to another SDB known asUARS.23,24 Only
Sufio˘gluetal.21assessedsleepfragmentation,
demonstrat-ingtheeffectsonsleeparchitecture,showingthescarcity
ofstudiesaboutthisaspect.
Nasal medications did not improve snoring. Two
studies12,13 used vasoconstrictors for a short period, but
bothonlyreducednasalresistanceandimprovedsubjective
aspectsofsleep.Possibly,thechronicuseof
vasoconstric-torsmight nothave the sameeffect,asit couldresultin
drug-inducedrhinitis.
Allstudieswithsurgicalintervention14---21decreasednasal
resistance,withmostofthemresultinginthereductionof
snoringandexcessivedaytimesleepiness,althoughtheydid
notreduce AHI. Twostudies19,21 showedsignificant
reduc-tioninAHI. Sufio˘glu etal.21 demonstratedtheincrease in
theslow-wavesleeppercentage.Twotrials19,20 showedan
increaseintotalsleeptimeandpercentageofREMsleep.
Insome studies,thesleeparchitecturewasnot reported,
indicating the need for better study of this aspect with
significantbehavioralandneurologicaleffects.Nosurgical
interventionevaluatedorshowedanychangeinthearousal
index.Anincreaseofthisindexsuggestsairflowlimitation
thatcausesmicro-arousals,withconsequentsleep
fragmen-tationandsometimes,intermittenthypoxia.This notonly
would result in metabolic disorders, but also irritability,
anxiety, difficulty in consolidating memory, and reduced
concentrationandattention, whichcouldimpairthe
indi-vidual’sproductivity.23,24
Threestudies that usedCPAP14,19,21 showedthat it was
possibletoreducethepressurenecessaryforeffectiveuse
following intervention, which improved treatment
Migueis
DP
et
al.
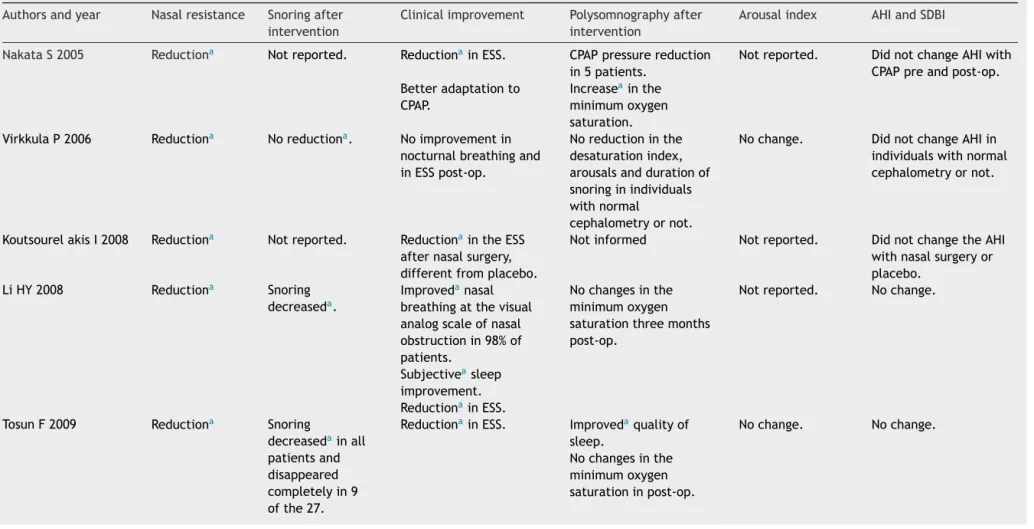
Table3 Changeswithsurgicaltreatment.
Authorsandyear Nasalresistance Snoringafter intervention
Clinicalimprovement Polysomnographyafter intervention
Arousalindex AHIandSDBI
NakataS2005 Reductiona Notreported. ReductionainESS. CPAPpressurereduction
in5patients.
Notreported. DidnotchangeAHIwith
CPAPpreandpost-op.
Betteradaptationto
CPAP.
Increaseainthe
minimumoxygen
saturation.
VirkkulaP2006 Reductiona Noreductiona. Noimprovementin
nocturnalbreathingand
inESSpost-op.
Noreductioninthe
desaturationindex,
arousalsanddurationof
snoringinindividuals
withnormal
cephalometryornot.
Nochange. DidnotchangeAHIin
individualswithnormal
cephalometryornot.
KoutsourelakisI2008 Reductiona Notreported. ReductionaintheESS
afternasalsurgery,
differentfromplacebo.
Notinformed Notreported. DidnotchangetheAHI
withnasalsurgeryor
placebo.
LiHY2008 Reductiona Snoring
decreaseda.
Improvedanasal
breathingatthevisual
analogscaleofnasal
obstructionin98%of
patients.
Nochangesinthe
minimumoxygen
saturationthreemonths
post-op.
Notreported. Nochange.
Subjectiveasleep
improvement.
ReductionainESS.
TosunF2009 Reductiona Snoring
decreasedainall
patientsand
disappeared
completelyin9
ofthe27.
ReductionainESS. Improvedaqualityof
sleep.
Nochange. Nochange.
Nochangesinthe
minimumoxygen
Systematic
review:
the
influence
of
nasal
obstruction
on
sleep
apnea
229
Table3 (Continued)
Authorsandyear Nasalresistance Snoringafter intervention
Clinicalimprovement Polysomnographyafter intervention
Arousalindex AHIandSDBI
BicanA2010 Reductiona Notreported ReductionainESSin
post-opofpatientswith
CPAP.
IncreaseainREM. Notreported. AHIdecreaseda.
IncreaseainN1,N2and
totalsleeptime,inthe
post-op.
Reductionainpressureto
CPAPinthepost-op.
NodifferenceinN3+N4
sleep.
Improvedasubjective
comfortofnasalflow.
Increaseainthe
minimumoxygen
saturation.
ChoiJH2011 Reductiona Snoring
decreaseda.
Reductionain
ESS.
IncreaseainREM. Nochange. DidnotchangetheAHI
ortheminimumoxygen
saturation,withisolated
nasalsurgery.
Increaseaintotalsleep
timeandsleep
efficiency.
Sufio˘gluM2012 Reductiona Subjective
improvementa
onlyofsnoring.
ReductionainESS. IncreaseainN3+N4. Notreported. DidnotchangetheAHI.
TheAHIdecreasedto
lessthan5/hin5
patients,whichmeans
thecureofOSAS.
IncreaseainCPAP
tolerance.
Improvementaof
subjectivecomplaintsof
obstruction,snoring,
apneaanddaytime
sleepiness.
Reductionofpressureof
CPAPinthepost-op.
Reduction*oftotal
durationofapneasand
hypopneas.
AHI,apneaandhypopneaindex;SDBI,sleep-disorderedbreathingindex;ESS,EpworthSleepinessScale;TST,totalsleeptime;N3+N4,slow-wavesleep;CPAP,continuouspositiveairway pressure.
intheminimumoxygensaturationaftersurgery,whichcan
resultinmetabolicandneurologicalbenefitstothe
individ-ual.
ThisreviewshowedthatmanyauthorsconsidertheAHI
tobeveryimportant, without assessingthe arousal index
andsleeparchitecture.Thismayresultinthe
underdiagno-sisof theUARS, impairingthe understanding of excessive
sleepinessassociatedwithit,whichcoulddeprivepatients
ofatreatmentthatcouldbringthembenefits.
Only two studies, carried out in 2011 and 2012, used
the2007 AAMSManual, indicating that theothers didnot
evaluate RERA and the SDBI, the sum of the number of
apneas,hypopneas, andRERAdividedbytotalsleeptime.
In the last task force to prepare the 2012 AAMS Manual,
RERAmeasurementbecamemandatory,anairflowlimitation
withtheformationofaplateauinthenasalcannula,lasting
10s,associatedwithawakening.Inthe2007AAMSManual,
measuringthe number of RERAwas optional, despite the
relevanceofUARSandSDBI.
Recently, arousals have been studied more frequently.
Terzanoetal.25describedarousalswithacyclicalternating
pattern(CAP)duringnon-REM(NREM)sleepinpatientswith
normalAHI,buthighrateofrespiratorydisorders.Theyhad
UARSwithfatigueanddaytimesleepiness,despitenormal
AHI,reinforcingtheassociationbetweenthenumberofCAP,
indicativeofNREMsleepfragmentation,withtheEpworth
SleepinessScale.However,theCAPhasnotbeenestablished
asacriterionintheAMMS-2012,indicatingtheneedfor
fur-therstudiestoreinforceitsclinicalsignificance.Finally,the
inclusionofCAPhasalteredsomeparadigms.
Arousaliscurrentlydefinedasfrequenciesgreaterthan
16Hz (nozones), preceded by 10s of sleep, lastingmore
than3s,whileCAPlastslongerthan2s.Theinclusion,for
instance,oftheCAPinAAMSManualcanincreasethe
sensi-tivityofthepolysomnographystudy,allowingthediagnosis,
treatment, and monitoring of previously neglected
disor-ders.Thestandardpolysomnographicreportofmoststudies
inthisreviewdoes notallow thequantificationofaspects
withsignificantclinicalrepercussions.
The articles by Choi etal.20 and Sufio˘gluet al.21 from
2011and2012, respectively, usedtheAMMS-2007Manual,
commentingonsleepfragmentationandarousalindex.
Friedmanetal.,26 showedthatpatientswithmoderate
tosevereOSASwhounderwentnasalreconstruction,
post-operativelyexhibitedworseobjectivesleepstudyfindings.
Possibly,thiswasduetoanexistingneuromuscularchangein
theupperairwaythatwasnotcorrected throughan
inter-ventionexclusively performed at the nasal level. Indeed,
during muscle relaxation, patients with less fragmented
sleepcanhavemoreREMsleep,aswellasmoreapneaand
hypopnea.However,thisparadoxicaleffectofnasalsurgery
ontheSDBIrequiresfurtherstudy.
Onefactorthatcomplicatesthedefinitionof
therapeu-ticsuccessisthelackofparametersforOSASimprovement.
Oneof themostcommonly usedcriterion forintervention
successis an improvement of SDBIto≤50%of the
preop-erativevalue,withapreoperativevalueof<20eventsper
hour.27 However,therearecriticisms regardingitsuse for
severeOSASor in patientswithpre-interventionSDBI
val-uescloseto20eventsperhour.Othersuccesscriteriawere
created, suchasa reductionin the SDBI toless than five
eventsperhour,improvementinoxygensaturationtolevels
>90%,andsignificantreductionofevents,28butthesedonot
adequatelyassesstheimprovementofpatientswithsevere
OSAS.Thus,aconsensusregardingthisdefinitionisneeded.
Another aspect observed during the selection of
arti-cles was the increasing number of studies performed
withportablepolysomnography without thepresenceof a
technician(polysomnography type2). These articleswere
excluded from this review. The AMMS-2012 Manual10 and
ICSD-322 consider portable polysomnography a useful tool
in clinicalpractice,but thepossibleloss ofthe qualityof
theexaminationduetolackofsupervisionbyatechnician
shouldbeevenbetterestablishedbyresearch.
Conclusion
Weobservedalargenumberofclinicaltrialsthatusedseptal
deviationandallergicrhinitisasfactorsinnasalobstruction
duringthelasttenyears.Onlyonestudy considerednasal
polyposis(NP)asacauseofobstruction.Persistentallergic
rhinitisis animportantfactor ofnasalobstruction,butits
intensitymayvary.NPhasmoreobjectivetoolsforassessing
theseverityoftheobstruction.
Onlyfourstudiesrecordedasignificantimprovementin
snoring; three studies showed a reduction in CPAP
pres-sure and seven reported subjective sleep improvement.
Thus,thenasalroleonthephysiopathologyofOSASremains
imprecise. Reduction in excessive daytimesleepiness was
observedinsomestudies,measuredbytheEpworth
Sleepi-nessScale.
Inmosttrials,nasalobstructionwasnotassociatedwith
AHI, indicating no improvement in OSAS with nasal
resis-tance reduction. In contrast, few researchers evaluated
polysomnographyindices,suchasthearousalindexand
per-centage of REM sleep, which could be altered, as nasal
obstructionsometimesdoesnotcausecompleteupper
air-way obstruction, but increases the negative intrathoracic
pressure,leadingtosleepfragmentation.Thus,more
stud-ies are required on the influence of nasal obstruction on
polysomnography.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.TufikS,Santos-SilvaR,TaddeiJA,BittencourtLR.Obstructive sleep apnea syndrome in theSao PauloEpidemiologic Sleep Study.SleepMed.2010;11:441---6.
2.PangK.TheroleofnasalsurgeryinthetreatmentofOSA.Curr OtorhinolaryngolRep.2013;1:20---4.
3.PoirierJ,GeorgeC,RotenbergB.Theeffectofnasalsurgeryon nasalcontinuouspositiveairwaypressurecompliance. Laryngo-scope.2014;124:317---9.
4.MeenEK,ChandraRK.Theroleofthenoseinsleep-disordered breathing.AmJRhinolAllergy.2013;27:213---20.
Systematicreview:theinfluenceofnasalobstructiononsleepapnea 231
6.Alt J, Smith T, Mace J, Soler Z. Sleep quality and disease severityinpatientswithchronicrhinosinusitis.Laryngoscope. 2013;123:2364---70.
7.MedronhoRA,BlochKV.Epidemiologia.2a
ed.SãoPaulo(SP): EditoraAtheneu;2008.
8.VonElmE.StrobeStatement[STROBEWebsiteupdated2014 Mar17];2014.Availablefrom:http://www.strobe-statement. org/pdf/index.php?id=available-checklists[cited12.08.14]. 9.JohnsMW.Anewmethodformeasuringdaytimesleepiness:the
Epworthsleepinessscale.Sleep.1991;14:540---5.
10.BerryRB,BrooksR,GamaldoCE,HardingSM,LIoydRM, Mar-cusCL,etal.,fortheAmericanAcademyofSleepMedicine. Themanual for the scoringof sleep and associated events: rules,terminologyandtechnicalspecifications(AASM).2nded. Westchester,IL:AmericanAcademyofSleepMedicine;2012. 11.KielyJL,NolanP,McNicholasWT.Intranasalcorticosteroid
ther-apyfor obstructivesleepapnoeainpatientswithco-existing rhinitis.Thorax.2004;59:50---5.
12.McLeanH,UrtonA,DriverH,TanAK,DayAG,MuntPW,etal. Effectoftreatingseverenasalobstructionontheseverity of obstructivesleepapnoea.EurRespirJ.2005;25:521---7. 13.ClarenbachCF,KohlerM,SennO,ThuenheerR,BlochK.Does
nasaldecongestion improveobstructive sleepapnea?JSleep Res.2008;17:444---9.
14.NakataS,NodaA,YagiH,YanagiE,MimuraT,OkadaT,etal. NasalresistancefordeterminantfactorofnasalsurgeryinCPAP failurepatientswithobstructivesleepapneasyndrome. Rhinol-ogy.2005;43:296---9.
15.VirkkulaP,BachourA,Hyt¨onenM,SalmiT,MalmbergH, Hurmer-intaK,etal.Snoringisnotrelievedbynasalsurgerydespite improvementinnasalresistance.Chest.2006;129:81---7. 16.KoutsourelakisI,GeorgoulopoulosG,PerrakiE,VagiakisE,
Rous-sosC,ZakynthinosSG.Randomised trialofnasal surgeryfor fixednasalobstructioninobstructivesleepapnoea.EurRespir J.2008;31:110---7.
17.LiHY, LinY, ChenNH, LeeLA, Fang TJ,Wang PC. Improve-mentinqualityoflifeafternasalsurgeryaloneforpatientswith obstructivesleepapneaandnasalobstruction.ArchOtolaryngol HeadNeckSurg.2008;134:429---33.
18.TosunF,KemikliK,YetkinS,OzgenF,DurmazA,GerekM.Impact ofendoscopic sinussurgeryonsleepquality inpatientswith chronic nasalobstructionduetonasal polyposis.JCraniofac Surg.2009;20:446---9.
19.BicanA,KahramanA,BoraI,KahveciR,HakyemezB.Whatis theefficacyofnasalsurgeryinpatientswithobstructivesleep apneasyndrome?JCraniofacSurg.2010;21:1801---6.
20.ChoiJH,KimEJ,KimYS,KimTH,ChoiJ,KwonSY,etal. Effec-tivenessofnasalsurgeryaloneonsleepquality,architecture, position,and sleep-disordered breathingin obstructivesleep apneasyndrome withnasalobstruction. AmJRhinolAllergy. 2011;25:338---41.
21.Sufio˘gluM,OzmenOA,KasapogluF,DemirUL,UrsavasA,Eris¸en L,etal.Theefficacyofnasalsurgeryinobstructivesleepapnea syndrome:aprospectiveclinicalstudy.EurArch Otorhinolaryn-gol.2012;269:487---94.
22.AmericanAcademyofSleepMedicine.International classifica-tionofsleepdisorders:diagnosticandcodingmanual(ICSD-3). 3rded.Westchester,IL:AmericanAcademyofSleepMedicine; 2014.
23.GuilleminaultC,StoohsR,ClerkA,CetelM,MaistrosP.Acause ofexcessivedaytimesleepiness.Theupperairwayresistance syndrome.Chest.1993;104:781---7.
24.PalombiniL,LopesMC,TufickS,GuilleminaultC,Bittencourt LR.Upperairwayresistancesyndrome:stillnotrecognizedand nottreated.SleepSci.2011;4:72---8.
25.TerzanoMG,ParrinoL,SmerieriA,ChervinR,ChokrovertyS, GuilleminaultC,etal.Atlas,rules,andrecordingtechniquesfor thescoringofcyclicalternatingpattern(CAP)inhumansleep. SleepMed.2002;3:187---99.
26.FriedmanM,TanyeriH,LimJW,LandsbergR,VaidyanathanK, CaldarelliD.Effectofimprovednasalbreathingonobstructive sleepapnea.OtolaryngolHeadNeckSurg.2000;122:71---4. 27.Friedman M, Ibrahim H, Bass L. Clinical staging for
sleep-disordered breathing. Otolaryngol Head Neck Surg. 2002;127:13---21.