www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Oral
cavity
squamous
cell
carcinoma:
factors
related
to
occult
lymph
node
metastasis
夽
,
夽夽
André
Fernandes
d’Alessandro
a,
Fábio
Roberto
Pinto
b,
Chin
Shien
Lin
b,
Marco
Aurélio
Vamondes
Kulcsar
b,
Cláudio
Roberto
Cernea
a,
Lenine
Garcia
Brandão
a,
Leandro
Luongo
de
Matos
b,∗aDisciplineofHeadandNeckSurgery,FaculdadedeMedicina,UniversidadedeSãoPaulo(USP),SãoPaulo,SP,Brazil bInstitutodoCâncerdoEstadodeSãoPaulo(ICESP),SãoPaulo,SP,Brazil
Received12November2013;accepted6July2014
Availableonline30March2015
KEYWORDS Carcinoma; Squamouscell; Mouth; Lymphatic metastasis; Prognosis
Abstract
Introduction:Electiveneckdissectionisrecommendedincases oforalcavitysquamouscell carcinomawithoutlymphnodemetastasisbecauseoftheriskofoccultmetastasis.
Objective:Thepresentstudyaimedtoevaluatepredictivefactorsforoccultlymphnode metas-tasisinpatientswithoralcavitysquamouscellcarcinomatreatedwithelectiveneckdissection andtheirimpactonoverallanddisease-freesurvival.
Methods:Fortysurgicallytreatedpatientswereretrospectivelyincluded.
Results:Tencases(25%)hadlymphatic metastasis.Of thestudiedvariables,perineuraland angiolymphaticinvasioninadditiontotumorthicknesswerestatisticallyassociatedwithlymph nodemetastasis.Onlyangiolymphaticinvasion was identifiedasanindependent risk factor foroccultmetastasisinthelogisticregression(OR=39.3;p=0.002).Therewasnoassociation betweenoverallanddisease-freesurvivalwiththepresenceofoccultlymphnodemetastasis. Conclusion:Metastaticdiseaseratewassimilartothatfoundintheliterature.Perineuraland angiolymphaticinvasionandtumorthicknesswereassociatedwithoccultmetastasis,butonly angiolymphaticinvasionshowedtobeanindependentriskfactor
© 2015Associac¸ãoBrasileira de Otorrinolaringologiae CirurgiaCérvico-Facial. Publishedby ElsevierEditoraLtda.Allrightsreserved.
夽 Pleasecitethisarticleas:d’AlessandroAF,PintoFR,LinCS,KulcsarMA,CerneaCR, BrandãoLG,etal.Oralcavitysquamouscell
carcinoma:factorsrelatedtooccultlymphnodemetastasis.BrazJOtorhinolaryngol.2015;81:248---54.
夽夽Institution:InstitutodoCâncerdoEstadodeSãoPaulo(ICESP),SãoPaulo,SP,Brazil.
∗Correspondingauthor.
E-mail:[email protected](L.L.deMatos).
http://dx.doi.org/10.1016/j.bjorl.2015.03.004
1808-8694/©2015Associac¸ãoBrasileiradeOtorrinolaringologia eCirurgiaCérvico-Facial. PublishedbyElsevierEditoraLtda.All rights
PALAVRAS-CHAVE Carcinoma;
Célulasescamosas; Boca;
Metástaselinfática; Prognóstico
Carcinomaespinocelulardacavidadeoral:fatoresrelacionadosàpresenc¸ade metástaseslinfonodaisocultas
Resumo
Introduc¸ão: Oesvaziamentocervicaleletivoérealizadodemaneirasistemáticanoscasosde carcinomaespinocelulardacavidadeoralsemlinfonodosclinicamentecomprometidosdevido àaltaincidênciademetástasesocultas.
Objetivo: Avaliarpacientescomcarcinomaespinocelulardecavidadeoraltratadoscom esvazi-amentocervicaleletivoquantoafatorespreditivosparaocorrênciademetástasesocultaseo impactodasmesmasnasobrevivênciaglobalelivredeprogressãodestespacientes.
Método: Quarentapacientescirurgicamentetratadosforamavaliadosemestudoretrospectivo. Resultados: Dezcasos(25%)apresentarammetástasesocultas.Dasvariáveisanalisadas,invasão perineuraleangiolinfáticaetambémaespessuratumoralforamestatisticamentesignificantes àanáliseunivariada.Apenasainvasãoangiolinfáticafoifatorindependentederiscode metás-tasesocultaspelaregressãologística(OR=39,3;p=0,002).Apresenc¸ademetástaseocultanão apresentoudiferenc¸aestatisticamentesignificanteemrelac¸ãoàstaxasdesobrevivênciaglobal elivredeprogressão.
Conclusão:Aincidênciademetástaseocultafoisemelhanteàliteratura.Ainvasãoperineural, angiolinfáticaeaespessuratumoralforamfatoresassociadosàpresenc¸ademetástaseoculta, porémapenasainvasãoangiolinfáticaapresentou-secomoumfatorderiscoindependentepara ocorrênciadofenômeno.
©2015Associac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial.Publicado por ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Squamouscellcarcinoma isthemost commonhistological type of cancer of the oral cavity, and has an important and well-established pattern of dissemination to cervical lymphnodes.1Even inpatientsclinicallywithout evidence ofmetastaticlymphnodes(N0),electiveneckdissectionin conjunctionwithresectionoftheprimarytumor,ispartof thestandard treatmentof thediseasebecausetheriskof occultmetastasisisgreaterthan20%.1---6
Several studies have triedto assessfactors that would predict occult metastases and their influence on survival rates,suchastumorthickness,perineuralinvasionand angi-olymphatic invasion.1,7---10 In attempts to reduce surgical morbidity,somehaveproposedalternativestoelectiveneck dissection, such as sentinel lymph node mapping11,12 and evenavoidinganysurgicalapproachtotheneckinselected cases;13,14 thelatter hasthe poorestsurvival results.5,15,16 Thus,elective neckdissection currentlyremains themost widelyusedtreatment.
The present study aimed to evaluate the risk of the presenceofoccultlymphnodemetastasesinpatientswith squamous cell carcinoma of the oral cavity submitted to resectionandelectiveneckdissection,inordertoidentify factors related to the development of nodal metastases, and to identify its impact on overall and disease-free survival.
Method
This wasa longitudinal historical cohort study that, after approvalbytheEthicsCommitteeofInstitutionalResearch
underNo.507/11,retrospectivelyassessedelectronic medi-calrecords of consecutive patients submitted to primary tumorresectionwithintenttocurecombinedwithelective neckdissectionin patients withoral cavitysquamouscell carcinoma(includingthelip).Fortypatientswereselected fromAprilof2009(beginningoftheHeadandNeckSurgery Service)untilDecemberof2012.
Inclusioncriteriaconsistedofcasesofsquamouscell car-cinoma of the oral cavity, whose initial treatment was a surgicalprocedurewithprimarylesionresectionand elec-tiveunilateralorbilateralneckdissection,dependingonthe lesionlocation,withallpatientsbeingconsideredN0at clin-icalexaminationandpreoperativeimagingtests.Neoplasms inothersitesthantheoralcavitywereexcluded,aswellas otherhistologicaltypes,patientswhohadsuspectedlymph nodedetectedintraoperatively,leadingtoconductchange intoradicaldissection,andpatientssubmittedtoprevious surgical treatment or chemotherapy and/or radiotherapy, evenforneoplasmslocatedatanothersiteintheheadand neck.
Patientswereassessedregarding:
1. Demographicdata:genderandage;
2. Clinicaldata:primarytumorlocation(forthisvariable, majororalcavitysubsitesweredividedintotongue,floor ofthemouth,retromolararea,lip,buccalmucosa,and alveolarborder).Patientswereonlyincludedwith squa-mous cell carcinoma of the lip when it extended to the buccal mucosa, justifying elective neck dissection accordingtotheinstitutionalprotocol;
andpT4aandpT1---pT3vs.pT4astratification),primary tumor thickness (in mm), presence or absenceof per-ineural and angiolymphatic invasion, surgical margins, pN stage,number of lymphnodes in pN+ cases, pres-enceorabsenceofcapsularleakageinmetastaticlymph nodes,andanatomopathologicalstagepergroups(I---IV) accordingtotheclassificationofAmericanjoint Commit-tee onCancer/Union for International CancerControl, UICC/AJCC(7thedition,2010);
4. Surgicaldata:relatedtotheperformedneckdissection; 5. Adjuvant treatments performed: radiotherapy and/or
chemotherapy;
6. Developmentoflocoregionalrecurrence,distant metas-tasis, and second primary tumor, as well as time of occurrenceoftheseevents;
7. Follow-up timein months,requiring a minimum of 12 monthsforpatientswhodidnotdieduringthisperiod; 8. Most recentoncological status (aliveand disease-free,
alivewiththedisease,asymptomaticdead,anddeaddue tocancer).
Statistical analysis was performed asdescribed below. Thevaluesobtainedbythestudy ofeachcontinuous vari-ablewereorganizedandexpressedasmean andstandard deviation,whereasqualitativevariableswereexpressedas absoluteandrelativefrequencies.Sampledistributionwas definedasparametricusingtheKolmogorov---Smirnovtest. Comparisonsof the frequency of a phenomenon between groupsofqualitativevariableswereperformedusingFisher’s exacttestorthechi-squaredtest.Thecomparisonbetween themeans ofacontinuousvariablewithparametric distri-butionbetweentwogroupswasperformedusingStudent’s
t-test.Thelogisticregressionmodelwasusedinthe multi-variateanalysis,establishingvaluesofoddsratio(OR)and 95%confidenceinterval(95%CI).
TheKaplan---Meiermethodwasusedforsurvivalanalysis andcomparisonofgroupswasperformedusingthelog-rank test.AllanalyseswereperformedusingStatisticalPackage fortheSocialSciences,(SPSSstatisticalsoftware),version 17.0(SPSSInc---Illinois,USA),withasignificancelevelof5% (p<0.05).
Results
Ofthe40patients,35(87.5%)weremalesandmeanagewas 60years(minimum40andmaximumof89years,standard deviationof12.9years).
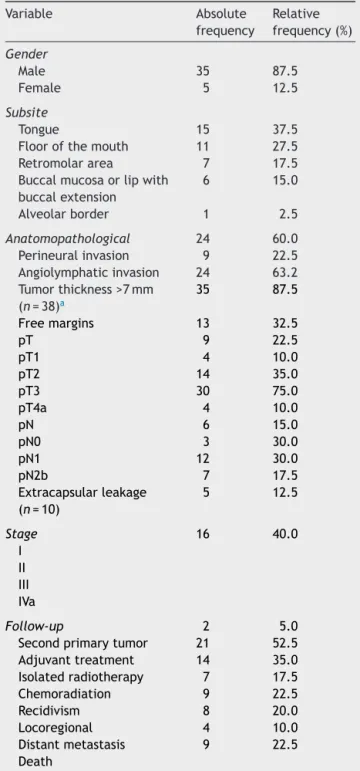
The most often affectedsubsiteswere thetongue and thefloorofthemouth(65%)andtherewasapredominance of advanced stages (stages III and IV=52.5%). As for the histologicalcharacteristicsofprimarytumors,meantumor thicknesswas1.4±1.2cm;infivecases(12.5%)thefinal sur-gicalmarginswereconsideredinvolved;24tumors(60%)had perineuralinvasionandnine(22.5%)showedangiolymphatic invasion.Meanfollow-upwas18monthsandninecasesof diseaseprogressionwereidentified(fiveexclusively locore-gionalrecurrences,onecaseofpulmonarymetastasiswith controlledprimarysiteandneck, andthreepatients with both)andmorethanhalf ofthepatients (52.5%)required adjuvant treatment. The descriptive data of the entire seriesareshowninTable1.
Table1 Demographic,clinical,andanatomopathological data(n=40).
Variable Absolute
frequency
Relative frequency(%)
Gender
Male 35 87.5
Female 5 12.5
Subsite
Tongue 15 37.5
Floorofthemouth 11 27.5
Retromolararea 7 17.5
Buccalmucosaorlipwith buccalextension
6 15.0
Alveolarborder 1 2.5
Anatomopathological 24 60.0
Perineuralinvasion 9 22.5
Angiolymphaticinvasion 24 63.2 Tumorthickness>7mm
(n=38)a
35 87.5
Freemargins 13 32.5
pT 9 22.5
pT1 4 10.0
pT2 14 35.0
pT3 30 75.0
pT4a 4 10.0
pN 6 15.0
pN0 3 30.0
pN1 12 30.0
pN2b 7 17.5
Extracapsularleakage
(n=10)
5 12.5
Stage 16 40.0
I II III IVa
Follow-up 2 5.0
Secondprimarytumor 21 52.5
Adjuvanttreatment 14 35.0
Isolatedradiotherapy 7 17.5
Chemoradiation 9 22.5
Recidivism 8 20.0
Locoregional 4 10.0
Distantmetastasis 9 22.5
Death
a Thickness:mean±standarddeviation=1.4±1.2cm.
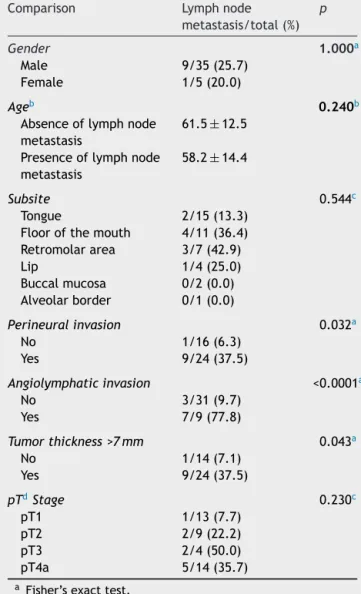
Table2 Univariateanalysisoffactorsrelatedtothe pres-enceofoccultlymphnodemetastasis.
Comparison Lymphnode
metastasis/total(%) p
Gender 1.000a
Male 9/35(25.7)
Female 1/5(20.0)
Ageb 0.240b
Absenceoflymphnode
metastasis
61.5±12.5
Presenceoflymphnode
metastasis
58.2±14.4
Subsite 0.544c
Tongue 2/15(13.3)
Floorofthemouth 4/11(36.4)
Retromolararea 3/7(42.9)
Lip 1/4(25.0)
Buccalmucosa 0/2(0.0)
Alveolarborder 0/1(0.0)
Perineuralinvasion 0.032a
No 1/16(6.3)
Yes 9/24(37.5)
Angiolymphaticinvasion <0.0001a
No 3/31(9.7)
Yes 7/9(77.8)
Tumorthickness>7mm 0.043a
No 1/14(7.1)
Yes 9/24(37.5)
pTdStage 0.230c
pT1 1/13(7.7)
pT2 2/9(22.2)
pT3 2/4(50.0)
pT4a 5/14(35.7)
a Fisher’sexacttest.
b Comparisonbetweenmeansofage---Student’st-test.
c Chi-squaredtest.
d Note: no statistically significant difference was observed
betweenthestratifiedpTstageandthepresenceofoccultlymph
nodemetastasis (p=0.274 and p=0.278,respectivelyfor pT1
andpT2vs.pT3andpT4a,andpT1---pT3vs.pT4a).
assessment(Table1),andnoneofthepatientsundergoing bilateralneckdissectionhadN2cstage.
ThevariabletumorthicknesswassubmittedtoROCcurve analysis,anditwasdeterminedthatthebestcutoffforrisk stratification ofoccult lymphnode metastaseswas>7mm (areaundertheROCcurveof68.2%;95%CI:50.3%---86.1%). The univariate analysis,detailed in Table 2, showed that thepresenceofperineuralinvasion(p=0.032;Fisher’sexact test), angiolymphatic invasion (p<0.0001; Fisher’s exact test),andtumorthickness>7mm(p=0.043;Fisher’sexact test)werefactorsrelatedtothepresenceofoccultlymph nodemetastases.
Variables with p<0.20 in the univariate analysis were submittedtoalogisticregressionmodel,showninTable3. It was verifiedthat angiolymphatic invasion wasthe only independent risk factor for the presence of occult lymph
Table3 Multivariateanalysisofriskfactorsforthe pres-enceofoccultlymphnodemetastasis.
Factor OR 95%IC pa
Presenceofangiolymphatic
invasion
39.3 3.7---420.9 0.002
Presenceofperineural
invasion
1.5 0.1---23.7 0.766
Tumorthickness>7mm 11.6 0.7---204.3 0.093
a Logisticregression.
node metastasis (OR=39.3; 95% CI: 3.7---420.9; p=0.002). Asthiswasaretrospectivestudy,thecalculationofpower forthisestimatewasconductedduring theanalysis,using themethodfor cohortstudies. ConsideringtheORof39.3 andtheproportionof25%ofoccultlymphnodemetastases inthisgroup,theinclusionof40patientsdeterminedthat thisestimatedemonstratedpower>90%.
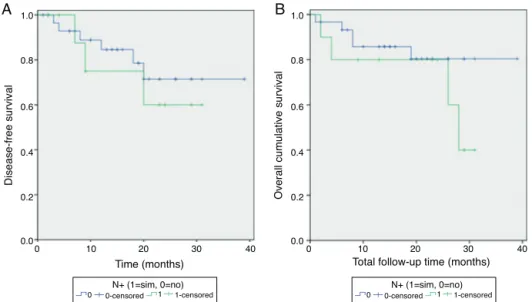
Survival analysisshowed that disease-freesurvival and overallcumulativesurvival(Figure1)were68.2%and64.1%, respectively.Eventhoughtherewasnostatistically signifi-cantdifference,patientswithoccultlymphnodemetastases showeda lowerdisease-freesurvival rate,aloweroverall survival, and a median survival of 28 months in the final analysis,comparedtopatientswithoutthisfactor(Table4; Figure2).
Discussion
The presence of occult metastases in squamous cell car-cinoma of the oral cavity is very prevalent due to its aggressiveness1 and neck treatment is mandatory, even in cases without clinical signs of involvement. Surgical treatment has an advantage over radiotherapy, since it establishesthepatient’scompletepathologicalstaging, pre-ventingunnecessaryuseofradiotherapyinsomecases.17
Thissampleshowedaprevalenceofmalepatients,with mosttumorslocatedinthetongueandfloorofthemouth, consistentwiththeliterature.3,7,16 Thepresence ofoccult metastases in 25% of cases was in agreement with other studies.1,3,4,18 With regard to all cases with positive neck involvement,it isnoteworthythatthreecaseshad metas-tasisinmorethanonecervicallevel,andinthreecasesthe metastaseswere stages II and/or III, withlevel I disease-free.NopatienthadlevelIVinvolvement.Thisshowsthat althoughsomecasesofskipmetastasesoccurred,dissection atlevelsI---III wouldhavebeensufficienttreatment forall patientsinthisseries.
Disease-free survival Cumulative survival 1.0
Survival Function Censored
0.8
0.6
0.4
0.2
0.0
0 10 20
A
B
Time (months) Total follow-up time (months) 30 40
1.0
0.8
0.6
0.4
0.2
0.0
0 10 20 30 40
Survival Function Censored
Figure1 Kaplan---MeierCurves.(A)Cumulativedisease-freesurvivalof68.2%;(B)Cumulativeoverallsurvivalof64.1%.
Table4 Analysisofoverallanddisease-freesurvival.
Variable Events/total Accumulatedsurvival(%) pa
Disease-freesurvival 0.587
Absenceoflymphnodemetastasis 6/30 71.4
Presenceoflymphnodemetastasis 3/10 60.0
Overallsurvival 0.248
Absenceoflymphnodemetastasis 5/30 80.4
Presenceoflymphnodemetastasis 4/10 40.0b
aLog-ranktest.
b Medianofsurvivalattainedat28months.
In the many existing studies, the major risk factors for occult metastases are angiolymphatic invasion, per-ineuralinvasion, and tumor thickness.1,2,4,8,9,17,19 This was corroboratedbythepresentstudy,butonlyangiolymphatic
invasion was shown to be an independent risk factor of occultmetastases.
Althoughstudiesincreasinglyfocusonthese characteris-ticsaspredictorsoflymphaticdissemination,fromaclinical
Disease-free survival
Overall cumulative survival
1.0
0-censored
0 1 1-censored
0.8
0.6
0.4
0.2
0.0
0 10 20
A
B
Time (months)
30 40 1.0
N+ (1=sim, 0=no)
0.8
0.6
0.4
0.2
0.0
0 10 20
Total follow-up time (months) 30 40
0-censored
0 1 1-censored
N+ (1=sim, 0=no)
pointofview,exceptforthickness,allarefactorsthatare inaccessibleuntiltumorresectionandthereforemaynotbe usedfor decision-making,suchasnottreatingtheneckor usinglessinvasivetreatmentssuchassentinellymphnode technique. When positron emissiontomography-computed tomography(PET-CT),whichhasbeenincreasinglyusedand studied, is negativefor the neck,it is considered enough evidencetojustifyexpectantconduct,butthepatient sam-plesevaluatedwerefewandfollow-upwasnotlongenough toevaluatesurvivalor morbiditieswhensalvage neck dis-sectionisemployed.19,23
The sentinellymphnode(SLN)techniqueforthe treat-mentofN0patientshasbeenstudiedsincethe1990s.Ithas similarratestoelectiveneckdissectionforthedetectionof occultmetastases.24,25 AEuropeanmulticenterstudy com-paredtwogroups,oneusingthesentinellymphnodeandone withsystematicextensiontoselectiveneckdissectionwitha follow-upoffiveyears;itfoundcervicalrecurrenceinthree casesconsiderednegativeintheSLNarmbutnorecurrence intheother group.24 Italsoshoweddifferencein disease-freesurvival,butwithoutstatisticalsignificance.24Another Europeanstudywithfollow-upof10years,inwhichSLNwas carriedoutwithoutsystematicneckdissectionin 53cases froma totalof 174, showedmethod failurerate of 4.8%, withnegativepredictivevalueof95.2%,consideredbythe authorsimilartothatofelectiveneckdissection.25
Tumor thickness has been widely studied as a predic-tor of cervical lymph node metastases in patients with squamouscellcarcinomaoftheupperaerodigestivetract, especiallybecauseupto40%ofpatientswiththesetumors exhibit occult metastases.26 Huang et al.27 performed a meta-analysisanalyzingtumorthicknessandtheriskof cer-vicallymphnode metastasis.Theyconcludedthata4-mm cutofffor tumor thicknesswouldbe astrong predictorof thepresenceofoccultcervicallymphnodemetastasis;they foundarateof16.6%amongpatientswithtumorthickness >4mm,comparedto4.5%amongthosewithtumorthickness ≤4mm.
Fukanoetal.28studied34patientswithtonguecarcinoma treatedwithearlysurgicalresectionswithoutpreoperative therapy.Meantumorthicknesswas6.4mm(0---18.2mm)and 64.7% of patients with tumor thickness >5mm had lymph nodemetastases,comparedto5.9%ofpatientswith thick-ness<5mm.Thepresentstudyestablishedacut-offof7mm as a predictor of occult neck metastases, established by theROCcurveanalysis.Thisindex,slightlyhigherthanthat foundintheliterature,isprobablyduetothefactthatthe presentstudywasperformedinapublicinstitution,inwhich patientspresentwithmoreadvancedneoplasmsatthe ini-tialdiagnosis.Themeantumorthicknesswas14mmand45% ofpatientshadpT3andpT4atumors,whichunfortunately iscomparabletomostBrazilianoncologicalinstitutions,and oneofthelimitationsforcomparisonofresults,especially withinternationalcaseseries.
Thisstudyalsodocumentedasmallproportionofoccult metastasesinpatients withpT1 or pT2stage(17.4%),but thisresultissimilartothatfoundintheliterature.Kelner etal.29foundratesof12.5%and22.4%fortheincidenceof lymphnodemetastasesinpatientswithsquamouscell carci-nomaoftheoralcavitythatwererespectivelypT1andpT2 (20.5%when thestageswere added).Thus,Poonachaand Go30 question whether elective neck dissection should be
performedin thispopulation despitetherecommendation oftheAmericanprotocol.
Pathologicalfeaturesarevaluableforindicationof adju-vanttreatmentwithradiotherapyand/orchemotherapy,as patientswithknownpresenceofcervical metastaseshave lowersurvivalrates,especiallydisease-freesurvival, com-paredtopatientswithoutneckinvolvement.Theoveralland disease-freesurvivalcurvesshowninthisstudydemonstrate theeffectofthepresenceoflymphnodeinvolvementon dis-easeevolution;evenwhentheinvolvementismicroscopic, the necessary adjuvant therapy is performed. However, thesepatientshaveloweroverallanddisease-freesurvival ratesthanpatientswithtumorsconfinedtotheprimarysite. The fact that the oncological follow-up period of five yearshasyettobecompletedisalimitationofthisstudy. Thisoccurred becausetheInstitute opened in2009; how-ever,theauthorsbelievethatthisfacthaslittleinfluenceon survivalanalysis.Itiswellknownintheliteraturethattumor recurrence occurs mainly in the first year of follow-up. Pintoetal.31 found that92.8%oflocoregionalrecurrence occurredwithinthefirst12monthsoffollow-upinpatients withsquamouscellcarcinomaoftheoralcavityand orophar-ynx.
Conclusions
Thisstudydemonstratedthattheincidenceofoccult metas-tasesinsquamouscellcarcinomaoftheoralcavitywas25% in a population consisting of 45% pT3 and pT4a patients. Amongthefactorsevaluated,perineuralandangiolymphatic invasionandtumor thickness>7mm wereassociated with thepresenceofoccultneckmetastases,butonly angiolym-phaticinvasionprovedtobeanisolatedriskfactorforthe occurrenceoftheevent. Disease-freesurvival andoverall survivalinthe twogroups exhibiteddifferences,although theywerenotstatisticallysignificant.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.PimentaAmaralTM,DaSilvaFreireAR,CarvalhoAL,PintoCA, KowalskiLP.Predictivefactorsofoccultmetastasisand prog-nosisofclinicalstagesIandIIsquamouscellcarcinomaofthe tongueandfloorofthemouth.OralOncol.2004;40:780---6.
2.ByersRM,El-NaggarAK,LeeYY,RaoB,FornageB,TerryNH, etal.Canwedetectorpredictthepresenceofoccultnodal metastasesinpatients withsquamouscarcinoma oftheoral tongue?HeadNeck.1998;20:138---44.
3.Yu S,LiJ,Li Z,ZhangW,ZhaoJ.Efficacyofsupraomohyoid neckdissectioninpatientswithoralsquamouscellcarcinoma andnegativeneck.AmJSurg.2006;191:94---9.
4.Lim YC, Kim JW, Koh YW, Kim K, Kim HJ, Kim KM, et al.
Perivascular---submandibular lymph node metastasis in squa-mouscellcarcinomaofthetongueandfloorofmouth.EurJ SurgOncol.2004;30:692---8.
dissectioninoralcavitycancerswithclinicallynode-negative neck.OralOncol.2011;47:320---4.
6.El-NaajIA,LeiserY,ShveisM,SaboE,PeledM.Incidenceoforal canceroccultmetastasisandsurvivalofT1-T2N0oralcancer patients.JOralMaxillofacSurg.2011;69:2674---9.
7.JerjesW,UpileT,PetrieA,RiskallaA,HamdoonZ,Vourvachis M,et al.Clinicopathologicalparameters, recurrence, locore-gionalanddistantmetastasisin115T1-T2oralsquamouscell carcinomapatients.HeadNeckOncol.2010;20:2---9.
8.Martínez-GimenoC,RodríguezEM,VilaCN,VarelaCL.Squamous cell carcinomaoftheoralcavity: aclinicopathologicscoring systemforevaluatingriskofcervicallymphnodemetastasis. Laryngoscope.1995;1057Pt1:728---33.
9.MortonRP,FergusonCM,LambieNK,WhitlockRM.Tumor thick-nessinearlytonguecancer.ArchOtolaryngolHeadNeckSurg. 1994;120:717---20.
10.VijayakumarM,BurrahR,SabithaKS,NadimulH,RajaniBC.To operateornottooperateN0neckinearlycancerofthetongue? Aprospectivestudy.IndianJSurgOncol.2011;2:172---5.
11.Paleri V, Rees G, Arullendran P, Shoaib T, Krishman S. Sen-tinelnode biopsyinsquamous cellcancer oftheoralcavity and oral pharynx: a diagnostic meta-analysis. Head Neck. 2005;27:739---47.
12.GoversTM,HanninkG, MerkxMA,TakesRP,RoversMM. Sen-tinel node biopsy for squamous cell carcinoma of the oral cavityandoropharynx:adiagnosticmeta-analysis.OralOncol. 2013;49:726---32.
13.VandenbrouckC,Sancho-GarnierH,ChassagneD,SaravaneD, CachinY,MicheauC.Electiveversustherapeuticradicalneck dissectioninepidermoidcarcinomaoftheoralcavity:results ofarandomizedclinicaltrial.Cancer.1980;46:386---90.
14.NieuwenhuisEJ,CastelijnsJA,PijpersR,vandenBrekelMW, Brakenhoff RH, van der Waal I, et al. Wait-and-see policy for the N0neck inearly-stageoral and oropharyngeal squa-mouscellcarcinomausingultrasonography-guidedcytology:is therearoleforidentificationofthesentinelnode?HeadNeck. 2002;24:282---9.
15.FakihAR,RaoRS,PatelAR.Prophylacticneckdissectionin squa-mouscellcarcinomaoforaltongue:aprospectiverandomized study.SeminSurgOncol.1989;5:327---30.
16.Kligerman J, Lima RA, Soares JR, Prado L, Dias FL, Freitas EQ, et al. Supraomohyoid neck dissection in the treatment ofT1/T2squamouscellcarcinoma oforalcavity.AmJSurg. 1994;168:391---4.
17.GendenEM,FerlitoA,SilverCE,TakesRP,SuárezC,OwenRP, etal.Contemporarymanagementofcanceroftheoralcavity. EurArchOtorhinolaryngol.2010;267:1001---17.
18.FerlitoA,SilverCE,RinaldoA.Electivemanagementoftheneck inoralcavitysquamouscarcinoma:currentconceptssupported byprospectivestudies.BrJOralMaxillofacSurg.2009;47:5---9.
19.KowalskiLP,SanabriaA.Electiveneckdissectioninoral carci-noma:acriticalreviewoftheevidence.ActaOtorhinolaryngol Ital.2007;27:113---7.
20.ShahJP,CandelaFC,PoddarAK.Thepatternsofcervicallymph nodemetastasesfromsquamouscarcinomaoftheoralcavity. Cancer.1990;66:109---13.
21.DavidsonBJ,KulkarnyV,DelacureMD,ShahJP.Posteriortriangle metastasesofsquamouscellcarcinomaoftheupper aerodiges-tivetract.AmJSurg.1993;166:395---8.
22.WoolgarJA.Detailedtopographyofcervicallymph-node metas-tasesfromoralsquamouscellcarcinoma.IntJOralMaxillofac Surg.1997;26:3---9.
23.GoshenE,DavidsonT,YahalomR,TalmiYP,ZwasST.PET/CT intheevaluationofpatientswithsquamouscellcancerofthe headandneck.IntJOralMaxillofacSurg.2006;35:332---6.
24.Alkureishi LW, Ross GL,Shoaib T, Soutar DS, Robertson AG, ThompsonR,etal.Sentinelnodebiopsyinheadandneck squa-mouscellcancer:5-yearfollow-upofaEuropeanmulticenter trial.AnnSurgOncol.2010;17:2459---64.
25.MelkaneAE,MamelleG, WyciskG, TemamS,JanotF, Casir-aghi O, et al. Sentinel node biopsy in early oral squamous cellcarcinomas:a10-yearexperience.Laryngoscope.2012;122: 1782---8.
26.PintoFR,deMatosLL,PalermoFC,KulcsarMA,CavalheiroBG, deMelloES,etal.Tumorthicknessasanindependentriskfactor ofearlyrecurrenceinoralcavitysquamouscellcarcinoma.Eur ArchOtorhinolaryngol.2013;271:1747---54.
27.Huang SH, Hwang D, Lockwood G, Goldstein DP, O’Sullivan B. Predictive value of tumor thickness for cervical lymph-node involvement in squamous cell carcinoma of the oral cavity:ameta-analysisofreportedstudies.Cancer.2009;115: 1489---97.
28.FukanoH,MatsuuraH,HasegawaY,NakamuraS.Depthof inva-sionasapredictivefactorforcervicallymphnodemetastasis intonguecarcinoma.HeadNeck.1997;19:205---10.
29.KelnerN,VartanianJG,PintoCA,Coutinho-CamilloCM, Kowal-ski LP. Does electiveneck dissection in T1/T2 carcinoma of theoraltongueand floorofthemouthinfluencerecurrence andsurvivalrates?BrJMaxillofacSurg.2014,pii:S0266-4356: 00127-2.
30.Poonacha TK, Go RS. Level of scientific evidence underly-ingrecommendationsarisingfromtheNationalComprehensive Cancer Network clinical practice guidelines. J Clin Oncol. 2011;29:186---91.