The role of integrated home-based care in patient
adherence to antiretroviral therapy
O papel da assistência domiciliar integrada na adesão
do paciente à terapia anti-retroviral
Neil Gupta
1, Angela Caulyt Santos da Silva
2and Luciana Neves Passos
2ABSTRACT
No n- a dhe re nce is o ne o f the prim a ry o b sta cle s to succe ssful a ntire tro vira l the ra py in HIV+ pa tie nts wo rldwide . In Bra zil, the Do m icilia ry The ra pe utic Assista nce is a m ultidisciplina ry a nd inte gra te d ho m e - b a se d a ssista nce pro gra m pro vide d fo r HIV+ pa tie nts co nfine d in the ir ho m e s due to physica l de ficie ncy. This study inve stiga te d ADT’s a b ility to m o nito r a nd pro m o te a ppro pria te a dhe re nce to ARV the ra py. Fifty-six individua ls we re re cruite d fro m thre e study gro ups: Gro up 1 - pa tie nts curre ntly in the ADT pro gra m , Gro up 2 - 21 pa tie nts pre vio usly tre a te d b y the ADT pro gra m , a nd Gro up 3 - 20 pa tie nts who ha ve a lwa ys b e e n tre a te d using co nve ntio na l a m b ula to ry ca re . Using m ultiva ria b le se lf- re po rting to e va lua te a dhe re nce , pa tie nts in the ADT pro gra m ha d significa ntly b e tte r a dhe re nce tha n pa tie nts in a m b ula to ry ca re ( F = 6.66, p = 0.003) . This e ffe ct wa s inde pe nde nt o f de m o gra phic a nd so cio e co no m ic cha ra cte ristics a s we ll a s m e dica l histo ry. Pa tie nts in the ADT pro gra m a lso sho we d a tre nd to wa rds gre a te r the ra pe utic succe ss tha n a m b ula to ry pa tie nts. The se re sults sugge st the inco rpo ra tio n o f cha ra cte ristics o f ADT in co nve ntio na l a m b ula to ry ca re a s a stra te gy to incre a se a dhe re nce to ARV the ra py.
Ke y-words: HIV th e ra p y. An ti re tro vi ra l th e ra p y. Ad h e re n c e . Ho m e - b a se d c a re .
RESUMO
O suce sso da te ra pia a ntire tro vira l de pe nde da a de sã o a o tra ta m e nto . A Assistê ncia Do m icilia r Te ra pê utica é um pro gra m a de a te ndim e nto m ultidisciplina r a pa cie nte s co m HIV/AIDS e co m dificulda de s de se de slo ca r pa ra a te ndim e nto a m b ula to ria l. Este e studo co m pa ra a a de sã o de pa cie nte s a o e sq ue m a ARV e m um pro gra m a ADT co m a q ue le s e m tra ta m e nto a m b ula to ria l co nve ncio na l. Fo ra m e studa do s: Grupo 1 - 15 pa cie nte s no pro gra m a de ADT, Grupo 2 - 21 pa cie nte s e m tra ta m e nto a m b ula to ria l co nve ncio na l, Grupo 3 - 20 pa cie nte s e m tra ta m e nto a m b ula to ria l co nve ncio na l q ue nunca fre q üe nta ra m o pro gra m a ADT. Os pa cientes inscrito s no pro gra m a ADT a presenta ra m significa tiva m ente m a io r a desã o a o tra ta m ento do que pa cientes a m bula to ria is ( F = 6.66, p= 0,003) . Os re sulta do s o b se rva do s nã o fo ra m influe ncia do s pe la s ca ra cte rística s de m o grá fica s, ca ra cte rística s so cio e co nô m ica s, o u histó rico m é dico . Pa cie nte s e m pro gra m a de ADT ta m b é m m o stra ra m um a te ndê ncia a m e lho r re spo sta te ra pê utica do q ue o s a m b ula to ria is. Este e studo suge re a utiliza çã o da s ca ra cte rística s do ADT co m o e stra té gia pa ra m e lho ra r a a de sã o à te ra pia a ntire tro vira l.
Pal avr as-chave s: Te ra p i a a n ti re tro vi ra l. HIV. Ad e sã o a o tra ta m e n to . Assi stê n c i a d o m i c i li a r.
1 . Nuc le o de Do e nç as Infe c c io sas do Ce ntr o B io mé dic o da Unive r sidade Fe de r al do Espír ito Santo , Vitó r ia, ES, B r asil. 2 . Ho spital Unive r sitar io Cassiano Antô nio Mo r ae s da Se c r e tar ia de Saúde do Espír ito Santo , Vitó r ia, ES, B r asil.
Financ ial Suppo r t: Har t Fe llo wship in He alth Po lic y and So c ial Me dic ine , Har t Le ade r ship Pr o gr am, Duk e Unive r sity, Dur ham, NC, USA.
Addr e ss to: Dr. Ne il Gupta. C/O Har t Fe llo ws Pr o gr am, B o x 9 0 2 4 8 , Duk e Unive r sity, Dur ham NC 2 7 7 0 8 - 0 2 4 8 , USA. e mail: ne ilg@ mail. me d. upe nn. e du
Re c e b ido par a pub lic aç ão e m 2 0 /8 /2 0 0 3 Ac e ito e m 7 /3 /2 0 0 5
One of the main obstac les to suc c essful antiretroviral ( ARV)
tr e atme nt o f HIV/AIDS patie nts wo r ldwide is patie nt no
n-adherenc e to the treatment regimen. Previous studies report that 6 0 to 6 9 % of patients in B razil c omply with ARV therapy, a
perc entage c onsidered insuffic ient to c ontrol the epidemic3 1 1.
Non-adherenc e has been found to be assoc iated with negative
c linic al outc ome in terms of blood viremia1 4, CD4 c ell c ounts3,
patient survival7, and is largely responsible for the emergence of
drug resistant forms of the virus6. The predictive value of economic
and soc iodemographic c harac teristic s is c ontroversial5 1 3, with
some studies reporting the assoc iation of age8, rac e1 0, inc ome1 0,
educ ation9, and health knowledge9 with adherenc e. Soc ial and
psyc hologic al aspec ts have also been implic ated in determining
Gupta N e t al
Other studies, however, have provided c ompelling evidenc e that the quality and c harac teristic s of health servic es are a greater
de te r m i n a n t to a dh e r e n c e th a n p a ti e n t o r tr e a tm e n t
c harac teristic s2. Some authors have suggested that in order to
inc rease adherenc e, health c are pro viders sho uld c o nsider
treatment strategies that plac e a greater emphasis on individual
c irc umstanc es, lifestyle, soc ial support and home life 1 1 6. Various
HIV/AIDS programs have implemented home-based c are, either
within or outside the traditional health c are system, to support
these proposals for personalized and integrated health c are
s e ttin gs1 2. On e s uc h pr o gr a m , de n o m in a te d Do m ic ilia r y
Therapeutic Assistanc e ( ADT) has been implemented in the state
of Espírito Santo, Brazil.
ADT is a fully integrated service that utilizes a multidisciplinary
he alth te am, c o nsisting o f a do c to r, nur se , so c ial wo r k e r, physiotherapist, and psyc hologist, to meet the needs of HIV+
patients c o nfined within their ho mes. Patients who pr esent
physic al defic ienc y that makes it impossible for them to seek
c o nventio nal c ar e in ho spital/ambulato r y c ar e settings, ar e referred to the ADT program by various units in the public health
system, primarily after hospital disc harge. As many of these
patients have previously demonstrated problems with treatment
adherenc e and often present greater diffic ulties in c ontinuing with medic ation, it is important to assess the effec tiveness of
this form of c are in promoting and monitoring appropriate
adherenc e.
The present study explores the role of the ADT program on
patient adherenc e to ARV medic ations. A multivariable indic ator o f adher enc e, tak ing into ac c o unt patient self-r epo r ts, last
treatment missed, and the frequenc y of individual diffic ulties over
the past year, is used to c ompare adherenc e between patients
under c are of the ADT program and those rec eiving c onventional ambulatory c are servic es.
MATERIAL AND METHODS
Sixty sub j e c ts r e c r uite d fo r the study we r e divide d into thr e e gr o ups: Gr o up 1 – patie nts c ur r e ntly e nr o lle d in the
ADT pr o gr am (c u rre n t ADT) , Gr o up 2 – patie nts who we r e
pr e vio usly e nr o lle d in the ADT pr o gr am b ut sub se q ue ntly disc har ge d to se e k tr e atme nt in c o nve ntio nal se ttings afte r
sho wing signific ant impr o ve me nt in physic al ab ility (p a st
ADT) , and Gr o up 3 – patie nts who had ne ve r b e e n e nr o lle d
in the ADT pr o gr am (n o n - ADT) and se e k tr e atme nt at the
Amb ulato r y Car e Se r vic e o f the Unive r sity Ho spital Cassiano
Antô nio Mo r ae s, a lar ge r e fe r e nc e ho spital in Vitó r ia, B r azil.
Patients fr o m the ADT pr o gr am wer e admitted to the pr o gr am
b ase d o n physic al o r psyc ho so c ial r e quir e me nts, r athe r than
b y vo luntar y insc r iptio n. Additio nally, no sub j e c ts in the no n-ADT gr o up had pr e vio usly q ualifie d o r b e e n o ffe r e d n-ADT
se r vic e s. All sub j e c ts we r e HIV+ , at le ast 1 8 ye ar s o f age , no t
pr e gnant, and had b e e n pr e sc r ib e d ARV the r apy fo r at le ast th r e e m o n th s o ve r th e pr e vio us ye a r. All s ub j e c ts we r e
r e c e iving ARV me dic atio ns pr o vide d fr e e o f c har ge b y the
B r azilian he alth se r vic e s.
Subjec ts were interviewed in their home or at the hospital. Subjec ts from the non-ADT group were randomly selec ted from
the daily agenda of c onsultations in the ambulatory c enter by a
rando m number generato r. These subj ec ts, therefo re, were
se le c te d inde pe nde nt o f o r de r o f ar r ival o r adhe r e nc e to
sc heduled appointments. All were requested to partic ipate in the study before or after their regular c onsultation, and signed
an informed c onsent form approved by the Institutional Review
Boards of the Centro Biomédic o of the Universidade Federal do
Espírito Santo ( Vitória, BR) and Duke University ( NC, USA) .
All interviews were c onduc ted by the same interviewer in reassuring, c omfortable loc ations with minimal distrac tion. If
the subjec t was c onsidered inc apable of c ompleting the interview
inde pe nde ntly, c ar e pr o vide r s we r e r e q ue ste d to assist in
ac c urately c ompleting the interview.
The questionnaire used for the interview solic ited personal data, patie nt se lf-r ating o f adhe r e nc e ( 0 -6 r ating) , r e c all o f
last do se misse d ( 0 - 4 r ating) , r e aso ns fo r failing to tak e
me dic atio ns ( 0 -3 r ating fo r e ac h o f 2 0 po ssib le r e aso ns) ,
date s and r e aso ns fo r ab ando nme nt, and o pinio ns o n he alth c a r e s e r vi c e s . Me d i c a l h i s to r y, i n c l u d i n g d i a gn o s e s ,
me dic atio ns, and e xam r e sults, we r e o b taine d fr o m patie nt
c har ts fo llo wing the inte r vie w. The CDC Gu i d e li n e s f o r Usi n g
An ti r e tr o vi r a l Age n ts Am o n g HIV- In f e c te d Ad u lts a n d Ad o le sc e n ts asse r t that vir al lo ad is a mo r e r e liab le indic ato r
o f the r ape utic suc c e ss than CD4 c e ll c o unts4; the r e fo r e , this
study defined suc c essful ther apy as an undetec tab le vir al lo ad
( < 4 0 0 c o pie s/ml) in the mo st r e c e nt vir al lo ad te st, r e po r te d at le ast thr e e mo nths afte r initiatio n o f tr e atme nt.
Patient adherence to prescribed ARV medication was assessed
by c alc ulating the patient’s Complianc e Sc ore. Complianc e Sc ore
being the sum of the self-rating for adherence ( 0 a 6 = never miss
à always miss/abandonment) , last dose missed ( 0 a 4 = never à today) , and frequenc y of missed treatment due to eac h of twenty
possible reasons ( 0 a 3 = never miss à frequently miss) . Using
th is fo r m ula , a Co m plia n c e Sc o r e o f 0 in dic a te s pe r fe c t
adherenc e, with 7 0 being the highest possible non-adherenc e sc ore. ( Subjec ts who had abandoned treatment at the time were
still asked for reasons why they missed treatment during the
period that they were taking medic ations over the last year. The
most c ompliant possible sc ore for these subjec ts was 1 0 ) .
Statistic al analysis was c ompleted by k-way ANOVA with Tukey HSD and Bonferroni post-hoc tests for numeric al c omparisons and Kruskal-Wallis test for nonparametric c omparisons.
RESULTS
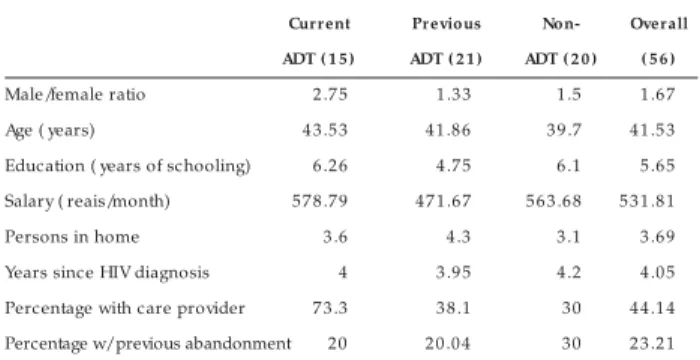
Demo gr aphic and so cio eco no mic char acter istics. A total of 5 6 subjec ts partic ipated in the study ( three selec ted sub j e c ts we r e unab le to b e inte r vie we d, o ne sub j e c t was pregnant and exc luded from the study) . The mean age was 4 1 .5 years and 6 2 .5 % were male and 3 7 .5 % female ( Table 1 ) . Re gar ding e duc atio nal le ve l, 1 6 .1 % had a se c o ndar y sc ho o l
formal educ ation. Average household inc ome was 5 3 2 reais per month ( approximately US$ 1 6 9 ) . On average, the subjec ts lived
with 3 .7 other family members, and 4 4 .1 % reported having a
primary c are provider that helps them with their ARV treatment. These c are-providers were most often mothers and spouses, but
also siblings, in-laws, children or hired workers. No demographic
or soc ioec onomic c harac teristic showed signific ant assoc iation
with Complianc e Sc ore or c linic al outc omes. Only perc entage o f sub j e c ts r e po r ting having a pr imar y c ar e pr o vide r was
signific antly assoc iated with study group ( p = 0 .0 3 1 ) .
Medical histor ies. Of all subjects, 3 0 .4 % had lived less than two years with a positive diagnosis for HIV, 6 0 .7 % for less than 4
years, and 9 1 .1 % for less than six years ( Table 1 ) . The most common opportunistic and co-infections among these subjects
were toxoplasmosis ( 3 5 .7 %) , tuberculosis ( 3 0 .4 %) , candidiasis
( 2 3 .2 %) , cytomegalovirus ( 1 2 .5 %) , herpes virus ( 1 2 .5 %) and
hepatitis C ( 1 2 .5 % ) . Half of all subjec ts were undergoing a treatment regimen of nucleoside analogue reverse transcriptase
inhibitors ( NRTIs) in combination with protease inhibitors ( PIs) ,
2 9 .6 % of subjects NRTIs with non-nucleoside reverse transcriptase
inhibitors ( NNRTIs) , 5 .6 % NNRTIs with PIs, 1 .9 % of subjects NRTIs
only, and 1 3 % triple-therapy consisting of all three categories of medic ations. None of these medic al fac tors were signific antly
associated with Compliance Score or clinical outcomes.
Clinical outcomes. Overall, 4 9 .9 % of subjec ts exhibited successful therapy ( also referred to as successful clinical outcome)
as demonstrated by undetectable viral load results ( Figure 1 ) .
Successful clinical outcome was seen in 5 7 .1 % of current ADT patients, 4 7 .6 % of previous ADT patients and 4 5 % of non-ADT
subjects. There was no significant association between study group
and clinical outcome.
Ad h e r e n c e t o ARV t r e a t m e n t . Th e o ve r a ll m e a n Complianc e Sc ore was 8 .2 7 , with values ranging from 0 ( perfec t
adherenc e) to 3 9 . The mean Complianc e Sc ore for c urrent ADT patients was 4 .0 , for previous ADT patients 6 .7 6 , and for
non-ADT patie nts 1 3 .0 5 ( Figur e 1 ) . Co mplianc e Sc o r e diffe r e d
signific antly b e twe e n c ur r e nt ADT and no n- ADT sub j e c ts
( F = 6 .6 6 , p = 0 .0 0 3 ) and between previous ADT and non-ADT subjec ts ( p = 0 .0 2 9 ) . Complianc e Sc ore was not signific antly
c orrelated with c linic al outc ome.
Adher ence difficulties/abando nment. Of the subjec ts interviewed, 2 3 .2 % had previously or c urrently abandoned ARV
therapy – 2 0 % of ADT patients, 2 0 % of previous ADT patients, and 3 0 % of non-ADT patients ( Table 1 ) . There was no signific ant
differenc e among these groups. The most frequently reported
reasons for missing treatment were a wa y fro m ho m e ( 4 6 % ) ,
fo rge tting ( 3 2 % ) , m e dica tio ns ra n o ut ( 3 2 % ) , side -e ffe cts/
sick ( 2 9 % ) , and sle e ping ( 2 7 % ) . These reasons were reported
evenly ac ross the three study groups.
Patient pr efer ences/opinions. The approval rating of ADT services by current and previous ADT patients was 9 7 % compared
to 8 3 % fo r amb ulato r y c ar e . Amo ng 3 3 sub j e c ts who had experienc ed both ADT and ambulatory c are servic es, 6 9 .7 %
preferred the ADT service, 1 5 .2 % preferred ambulatory care, and
1 5 .2 % had no preference.
DISCUSSION
Home-based c are has been used to personalize c are in a
wide variety of health fields, inc luding HIV/AIDS c are, not only
to provide improved assistanc e for patients but also to reduc e burdens on overc rowded and under resourc ed heath systems.
However, the effec t of these programs on treatment adherenc e
has yet to be established. Ac c o r ding to the ADT Gu i de f o r
Pro ce dure s in HIV/AIDS, one of the princ iple objec tives of the
ADT program is to pro m o te the i m p ro ve m e n t o f tre a tm e n t
Table 1 - Su bject popu lation profile.
Cur r ent Pr evious Non- Over all
ADT ( 1 5 ) ADT ( 2 1 ) ADT ( 2 0 ) ( 5 6 )
Male/female ratio 2 .7 5 1 .3 3 1 .5 1 .6 7
Age ( years) 4 3 .5 3 4 1 .8 6 3 9 .7 4 1 .5 3
Education ( years of schooling) 6 .2 6 4 .7 5 6 .1 5 .6 5
Salary ( reais/month) 5 7 8 .7 9 4 7 1 .6 7 5 6 3 .6 8 5 3 1 .8 1
Persons in home 3 .6 4 .3 3 .1 3 .6 9
Years since HIV diagnosis 4 3 .9 5 4 .2 4 .0 5
Percentage with care provider 7 3 .3 3 8 .1 30 4 4 .1 4
Percentage w/ previous abandonment 20 2 0 .0 4 30 2 3 .2 1
All values are group means unless otherwise indicated. Study group sample size given in parenthesis.
0
2
4
6
8
10
12
14
Current ADT Previous ADT Non-ADT
Study Group
0% 10% 20% 30% 40% 50% 60% 70%
Poorer adherence
Average Compliance Score Therapeutic success
Mean
Compliance
Score
%
therapeutic
success
a d h e re n c e o f HIV/AIDS p a ti e n ts1 2. The pr e se nt study is the
fir st to c o nfir m the suc c e ss o f ADT in ac hie ving this o b j e c tive .
Adh e r e n c e a m o n g pa tie n ts in th e ADT pr o gr a m wa s s ign ific a n tly b e tte r th a n pa tie n ts wh o we r e tr e a te d with
c onventional ambulatory c are and had never been under the
c are of the program ( F = 6 .6 6 , p = 0 .0 0 3 ) . Adherenc e among
subjec ts who had previously been in the ADT program but were now under c onventional c are was between these two groups and
also significantly better than non-ADT subjects ( p = 0 .0 2 9 ) . These
effec ts were independent of demographic , soc ioec onomic , and
treatment c harac teristic s, all of whic h were found not to be signific antly assoc iated with adherenc e.
Studies have traditionally used self-report as the primary tool
to assess patient adherenc e, using measures suc h as self-rating,
rec all of last-dose missed, or report of pills missed in past three
da ys . Se lf- r e po r t, a lth o ugh th o ugh t to o ve r e s tim a te tr ue adherenc e, has been demonstrated to be a reliable measure of
adhe r e nc e and is m o r e r e adily availab le than alte r native
tec hniques suc h as pill c o unts, elec tr o nic mo nito r ing, and
presc ription refill logs1 0. All existing studies establish a c ut-off
point, suc h as 80% o f pills ta k e n in pa st thre e da ys or se
lf-ra ting o f 80% a dhe re nce, to c ategorize subjec ts as a dhe re nt or
n o n - a d h e re n t5 1 3. Suc h m e a s ur e m e n ts , h o we ve r, gr e a tly
oversimplify the definition of adherenc e, establish an arbitrary threshold for adherenc e, and rely on very little data to determine
adherenc e. The Complianc e Sc ore used in this study is unique
as it inc ludes respo nses to all traditio nally used self-repo rt
measures, as well as inc orporating the frequenc y of missing tr e atme nt due to spe c ific adhe r e nc e o b stac le s, to c r e ate a
c ontinuous measure of adherenc e rather than dividing subjec ts
into disc rete adherenc e c ategories.
Patients in the ADT program also displayed a higher rate of
therapeutic suc c ess ( 5 7 .1 % ) against non-ADT patients ( 4 5 % ) .
Whereas this differenc e was not statistic ally signific ant, the trend
towards therapeutic suc c ess reflec ts ADT’s effec t on adherenc e
( Figure 1 ) . Although this trend is apparent as an overall effec t,
c linic al outc ome was not direc tly c orrelated to adherenc e within
individual patients. This suggests that therapeutic suc c ess is not
a o ne - dim e nsio nal o r highly pr e dic tab le o utc o m e pur e ly
de pe n de n t o n pa tie n t a dh e r e n c e . I n a dditio n to pa tie n t
a dh e r e n c e , th e r a te a t wh ic h vir a l lo a d de c lin e s to wa r d
undetec table levels is affec ted by the baseline CD4+ T c ell c ount,
initial viral load, potenc y of drug regimen, previous exposure to
ARV age nts, o ppo r tunistic infe c tio ns, dr ug r e sistanc e , and
malabsorption4.
The most frequently reported reasons for failing to adhere
to treatment regimen were a wa y fro m ho m e, fo rge tting, o ut o f
m e dica tio ns, side e ffe cts/ fe e ling ill and sle e ping. The suc c ess of the ADT program in promoting patient adherenc e to ARV
therapy, as c ompared to c onventional ambulatory c are, c an be
attributed in part to the servic e’s ability to assist patients to
o ve r c o m e suc h o b stac le s to adhe r e nc e . The r ape utic and
integrated home-based c are promotes an extended relationship
established between health c are team and patient. Furthermore,
it offers greater attention for family and c ommunity members,
allowing for c loser monitoring of patient needs, in terms of medic al attention, medic ations, physiotherapeutic equipment/
rehabilitation, and social and psychological support. Additionally,
in c onc entrating therapy and rehabilitation within the home, this
form of assistanc e establishes primary c are providers within the
home or c ommunity, fortifying the patient’s immediate soc ial suppo r t ne two r k and gr e atly inc r e asing pe r so nal atte ntio n
rec eived by the patient in the daily adherenc e to ARV therapy.
This fact is apparent in the high percentage of ADT patients ( 7 3 %)
reporting being cared for by a primary care provider as compared to non-ADT patients ( 3 0 % ) . The advantages of the ADT program
are apparent in patient opinions as well, sinc e 9 7 % of patients
approved of its servic es and 6 9 % preferred the servic e over ambulatory c are.
The Brazilian Ministry of Health reports that in the year 2 0 0 0 , the Brazilian government spent approximately $ 3 3 2 million on
the provision of high-cost ARV medications, or $ 4 ,1 3 7 per patient.
In light of the suc c ess of ADT to monitor and promote patient
adherenc e, the c osts of the extended resourc es of integrated home-based c are would likely be justified as a c ost-effec tive
measur e via the mo r e effec tive allo c atio n and use o f these
me dic atio ns. This pr e liminar y study j ustifie s lar ge r, mo r e
c omprehensive adherenc e studies in the future, whic h would inc lude in-depth analysis of unsuc c essful therapy ( infec tions,
death and total non-adherenc e) , c onfirmation of self-report
methods with an alternative measure of adherenc e ( i.e., pill
c o unts) , examinatio n o f fur ther HIV c ar e settings in B r azil ( r e fe r e nc e c e nte r s, day ho spitals, no n-pr o fit ho me s) , and
extensive c ost-benefit analyses.
Considering both therapeutic and public health advantages,
we rec ommend that home-based c are for physic ally defic ient
HIV/AIDS patients by multidisc iplinary teams be c onsidered as an important and valuable alternative to c onventional ambulatory
and ho spital c ar e. Fur ther mo r e, c har ac ter istic s o f the ADT
program, suc h as inc reased attention and support by health c are
professionals, integrated health c are servic es, and strengthened soc ial network for the patient, should be inc orporated into the
prac tic e of c onventional HIV c are as a means to inc rease all
patients’ adherenc e to ARV therapy.
ACKNOWLEDGEMENTS
We thank the ADT and HUCAM he alth pr o fe ssio nals fo r
the ir assistanc e in this study. We ar e also e xtr e me ly gr ate ful to Dr. Reynaldo Dietze and the Nuc leo de Do enç as Infec c io sas,
as we ll as the Har t Fe llo wship, fo r the ir c o ntinuing suppo r t.
REFERENCES
1 . B ar tle tt JA. Addr e ssing the c halle nge s o f adhe r e nc e . Jo ur nal o f Ac q uir e d Immune De fic ie nc y Syndr o me 2 9 : S2 -1 0 , 2 0 0 2 .
2 . B asso CR, B attiste lla Ne me s MI, Castanhe ir a ERL, Me lc hio r R, B r itto e Alve s MTS, Do nini AA, B r aga P, David JSE, Tunala LG. Fac ing c halle nge s o n HAART adhe r e nc e in B r azil: the r o le o f q uality o f c ar e . Ab str ac t B 1 0 4 4 2 o f AIDS Co nfe r e nc e , B ar c e lo na, 2 0 0 2 .
3 . B rigido LF, Rodrigues R, Casseb J, Oliveira D, Rossetti M, Menezes P, Duarte AJ. Impac t of adherenc e to antiretroviral therapy in HIV-1 -infec ted patients at a university public servic e in B razil. AIDS Patient Care STDS 1 5 :5 8 7 -5 9 3 , 2 0 0 1 .
4 . Dyb ul M, Fauc i AS, B ar tle tt J G, Kaplan J E, Pau AK. Guide line s fo r using a n ti r e tr o vi r a l a ge n ts a m o n g HI V- i n fe c te d a d u l ts a n d a d o l e s c e n ts : r e c o mme ndatio ns o f the pane l o n c linic al pr ac tic e s fo r tr e atme nt o f HIV. Mo r b idity and Mo r tality We e k ly Re po r t 5 1 : 1 - 4 6 , 2 0 0 2 .
5 . Eldr e d LJ , Wu AW, Chaisso n RE, Mo o r e RD. Adhe r e nc e to antir e tr o vir al and pne umo c ystis pr o phylaxis in HIV dise ase . Jo ur nal o f Ac q uir e d Immune De fic ie nc y Syndr o me Human Re tr o vir al. 1 8 : 1 1 7 - 1 2 5 , 1 9 9 8 .
6 . Fr ie dland GH, Williams A. Attaining highe r go als in HIV tr e atme nt: the c e ntr al impo r tanc e o f adhe r e nc e . AIDS 1 3 : S6 1 -7 2 , 1 9 9 9 .
7 . Gar c ia- de - Olalla P, Kno b e l H, Car mo na A, Gue lar A, Lo pe z- Co lo me s J L, Cayla J A. Impac t o f adhe r e nc e and highly ac tive antir e tr o vir al the r apy o n sur vival in HIV- infe c te d patie nts. J o ur nal o f Ac q uir e d Immune De fic ie nc y Syndr o me 3 0 : 1 0 5 -1 1 0 , 2 0 0 2 .
8 . Go r dillo V, de l Amo J, So r iano V, Go nzale z-Laho z J. So c io de mo gr aphic and psyc ho lo gic al var iab le s influe nc ing adhe r e nc e to antir e tr o vir al the r apy. AIDS. 1 3 : 1 7 6 3 -1 7 6 9 , 1 9 9 9 .
9 . Kalic hman SC, Catz S, Ramac handr an B . B ar r ier s to HIV/AIDS tr eatment and tr e atme nt adhe r e nc e amo ng Afr ic an-Ame r ic an adults with disadvantage d educ atio n. Jo ur nal o f the Natio nal Medic al Asso c iatio n 9 1 :4 3 9 -4 4 6 , 1 9 9 9 .
1 0 . Kle e b e r ge r CA, Phair JP, Str athde e SA, De te ls R, Kingsle y L, Jac o b so n LP. De te r minants o f he te r o ge ne o us adhe r e nc e to HIV-antir e tr o vir al the r apie s in th e Multic e n te r AI DS Co h o r t Study. J o ur n a l o f Ac q uir e d I m m un e De fic ie nc y Syndr o me 2 6 : 8 2 -9 2 , 2 0 0 1 .
1 1 . Laur e nc e J. Adhe r ing to antir e tr o vir al the r apie s. AIDS Patie nt Car e STDS 1 5 : 1 0 7 -1 0 8 , 2 0 0 1 .
1 2 . Mi n i s té r i o d a S a ú d e . As s i s tê n c i a D o m i c i l i a r Te r a p ê u ti c a : gu i a d e pr o c e dime nto s e m HIV/Aids. Ministé r io da Saúde , B r asília, 1 9 9 9 .
1 3 . Nemes MIB , De So uza MFM, Kalic hman AO, Gr angeir o A, So uza RA, Lo pes JF. Avaliaç ão da ader ênc ia ao tr atamento po r antir etr o vir ais de usuár io s de ambulató r io s do sistema públic o de assistênc ia à Aids no Estado de São Paulo : pr evalênc ia da ader ênc ia e fato r es asso c iado s. Ministér io da Saúde, 1 9 9 9 .
1 4 . Silve ir a MP, Dr asc hle r ML, Le ite JC, Pinhe ir o CA, Da Silve ir a VL. Pr e dic to r s o f Un de te c ta b le Pla s m a Vir a l Lo a d in HI V- Po s itive Adults R e c e ivin g Antir e tr o vir al The r apy in So uthe r n B r azil. B r azilian Jo ur nal o f Infe c tio us Dise ase 6 : 1 6 4 -1 7 1 , 2 0 0 2 .
1 5 . Singh N, B e r man SM, Swinde lls S, J ustis J C, Mo hr J A, Sq uie r C, Wage ne r MM. Adhe r e nc e o f hum an im m uno de fic ie nc y vir us- infe c te d patie nts to antir e tr o vir al the r apy. Clinic al Infe c tio us Dise ase 2 9 : 8 2 4 -8 3 0 , 1 9 9 9 .