Bancroftian filariasis in an endemic area of Brazil:
differences between genders during puberty
Filariose bancroftiana em uma área endêmica do Brasil:
diferenças entre os sexos durante a puberdade
Cynthia Braga
1, Inês Dourado
2, Ricardo Ximenes
3,
Janaína Miranda
1and Neal Alexander
4ABSTRACT
Ge n d e r d i f f e re n c e s i n su sc e p ti b i li ty to i n f e c ti o u s d i se a se s h a ve b e e n o b se rve d i n va ri o u s stu d i e s. A su rve y wa s p e rf o rm e d i n a b a n c ro f ti a n f i la ri a si s e n d e m i c a re a i n th e c i ty o f Oli n d a , Bra zi l. All re si d e n ts a ge d 5 ye a rs o r o ld e r we re e x a m i n e d b y th i c k b lo o d f i lm . Pe o p le a ge d 9 to 1 6 ye a rs we re i n te rvi e we d a n d a lso te ste d f o r f i la ri a l a n ti ge n a e m i a . Da ta we re a n a lyze d b y c o n ti n ge n c y ta b le m e th o d s a n d re gre ssi o n m o d e ls. Th e ri sk o f m i c ro f i la ra e m i a f o r m a le s wa s si gn i f i c a n tly h i gh e r. Am o n g th o se a ge d 9 to 1 6 ye a rs, th e a n a lysi s o f ge n d e r a n d f i la ri a si s b y a ge sh o we d th a t b o ys f ro m 1 5 to 1 6 ye a rs
h a d a h i gh e r ri sk o f i n f e c ti o n th a n gi rls. No a sso c i a ti o n wa s f o u n d b e twe e n m e n a rc h e a n d f i la ri a si s i n gi rls. Th e d a ta
su gge st th a t va ri a ti o n s b e twe e n ge n d e r i n f i la ri a si s c o u ld re su lt, a t le a st i n p a rt, f ro m a n i n c re a se i n su sc e p ti b i li ty o f m e n . Th i s e p i d e m i o lo gi c f e a tu re n e e d s to b e c o n si d e re d wh i le f o rm u la ti n g e li m i n a ti o n p la n s.
Ke y-words: Fi la ri a si s. Ge n d e r d i f f e re n c e s. Pu b e rty. Ri sk f a c to rs.
RESUMO
Dife re n ç a s e n tre o s se xo s q u a n to à su sc e ptib ilida de à s do e n ç a s in fe c c io sa s tê m sido o b se rva da s e m vá rio s e stu do s. Um in q u é rito de pre va lê n c ia fo i re a liza do e m u m a á re a e n dê m ic a de fila rio se b a n c ro ftia n a n a c ida de de Olin da , Bra sil. To do s o s re side n te s c o m ida de > 5 a n o s fo ra m e xa m in a do s pe la go ta e spe ssa . Mo ra do re s c o m ida de e n tre 9 e 16 a n o s fo ra m e n tre vi sta d o s e te sta d o s p a ra a p re se n ç a d e a n ti ge n e m i a f i la ri a l. Os d a d o s f o ra m a n a li sa d o s u ti li za n d o ta b e la s d e c o n tin gê n c ia e m o de lo s de re gre ssã o . O risc o de m ic ro fila ra e m ia n o s ho m e n s fo i sign ific a tiva m e n te m a is e le va do . Me n in o s c o m ida de e n tre 15 e 16 a n o s tive ra m m a io r risc o de in fe c ç ã o fila ria l do q u e a s m e n in a s. Os da do s su ge re m q u e va ria ç õ e s e n tre o s se xo s n a fila rio se po de m re su lta r de u m a u m e n to n a su sc e ptib ilida de do s ho m e n s a pa rtir da pu b e rda de ta rdia . Essa c a ra c te rístic a e pide m io ló gic a de ve se r c o n side ra da a o se fo rm u la re m o s pla n o s de e lim in a ç ã o da e n de m ia .
Pal avr as-chave s: Fi la ri o se . Di f e re n ç a s e n tre se x o s. Pu b e rd a d e . Fa to re s d e ri sc o .
1 . Ce ntr o de Pe sq uisas Agge u Magalhãe s da Fundaç ão Oswaldo Cr uz, Re c ife , PE. 2 . Instituto de Saúde Co le tiva da Unive r sidade Fe de r al da B ahia, Salvado r, B A. 3 . De par tame nto de Me dic ina Tr o pic al da Unive r sidade Fe de r al de Pe r namb uc o , Re c ife , PE. 4 . Lo ndo n Sc ho o l o f Hygie ne and Tr o pic al Me dic ine , Lo ndo n Unive r sity, Lo ndo n, UK.
Addr e ss to: Dra
Cynthia B r aga. De pto
Par asito lo gia/CPq AM/FIOCRUZ. Av. Pr o f. Mo r ae s Re go s/n, Cidade Unive r sitár ia, 5 0 6 7 0 - 4 2 0 Re c ife , PE, B r asil Te l: 5 5 8 1 3 3 0 1 - 2 5 0 0 Fax: 5 5 8 1 3 4 5 3 - 1 9 1 1
e - mail: b r aga@ c pq am. fio c r uz. b r Re c e b ido par a pub lic aç ão e m 1 0 /3 /2 0 0 4 Ac e ito e m 2 /3 /2 0 0 5
Gender differenc es in susc eptibility to several diseases have
b e e n o b s e r ve d in a n um b e r o f s tudie s1 1 2 9. I n h um a n s ,
epidemiologic al, laboratory and c linic al studies have shown
var iatio ns b e twe e n ge nde r in par asitic dise ase s inc luding
sc histosomiasis, filariasis,leishmaniasis and onc hoc erc iasis, as well as other infec tions suc h as rubella, measles, hepatitis B, and tuberc ulosis1 1.
Filar ial sur ve ys c ar r ie d o ut in B r azil and o the r e nde mic c o untr ies have o b ser ved a gr eater expr essio n o f infec tio n and
morbidity in males4 9 1 2 1 5 2 5. Usually microfilaraemia and filarial
antigenaemia, parasitic burdens and clinical manifestations are more frequently observed among males than females. Different levels of
exposure to infec ted mosquitoes might explain these patterns.
However, epidemiologic studies which investigated the influence of
socioeconomic factors, occupational exposure, individual protection
and type of clothing did not confirm their effect5.
to the beginning of women’s reproduc tive lives. This observation
led the authors to c onc lude that hormonal fac tors related to
pregnanc y might limit the fertility of the adult worms, or even make women more resistant to filarial re-infec tion. Alexander
and Grenfell3 reported a reduc tion in the parasitic burden among
women during the reproduc tive period in an endemic population
of Papua New Guinea, although the comparison between pregnant women and c ontrols demonstrated no evidenc e of a relationship
between parasite burden and pregnanc y.
In spite of efforts to c larify the mec hanisms behind gender
differenc es in lymphatic filariasis, there is no c onsensus as to
whether the differenc es are better explained by an environmental or immunologic al hypothesis, that is, as a c onsequenc e of less
exposure to the vec tor, or inc reased resistanc e to the parasite5 7.
This study inve stigate d the asso c iatio ns o f b io lo gic al and
environmental fac tors to banc roftian filariasis between genders during puberty. Among girls, menarc he was used as a proxy for
estrogen produc tion.
MATERIAL AND METHODS
The study was c arried out in Olinda, a c ity in Northeastern
Brazil, where a previous parasitologic al baseline survey found a
spatial c luster of filariasis c ases6. The area was mapped and data
were collected through a door-to-door survey performed between
Dec ember 1 9 9 9 and September 2 0 0 0 .
All households were registered and residents aged 5 years and
older were invited to be examined by thick film technique. 6 0
µ
lblood samples were drawn between 9 p.m. and midnight. Participants between the ages of 9 and 1 6 years were asked to provide an
additional blood sample to test filarial antigenaemia and then were
given a questionnaire to obtain information about time of residence
in the area, use of a bednet, occurrence of menarche, history of pregnancy and use of hormonal contraceptives.
Circ ulating filarial antigen was c hec ked using either the i m m u n o c h r o m a to gr a p h i c c a r d te s t ( AMR AD I CT, Ne w South Wales, Australia) or Og4 C3 -ELISA ( TropBio, Townsville, Australia) , whic h have similar princ iple and ac c urac y1 7.
The outcome variables were the prevalence of microfilaraemia ( mf) , the prevalenc e of c irc ulating filarial antigen ( CFA) , and mic ro filarial density. Gender and age-spec ific prevalenc e o f mic rofilaraemia and filarial antigenaemia were estimated. The mean mic rofilarial density was analyzed by negative binomial
regression1 0. Logistic regression was used to test the association
RESULTS
Epidemiological patter n of bancr oftian filar iasis in the whole population.Among 5 ,2 5 8 residents that took part in the parasitologic al survey, 3 2 8 ( 6 .2 % ) were positive by thic k
film tec hnique. There was a statistic ally signific ant assoc iation
between sex and mf (
χ
12= 3 3 .1 9 ; p < 0 .0 0 0 1 ) . The risk formales was signific antly higher than the risk for females, even afte r adj ustme nt b y age gr o up ( adj uste d OR = 1 .9 4 ; 9 5 %
CI: 1 .5 5 -2 .4 3 ; p< 0 .0 0 0 1 ) .
In males, the mf prevalenc e varied with age; it was 5 .4 % in
the 5 to 9 age group, inc reased two-and-a-half times in the 1 5 to
1 9 age group, remained c onstant through the 2 0 to 2 9 age group
and de c r e ase d to 4 .7 % b y age 5 0 . The se diffe r e nc e s we r e statistic ally signific ant (
χ
6
2
= 2 9 .9 9 ; p < 0 .0 0 0 1 ) ( Figure 1 ) . Among females, the mf prevalenc e that was 3 .9 % in the 5 to 9age group rose to 6 .0 % in the 1 5 to 1 9 group and then steadily dec reased until reac hing 2 .8 % in those over the age of 5 0 . These
differences in female age-specific prevalence were not statistically
signific ant (
χ
6
2
= 6 .5 6 ; p = 0 .3 6 3 ) ( Figure 1 ) . The test of interac tion between sex and age group was performed, but no signific ant differenc e was observed (χ
6
2
= 7 .6 2 ; p = 0 .2 6 7 ) . The estimated mean mic rofilaraemic density of 1 .6 3 ( 9 5 % CI:1 .1 8 -2 .2 7 ) mf/6 0 ml for males was signific antly higher than the
value of 0 .4 5 ( 9 5 % CI: 0 .3 4 -0 .6 0 ) mf/6 0 ml observed in females
(
χ
6
2
1= 3 0 .4 8 ; p < 0 .0 0 0 1 ) .0 2 4 6 8 10 12 14
5-9 10-14 15-19 20-29 30-39 40-50 >50
Age group (years)
Mic
rofila
riae
Pr
eva
len
ce
(%)
females males
Fi gu r e 1 - Mi cr of i l ar ae m i a pr e val e n ce , accordi n g to age an d se x am on g the total stu dy popu l ati on *.
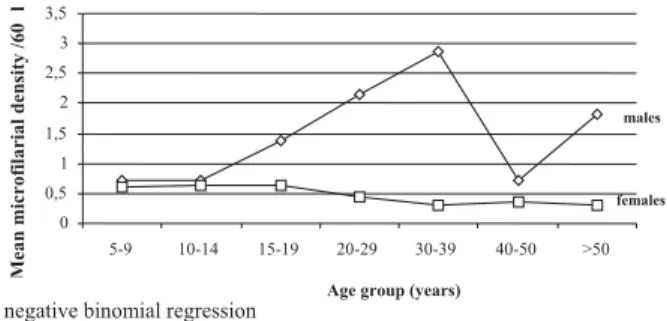
The mean mic rofilarial density in males was similar to that
in females until the 1 0 -1 4 age group, at whic h point male mean
density inc reased sharply, peaking between the ages of 3 0 and
stable through the 1 5 -1 9 year age group, after which a slight decline
was observed (
χ
6
2
= 3.63; p = 0.726) ( Figur e 2 ) .Relation between filar ial infection, biological factor s and bednet use in 9 -1 6 year olds.From the 1 ,5 1 1 boys and girls aged 9 to 1 6 registered in the area, 1 ,1 3 0 ( 7 2 .7 %) were
interviewed and examined by thick film. Of those taking part, 790
( 70%) were also tested for CFA by ICT card test ( 674) or Og4C3-ELISA ( 116) . Those who were tested for CFA did not differ significantly
from those who were not tested in age, sex or mf prevalence; this
finding ensures the comparability of the two groups ( data not shown) .
In o rder to examine the po tential c o nfo unding effec t o f
environmental factors in the association between filarial infection a nd s e x, the e ffe c t o f b e dne t us e a nd the pr e s e nc e o f a
microfilaraemic adult in the household was tested. The magnitude
of the adjusted associations between sex and mf ( OR = 1 .6 4 ; 9 5 %
CI: 1 .0 2 -2 .6 4 ) and CFA ( OR = 1 .3 1 ; 9 5 % CI: 0 .9 5 -1 .8 2 ) were similar to those obtained prior to adjustment. Bednet use was also
tested as an effect modifier in the association between sex and mf,
but the result was not statistically significant (
χ
12= 2.34; p = 0.12) .Due to the observed interaction between age and sex and also
the fact that menarche only occurs in females, the association between filarial infection and co-variables was estimated separately
for each sex. No association was found between menarche and mf
( OR = 0 .6 5 ; 9 5 % CI: 0 .1 6 -2 .6 8 ) or CFA ( OR = 0 .9 0 ; 9 5 % CI:
0 .3 1 -2 .6 3 ) . Moreover, not using a bednet did not increase risk of mf ( OR = 1 .6 4 ; 9 5 % CI: 0 .5 6 -4 .8 1 ) or CFA ( OR = 1 .7 6 ; CI
9 5 %:0 .9 4 -3 .3 1 ) in girls. In boys, however, not using a bednet was
associated with an increased risk of mf ( OR = 6 .2 4 ; 9 5 % CI: 1 .4 7
-2 6 .4 5 ) and CFA ( -2 .6 6 ; 9 5 % CI: 1 .3 8 -5 .1 0 ) . The presence of a microfilaraemic adult in the household was a risk of mf for both
boys ( OR = 3 .1 0 ; CI 9 5 %:1 .4 6 -6 .5 0 ) and girls ( OR = 3 .5 7 9 5 %
CI: 1 .5 6 -8 .1 5 ) , but was not associated with CFA.
DISCUSSION
In ac c ordanc e with previous observations4 9 1 2 1 5 2 5, this study
showed a steady inc rease of both mic rofilaraemia and parasitic b ur den in males b eginning at age 1 4 . It is kno wn that the
se nsitivity o f thic k film inc r e ase s with highe r mic r o filar ial
density1 7. Sinc e females usually exhibit lower parasite burdens
than males4, differential misc lassific ation may underestimate the
mic rofilarial prevalenc e in females and c ontribute to an apparent
gender differ enc e. In this study, analysis o f the asso c iatio n
b e twe e n ge n de r a n d fi l a r i a l i n fe c ti o n du r i n g p u b e r ty
demonstrated that, although the prevalenc e of mic rofilaraemia was signific antly higher in boys than in girls, this differenc e was
not observed for filarial antigenaemia. This finding is c onsistent
with the lower sensitivity of the thic k film tec hnique in females.
Assuming higher validity of the filarial antigenaemia results,
the c rude data do not suggest a gender differenc e in the 9 -1 6 age range. Nevertheless, the stratified analysis by age showed a
signific antly higher risk of filarial infec tion in 1 5 to 1 6 -year-old
boys. The test for an age-sex interac tion reinforc ed this finding
that that the effec t of sex on filarial antigenaemia varies by age group. Therefore, it seems that c hanges in susc eptibility to filarial
infec tion might oc c ur in men during the later stages of puberty.
This phenomenon c ould be explained by the influenc e of either
biologic al or behavioral fac tors ac ting in this period of life.
Cu le x q u i n q u e f a sc i a tu s is an e ndo philic mo sq uito o f
noc turnal habits that usually breeds in areas around dwellings. Although information c onc erning its biting behavior in Brazil is lac king, an entomologic al study in India found that the peak biting period of Cule x ranged between midnight and 3 a.m.8.
Considering this, different behavioral patterns between genders,
such as current use of bednets, fans or insecticides while sleeping, * Numb e r o f o b se r vatio ns: male s = 2 , 1 8 1 and fe male s = 3 , 0 7 1
Fi gu r e 2 - Me an m i cr of i l ar i al de n si ty, accordi n g to age an d se x am on g the total stu dy popu l ati on *.
Among the 608 girls who provided information about menarche,
3 0 3 ( 4 9 .8 %) reported its occurrence, 1 6 ( 2 .6 %) had previously
been pregnant and 5 ( 0 .8 %) were using hormonal contraceptives.
In the 9 to 1 6 -ye ar-o ld po pulatio n, the o ve r all pr e vale nc e
o f mic r o filar ae mia was 6 .9 % ( 9 5 % CI: 5 .5 -9 .8 ) and that o f antige nae mia was 2 5 .7 % ( 9 5 % CI: 2 3 .2 -3 0 .7 ) .
The crude odds ratio ( OR) for the association between mf
and sex indicated a higher risk of mf among boys ( OR = 1 .6 0 ; 9 5 %
CI: 1 .0 1 2 .5 5 ) . The ageadjusted OR ( OR = 1 .6 3 ; 9 5 % CI: 1 .0 2
-2.60) was similar to the crude OR, indicating little, if any, confounding effec t. For CFA, the differenc e was not statistic ally signific ant
before or after age adjustment. The age-stratified analyses of sex
and both mf and CFA showed that boys aged 1 5 to 1 6 years had a
higher risk of filarial infection than girls of the same age ( Table 1 ) .
A statistic ally signific ant interac tion was observed between age and sex when the outc ome was CFA, suggesting that, at least
for filarial antigenaemia, age modified the assoc iation with sex
(
χ
6
2
= 9 .5 5 ; p = 0 .0 2 ) ( Table 1 ) .Table 1- Odds ration an d 95% CI for the association between filarial in fection , sex an d age grou p.
Microfilaraemia ( n = 1 ,1 3 0 ) Antigenaemia ( n = 7 9 0 )
OR ( 9 5 % CI) OR ( 9 5 % CI)
boys versus girls boys versus girls
Sex 1 .6 0 ( 1 .0 1 -2 .5 5 ) 1 .2 5 ( 0 .9 1 -1 .7 2 ) Age gr oup ( years)
9 – 1 0 1 .8 0 ( 0 .7 3 -4 .3 7 ) 1 .7 0 ( 0 .8 7 -3 .3 1 )
1 1 – 1 2 0 .9 1 ( 0 .3 7 -2 .2 2 ) 0 .9 6 ( 0 .5 1 -1 .8 1 )
1 3 – 1 4 1 .1 7 ( 0 .3 7 -3 .7 3 ) 0 .6 5 ( 0 .3 3 -1 .2 6 )
1 5 – 1 6 3 .2 1 ( 1 .3 0 -7 .9 6 ) 2 .4 7 ( 1 .3 0 -4 .7 0 )
Age
adjusted OR 1 .6 3 ( 1 .0 2 -2 .6 0 )
-Intera ctio n test:= 4.24; p= 0.241 Intera ctio n test = 9.65; p= 0.022 3 0 0,5 1 1,5 2 2,5 3 3,5
5-9 10-14 15-19 20-29 30-39 40-50 >50
Age group (years)
Mean m icrof ilar ial d e n sity /60 m l *
* negative binomial regression
all the relevant behavioral factors7, the data suggest that individual
protec tion may not play a dec isive role in the gender differenc es
in lymphatic filariasis.
In girls, the oc c urrenc e of menarc he, used as a proxy for inc reased estrogen produc tion, was not protec tive against filarial
infec tion. Moreover, age and non-use of bednet did not c onstitute
risks of infec tion for this sex.These data suggest that pubesc ent
c hanges, whether hormonal or behavioral, do not influenc e female susc eptibility to filarial infec tion. These results reproduce, to some extent, experimental studies that investigated the role of
sexual hormones on the response to c ertain infec tious diseases
in animals. The removal of ovaries in female rats did not produc e any effec t on the intensity of the parasitism2 2 2. Conversely, the
administration of testosterone or removal of the testis in male
rats did alter the response to parasitic infec tion1 8 1 9 2 0.
Therefore, our data suggest that the observed variations
between genders in banc roftian filariasis c ould result, at least in part, from inc reased susc eptibility, possibly of physiologic al
origin, of men in the late stages of puberty.
Researc h has shown that men are often more susc eptible to
infec tions c aused by parasites, fungi, bac teria and viruses1 1. In
addition, mortality rates are usually higher in males than in females2 1. Paradoxic ally, the use of health servic es is less frequent
in th e m a le po pula tio n1 3 2 7. Th e s e s o c ia l a n d b io lo gic a l
partic ularities of genders have not been ac c ounted for in the
fo rmulatio n o f public health po lic ies to prevent, c o ntro l o r eliminate diseases. For lymphatic filariasis, males not only exhibit
more signs and symptoms of lymphatic damage, they also typically
express more mic rofilaraemia and higher parasite burdens.
These features c harac terize men as an important reservoir of filarial parasites that c ould maintain and spread disease in the
c o m m un ity. Th e r e fo r e , c o m m un ic a tio n a n d e duc a tio n a l
approac hes for elimination programs should foc us on males by promoting their c omplianc e with the mass c hemotherapy for
lymphatic filar iasis and e nc o ur aging tho se with signs and symptoms to seek early diagnosis in order to prevent more severe forms of filariasis.
ACKNOWLEDGEMENTS
We thank to Professor Andre Furtado, Dr. Alexandre B. de Carvalho and Minister of Health of Olinda for the logistic support. Also thank to Fabio Brayner, Luiz Alves and Sergio Santos for
their essential c ontribution during the fieldwork.
3 3 5 -3 5 3 , 1 9 9 0 .
5 . B r ab in L, B r ab in B J. Par asitic infe c tio ns in wo me n and the ir c o nse que nc e s. Advanc e s in Par asito lo gy 3 1 : 1 - 8 1 , 1 9 9 2 .
6 . B r aga C, Xime ne s RA, Alb uq ue r q ue M, So uza WV, Mir anda J , B r ayne r F, Alve s L, Silva L, Do ur ado I. Avaliaç ão de um indic ado r só c io - amb ie ntal utilizado no r astr e ame nto de ár e as de tr ansmissão de filar io se linfátic a e m e spaç o s ur b ano s. Cade r no s de Saúde Púb lic a 1 7 : 1 2 1 1 - 1 2 1 8 , 2 0 0 1 .
7 . B undy D. Ge nde r-de pe nde nt patte r ns o f infe c tio n and dise ase . Par asito lo gy To day 4 : 1 9 6 - 1 8 9 , 1 9 9 8 .
8 . Chandr a G. Sho r t r epo r t: peak per io d o f filar ial tr ansmissio n. The Amer ic an J o ur nal o f Tr o pic al Me dic ine and Hygie ne 5 3 : 3 7 8 - 3 7 9 , 1 9 9 5 .
9 . Chante au S, Glazio u P, Plic har t C, Luq uiaud P, Mo ulia- Pe lat J P, N’guiye n. Wu c h e re ri a b a n c ro f ti filar iasis in Fr e nc h Po lyne sia: age - spe c ific patte r ns o f mic r o filar e mia, c ir c ulating antige n, and spe c ific IgG and IgG4 r e spo nse s ac c o r ding to tr ansmissio n le ve l. Inte r natio nal J o ur nal o f Par asito lo gy 2 5 : 8 1 - 8 5 , 1 9 9 5 .
1 0 . Ellio t J M. So m e m e tho ds fo r statistic al analysis o f sam ple s o f b e nthic inve r te b r ate s. Fr e shwate r B io lo gy Asso c iatio n, Cumb r ia, 1 9 7 7 .
1 1 . Go b le FC, Ko no pk a EA. Se x as a fac to r in infe c tio us dise ase . Tr ansac tio ns o f the Ne w Yo r k Ac ade my o f Sc ie nc e s 3 5 : 3 2 5 - 3 4 6 , 1 9 7 3 .
1 2 . Ito h M, Weer aso o r iya MV, Gunawar dena NK, Mudalige MP, Samar awic kr ema WA, Kimur a E. Wuc he r e r ia b anc r o fti antige nae mia in Sr i Lank a. Tr o pic al Me dic ine and Inte r natio nal He alth 4 : 2 0 7 - 2 1 0 , 1 9 9 9 .
1 3 . Kandrac k M, Grant KR, Segall A. Sex differenc es in health related behavior: some unanswered questions. Soc ial Sc ienc e and Medic ine 5 : 5 7 9 -5 9 0 , 1 9 9 1 .
1 4 . Klein JL. The effec ts of hormones on sex differenc es in infec tion: from genes to behavior. Neurosc ienc e and B iobehavioral Review 2 4 : 6 2 7 -6 3 8 , 2 0 0 0 .
1 5 . Mac iel A, Roc ha A, Marzoc hi K, Medeiros Z, Carvalho AB , Regis L, Souza W, Lapa T, Furtado A. Epidemiologic al study of banc roftian filariasis in Rec ife, northeastern B razil. Memórias do Instituto Oswaldo Cruz 9 1 : 4 4 9 - 4 5 5 , 1 9 9 6
1 6 . Mavo ungo u D, Lanso ud- So uk ate J , Dupo nt A. Ste r o id and go nado tr o pin ho r mo ne le ve ls in yo ung Afr ic an wo me n with filar ial infe c tio n. J o ur nal o f Ste r o id and B io c he mistr y 3 4 : 5 7 7 - 5 8 0 , 1 9 8 9 .
1 7 . Mc Car thy J . Diagno sis o f lymphatic filar ial infe c tio n. In: Nutman TB ( e d) Lymphatic Filar iasis, Impe r ial Co lle ge Pr e ss, Lo ndo n, p. 1 2 7 - 1 5 0 , 2 0 0 0 .
1 8 . Mo c k B A, Nac y CA. Ho r mo nal mo dulatio n o f se x diffe r e nc e s in r e sistanc e to Le i sh m a n i a m a jo r syste m ic infe c tio ns. I nfe c tio n and I m m unity 5 6: 3 3 1 6 -3 3 1 9 , 1 9 8 8 .
1 9 . Nak anishi H, Ho r ii Y, Te r ashima K, Fuj ita K. Effe c t o f te sto ste r o ne o n the susc e ptib ility o f C5 7 B L/6 mic e to infe c tio n. J o ur nal o f Par asito lo gy 7 5: 4 5 5 -4 6 0 , 1 9 8 9 .
2 0 . Nak azawa M, Fantappie MR, Fr e e man GL, Elo i Santo s S, Olse n NJ , Ko vac s WJ , Se c o r WE, Co lle y DG. Sc histo so ma manso ni: susc e ptib ility diffe r e nc e s
b e twe e n male and fe male mic e c an b e me diate d b y te sto ste r o ne dur ing e ar ly infe c tio n. Expe r ime ntal Par asito lo gy 8 5: 2 3 3 - 2 4 0 , 1 9 9 7 .
2 1 . Owens IPF. Sex differ enc es in mo r tality r ate. Sc ienc e 2 9 7 : 2 0 0 8 -2 0 0 9 , 2 0 0 2 .
2 2 . Ro b e r ts C, Sato sk ar A, Ale xande r J. Se x Ste r o ids, Pr e gnanc y-asso c iate d Hormones and Immunity to Parasitic Infec tion. Parasitology Today 1 2 : 3 8 2 -3 8 8 , 1 9 9 6 .
2 4 . Sc huur s AH, Ve r he ul HA. Effe c ts o f ge nde r and se x ste r o ids o n the immune r e spo nse . Jo ur nal o f Ste r o id and B io c he mistr y 3 5 : 1 5 7 - 1 7 2 , 1 9 9 0 .
2 5 . Ste e l C, Otte s e n EA, We lle r PF, Nutm a n TB . Wo r m b ur de n a n d h o s t
r e spo nsive ne ss in Wu c he re ri a b a n c ro f ti infe c tio n: use o f antige n de te c tio n to r e fine e ar lie r asse ssme nts fr o m the So uth Pac ific . The Ame r ic an Jo ur nal o f Tr o pic al Me dic ine and Hygie ne 6 5 : 4 9 8 - 5 0 3 , 2 0 0 1 .
2 6 . Styr t B , Sugar man B . Estr o ge ns and infe c tio n. Re vie ws o f Infe c tio n Dise ase 1 3 : 1 1 3 9 -1 1 5 0 , 1 9 9 1 .
2 7 . Tr avasso s C, Viac ava F, Pinhe ir o R, B r ito A. Utilizaç ão do s se r viç o s de saúde no B r asil: gê ne r o , c ar ac te r ístic as familiar e s e c o ndiç ão so c ial. Re vista Paname r ic ana de Salud Pub lic a 1 1 : 3 6 5 - 3 7 3 , 2 0 0 2 .
2 8 . Ve r the lyi D. Se x ho r mo ne s as immuno mo dulato r s in he alth and dise ase . Inte r natio nal Immuno phar mac o lo gy 1 : 9 8 3 - 9 9 3 , 2 0 0 1 .