Licenciado sob uma Licença Creative Commons DOI: http://dx.doi.org/10.1590/1980-5918.030.002.AO07
[T]
Evolution of disability in traffic accident victims in
rehabilitation, characterized by the International
Classification of Functioning, Disability and Health (ICF)
Evolução da deiciência em vítimas de acidente de trânsito em
reabilitação, caracterizada pela Classiicação Internacional
de Funcionalidade, Incapacidade e Saúde (CIF)
Ligia Regina de Oliveira[a], Ana Paula Fontes da Silva Macedo[a], Cássia Maria Buchalla[b], João Henrique Gurtler Scatena[a]*
[a] Universidade Federal de Mato Grosso (UFMT), Cuiabá, MT, Brazil [b] Universidade de São Paulo (USP), São Paulo, SP, Brazil
[R]
Abstract
Introduction: The International Classification of Functioning, Disability and Health (ICF) enables moni -toring of the clinical evolution of a patient. Objective: This study aimed to characterize the evolution of disabilities in patients undergoing physical therapy following traffic accidents, using the ICF. Methods: A longitudinal study of 53 accident victims was conducted between April and October 2010, in a rehabilita -tion unit in the capital of Mato Grosso State, Brazil. Data from physical therapy evalua-tion were collected in 2 stages and coded by the ICF. Results: The average time between evaluation and reevaluation was 73.4 days. The evolution of functional impairment demonstrated a reduction in the number of patients with deficits, except for muscle tone functions. On initial evaluation, 90.6% had difficulty with sensory functions and pain, varying from mild to complete, decreasing to 67.9% on reevaluation, with pain still mostly pres -ent. Almost all patients (96.2%) had a disability of neuromusculoskeletal and movement related functions
* LRO: PhD, email: [email protected]
on initial assessment, with a decrease to 15.7% of patients on reevaluation. The greatest improvements were observed in the categories of muscle strength (36.7%) and gait pattern (30.6%). On reevaluation, im -provement was also observed regarding perceived impairment of body structures, especially for those with severe and complete disability. Conclusion: The study confirmed a reduction in the percentage of patients with some form of disability, and positive development in functional capacity. The use of ICF enabled evalu -ation of physical disabilities and monitoring of the evolution of patients undergoing physical therapy.
Keywords: Disability Evaluation. International Classification of Functioning, Disability and Health. Traffic Accidents. Rehabilitation. Physical Therapy Specialty.
Resumo
Introdução: A Classificação Internacional de Funcionalidade, Incapacidade e Saúde (CIF) permite acompanhar a evolução clínica do paciente. Objetivo: Este estudo objetivou caracterizar a evolução das deficiências em vítimas de acidentes de trânsito, em tratamento fisioterápico, utilizando essa ferramenta. Métodos: Estudo longitudinal, com total de 53 vítimas de acidentes atendidas entre abril e outubro de 2010 em uma unidade de reabilitação na capital do Estado de Mato Grosso, Brasil. Os dados da avaliação fisioterápica foram coletados em dois momentos e codificados pela CIF. Resultados: O tempo médio entre a avaliação e a reavaliação foi 73,4 dias. Em relação à evolução das deficiências das funções do corpo observou-se redução no número de pacientes com tais alterações, exceto tônus muscular. Na primeira avaliação 90,6% apresentaram alterações de grau leve a completo quanto às funções sensoriais e dor reduzindo-se para 67,9% na reavaliação, sendo a dor a função mais comprometida. Em re-lação às funções neuromusculoesqueléticas e relacionadas ao movimento a quase totalidade dos pacientes (96,2%) apresentou alguma deficiência na primeira avaliação, percentual reduzido em 15,7% na reavaliação. As maiores reduções deram-se nas categorias: força muscular (36,7%) e padrão da marcha (30,6%). Na reavaliação observou-se diminuição das deficiências relacionadas à estrutura do corpo, especialmente nos níveis de deficiência grave e completa. Conclusão: Com este estudo pode-se comprovar a redução no percentual de pacientes com algum tipo de deficiência física e a evolução positiva no quadro funcional. O uso da CIF permitiu conhecer as deficiências físicas e acompanhar a evolução dos pacientes submetidos a tratamento fisioterápico.
Palavras-chave: Avaliação da Deficiência. Classificação Internacional de Funcionalidade. Incapacidade e Saúde. Acidentes de Trânsito. Reabilitação. Fisioterapia.
Introduction
In the analysis of the health status of a popula -tion, mortality and morbidity indicators are primarily used. However, it is necessary to go beyond the limits of such an analysis to measure the loss of health due to disease and injury. A decline in a healthy and full life often leads to use of the healthcare system (1 - 6).
Traffic accidents are a major global public health problem, responsible for 1.2 million deaths and about 20 to 50 million injuries, of which 10 million are dis -abling and permanent (2, 7). In Brazil, the death rate from traffic accidents has been stable, even with an increase in the number and severity of such accidents (8 - 12). Consequently, the number of survivors has
increased, and therefore the number of disabled in -dividuals (12). The World Health Organization esti -mates that by 2020, road accidents will be the third leading cause of disability, and the leading cause in the productive age group (9 - 10). To put this into per -spective, in the last decade, for each person killed in a traffic accident in Brazil, official statistics recorded about 13 injured (13).
269 after 3 months of follow-up; this period was deter -mined by the need to end the study. In addition, the patients who continued treatment in another unit were reevaluated, and home visits were made to col -lect data. Both the first evaluation and reassessment were carried out by a single researcher with a degree in physical therapy.
Despite undergoing initial evaluation, 15 patients were excluded, because they did not continue treat -ment at the study venue or in any other rehabilitation setting, and 1 patient could not be located for reas -sessment. Thus, the study population was composed of 53 individuals.
A specific form was created to record the func -tional assessment, including anamnesis and physical exam (inspection, pain assessment, palpation, evalua -tion of movement amplitude, sensitivity tests, tests on manual muscle strength, special orthopedic and/or neurological tests). This instrument was previously tested in 5 patients who were starting orthopedic physical therapy. It was possible to verify the appli -cability of the form and standardize data collection procedures. Data from the pilot study were not used in the study results.
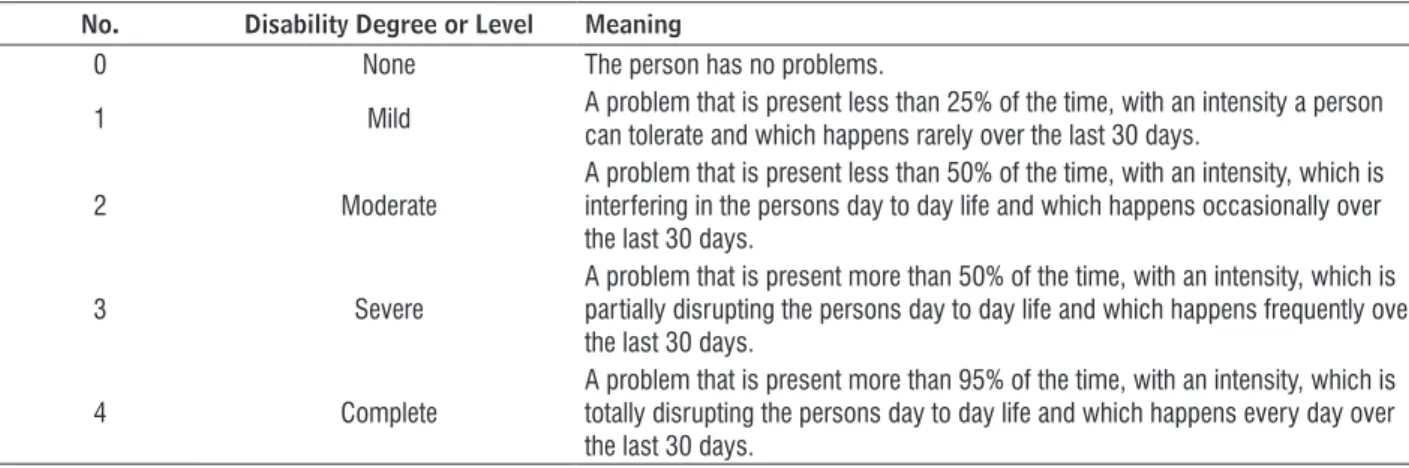
After collection, data were coded according to 2 ICF components (15): a) Body Function and b) Body Structure. Information about other components (Activity/Participation and Environmental Factors) was also collected, but is not included in this study. As the objective was to assess the evolution of disabil -ity, each category was analyzed according to severity level at the time of evaluation and reevaluated. In order to assess the extent (magnitude) of disability for each classification of function and body structure according to the ICF, a qualifier (15) was assigned, as shown in Figure 1.
For the purpose of this study, a disability was con -sidered to be any problem in body function or struc -ture that constitutes a defect, loss, or other impor -tant deviation from normal. Body functions are those related to physiological functions of body systems, whereas body structures are anatomical parts of the body, such as organs, limbs and this components (15).
The research was approved by the Research Ethics Committee of the University Hospital Julio Müller at the Federal University of Mato Grosso, Cuiabá, MT, Brazil, under Approval No. 772/CEP-HUJM/10. All participants gave signed informed consent before starting the evaluation.
health and health-related conditions, as well as their effects and determinant factors, thereby establishing a common language for describing such conditions; this improves communication between users, and provides a systematic coding scheme to be used by health information systems, enabling increased un -derstanding of health and disease issues (15).
According to the World Report on Disability (16), the principles and applications of the ICF also provide an advance in the understanding and measurement of disability. Moreover, the ICF can be used as a mul -tidisciplinary tool to monitor the stages of evolution of disease or health problems.
The use of ICF in the physical therapy area is rec -ognized by several authors (17 - 21); the ICF is even used to establish recommendations for rehabilita -tion, and for functional evalua-tion, planning of thera -peutic intervention, and to evaluate the results (22). However, Escorpizo et al. (20) reported that despite the efforts to implement ICF, there is little evidence of use of this tool by physiotherapists. Due to its com -plexity and scope, there is also little use of the ICF by other health professionals (23). On the other hand, some authors claim that implementation of the ICF by interdisciplinary teams improves the quality of the rehabilitation process (22, 23, 24).
In a recent systematic analysis on the use of ICF in Brazil (25), the authors found few quantitative obser -vational epidemiological studies, and pointed out the lack of follow-up on the population under analysis. This study aims to characterize the evolution of dis -abilities in patients undergoing physical therapy due to traffic accidents, using the ICF.
Methods
An observational longitudinal study was carried out in a reference rehabilitation center for the state of Mato Grosso, aimed at assessing the evolution of physical disabilities in 69 individuals who underwent physiotherapy treatment from April 5 to July 5, 2010, and who had been injured in traffic accidents within 12 months before the start of physical therapy.
No. Disability Degree or Level Meaning
0 None The person has no problems.
1 Mild A problem that is present less than 25% of the time, with an intensity a person can tolerate and which happens rarely over the last 30 days.
2 Moderate
A problem that is present less than 50% of the time, with an intensity, which is interfering in the persons day to day life and which happens occasionally over the last 30 days.
3 Severe
A problem that is present more than 50% of the time, with an intensity, which is partially disrupting the persons day to day life and which happens frequently over the last 30 days.
4 Complete
A problem that is present more than 95% of the time, with an intensity, which is totally disrupting the persons day to day life and which happens every day over the last 30 days.
Figure 1 - Qualifying the extent of disability Note: Adapted from WHO, 2015.
Results
Of the 53 patients whose evolution could be moni -tored, 83.0% (44) were treated at the study venue; most were young (average age = 32 years), male (62.3%), and motorcyclists (66.0%). More than half of the patients had fractures (53.5%), and most injuries involved lower (43.4%) and upper (26.4%) limbs.
The average time between the date of the accident and the first evaluation was 131 days, while the wait -ing time between this evaluation and the reevaluation was 73.4 days (SD = 25.5 days). The minimum time between the 2 evaluations was 7 days and the maxi -mum was 92 days. The classification at the first visit was based on the ICF, making it possible to concur -rently identify deficiencies and disabilities for plan -ning of care.
The body functions classified by ICF in this study were usually sensory functions and pain - b2, and neu
-romusculoskeletal and movement-related functions - b7 (mobility of joint functions, muscle power, muscle
tone, and gait pattern). Body structures evaluated were usually related to movement (head and neck re -gion, shoulder, upper extremity, pelvic re-gion, lower extremity and trunk).
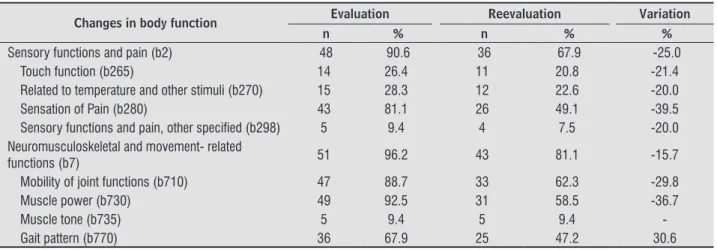
With regard to body function, the ICF enabled assessment of the number of patients with specific changes/problems, except for muscle tone. Table 1 shows that the greatest improvements were in the categories of sensation of pain (39.5%), muscle pow -er (36.7%), and gait patt-ern (30.6%).
With regard to sensory functions and pain (b2), 48
(90.6%) subjects were found to have some initial defi -cits, while at reevaluation the number was reduced to
36 (67.9%), with pain being the function with greater magnitude on both assessments (Table 1).
Among the 43 who initially reported pain, 39.5%
did not report pain in the reevaluation (Table 2). Severe or complete degree of pain was reported by 65.1% on initial evaluation, and decreased to 16.3% on reevaluation, a 75.0% reduction. There was also a migration from patients initially classified with widespread pain to localized pain on reevaluation.
Regarding neuromusculoskeletal and
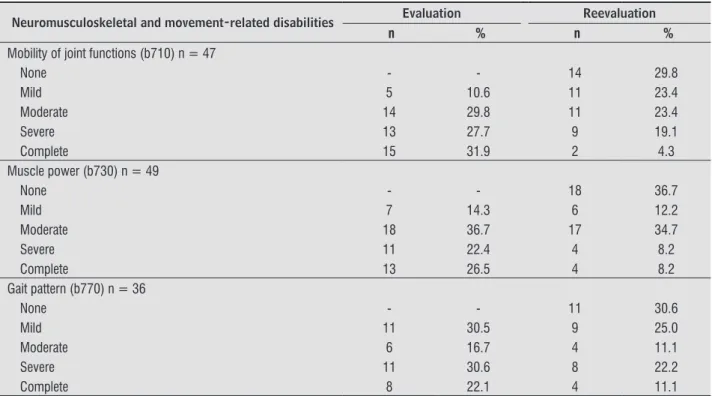
movement-related functions (b7), almost all patients (96.2%) showed some disability on the first evaluation, with a reduction to 15.7% on reevaluation (Table 1). Among those with disabilities related to mobility of joint func
-tions, 59.6% had initial severe or complete disability,
with a decrease to 23.4% on reevaluation (Table 3). Concerning muscle power, the results were the
same as for the remaining components described above, with severe or complete disability on the first evaluation (48.9%) evolving to mild or no disability (48.9%) on reevaluation. It should be noted that the category “no disability”, which was not verified dur -ing the evaluation, contributed to the highest percent -age (36.7%) on reevaluation (Table 3).
Of the 36 patients who presented gait pattern
changes at the beginning of treatment, 25 (69.4%) retained some deficits on reevaluation, with levels of severity (severe or complete) reduced from 52.7% at initial evaluation to 33.3% on reassessment (Table 3).
All patients presented at least one disability of body structure at the initial evaluation, and 10 (18.9%) had no disability when they were reevaluated.
271
Table 1 - Distribution of changes in body function in victims of traffic accidents on initial evaluation and on reevaluation (N = 53). Cuiabá/MT, 2010
Changes in body function Evaluation Reevaluation Variation
n % n % %
Sensory functions and pain (b2) 48 90.6 36 67.9 -25.0
Touch function (b265) 14 26.4 11 20.8 -21.4
Related to temperature and other stimuli (b270) 15 28.3 12 22.6 -20.0
Sensation of Pain (b280) 43 81.1 26 49.1 -39.5
Sensory functions and pain, other speciied (b298) 5 9.4 4 7.5 -20.0 Neuromusculoskeletal and movement- related
functions (b7) 51 96.2 43 81.1 -15.7
Mobility of joint functions (b710) 47 88.7 33 62.3 -29.8
Muscle power (b730) 49 92.5 31 58.5 -36.7
Muscle tone (b735) 5 9.4 5 9.4
-Gait pattern (b770) 36 67.9 25 47.2 30.6
Table 2 - Distribution of the degree of disability related to sensory function and pain in victims of traffic accidents on evaluation and reevaluation. Cuiabá/MT, 2010
Disabilities of sensory function and pain Evaluation Reevaluation
n % n %
Touch function (b265) n = 14
None - - 3 21.4
Mild 5 35.7 5 35.7
Moderate 4 28.6 4 28.6
Severe 1 7.1 2 14.3
Complete 4 28.6 -
-Related to temperature and other stimuli (b270) n = 15
None - - 3 20.0
Mild 5 33.3 5 33.3
Moderate 4 26.7 4 26.7
Severe 1 6.7 3 20.0
Complete 5 33.3 -
-Sensation of pain (b280) n = 43
None - - 17 39.5
Mild 6 14.0 8 18.6
Moderate 9 20.9 11 25.6
Severe 19 44.2 6 14.0
Complete 9 20.9 1 2.3
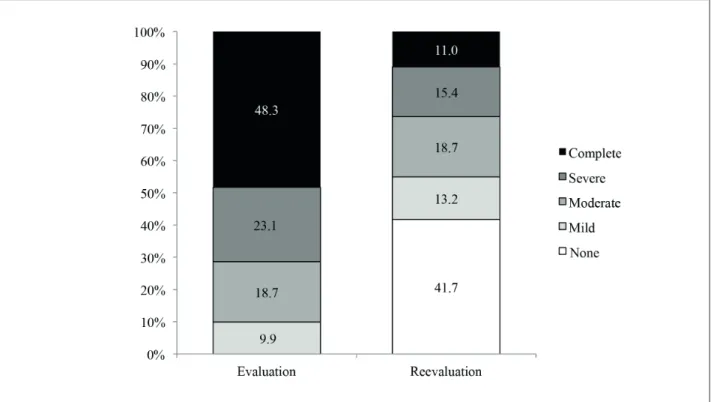
(To be continued) changes in body structure were reduced to 53, which
represents an improvement of 41.8%. Regarding this component, there was a reduction of 63.1% in the severe and complete disability levels, from the time of initial evaluation to that of reevaluation, and a significant percentage (41.7%) had no disability at all (Figure 2).
Structures related to movement (s7)were the most
Table 2 - Distribution of the degree of disability related to sensory function and pain in victims of traffic accidents on evaluation and reevaluation. Cuiabá/MT, 2010
Disabilities of sensory function and pain Evaluation Reevaluation
n % n %
Sensory functions and pain, other speciied (b298) n = 5
None - - 1 20.0
Mild 1 20.0 2 40.0
Moderate 1 20.0 1 20.0
Severe 1 20.0 1 20.0
Complete 2 40.0 -
-Table 3 - Distribution of the degrees of disability related to neuromusculoskeletal and movement-related function in vic-tims of traffic accidents on evaluation and reevaluation. Cuiabá/MT, 2010
Neuromusculoskeletal and movement-related disabilities Evaluation Reevaluation
n % n %
Mobility of joint functions (b710) n = 47
None - - 14 29.8
Mild 5 10.6 11 23.4
Moderate 14 29.8 11 23.4
Severe 13 27.7 9 19.1
Complete 15 31.9 2 4.3
Muscle power (b730) n = 49
None - - 18 36.7
Mild 7 14.3 6 12.2
Moderate 18 36.7 17 34.7
Severe 11 22.4 4 8.2
Complete 13 26.5 4 8.2
Gait pattern (b770) n = 36
None - - 11 30.6
Mild 11 30.5 9 25.0
Moderate 6 16.7 4 11.1
Severe 11 30.6 8 22.2
Complete 8 22.1 4 11.1
Discussion
This study assessed the evolution of disability in patients who had been victims of traffic accidents, at the beginning of treatment and after physical therapy. Changes could be seen in functionality, by using ICF parameters and criteria (15).
Qualifiers that measure the magnitude of dis -ability showed improvement in the health status of patients for both body function and structure. It should be noted that just over half of these patients had not yet completed treatment at the end of the
study. A possible third assessment of this group could lead to even more favorable results.
273 Concerning neuromusculoskeletal and
movement-related functions (b7), the most relevant categories were those of mobility of joint and muscle power, coinciding with the findings of another study (27). It is believed that the high prevalence of changes in mobility of joint functions and muscle power have been mainly due to the immobilization time required for the consolidation of fractures, the most common injuries in the population studied. A more favorable evolution was observed for disabilities related to muscle power, characterized not only by reduction of such disabilities at reevaluation, but also by reduction of the level of severity.
in 3 subcategories: pain sensation, muscle strength, and gait pattern.
Among the sensory and pain-related functions (b2), sensation of pain was predominant, both on initial evaluation and at reevaluation. However, there was a sharp reduction in individuals reporting pain on reevaluation, as well as a migration to lower pain levels, or even to absence of pain.
The improvement in symptoms related to changes in body function observed in this study suggests that these disabilities were mostly temporary, and/or that physical therapy was effective.
Figure 2 - Distribution of disability levels related to body structure in victims of traffic accidents at the time of evaluation and reevaluation (N = 91). Cuiabá/MT, 2010.
In the studied population, injuries and trauma caused by traffic accidents caused complete or seri -ous disabilities in most compromised structures, as observed during the initial evaluation. As stated by the ICF, a severe or complete disability is one that is present more than 50% of the time, with an inten -sity that partially or totally hinders daily life, and is frequently present in the last 30 days (15).
On reevaluation, a decrease in body structure disabilities was recorded, with a significant reduc -tion in the levels of severe and complete disability.
The improvement occurred in all subcategories, es -pecially in movement-related structures.
2. Ministério da Saúde. Secretaria de Vigilância em Saúde. Impacto da violência na saúde dos brasileiros. Brasília: Ministério da Saúde; 2005. Portuguese. 3. Costa JLC. Metodologias e indicadores para avaliação
da capacidade funcional: análise preliminar do Suple -mento Saúde da Pesquisa Nacional por Amostra de Domicílios – PNAD, Brasil, 2003. Cienc Saude Coletiva. 2006;11(4):927-40.
4. Mello Jorge MHP, Koizumi MS. Acidentes de trânsito no Brasil: um atlas de sua distribuição. São Paulo: Associação Brasileira de Medicina de Tráfego; 2007. Portuguese.
5. Ministério da Saúde. Secretaria de Assistência à Saúde. Política Nacional de Saúde da Pessoa Porta -dora de Deficiência. Brasília: Ministério da Saúde; 2008. Portuguese.
6. Soares BAC, Scatena JHG, Galvão ND. Acidentes e vio -lências na Grande Cuiabá: o que retrata a demanda dos serviços de emergência. Epidemiol Serv Saude. 2009;18(3):265-76.
7. Organização Mundial da Saúde. Relatório mundial sobre violência e saúde. Genebra; 2002.
8. Norin H, Krafft M, Korner J, Nygran A, Tingvall C. In -jury severity assessment for car occupants in frontal impacts, using disability scaling. J Clin Epidemiol. 1997;50(1):95103.
9. Mota Jr SC. A mudança da qualidade de vida profis -sional dos politraumatizados vítimas de acidentes de trânsito [final paper]. Maceió (Brazil): Associação Brasileira de Medicina de Tráfego; 1999. Portuguese. 10. Ameratunga SN, Norton RN, Bennett DA, Jackson RT. Risk of disability due to car crashes: a review of the literature and methodological issues. Injury. 2004;35(11):1116-27.
11. Ameratunga SN, Norton RN, Connor JL, Robinson E, Civil I, Coverdale J, et al. A population-based cohort study of long-term changes in health of car driv -ers involved in serious crashes. Ann Emerg Med. 2006;48(6):729-36.
12. Mello Jorge MHP, Koizumi MS. Sequelas visíveis de acidentes de trânsito: primeiros dados brasileiros. Abramet. 2012;29(1):36-45.
in relation to body function or structure, contributes to improvement of activities of daily living.
The present study found that disabilities caused by traffic accidents have distinct characteristics and evolution, such that the same injury may affect func -tional and structural integrity according to the char -acteristics of the individual. In this regard, Almeida (27) states that the ICF is an advance on attempts to understand the needs and specific conditions of per -sons with disabilities, and is a tool that enables evalu -ation of an individual’s multi-directional functionality. Although this study was limited to the analysis of 2 components of the ICF in a very specific population, it proved to be useful in describing the evolution of disabilities in victims of traffic accidents undergoing rehabilitation.
The application of the ICF to health services proved to be feasible and should be encouraged, since it also proved useful as a statistical tool for collect -ing and record-ing data. Therefore, consider-ing the scarcity of epidemiological studies using ICF as a re -search tool, we encourage its use, whether to measure results, quality of life, or other factors.
Conclusion
This study characterized the evolution of disabil -ity in victims of traffic accidents undergoing rehabili -tation by emphasizing the importance of the ICF as a tool for classification and description of a disability and its evolution. As shown by the results, application of the ICF revealed an important reduction of severe and complete levels of disability, and demonstrated a positive and reproducible trend when the ICF com -ponents were analyzed in greater detail.
Use of the ICF brings a new approach to the assess -ment of victims of traffic accidents, thus contributing to the understanding of the functionality process in -herent to a problem that influences the quality of life.
References
275
22. Rentsh HP, Bucher P, Dommen Nyffeler I, Wolf C, Hefti H, Fluri E, et al. The Implementation of the “In -ternational Classification of Functioning, Disability and Health (ICF)” in Daily Practice of Neuroreha -bilitation: an Interdisciplinary Project at the Kan -tonsspital os Lucerne, Switzerland. Disabil Rehabil. 2003;25(8):411-21.
23. Riberto M. Core sets da Classificação Internacional de Funcionalidade, Incapacidade e Saúde. Rev Bras Enferm. 2011;64(5):938-46.
24. Scheuringer M, Stucki G, Huber EO, Brach M, Schwar -zkopf SR, Kostanjsek N, et al. ICF Core Set for pa -tients with musculoskeletal conditions in early post-acute rehabilitation facilities. Disabil Rehabil. 2005;27(7-8):405-10.
25. Castaneda L, Bergmann A, Bahia L. A Classificação In -ternacional de Funcionalidade, Incapacidade e Saúde: uma revisão sistemática de estudos observacionais. Rev Bras Epidemiol. 2014;17(2):437-51.
26. Araújo ES. A Classificação Internacional de Funciona -lidade, Incapacidade e Saúde (CIF) em fisioterapia: uma revisão bibliográfica [master´s thesis]. São Paulo: Faculdade de Saúde Pública da Universidade de São Paulo; 2008. Portuguese.
27. Almeida MCRR. Classificação de Funcionalidade, Incapacidade e Saúde – CIF: aplicação em um hos -pital público [dissertation]. São Paulo: Faculdade de Saúde Pública da Universidade de São Paulo; 2002. Portuguese.
28. Fechio MB, Pacheco KMB, Kaihami HN, Alves VLR. A re -percussão da lesão medular na identificação do su -jeito. Acta Fisiátrica. 2009;16(1):38-42.
29. Jácomo AAE, Garcia ACF. Análise dos acidentes auto -mobilísticos no Centro de Reabilitação Dr. Henrique Santillo (CRER). Acta Fisiátrica. 2011;18(3):124-9. 30. De Carlo MMRP, Elui VMC, Santana CS, Scarpelini S,
Alves ALA, Salim FM. Trauma, reabilitação e quali -dade de vida. Medicina (Ribeirão Preto). 2007; 40(3):335-44.
Received in 10/25/2015
Recebido em 25/10/2015
Approved in 07/07/2016
Aprovado em 07/07/2016
13. Mello Jorge MHP, Koizumi MS. Acidentes de trân -sito no Brasil: um atlas de sua distribuição. São Paulo: Associação Brasileira de Medicina de Tráfego; 2013. Portuguese.
14. Sampaio RF, Luz MT. Funcionalidade e incapacidade humana: explorando o escopo da classificação inter -nacional da Organização Mundial de Saúde. Cad Saude Publica. 2009;25(3):475-83.
15. Organização Mundial da Saúde. Organização Pan Americana da Saúde. Centro Colaborador da Orga -nização Mundial da Saúde para a Família de Classifi -cações Internacionais. CIF: Classificação Internacional de Funcionalidade, Incapacidade e Saúde. São Paulo: Edusp; 2015. 336p. Portuguese.
16. Organização Mundial da Saúde. Relatório Mundial so -bre a Deficiência. São Paulo: SEDPcD; 2012. Portuguese. 17. World Confederation for Physical Therapy (WCPT). 15th WCPT General Meeting; June 4 2003. Barce -lona, Spain.
18. Finger ME, Cieza A, Stoll J, Stucki G, Huber EO. Iden -tification of intervention categories for physical therapy, based on the classification of functioning, disability and health: a Delphi exercise. Phys Ther. 2006;86(9):1203-20.
19. Penney J, MacKay-Lyons MJ, McDonald A. Evidence-Based Stroke Rehabilitation: Case Analysis Us -ing the International Classification of Function-ing, Disability and Health Framework. Physiother Can. 2007;59(1):22-38.
20. Escorpizo R, Stucki G, Cieza A, Davis K, Stumbo T, Riddle DL. Creating an Interface Between the Inter -national Classification of Functioning, Disability and Health and Physical Therapist Practice. Phys Ther. 2010;90(7):1053-63.