w w w . r b o . o r g . b r
Original
Article
Analysis
on
the
serum
levels
of
the
biomarker
CTX-II
in
professional
indoor
soccer
players
over
the
course
of
one
season
夽
Rodrigo
Miziara
Severino
∗,
Pedro
Baches
Jorge,
Mauro
Olivo
Martinelli,
Marcos
Vaz
de
Lima,
Nilson
Roberto
Severino,
Aires
Duarte
Junior
SchoolofMedicalSciences,SantaCasadeSãoPaulo,SãoPaulo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received22February2014 Accepted30June2014 Availableonline16April2015
Keywords: Osteoarthritis Jointcartilage
Pharmacologicalbiomarkers
a
b
s
t
r
a
c
t
Objective:TheaimofthisstudywastoanalyzethebloodserumlevelsofCTX-IIin profes-sionalindoorsoccerplayers,atthreedifferenttimesduringoneseason:atthestartofthe pre-season,fourmonthslater(atimethatmarksthemiddleoftheseason)andattheend oftheseason.
Methods:Fourteenmalesoccerplayersofmeanage19yearswereincluded.Bloodsamples of3mLwerecollectedfromeachindividual.ThesampleswereanalyzedbymeansofElisa tests.
Results:TherewasasignificantincreaseintheserumlevelofCTX-IIintheindoorsoccer players,fromthebeginningtotheendoftheseason(p<0.01).
Conclusion: Thesedatasuggestthatjointdegradationhadoccurredinthesesoccerplayers, bytheendofthisperiod.Itisevidentthatfurtherstudiesareneeded,withmethodological rigor,soastomakeaneffectivecontributiontowardpreciseelucidationoftheetiologyof thisosteoarthritisanditsrelationshipwiththebiomarkers,asatoolforearlydiagnosis.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
Análise
dos
níveis
séricos
do
biomarcador
CTX-II
em
atletas
profissionais
de
futebol
de
salão
durante
uma
temporada
Palavras-chave: Osteoartrite Cartilagemarticular
Biomarcadoresfarmacológicos
r
e
s
u
m
o
Objetivo:AnalisarosníveisséricossanguíneosdeCTX-IIematletasprofissionaisdefutebol desalão,emtrêsmomentosdistintosduranteumatemporada:noiníciodapré-temporada, quatromesesapós(períodoquemarcaomeiodatemporada)enofimdatemporada. Métodos:Foramincluídos14atletasdogêneromasculinoemédiadeidadede19anos.Foram coletados3mLdesanguedecadaindivíduo.Asamostrasforamanalisadaspelotestedotipo Elisa.
夽
WorkdevelopedintheDepartmentofOrthopedicsandTraumatology,SantaCasadeSãoPaulo,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](R.M.Severino). http://dx.doi.org/10.1016/j.rboe.2015.04.001
Resultados: HouveaumentosignificativodosníveisséricosdeCTX-IInosatletasdefutebol desalão,comparando-seoinícioeofimdeumatemporada(p<0.01).
Conclusão:Essesdadossugeremaocorrênciadedegradac¸ãoarticularnosatletas,aotérmino desseperíodo.Ficaevidenteanecessidadedefuturosestudos,comrigormetodológico,que possamcontribuirefetivamenteparaaelucidac¸ãoprecisadaetiologiadaOAesuarelac¸ão comosbiomarcadorescomoinstrumentodediagnósticoprecoce.
©2014SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Primaryosteoarthritis(OA)isamultifactorialdisease charac-terizedbyirreversiblejointdegeneration,withformationof osteophytesandreductionofthejointspace.Itpresentsthe followingmainsymptoms:progressiveincreaseinpain,lossof function,limitationsonday-to-dayactivitiesandrestrictions onsportspractice.1–7
Sometheorieshavecorrelatedcontinualintensepractice ofphysicalactivitywithdevelopmentofprimaryOAinelite athletes,causedbyjointoverloading.Moreover,therehasbeen speculationregardinghowthejointcartilagerespondstothis overloading.However,therelationshipbetweenjointcartilage damageandintensephysicalactivitystillseemstobeamatter ofcontroversyintheliterature.8,9
Some studies have demonstrated that athletes who practicesportsthat includerapidaccelerationwithinstant decelerationor continuous training witha high impacton joints,orwhocompeteatelitelevelforprolongedperiodsof time,presentgreaterlikelihood ofdevelopingOA.However, thetypesandintensitiesofexercisesthatareharmfultojoint cartilageremainunknown.8–11
OA presents aninitial asymptomatic phase,which may beinfluencedbythelevelofoverloadingtowhichthejoint is exposed in a physical activity. However, identification of this joint damage is difficult, given the limitations of the assessment instruments available. In this light, recent studies have demonstrated that biochemical biomarkers are a potentialoption forearly detection ofasymptomatic OA.9,12,13
Underphysiologicalconditions,themetabolismoftypeII collagenisslow.Itsfibrilshaveahalf-lifemeasuredinyears. Intheinitialstagesofcartilagedegeneration,degradationof thesecollagenfibrilsisobserved.Enzymesnamed metallo-proteinases are released, and thesecontribute toward this degradation,especiallycollagenases andaggrecanases. Col-lagenases are responsible forcleaving type IIcollagen and produce fragmentsof this collagen. Specificantibodies for thesefragmentscanbedetectedinsynovialfluid, bloodor urineandhavebeenstudiedaspotentialbiomarkersforthe onsetofjointdegradation.2,5,7
Whenajointcomponentisdegradedandejectedoutofits originaltissue,measuringthisinthejointfluidwouldbethe mostprecisemethod.Onebiomarkerofjointdegradationis theC-telopeptideoftypeIIcollagen(CTX-II).UseofCTX-IIas amarkerforprogressionofcartilaginouslesionsanditsdirect relationshipwithradiologicalgradesandclinical scoresfor OAhavebeenprovenintheliterature.Therefore,assayingof
CTX-IIlevelsseemstobeaneffectivemannerforascertaining typeIIcollagenturnover.14–21
Biomarkersareinstrumentsformeasuringtheprogression ofdiseases or the effectsoftreatment ondisease progres-sion.Thus,theycanserveastoolsforelucidatingtheeffects ofexerciseonjointcartilage andthepossibledevelopment ofprimaryOA.12,13Inthislight,theobjectiveofthepresent studywastoanalyzeandcomparebloodserumassaylevels ofthebiomarkerCTX-IIinprofessionalindoorsoccerplayers, atthreedifferenttimesduringoneseason.
Methods
Thiswasaprospectivelongitudinalstudythatwasapproved bytheResearchEthicsCommitteeofSantaCasade Misericór-diadeSãoPaulo.
Thestudyincluded14playersinaprofessionalindoor soc-certeam(under-21category).Theplayersweremale,ofmean age19years,allinthesameteam,andweresubjectedtothe sametrainingandmatchload.
Players withpreviousknee surgery(twoplayers)or who were using chondroprotectant medications (three players) wereexcluded.
In addition, four players who were undergoing physio-therapytreatmentforfemoropatellaroverloadduetomuscle imbalanceinthepelvicbeltwereexcludedbecausethey pre-sentedpainofpatellaroriginthatlimitedtheirsportspractice atthebeginningoftheseason.
CTX-IIlevelswereassayedatthreetimes:A–atthe begin-ning ofthe pre-season; B–four months later(atime that markedthemiddleoftheseason);andC–attheendofthe season.
Bloodsamples(3mL)werecollectedfromeachindividual bymeansofsimplepunctureinthenon-dominantarm,using vacuumcollectionkits.Thebloodsampleswerecentrifuged andstoredatatemperatureof−80degrees,untilallthe sam-pleswerereadytobetested.
EachsamplewasanalyzedbymeansofanELISAtestfor detectinghumanCTX-II(HuCTX-IIkit,CusabioBiotech, cata-lognumberCSB–E09323h,batchS20045731,producedinthe UnitedStates).Thiskitpresents100%specificityforhuman CTX-IIalone,withoutcross-reactions,andwithaminimum detectable leveloflowerthan 0.3ng/mL. Thistestwas per-formedinaprivatelaboratoryinthecityofSãoPaulo,with costsentirelybornebytheresearchers.
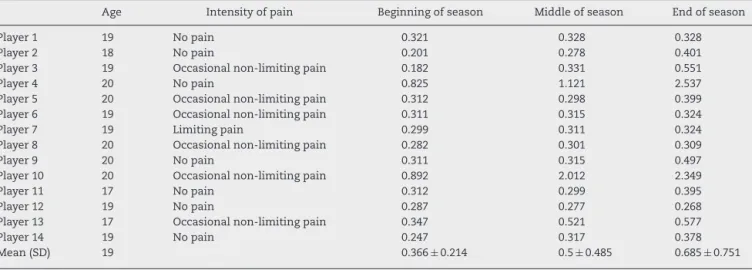
Table1–DataonindividualsandtheirCTX-IIassaylevels(inng/mL),observedforeachplayerateachtimeduringthe season.
Age Intensityofpain Beginningofseason Middleofseason Endofseason
Player1 19 Nopain 0.321 0.328 0.328
Player2 18 Nopain 0.201 0.278 0.401
Player3 19 Occasionalnon-limitingpain 0.182 0.331 0.551
Player4 20 Nopain 0.825 1.121 2.537
Player5 20 Occasionalnon-limitingpain 0.312 0.298 0.399 Player6 19 Occasionalnon-limitingpain 0.311 0.315 0.324
Player7 19 Limitingpain 0.299 0.311 0.324
Player8 20 Occasionalnon-limitingpain 0.282 0.301 0.309
Player9 20 Nopain 0.311 0.315 0.497
Player10 20 Occasionalnon-limitingpain 0.892 2.012 2.349
Player11 17 Nopain 0.312 0.299 0.395
Player12 19 Nopain 0.287 0.277 0.268
Player13 17 Occasionalnon-limitingpain 0.347 0.521 0.577
Player14 19 Nopain 0.247 0.317 0.378
Mean(SD) 19 0.366±0.214 0.5±0.485 0.685±0.751
applied(95%confidenceintervalandpvalue<0.05).This non-parametrictestwasthebestoptionbecauseitwasimpossible toassumethatthesamplehadnormaldistribution.
Results
Table1presentsthedataoneachindividualandthemarker levelsobservedforeachofthemateachtimeduringthe sea-son.Itcouldbeseenthat twoplayers(4and 10)presented discrepantdata,withmuchhigherassayedlevelsthanthoseof theotherplayersevaluatedinthisstudy,inalltheevaluations. Nevertheless,theseparticipantsdidnotreportanydeclinein physicalperformance,oranypresenceofsymptomssuchas pain,edemaorinstability.
Individuals3, 5and 10 presented pain at the origin of the patellar tendon in one knee, which became worse at the end ofthe sports practice, improved with physiother-apy and did not limit their participation in training and matches.Individual13presentedaconditionofnon-limiting painabovetheinsertionofthepesanserinus.Also, individ-uals6and8complainedoflateralpainintheirknees,above thelateralepicondyle,duringsportspractice,whichwasalso non-limiting.
Becauseofthetendinousoriginofthepaininthe individ-ualsincludedinthis study(patellartendinopathy,anserine tendinopathyandfrictionoftheiliotibialtract),itwasdecided not to include them separately in statistical comparisons regardingdegradationoftypeII collagenexclusivelyofthe cartilaginoustissue.
ComparisonofCTX-IIassaylevelsbetweendifferenttimes duringtheseason
Becauseofthelimitedsizeofthesample,whichwasselected in a non-randomized manner because this was a closed indoorsoccerteam, thedistribution oftheindividuals and resultsfromthesamplecannotbeconsideredtobenormal. Whenthisoccurs,nonparametricstatisticaltestsneedtobe used.In thegraphicdistribution ofthe data, two individu-alshad values that were very different from those of the
remainderoftheteamandwhichwereconsideredtobe out-liers.
Toavoidtheriskofstatisticalerror,twoseparateanalyses wereperformed:1–comparisonsusingthecompletedata;and 2–comparisonsusingreduceddata(withouttheinformation onplayers4and10)(Table2).
Incomparingthe valuesfrom thefirsttwoanalyses,i.e. beginningoftheseasonversusmiddleoftheseason,no sta-tisticallysignificantdifferencesbetweenthesamplescouldbe seen,ineitherofthecomparisons(1and2).
In the analysisbetween the middle and the endof the season,therewasasignificantdifferenceinassayedlevels, inthecomparisonamongthe14participants(p<0.02). How-ever,whenplayers4and10weretakenoutoftheanalysis, nosignificantdifferencecouldbeseen(analysiswithreduced data).
Incomparingthebeginningandendoftheseason,both analyses(comparisons1and2)indicatedthattherewasa sta-tisticallysignificantincreaseintheCTX-IIbiomarker(p<0.003 andp<0.01,respectively).Inotherwords,betweenthe begin-ningandtheendoftheseason,therewasasignificantincrease inthe levelofthe CTX-IIjoint degradationbiomarker, irre-spective of whether the extreme results were taken into consideration.
Table2–Comparisonofassayedlevelsforthe biomarkerCTX-II(inng/mL)observedbetweenthe differenttimesduringtheseason.Completedata(14 players)andreduceddata(12players:players4and10 weredisregarded).
Comparison Meandifference p
Completedata
Beginningvs.middle 0.134 0.06 Middlevs.end 0.186 0.02 Beginningvs.end 0.320 0.003
Reduceddata
Discussion
Thisstudyaimedtoanalyzeandcomparebloodserumassay levelsforthebiomarkerCTX-IIamongprofessionalindoor soc-cerplayers,atthreedifferenttimesduringoneseason.From theresultsobserved,itcouldbeseenthattherewasa statis-ticallysignificantincreaseinCTX-II betweenthebeginning and endofthe season.Ithasbeen well establishedinthe literaturethatincreasedlevelsofthebiomarkerCTX-IIarea predictivefactorforjointdegradation.Thus,itisbelievedthat earlyidentificationofCTX-IIlevelswouldbeausefultoolfor makingequallyearlydiagnosesofprimaryosteoarthritis(OA) andtakingpreventiveaction.22,23
Corroborating the findings ofthe present study,O’Kane etal.22evaluateddifferentsportscategoriesanddemonstrated through urine analyses that samples from marathon run-nerspresentedhigherCTX-IIlevelsthanthoseofswimmers orrowers.Accordingtotheseauthors,runnersexposetheir lower-limbjointstorepetitiveaxialoverloading,whichmay causeearlydamagetotheirjointcartilage.
The pure and simple increase in CTX-II in the players studiedhere does not necessarilymean that theyare suf-feringorwillsufferosteoarthrosis.Itisknownthatpatients witharthrosishavehighlevelsofthisserumbiomarkerand increasedlevelsaredirectlyrelatedtoradiographicworsening, accordingtotheKelgreen-Laurenceclassification.16Whatwe canbesureoffromthesedataisthat,atleastduring competi-tions,chondraldegradationwashigherinthepatientsstudied, sincethebiomarkerCTX-IIcomesfromdestructionoftypeII collagen,exclusivelyinjointcartilage.
Itispossiblethat changes totraining, intensificationof anaerobicexerciseswithmusclestrengthening,compulsory physiotherapeuticfollow-upandevenuseof chondroprotec-tantmedicationsmightbeviablesolutionsforjointprotection. Inordertoprotectthejointhealthofsoccerplayers,teams shouldstarttothinkaboutthistypeofpreventivestrategy.
After all, the aim today should be prevention before treatment. Injury avoidance through practicing preventive medicineshouldbethefocusofexerciseandsportsmedicine, sincecareerscancertainlybeprolongedinthismanner.
Thepossiblelimitationsofthisstudyarethesmallsample size(n=14)andtheabsenceofacontrolgroupforcomparisons betweenfindings.Thesamplesizeisexplainedbythefact thatthisstudyinvestigatedasingleteamwithinthiscategory, whosememberswereallsubjectedtothesametrainingand competitionloads.Itwasdecidednottouseacontrolgroup, becauseouraimwasonlytoascertainwhethertherewould beanyincreaseinjointcollagendegradationoverthecourse ofasingleseasonoftrainingandcompetition.Inotherwords, theindividualsbecametheirowncontrols.
OtherstudiesunderwaywithintheSportsTraumaGroup ofSantaCasadeSãoPauloarecomparingtypesofsportsand controlgroups, includingindoorsoccer.Preliminarystudies indicatethattherearelargedifferencesregardingtypeII col-lagendegradation.
Thediscrepanciesencounteredinoursample,intwoof the individuals analyzed, can be explainedby avariety of theories. These include the notionsthat the markers may havebeeninfluencedbytheindividuals’hormonalstate,diet
or geneticfactors,22 giventhat neitherofthese individuals reportedanyreductioninphysicalperformance,orany symp-tomssuchaspain, edemaorinstability. AccordingtoDam etal.,24theamountofcartilagedegradationestimatedfrom thebiomarkerCTX-IIisrelatedtothepresenceofpain.
Conclusion
Therewasasignificantincreaseintheserumlevelsof CTX-IIintheindoorsoccerplayers,comparingthebeginningand endoftheseason.Thesedatasuggestthatincreased degra-dationoftypeIIjointcollagenwasoccurringattheendof this period.Itisclearthatfurtherstudiesareneeded,with appropriatemethodologicalrigor,soastomakeeffective con-tributionstowardpreciseelucidationoftheetiologyofOAand itsrelationshipwithbiomarkersasatoolforearlydiagnosis.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
r
e
f
e
r
e
n
c
e
s
1.AnderssonML,ThorstenssonCA,RoosEM,PeterssonIF, HeinegårdD,SaxneT.Serumlevelsofcartilageoligomeric matrixprotein(COMP)increasetemporarilyafterphysical exerciseinpatientswithkneeosteoarthritis.BMC MusculoskeletDisord.2006;7:98.
2.BruyereO,ColletteJH,EthgenO,RovatiLC,GiacovelliG, HenrotinYE,etal.Biochemicalmarkersofboneandcartilage remodelinginpredictionoflongtermprogressionofknee osteoarthritis.JRheumatol.2003;30(5):1043–50.
3.DiCesareP,HauserN,LehmanD,PasumartiS,PaulssonM. Cartilageoligomericmatrixprotein(COMP)isanabundant componentoftendon.FEBSLett.1994;354(2):237–40. 4.FernandesFA,PucinelliML,daSilvaNP,FeldmanD.Serum
cartilageoligomericmatrixprotein(COMP)levelsinknee osteoarthritisinaBrazilianpopulation:clinicaland
radiologicalcorrelation.ScandJRheumatol.2007;36(3):211–5. 5.GarneroP,DelmasPD.Biomarkersinosteoarthritis.CurrOpin
Rheumatol.2003;15(5):641–6.
6.TsengS,ReddiAH,DiCesarePE.Cartilageoligomericmatrix protein(COMP):abiomarkerofarthritis.BiomarkInsights. 2009;4:33–44.
7.VilímV,VytásekR,OlejárováM,MachácekS,GatterováJ, ProcházkaB,etal.Serumcartilageoligomericmatrixprotein reflectsthepresenceofclinicallydiagnosedsynovitisin patientswithkneeosteoarthritis.OsteoarthrCartil. 2001;9(7):612–8.
8.BuckwalterJA,LaneNE.Athleticsandosteoarthritis.AmJ SportsMed.1997;25(6):873–81.
9.KujalaUM,KaprioJ,SarnaS.Osteoarthritisofweightbearing jointsoflowerlimbsinformerelitemaleathletes.BrMedJ. 1994;308(6923):231–4.
10.PatraD,SandellLJ.Recentadvancesinbiomarkersin osteoarthritis.CurrOpinRheumatol.2011;23(5):465–70. 11.SaxonL,FinchC,BassS.Sportsparticipation,sportsinjuries
andosteoarthritis:implicationsforprevention.SportsMed. 1999;28(2):123–35.
13.NeidhartM,Müller-LadnerU,FreyW,BosserhoffAK,
ColombaniPC,Frey-RindovaP,etal.Increasedserumlevelsof non-collagenousmatrixproteins(cartilageoligomericmatrix proteinandmelanomainhibitoryactivity)inmarathon runners.OsteoarthrCartilage.2000;8(3):222–9.
14.HuebnerJL,KrausVB.Assessmentoftheutilityofbiomarkers ofosteoarthritisintheguineapig.OsteoarthrCartilage. 2006;14(9):923–30.
15.MazièresB,GarneroP,GuéguenA,AbbalM,BerdahL, LequesneM,etal.Molecularmarkersofcartilagebreakdown andsynovitisatbaselineaspredictorsofstructural
progressionofhiposteoarthritis.TheECHODIAHCohortAnn RheumDis.2006;65(3):354–9.
16.BruyereO,ColletteJ,KothariM,ZaimS,WhiteD,GenantH, etal.Osteoarthritis,magneticresonanceimaging,and biochemicalmarkers:aoneyearprospectivestudy.Ann RheumDis.2006;65(8):1050–4.
17.DamEB,LoogM,ChristiansenC,ByrjalsenI,FolkessonJ, NielsenM,etal.Identificationofprogressorsinosteoarthritis bycombiningbiochemicalandMRI-basedmarkers.Arthritis ResTher.2009;11(4):R115.
18.FelsonDT,LohmanderLS.Whitherosteoarthritisbiomarkers? OsteoarthrCartilage.2009;17(4):419–22.
19.SowersMF,Karvonen-GutierrezCA,YosefM,JannauschM, JiangY,GarneroP,etal.LongitudinalchangesofserumCOMP
andurinaryCTX-IIpredictX-raydefinedkneeosteoarthritis severityandstiffnessinwomen.OsteoarthrCartilage. 2009;17(12):1609–14.
20.KarsdalMA,ByrjalsenI,Bay-JensenAC,HenriksenK,RiisBJ, ChristiansenC.Biochemicalmarkersidentifyinfluenceson boneandcartilagedegradationinosteoarthritis–theeffectof sexKellgren-Lawrence(KL)score,bodymassindex(BMI),oral salmoncalcitonin(sCT)treatmentanddiurnalvariation.BMC MusculoskeletDisord.2010;11:125.
21.IshijimaM,WatariT,NaitoK,KanekoH,FutamiI,
Yoshimura-IshidaK,etal.Relationshipsbetweenbiomarkers ofcartilage,bone,synovialmetabolismandkneepainprovide insightsintotheoriginsofpaininearlykneeosteoarthritis. ArthritisResTher.2011;13(1):R22.
22.O’KaneJW,HutchinsonE,AtleyLM,EyreDR.Sport-related differencesinbiomarkersofboneresorptionandcartilage degradationinenduranceathletes.OsteoarthrCartilage. 2006;14(1):71–6.
23.AtturM,Krasnokutsky-SamuelsS,SamuelsJ,AbramsonSB. Prognosticbiomarkersinosteoarthritis.CurrOpin
Rheumatol.2013;25(1):136–44.