www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
The
role
of
Onodi
cells
in
sphenoiditis:
results
of
multiplanar
reconstruction
of
computed
tomography
scanning
夽
,
夽夽
Mehmet
Senturk
a,
Ibrahim
Guler
b,∗,
Isa
Azgin
a,
Engin
Umut
Sakarya
a,
Gultekin
Ovet
a,
Necat
Alatas
a,
Ismet
Tolu
c,
Omer
Erdur
daKonyaEducationandResearchHospital,DepartmentofOtolaryngology,Head,andNeckSurgery,Konya,Turkey bMedicalFaculty,Selc¸ukUniversity,DepartmentofRadiology,Konya,Turkey
cKonyaEducationandResearchHospital,DepartmentofRadiology,Konya,Turkey
dMedicalFaculty,Selc¸ukUniversity,DepartmentofOtolaryngology,Head,andNeckSurgery,Konya,Turkey
Received26August2015;accepted25January2016 Availableonline20April2016
KEYWORDS Anatomicvariation; Computed
tomography; Onodicell; Sphenoiditis
Abstract
Introduction:Onodicellsarethemostposteriorethmoidaircellsandextendsuperolateralto
thesphenoidsinus.Thesecellsarealsointimatelyrelatedwiththesphenoidsinus,opticnerve,
andcarotidartery.Radiologicevaluationismandatorytoassessforanatomicvariationsbefore
anytreatmentmodalitiesrelatedtothesphenoidsinus.
Objective:ToevaluatetheeffectofOnodicellsonthefrequencyofsphenoiditis.
Methods:Aretrospectiveanalysiswasperformedin618adult patientswhounderwent
high-resolutioncomputedtomographybetweenJanuary2013andJanuary2015.Theprevalenceof
Onodicellsandsphenoiditiswasevaluated.WhetherthepresenceofOnodicellsleadstoan
increaseintheprevalenceofsphenoiditiswasinvestigated.
Results:Onodicellpositivitywasobservedin326of618patientsanditsprevalencewasfound
tobe52.7%.Inthestudygroup,60.3%(n=73)wereipsilaterally(n=21)orbilaterally(n=52)
Onodi-positive, whereas 39.7% (n=48) were Onodi-negative (n=35) or only contralaterally
Onodi-positive(n=13).Ofthe controlgroup,48.3%(n=240)wereOnodi-positive and51.7%
(n=257)were Onodinegative.The co-existenceofOnodicellsipsilaterally wasobservedto
increasetheidentificationofsphenoiditis1.5-fold,andthisfindingwasstatisticallysignificant
(p<0.05).
夽
Pleasecitethisarticleas:SenturkM,GulerI,AzginI,SakaryaEU,OvetG,AlatasN,etal.TheroleofOnodicellsinsphenoiditis:results ofmultiplanarreconstructionofcomputedtomographyscanning.BrazJOtorhinolaryngol.2017;83:88---93.
夽夽
Thismanuscriptwaspresentedasoralpresentationatthe11thTurkishNationalRhinologyCongress,Antalya,April16---19,2015.The protocolofthisstudywasapprovedbytheinstitutionalreviewboardoftheMedicalFacultyofMeram,UniversityofNecmettinErbakan, Konya.
∗Correspondingauthor.
E-mail:[email protected](I.Guler).
PeerReviewundertheresponsibilityofAssociac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial.
http://dx.doi.org/10.1016/j.bjorl.2016.01.011
Conclusion: TheprevalenceofsphenoiditisappearstobehigherinpatientswithOnodicells.
However,itisnotpossibletostatethatOnodicellsarethesinglefactorthatcausesthisdisease.
Furtherstudiesareneededtoinvestigatecontributingfactorsrelatedtosphenoiditis.
© 2016 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Published
by Elsevier Editora Ltda. This is an open access article under the CC BY license (http://
creativecommons.org/licenses/by/4.0/).
PALAVRAS-CHAVE Variac¸ãoanatômica; Tomografia
computadorizada; CéluladeOnodi; Esfenoidite
PapeldascélulasdeOnodinaesfenoidite:resultadosdatomografiacomputadorizada comreconstruc¸ãomultiplanar
Resumo
Introduc¸ão: AscélulasdeOnodisãoascélulasetmoidaismaisposteriores,queseprolongam
superolateralmenteaoseioesfenoidal.Essascélulastambémseencontramemíntimarelac¸ão
comoseioesfenoidal,onervoópticoeaartériacarótida.Paraanálisedevariac¸õesanatômicas
antesdaimplementac¸ãodequalquermodalidadeterapêuticarelacionadaaoseioesfenoidal,
aavaliac¸ãoradiológicaéobrigatória,
Objetivo: NossoobjetivofoiavaliaropapeldascélulasdeOnodinafrequênciadeesfenoidite.
Método: Emnossoestudo,foirealizadaumaanáliseretrospectivaem 618pacientesadultos
quesesubmeteramàtomografiacomputadorizadadealtaresoluc¸ãoentrejaneirode2013e
janeirode2015.AvaliamosaprevalênciadecélulasdeOnodiedeesfenoidite.Investigamosse
apresenc¸adecélulasdeOnodilevaaumaumentonaprevalênciadeesfenoidite.
Resultados: A positividadeparacélulas deOnodi foiobservadaem326 de618pacientes,e
suaprevalênciafoide52,7%.Nogrupodeestudo,60,3%(n=73)eramCO-positivas:ipsilateral
(n=21)oubilateralmente(n=52);e39,7%(n=48)eramCO-negativas(n=35)ouapenas
con-tralateralmenteCO-positivas(n=13).Nogrupodecontrole,48,3%(n=240)eramCO-positivas;
e51,7%(n=257)eramCO-negativas.ObservamosqueacoexistênciadeCOipsilateralmente
aumentava em 1,5vezes a associac¸ãocom esfenoidite, eesse achado foi estatisticamente
significante(p<0,05).
Conclusão:AprevalênciadeesfenoiditeparecesermaiorempacientescomcélulasdeOnodi,
mas nãoépossívelafirmarqueelassãoisoladamenteofator causadordestadoenc¸a.Novos
estudosprecisamserrealizadosparaumainvestigac¸ãodosfatorescontributivosrelacionados
àesfenoidite.
© 2016 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Publicado
por Elsevier Editora Ltda. Este ´e um artigo Open Access sob uma licenc¸a CC BY (http://
creativecommons.org/licenses/by/4.0/).
Introduction
TheOnodicell(OC)isdefinedasthemostposteriorethmoid cell,andmayextendtothesphenoidsinus(SS)superiorly and laterally. The importance of these cells comes from theircloserelationshipwiththeopticnerve(ON),SS,and hypophysealfossa.1Nomuraetal.2statedthatOCsdisplace
theSSdownward,reducingitsvolume,andthereforecould be associated with sphenoiditis. Ozturan etal.3 reported
thattheco-existenceof theOCmayalterthe morpholog-icalchangesinthefloorand/orthelateralwalloftheSS. Inaddition,itwasmentionedthatpooraerationand ineffi-cientdrainageoftheOCleadtostasisofsecretions,causing recurrent infectionsin mucoceles, opticneuritis,or optic neuropathies.4---6
Identification of OCsis possible using computed tomo-graphy(CT)scanning.Itis necessary toexamineallthree dimensions (axial, coronal, and sagittal) meticulously to identifyOCs. The accurateprevalence ofOCsis notclear becauseCTscanstudiesoftheprevalenceofOCsinadults haveproducedvariedresults,rangingfrom7%to65%.1,3,7---9
AlthoughtherearestudiesontheprevalenceofOCsinadult
patients, it was not possible to finda study on the rela-tionshipbetweenthisanatomicalvariationandsphenoiditis. TheonlystudyfoundinPubMedwasthatconductedbyKim etal.10 withachildpopulation,whichreportedthat
sphe-noidsinusitisinchildrenisnotassociatedwiththepresence of OCs. Moreover, since developmentof the SS continues until the end of childhood,11,12 a study on the
relation-shipbetweenthepresenceofOCsandsphenoiditisinadult patients will probably yield more reliable results than a studyconductedwithchildren.
In this study, the aim was to investigate whether the presenceofOCscausesanincreaseinthefrequencyof sphe-noiditisbyanalyzingthin-slicemultiplanar(axial,coronal, andsagittal)reconstructedhigh-resolutioncomputed tomo-graphy(HRCT)inadultpatientswithOCs,aswellasgender andageprofiles.
Methods
obstruction), had clinical findings (inflammatory findings wereobservedandconfirmedwithnasalendoscopic exam-ination) of chronic sinus disease (not for allergic rhinitis orrecurrentacutesinusitis),andhadundergone paranasal sinus computed tomography (HRCT) in the Konya Educa-tion and Research Hospital between January 2013 and January 2015 were included in the study. Also, review-ing the patients’ records, those who had any history of trauma, nasal polyp, cysticfibrosis, asthma, immunosup-pressivedisease,malignancy,anopacificationresemblinga massradiologicallyorahistoryofpreviousendoscopicsinus surgery,aswellaspatientswithcongenitalmalformations, wereexcludedfromthestudy.Theprotocolofthisstudywas approvedbythe institutionalreview board oftheMedical FacultyofMeram,NecmettinErbakanUniversity,Konya.
In the Radiology Clinic,the routine CT imaging proce-durestepsweredefinedasfollows:scanswereperformed witha128-slicemultidetectorcomputedtomographic scan-ner(IngenuityCT,PhilipsHealthcare,Andover,MA).Imaging parameters were as follows: Kv=120; mA=160; rotation
time=0.5s; collimation=64×0.625; FOV=220mm. The
iterativereconstructiontechniquewasemployedtoreduce radiation dose during scans. Axial images were recorded whilethepatientwasinthesupinepositionandtheheadwas inaneutralposition.Theimagescoveredtheareafromthe apexofthefrontalsinuses tothenasalmaxillaryprocess, paralleltothehardpalate.AxialCTimageswereobtained with a section thickening of 0.625mm, and these source data were used to obtain associated coronal and sagittal imageswith0.9-mmslicethickness.Imageswereanalyzed onaworkstation (IntelliSpacePortal;PhilipsHealthcare ---Andover,MA, UnitedStates).Nopatientunderwentanew CTexaminationforthisstudy.Theretrospectiveanalysiswas performed usingCTimagesrecordedin thedigitalarchive oftheRadiologyClinic.
InpatientswhounderwentanHRCTexamination,theOC wasdefinedasthemostposteriorethmoidalaircell, extend-ingsuperolaterallytothesphenoidsinus.Afterapplication of additionalradiologicalcriteria, suchasCTscanquality and technicaladequacy, bytwo independentobservers (a
radiologistandanotolaryngologist),663resultsofCTscans wereexamined. TheOCsweredeterminedby axial, coro-nal, and sagittal multiplanar HRCT scans. Identified OCs weredividedasfollows:(i)negativeOCfindings;(ii) right-sidedOCfindings;(iii)left-sidedOCfindings;(iv)bilateral OC findings. This study used the definition of sphenoidi-tis as the presence of mucosal thickening greater than 2mm, as described by Gliklich and Metson.13 The
sphe-noiditis identified on CT were classified as follows: (a) negativesphenoiditis;(b)right-sidedsphenoiditis;(c) left-sidedsphenoiditis;(d)bilateralsphenoiditis.Whilethestudy groupwasconsistedof sphenoiditis-positivepatients, con-trolgroupwasconsistedofsphenoiditis-negative patients. In the study group, Onodi-positive patients consisted of sphenoiditis-positiveplusipsilateralorbilateralOC-positive patients.Sincethepresenceofunilateral Onodicellisnot expected to affect contralateral sphenoid sinus anatomi-cally,itwasconsideredthatthepresenceofunilateralOnodi cellsisnotsuitabletobeinassociationwithcontralateral sphenoidsinusitis.Thus,thepatientswithsphenoiditisplus onlycontralateral Onodicellpositivitywerealsoincluded intotheOC-negativepatientsinstudygroup.The frequen-cies of sphenoiditis in OC-positive and negative patients werecalculatedconsideringgenderandage.
Statisticalmethods
Univariate and multivariate logistic regression analyses wereperformedwithforwardlogisticregressionanalysisto identifyfactorslinkedwithOCsandsphenoiditis.OC, sphe-noid sinusitis,gender, and ageswere chosen as predictor variables.Thecategorizeddatawereevaluatedbythe chi-squaredtest.Student’st-testfor paired-sampleswasused tocomparethesameparameterswithnormaldistribution.A p-valueof0.05orlessindicatesastatisticallysignificant dif-ference.TheanalyseswereperformedusingSPSSStatistics v.21,(IBM®---NewYork,UnitedStates).
Results
Six-hundredandeighteenpatientsmeetingthestudy crite-ria were included; 353 were male (57.1%) and 265 were female(42.9%).Themeanagewas36.4years(range18---87 years;median=34years).Themeanageoffemaleswas37.8 years,andthemeanageofmaleswas35.4years.
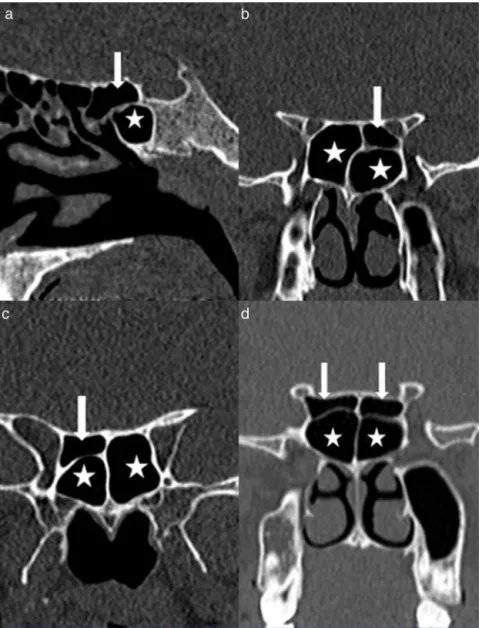
Onodicellpositivitywasobservedin326of618patients and its prevalence was found to be 52.7%. Of the 326 OC-positivepatients,28.8%(n=94)wereright-sided,23.9% (n=78)left-sided,and47.3%(n=154)bilateral(Fig.1).
While121patients(19.6%)withsphenoiditisacceptedas the study group, 497 patients (80.4%) without sphenoidi-tis accepted as the control group. Of the study group, 60.3%(n=73)consistedofmalepatientsand39.7%(n=48) werefemalepatients.Sphenoiditiswassignificantlyhigher inmales thanin females(p<0.05).Right-sided sphenoidi-tiswasidentifiedin 38%(n=46),left-sidedsphenoiditisin 31.4% (n=38), and bilateral sphenoiditis in 30.6% (n=37) (Fig. 2). In the study group, 13 patients who had only contralateralOC-positivitywereacceptedasOC-negative. Ofthe studygroup, 60.3%(n=73) wereipsilateral(n=21) or bilateral (n=52) OC-positive, and 39.7% (n=48) were
Figure2 TheCTscansoftheparanasalsinusesshowsbilateral sphenoiditis(arrows).
OC-negative (n=35) or only contralateral OC-positive (n=13)(Table1).The co-existenceofOCipsilaterally was observedtoincreasetheidentification ofsphenoiditis 1.5-fold,and thisfindingwasstatistically significant(p<0.05) (Fig.3).
Therewere 280 (56.3%)malepatients and217 (43.7%) femalepatientsinthecontrolgroup.Ofthecontrolgroup, 48.3% (n=240) were OC-positive, whereas 51.7% (n=257) wereOC-negative.Of the240 OC-positive patientsof the controlgroup,right-sidedOCwasidentifiedin13.9%(n=69) patients,left-sidedOCin11.3%(n=56)patients,and bilat-eralOCin23.1%(n=115)patients.
300
250
200
150
100
50
0
Sphenoiditis positive Sphenoiditis negative
Presence of sphenoiditis
The n
u
mber of identified cases
Onodi cell positive Onodi cell negative
Table1 CrosstabulationofsphenoiditisandOnodicells.
PresenceofOnodicell(n) Presenceofsphenoiditis(n)
Rightsphenoiditis
(n=46)
Leftsphenoiditis
(n=38)
Bilateral
sphenoiditis(n=37)
Negativesphenoiditis
(n=497)
RightOnodicell(n=94) 12 5 8 69
LeftOnodicell(n=78) 8 9 5 56
BilateralOnodicell(n=153) 14 10 14 115
NegativeOnodicell(n=293) 12 14 10 257
Discussion
Chronicsinus disease may impair the quality of life, and the SS, as well as all sinuses, may be affected by the chronic sinusitis disease processes. Endoscopic endonasal sinussurgeryiscurrentlyacceptedtreatmentmodalityfor chronicsinusitisifmedicaltreatmentisinsufficient.14,15In
addition,smallanatomicalvariationsmaybepresentaround theparanasalsinuses.TheOCisasphenoethmoidalcelland isoneofthecellvariationsaroundtheSS.S˘andulescuetal.16
suggestedthatimportantvariationsoccuratthe sphenoeth-moidaljunction,and most ofthese variationsare related tothe presence of theOC and intrasinusal protrusions of theON.Ozturanetal.3statedthatOCpneumatizationmay
reachandsurroundtheONinvariousextensions.
An accurate evaluation of these structures is possible withHRCT.TheHRCTscancanclearlyshowtherelationship between the OC andthe sphenoid sinus. The multiplanar reconstructiontechniquehasrecentlybeendevelopedasa newimaging technique in the fieldof CT.17 The reported
studiesregarding the prevalence of OCsvarygreatly,and computedtomography(CT)scanssuggestthatprevalenceis between7%and65%.1,3,7---9,18Incadaverstudies,this
preva-lence was found to be 60% by Tanaviratananich et al.19
and15%by Tanand Ong.20 Inthe presentstudy,
multipla-nar(axial,coronal,sagittal)reconstructedHRCTscansand thinsliceswereused,andOCswerefoundin52.7%ofthe patients.Thisfindingwasconsistentwiththeliterature.
NumerousstudiesreportedthatOCshaveclinical signif-icanceforvariousreasons. Whenusingendoscopy, theOC mayeasilybeconfusedwiththeSS.Nomuraetal.2reported
thattheOCdisplacestheSSdownwardandreducesits vol-ume,andsocouldbeassociatedwithsphenoiditis.InaCT study1regarding therelationshipbetween theOCandthe
sphenoidostium(SO),itwasfoundthattheOCcausedthe verticalanglesanddistancesfromtheSOtotheOCbecome larger,whichwouldresultfromtheSObeingdisplacedmore inferiorlyintheOnodigroup,soitwouldbelocatedfarther fromthesuperolateralpositionof theON.Ozturanetal.3
statedthatthecoexistence ofthe OCmayalterthe mor-phologicalchanges inthe floor and/or the lateralwall of theSS.Cheeetal.4statedthatpooraerationanddrainage
oftheOnodiaircellsleadtostasisofsecretionsandcause thepatienttobepronetorecurrentinfections.TheOCmay beassociatedwithmucocelesandopticneuritisbecauseof thesepossibleanatomicvariations.5,6
Analysis of the relationship between anatomical varia-tionsin paranasalsinusesand chronicrhinosinusitisonCT scansof113childrenfoundthatOCswerenotsignificantly
correlatedwithsphenoidsinusitis.10However,inthatstudy,
children were between 5 and 16 years of age, so devel-opment of pneumatization of the sphenoid sinus was not completedinallpatients,andtheOCwasobservedinonly 11patients.Additionally, thecharacteristicsof sinusitisin children may be very different from those of adults. No studieshaveinvestigatedtherelationshipbetweenOCand sphenoiditis in adults.Regarding patients with sphenoidi-tis,60.3% (n=73)were ipsilateralor bilateral OC-positive patients and39.7% (n=48) wereOC-negativeor only con-tralateralOC-positivepatients.Theco-existenceofOCwas observed to increase the identification of sphenoiditis by 1.5-fold,whichwasstatisticallysignificant.
This study has some limitations: when the considering the developing the sinusitis in general, it is not possible to state that OC is the single factor that causes this dis-ease. Inthis connection, asthisstudy is across sectional study, even though it wasobserved that the presence of sphenoiditiswasmore prevalentinpatients withOC,it is not possible to attribute causality among this study fac-tor and the outcome. In patients withsphenoid sinusitis, other locationaland dimensional features of OCsmay be neededtobeexploredregardingthisintimaterelationship, suchasdegreeofaerationandwhetherornotthedrainage pathways of the sphenoid sinuses arecorrupted. In addi-tion,thedefinitivediagnosisofsinusitiscanbeestablished by sinus cavity cultures.21 However, in the case of
sphe-noiditis, it is very difficult to obtain sinus cavity culture samplingbecauseanatomicallyreachingthesinuscavityis nearlyimpossibleinoutpatientconditions,except interven-tionalconditions.Toprovideoptimalconditionsfordiagnosis ofsinusitis,theauthorsobservedandconfirmedthe puru-lent secretion flowing down fromthe sinuses under nasal endoscopicexamination. Furtherstudiesmaybe usefulto establish exact natureof sphenoidaldisease in the cases withco-existenceofOCandsphenoiditisbymeansofculture samplingfromthesphenoidsinuscavityduringintervention.
Conclusion
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
TheauthorsthankAssistantProfessorDr.LütfiSaltukDemir for hisstatistically contribution, fromthe Department of PublicHealth,Meram MedicalFaculty, NecmettinErbakan University,Konya,Turkey.
References
1.HwangSH,JooYH,SeoJH,ChoJH,KangJM.Analysisof sphe-noidsinusintheoperativeplaneofendoscopictranssphenoidal surgeryusingcomputedtomography.EurArchOtorhinolaryngol. 2014;271:2219---25.
2.NomuraK,NakayamaT,AsakaD,OkushiT,HamaT,Kobayashi T, et al. Laterally attached superior turbinate is associated withopacificationofthesphenoidsinus.Auris NasusLarynx. 2013;40:194---8.
3.OzturanO,YenigunA,DegirmenciN,AksoyF,VeysellerB. Co-existenceoftheOnodicellwiththevariationofperisphenoidal structures.EurArchOtorhinolaryngol.2013;270:2057---63.
4.CheeE,Looi A. Onodisinusitispresenting withorbitalapex syndrome.Orbit.2009;28:422---4.
5.DeshmukhS, DeMonteF.Anterior clinoidalmucocelecausing optic neuropathy: resolution with nonsurgical therapy. Case report.JNeurosurg.2007;106:1091---3.
6.KlinkT,PahnkeJ,HoppeF,LiebW.AcutevisuallossbyanOnodi cell.BrJOphthalmol.2000;84:801---2.
7.ShinJH,KimSW,HongYK,JeunSS,KangSG,KimSW,etal. TheOnodicell:anobstacletosellarlesionswitha transsphe-noidal approach. Otolaryngol Head Neck Surg. 2011;145: 1040---2.
8.Tomovic S, Esmaeili A, Chan NJ, Choudhry OJ, Shukla PA, Liu JK, et al. High-resolution computed tomography analy-sisoftheprevalenceofOnodicells.Laryngoscope.2012;122: 1470---3.
9.AkdemirG, TekdemirI, Altin L. Transethmoidalapproach to theopticcanal:surgicalandradiological microanatomy.Surg Neurol.2004;62:268---74.
10.Kim HJ, Jung Cho M, Lee JW, Tae Kim Y, Kahng H, Sung Kim H, et al. The relationship between anatomic variations of paranasal sinuses and chronic sinusitis in children. Acta Otolaryngol.2006;126:1067---72.
11.KozakFD,OspinaJC.Characteristicsofnormalandabnormal postnatalcraniofacialgrowthanddevelopment.In: FlintPW, HaugheyBH,LundVJ,NiparkoJK,RichardsonMA,RobbinsKT, etal.,editors.Cummingsotolaryngologyheadandnecksurgery. Philadelphia,PA:Mosby&Elsevier;2010.p.2613---37.
12.StammbergerH,LundVJ.Anatomyofthenoseandparanasal sinuses. In: Gleeson M, Browning GG, Burton MJ, Clarke J, HibbertJ,JonesNS,etal.,editors.Scott-Brown’s otolaryngol-ogy,headandnecksurgery.London:HodderArnold;2004.p. 1315---43.
13.GliklichRE,MetsonR.Acomparisonofsinuscomputed tomogra-phy(CT)stagingsystemsforoutcomesresearch.AmJRhinol. 1994;8:291---7.
14.WormaldPJ.Theaggernasicell:thekeytounderstandingthe anatomy ofthe frontalrecess.Otolaryngol Head Neck Surg. 2003;129:497---507.
15.Hwang SH, Park CS, Cho JH, Kim SW, Kim BG, Kang JM. Anatomical analysisofintraorbital structuresregardingsinus surgeryusingmultiplanarreconstructionofcomputed tomogra-physcans.ClinExpOtorhinolaryngol.2013;6:23---9.
16.S˘andulescu M, Rusu MC, Ciobanu IC,Ilie A, Jianu AM. More actors,differentplay:sphenoethmoidcellintimatelyrelated tothemaxillarynervecanalandcavernoussinusapex.RomJ MorpholEmbryol.2011;52:931---5.
17.Sapc¸i T, Derin E, Almac¸ S, Cumali R, SaydamB, Karavus¸M. Therelationshipbetweenthesphenoidandtheposterior eth-moidsinusesandtheopticnervesinTurkishpatients.Rhinology. 2004;42:30---4.
18.HartCK,TheodosopoulosPV,ZimmerLA.Anatomyoftheoptic canal: a computed tomography study of endoscopic nerve decompression.AnnOtolRhinolLaryngol.2009;118:839---44.
19.Thanaviratananich S,ChaisiwamongkolK, Kraitrakul S, Tang-sawadW.TheprevalenceofanOnodicellinadultThaicadavers. EarNoseThroatJ.2003;82:200---4.
20.TanHK,OngYK.Sphenoidsinus:ananatomicandendoscopic studyinAsiancadavers.ClinAnat.2007;20:745---50.