REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
OfficialPublicationoftheBrazilianSocietyofAnesthesiologywww.sba.com.br
SCIENTIFIC
ARTICLE
Bedside
prediction
of
right
subclavian
venous
catheter
insertion
length
Yoon
Ji
Choi
a,
Kyung-Don
Hahm
b,∗,
Koo
Kwon
b,
Eun-Ho
Lee
b,
Young
Jin
Ro
b,
Hong
Seuk
Yang
baDepartmentofAnesthesiologyandPainMedicine,SeoulPaikHospital,CollegeofMedicine,InjeUniversity,Seoul,
RepublicofKorea
bDepartmentofAnesthesiologyandPainMedicine,AsanMedicalCenter,UniversityofUlsanCollegeofMedicine,Seoul,
RepublicofKorea
Received10July2013;accepted8October2013 Availableonline13August2014
KEYWORDS
Centralvenous catheter; Clavicularnotch; Subclavianvein
Abstract
Backgroundandobjective: Thepresentstudyaimedtoevaluatewhetherrightsubclavianvein
(SCV)catheterinsertiondepthcanbepredictedreliablybythedistancesfromtheSCVinsertion
sitetotheipsilateralclavicularnotchdirectly(denotedasI-IC),viathetopoftheSCVarch,or
viatheclavicle(denotedasI-T-ICandI-C-IC,respectively).
Method: Intotal,70SCVcatheterizationswerestudied.TheI-IC,I-T-IC,andI-C-ICdistancesin
eachcaseweremeasuredafterultrasound-guidedSCVcatheterinsertion.Theactuallengthof
thecatheterbetweentheinsertionsiteandtheipsilateralclavicularnotch,denotedasL,was
calculatedbyusingchestX-ray.
Results:LdifferedfromtheI-T-IC,I-C-IC,andI-ICdistancesby0.14±0.53,2.19±1.17,and
−0.45±0.68cm,respectively.ThemeanI-T-ICdistancewasthemostsimilartothemeanL
(intr-aclasscorrelationcoefficient=0.89).ThemeanI-ICwassignificantlyshorterthanL,whilethe
meanI-C-ICwassignificantlylonger.Linearregressionanalysisprovidedthefollowingformula:
PredictedSCVcatheterinsertionlength(cm)=−0.037+0.036×Height(cm)+0.903×I-T-IC(cm)
(adjustedr2=0.64).
Conclusion: TheI-T-ICdistancemay beareliablebedsidepredictoroftheoptimalinsertion
lengthforarightSCVcannulation.
© 2013SociedadeBrasileirade Anestesiologia.Publishedby ElsevierEditoraLtda.Allrights
reserved.
∗Correspondingauthor.
E-mail:[email protected](K.-D.Hahm).
PALAVRAS-CHAVE
Catetervenoso central;
Entalheclavicular; Veiasubclávia
Previsãodocomprimentodeinserc¸ãodecateteremveiasubcláviadireitaàbeirado leito
Resumo
Justificativaeobjetivo:Opresenteestudotevecomoobjetivoavaliarseaprofundidadede
inserc¸ãodecateteremveiasubclávia(VSC)direitapodeserprevistadeformaconfiávelpelas
distâncias do local de inserc¸ão naVSC até a incisura clavicular ipsilateral (I-IC), passando
diretamentepelapartesuperiordoarcodaVSCoudaclavícula(denominadasI-T-ICeI-C-IC,
respectivamente).
Método: Nototal,70cateterismosdeVSCforamestudados.AsdistânciasI-IC,I-T-ICeI-C-ICde
cadacasoforammensuradasapósainserc¸ãodocateterguiadaporultrassom.Ocomprimento
docateterentreolocaldeinserc¸ãoeaincisuraclavicularipsilateral(L)foicalculadopormeio
deradiografia.
Resultados: Asdiferenc¸as em centímetrosdeL em relac¸ãoàsdistâncias I-T-IC,I-C-ICe I-IC
foramde0,14±0,53;2,19±1,17e0,45±0,68respectivamente.AmédiadeI-ICfoi
significa-tivamentemenorqueL,enquantoamédiadeI-C-ICfoisignificativamentemaior.Aanálisede
regressãolinearforneceuaseguintefórmula:Comprimentoprevistodainserc¸ãodecateterem
VSC(cm)=−0,037+0,036xAltura(cm)+0,903xI-T-IC(cm)(r2ajustado=0,64).
Conclusão:AdistânciaI-T-ICpodeserumpreditivoconfiáveldocomprimentodeinserc¸ãoideal
paracanulac¸ãoemVSCdireita.
©2013SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Todosos
direitosreservados.
Introduction
Several landmarks,1,2 simple formulas,3 and
electrocardiography4 have been used for the optimal
insertion depth of the central venous catheter. However, for subclavian venous cannulations, such confirmatory techniquesareoflimiteduse.
A recent study5 suggested thatadding (i) the distance
between theinsertion point of needle and the ipsilateral clavicular notch to(ii) the vertical distance between the carinaandtheipsilateralclavicularnotchgeneratesa reli-abletippositionnearthecarinalevelthatguidessuitable andsafepositioningofthecentralvenouscathetertipabove thepericardialreflection.1However,thismethodhassome
limitations.Thismethodrequiresachestradiographthatis neededtoevaluatetheverticaldistancebetweenthecarina andtheipsilateralclavicularnotch.And,thesubclavianvein followsacurvedpath.6 Thus,thismethodmaybeshorter
thantheoptimalinsertiondepth.
The aimof thepresent study wastoevaluatewhether severaldistancesfromtheinsertionpointofneedletothe ipsilateralclavicularnotch,runningdirectly(denotedas I-IC),viathesubclavianveintop,orviatheclavicle(denoted asI-T-ICandI-C-IC,respectively),arereliablebedside pre-dictorsoftheoptimalinsertionlengthforultrasound-guided rightsubclavianvenouscannulation.
Method
Written informed consent was obtained from all patients after approval of the trial by the Institutional Review Board(2012---0104)andClinicalResearchinformationService (KCT0000612).Allpatientsrequiredsubclavianvenous can-nulationoverthecourseofa6monthperiod.Thepatients
whodidnotagreetoparticipateinthestudywereexcluded from this study,as werepatients who had some spine or vesseldeformitiesorinwhomthepositioningofthecentral venouscatheterwasinadequate.
Patient ages, gender, heights, and weights were recorded. On arrival in the operating room, the patients were monitored. After the induction of anesthesia, skin preparationandsteriledrapingwereperformed.Subclavian venous catheterization was performed by using a four-lumen central venous catheter (Arrow International Inc., Reading,PA,USA)andtheinfra-clavicularapproachwitha sonography-guided longitudinal view. The probe (SonoSite S-Series,Bothell,WA,USA)wasplacedparalleltothelong axisofthesubclavianveinandtheneedlewasinserted adja-cent to the short edge of the probe so that it remained visibleasittraveledthroughtheoverlyingtissuesintothe subclavianvein.7,8Subsequently,thecatheterwasinserted
by usinga guide-wire. To determine the correctdepth of catheterinsertion,thepatient’sheadandneckwereplaced intheneutralpositionafterinsertionofthecatheterandan intra-operativefull-inspiration chestradiographwastaken toestablish the fact that thecentral venous cathetertip wasatthelevelofthecarina.2Tooptimizethepositionof
C
G F
I
B
L E
IC
A T
D
Figure1 TheI-T-IC,I-C-IC,andI-ICdistancesweremeasured afterultrasound-guidedinsertionoftherightsubclavianvenous cannulationcatheter.The bluecircleindicates theipsilateral clavicularnotch(IC).Theactualtotalcatheterinsertionlength (L+A)wascalculated byadding(i)thedistancebetween the needleinsertionpointandtheipsilateralclavicularnotch(this distanceisdesignatedas L)to (ii)thedistancebetween the ipsilateralclavicularnotchandthecathetertip(thisdistance is designatedas A).The I-T-IC distance isthe distance from the needleinsertion point to the ipsilateral clavicular notch viathetopofthesubclavian vein(i.e.,distanceD+distance E) thatisindicated bythe yellowline.TheI-C-ICdistanceis thedistancefromtheneedleinsertionpointtotheipsilateral clavicularnotchviatheclavicle(i.e.,distanceF+distanceG) thatisindicatedbythegreenline.TheI-ICdistanceisindicated byBandtheredline,andisthedirectdistancefromtheneedle insertionpointtotheipsilateralclavicularnotch.
measured on the surface of skin after inserting the sub-clavianveincannulationcatheter,andI-T-ICwasguidedby ultrasound.TheI-ICdistanceisthedirectlinebetweenthe insertionpointofneedleandtheipsilateralclavicularnotch; itis indicated inFig.1 bythe redline anddenotedasB. PointT,whichwasdefinedasthehighestpointofthe sub-clavianveinarch,wasdeterminedbyusingultrasound.The I-T-IC distance (denoted by the yellow line in Fig.1) was determinedbyadding(i)thedistancebetweentheinsertion pointofneedleandpointT(thedistancedenotedbyD)to (ii)thedistancebetweenpointTandtheipsilateral clavic-ularnotch(thedistancedenotedbyE).TheI-C-ICdistance (denoted by the green line in Fig. 1) wasdetermined by adding(i)theshortestdistancebetweentheclavicle(point C)andtheinsertionpointofneedle(thedistancedenoted byF)to(ii)thedistancebetweentheclavicle(pointC)and theipsilateralclavicularnotch(thedistancedenotedbyG). Regardingsample size,itwasdeterminedthat75 mea-surementswere neededfor a significancelevel of0.05, a power of90%,and anexclusionrate of15%.These deter-minationswere based onthe results of a previous study5
thatreportedadistanceof1cmfromthecarinaasbeinga safecentralvenouscathetertiplevel(theSDwas1.2cm). All variables areexpressed asmean±standard deviation, ornumberofsamples.Apairedt-testwith95%confidence intervals was used to evaluate the differences between L and the I-T-IC,I-C-IC, or I-IC distances. The agreement
Table1 Demographiccharacteristicsofthepatients.
Patientcharacteristics(n=70)
Age(years) 58.36±15.11
Gender(M/F) 21/49
Height(cm) 157.63±8.55
Weight(kg) 61.49±10.34
Thevaluesareexpressedasmean±SDornumberofpatients.
betweenLandI-T-IC,I-C-IC,orI-ICwasassessedby calculat-ingtheintraclasscorrelationcoefficient(ICC).Correlations betweentheL+AandI-T-ICdistancesandother variables were assessed by using Pearson correlation analysis. Lin-earregressionwas performed todevelop amodel for the predicted L+A on the basis of I-T-IC and patient height. For the final predicted models, a bootstrap analysis was performed: 1000 bootstrap replicates were generated by randomsamplingfromthe original dataset with replace-ment. The regression coefficient of the bootstrap bias ---correctedpredictionequationwasestimatedbyconsidering biaswith samples of 1000 bootstrap replications. All sta-tisticaldata wereanalyzed by usingSPSS 20.0(SPSS Inc., Chicago,IL).Ap-valuelessthan0.05wasconsideredtobe statisticallysignificant.
Results
Of the 75 patients who were originally enrolled in this study, three patients changed their minds about partic-ipating before the study began, and two patients were excluded becausethetip wasin an internal jugularvein. As a consequence, the final study cohort comprised 70 subclavianveincatheterizationsthatwereperformedwith sonographicguidance.Thepatientcharacteristics are pre-sentedinTable1.
Themeanactualtotallengthofthesubclaviancatheter (L+A)thatwasinsertedwas14.10±1.46cm.Table2lists the means of L (the length of the catheter between the insertion point of needle and the ipsilateral clavicular notch),thedistancesofI-ICandI-C-IC,andI-T-ICthatwere measuredonthesurfaceofskin.Todeterminehowwellthey
Table2 Distancesused topredictthe optimallength of
subclavianvenouscannulationandtheiragreementwithL.
Measurements Mean±SD t-Statistic p-Value ICC
L(cm) 92.2±11.6
I-T-IC(cm) 93.5±11.7 1.45 0.15 0.89
I-C-IC(cm) 114.0±15.5 −17.60 <0.001a 0.28
I-IC(cm) 87.6±10.8 −5.64 <0.001a 0.76
Thevaluesareexpressedasmean±SD.
ICC,intraclasscorrelationcoefficient;L,catheterlengthfrom theneedleinsertionpointtotheipsilateralclavicularnotch; I-T-IC,thedistancefromtheneedleinsertionpointtotheipsilateral clavicularnotchviathetopofthesubclavianvein;I-C-IC,the distancefromtheneedleinsertionpointtotheipsilateral clav-icularnotchviatheclavicle;I-IC,thedirectdistancefromthe needleinsertionpointtotheipsilateralclavicularnotch.
2
1
0
–1
–2
6 7 8 9 10 11 Average of L and I-T-IC (cm)
Diff
erences betw
een L
and I-T
-IC (cm)
Diff
erences betw
een L
and I-C-IC (cm)
Diff
erences betw
een L
and I-I-IC (cm)
Average of L and I-C-IC (cm) Average of L and I-I-IC (cm) 12 13 14 15 6 7 8 9 10 11 12 13 14 15 6 7 8 9 10 11 12 13 14 15
+1.96 SD
Mean
–1.96 SD
+1.96 SD
Mean
–1.96 SD
+1.96 SD
Mean
–1.96 SD
A
B
C
8
6
4
2
0
–2
2
0
–2
Figure2 Bland---AltmanplotsshowingtheaveragesanddifferencesbetweenLandI-T-IC(A),I-C-IC(B),orI-IC(C).Themean differenceswere 0.14,2.19, and−0.45cm, respectively.L, thelength ofthe catheterfromthe needleinsertion point tothe ipsilateralclavicularnotch;I-T-IC,thedistancefromtheneedleinsertionpointtotheipsilateralclavicularnotchviathetopofthe subclavianvein;I-C-IC,thedistancefromtheneedleinsertionpointtotheipsilateralclavicularnotchviatheclavicle;I-IC,the directdistancefromtheneedleinsertionpointtotheipsilateralclavicularnotch.
predicted optimal subclavian venous cannulation depth, their agreement with L wasassessed. The L and the I-T-ICdidnotdiffersignificantly(p=0.15).However,Ldiffered significantlyfrombothI-C-IC(p<0.001)andI-IC(p<0.001). Bland---Altmanplotsdemonstratedlargevariationsinthe dif-ferencesbetweenLandI-ICandbetweenLandI-C-IC.The meandifferencesbetweenLandI-T-IC,I-C-IC,orI-ICwere 0.14, 2.19, and −0.45cm, respectively. The differences between I-T-IC and L were smaller than the differences betweenLandI-ICandbetweenLandI-C-IC(Fig.2).
The meandifferencebetween I-T-ICandLwas0.14cm [95% confidence interval (CI) 0.01, 0.26], and the ICC of agreementwas0.89(95%CI0.83,0.93).The mean differ-encebetweenI-C-ICandLwas2.19cm(95%CI1.91,2.47), andtheICC ofagreement was0.28(95% CI−0.09,0.62). ThemeandifferencebetweenI-ICandLwas−0.45cm(95% CI−0.61,−0.29),andtheICCofagreementwas0.76(95% CI0.46,0.88).TheICCvalueslistedinTable2indicatethat theI-T-ICdistancetendedtobethemostsimilartoL.
Thetotalinsertionlengthofsubclavianvenouscatheter (L+A distance in Fig. 1) correlated significantly with I-T-IC (r=0.78, p<0.0001), patient age (r=−0.72, p=0.55), weight(r=0.11,p=0.36),andheight(r=0.36,p=0.002).
Using linear regression, the following formula was devisedtopredictL+A:
Predicted L+A (cm)=−0.037+0.036×Height (cm)+0.903×I-T-IC(cm),adjustedr2=0.64.
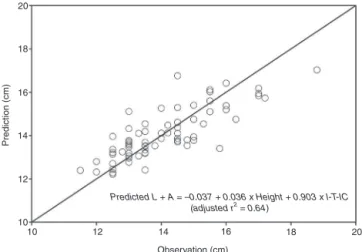
Fig.3showedthattheL+Avaluespredictedbythis for-mularelatedtotheobservedL+Avalue.
None of the patients showed any complications during thedeterminationoftheI-IC,I-T-IC,I-C-IC,andLdistances, norduringorafterrightsubclavianveincannulation.
Discussion
Ofthethreeanatomiclandmarksinvestigatedhere,onlythe I-T-ICdistancesuccessfullypredictedtheoptimalsubclavian venouscatheterlength,whichsuggeststhatitmaybea use-fulbedsidepredictorofthecorrectcatheterinsertionlength thatistobeusedduringrightsubclavianvenouscannulation. Moreover,by usinga formula based onI-T-IC and height, the optimal right subclavian venous catheter insertion lengthcouldbepredicted withouthavingtomakeachest radiograph.
20
18
16
14
12
10
10 12 14 16
Predicted L + A = –0.037 + 0.036 x Height + 0.903 x I-T-IC (adjusted r2 = 0.64)
Observation (cm)
Prediction (cm)
18 20
Figure 3 Relationship between the total insertion length predicted by the following formula and the observed total insertion length (L+A). Predicted L+A (cm)=−0.037+0.036×Height+0.903×I-T-IC (adjusted
r2=0.64).I-T-IC,thedistancefromtheneedleinsertionpoint
totheipsilateralclavicularnotchviathetopofthesubclavian vein.
There are no gold standards for predicting the opti-mal length of catheterinsertionduring subclavian venous cannulation. To determine theoptimal insertionlength of the central venous catheter, several landmarks,1,2 simple
formulas,3andelectrocardiography4havebeenused.
How-ever,forsubclavianvenouscannulations,suchconfirmatory techniquesareoflimiteduse.
Fletcher etal. suggested that central venous catheter tipsshouldlie abovethepericardialreflection.9 Ifcentral
morefrequently than cathetertipplaced belowthe peri-cardial reflection.10,11 Andan angle of the centralvenous
cathetertiptovesselwallandthetypeoffluidinfusedcan leadtovesselerosion,painoninjectionofdrugs,infection, andthrombosis.12,13
Topographic landmarks, including the angle of Louis14
and the right third intercostal space15 have been used
toguide the correct positioningof the subclavianvenous catheter tip. Both of them are related to the horizon-tal plane of thetracheal carina.6 In theprevious studies,
formulas12,13,16usingpatientheightorskin-to-veindistance
also recommended. While the techniques based on both of these landmarks are easy to use without any poten-tialcomplications,theycanalsobeaffectedbyanatomical variation between patients and radiological and physical landmarks,andpatient’sheight,simultaneously.
Kimetal.17 showedthattheoptimalcatheterinsertion
length during right subclavian venous cannulation was 12.9±0.9cm, while Ryu et al.5 suggested that 13.8cm
(10.5---18.0cm) of subclavian venous catheter insertion would be optimal when the infra-clavicular landmark approach was used. However, this fixed length does not considerheight,thepreferredinsertionpointofthe practi-tioner,orthemethodofsubclavianvenouscannulation,all ofwhichmightinfluencethefinallocationofthecatheter tip.
To determine the optimal insertion length of the central venous catheter, electrocardiography4 (ECG) was
performed.ThepeakP-waveisusuallyobservedwhenthe central venous catheter tip was placed at the superior vena cava/right atrium junction. At about 4.0cm above the superior vena cava/rightatrium junction,the P-wave returns to a normal shape and size.4 Moreover, a
trans-esophageal echocardiography guidance of central venous catheter placement may also effectively be conducted. However,bothof thesetechniques needadditional equip-ment and are potentially associated with increased costs andrisksoffurthercomplications.18,19
A previous study1 has shown that the carina was
sug-gestedtobeareliablelandmarkfordeterminingthemost appropriate and safest position of the subclavian venous catheter tip abovethe pericardial reflection. The advan-tages of this approach include the fixation of the carina toconnectivetissue,whichensures preservationof place-ment(evenunderconditionsofpulmonary pathology)and areducedrisk ofcardiac tamponade.Thus,this landmark was also usedin the present study.Notably, the internal jugular vein and the subclavian vein can be found easily beneaththeipsilateralclavicularnotch,whichisthesiteof articulationwiththesternalendoftheclavicleandcanbe readilypalpatedbyhand.6,20 Therefore,inanotherstudy,5
the carina served as a landmark of adequate subclavian veininsertionlengthtogetherwithanestimateofthe inser-tionlength, which wascalculatedon thebasis of a chest radiographtakenbeforecentralvenous catheterinsertion by adding (i)the distance between the insertionpoint of needletothe ipsilateralclavicular notchto(ii)the verti-caldistancebetweentheipsilateralclavicularnotchtothe carina.However,thismethodhassomelimitations.First,a chestradiographisneededtoevaluatetheverticaldistance betweentheipsilateralclavicularnotchandthecarina. Sec-ond,thesubclavianveinfollowsacurvedpath:theaxillary
veinextendsfromthe axillary area,througheitherabove orbelowtheclavicle,tobeneaththeipsilateralclavicular notch.6 Thus,the distancebetween theinsertionpoint of
needleandtheipsilateralclavicularnotchmaybeshorter than the optimal insertion length. The vertical distance betweenthecarinaandtheipsilateralclavicularnotchmay betooshortbecausethesubclavianveiniscurvedand prac-titionertriedwithvariousinsertionpointastheirproperand technique.Thus,theuseof theverticaldistancebetween theipsilateralclavicularnotchandthecarinacanresultin subclavianvenouscathetermalpositionandcanevencause complications.Inthepresentstudy,theI-ICvalueswere sig-nificantlyshorterthanL.Itshouldbenotedthattheuseof ultrasoundtodeterminethehighestpointofthesubclavian veincanalsobechallengingsometimes.
Inthepresentstudy,thesubclavianveinwascannulated byusingasonography-guidedlongitudinalapproach. Ifthe usual the infra-clavicular landmark-guided technique is used, it could lead to puncture of the posterior wall of thesubclavianvein,whichliesextremelyclosetothelung apex.However,byusingthesonography-guidedlongitudinal approach,the preferredpuncture sitein theaxillary vein (ratherthanthesubclavianvein)ispuncturedeasily,which can decrease the likelihood of pneumothorax.7 Moreover,
theaxillaryvenouspuncturebetweenthesubclaviusmuscle and the costoclavicular ligament complex decreases the likelihood of trapping the catheter.21 It should be noted,
however,thatthesonography-guidedlongitudinalapproach can lead to more variable subclavian venous catheter lengths than the infra-clavicular landmark technique because the insertion point may vary depending on the practitioner;moreover, axillary vein puncture means that alongerlengthof curvedveinis involved.To compensate for this, the I-T-IC distance was measured in the present study.Indeed,ofthevariousdistancesthatweremeasured, theI-T-ICdistancewasfoundtobethemostsimilartothe actuallength.
TheI-T-ICdistancehassomelimitations.Itissometimes difficulttoidentifythetopofthesubclavianveinbecause thetopof thesubclavianveincan behiddenbeneaththe clavicle;thus,skillisrequiredtofindthislandmark.In addi-tion,the A distance must be measured on the basis of a chestradiography.Therefore,aformulatopredictL+Awas calculatedonthebasisofI-T-ICandheightalone.This for-mulacouldbeusedtoidentifytheoptimalinsertionlength insomesituations.
In conclusion, the I-T-IC distance may enable reliable bedsidepredictionofthebestoptimalinsertionlengthofa rightsubclavianveincatheter,evenwhensonographic guid-anceisusedtoplacethecatheter.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgements
References
1.Schuster M, Nave H, Piepenbrock S, et al. The carina as a landmarkincentralvenouscatheterplacement.BrJAnaesth. 2000;85:192---4.
2.StonelakePA,BodenhamAR.Thecarinaasaradiological land-markfor central venouscathetertipposition.Br JAnaesth. 2006;96:335---40.
3.Chalkiadis GA,Goucke CR. Depthofcentralvenouscatheter insertioninadults:anauditandassessmentofatechniqueto improvetipposition.AnaesthIntensiveCare.1998;26:61---6. 4.Jeon Y, Ryu HG, Yoon SZ, et al. Transesophageal
echocar-diographicevaluation ofECG-guidedcentralvenouscatheter placement.CanJAnaesth.2006;53:978---83.
5.RyuHG,BahkJH,KimJT,etal.Bedsidepredictionofthecentral venouscatheterinsertiondepth.BrJAnaesth.2007;98:225---7. 6.EllisH, DussekJE. Surfaceanatomy.In: PLW,editor. Gray’s anatomy. 38thed.NewYork: ChurchillLivingstone;1995. p. 1916.
7.MauroMA,JaquesPF.Radiologicplacementoflong-termcentral venouscatheters:areview.JVascIntervRadiol.1993;4:127---37. 8.MachiJ, Takeda J, KakegawaT. Safe jugularand subclavian venipuncture under ultrasonographic guidance. Am J Surg. 1987;153:321---3.
9.FletcherSJ,BodenhamAR.Safeplacementofcentralvenous catheters:whereshouldthetipofthecatheterlie?BrJAnaesth. 2000;85:188---91.
10.TocinoIM,WatanabeA.Impendingcatheterperforationof supe-riorvenacava:radiographicrecognition.AJRAmJRoentgenol. 1986;146:487---90.
11.DuntleyP,SieverJ,KorwesML,etal.Vascularerosionby cen-tral venouscatheters.Clinicalfeatures and outcome.Chest. 1992;101:1633---8.
12.Raad II, Luna M, Khalil SA, et al. The relationship between thethromboticandinfectiouscomplicationsofcentralvenous catheters.JAMA.1994;271:1014---6.
13.CadmanA,LawranceJA,FitzsimmonsL,etal.Toclotornot toclot?Thatisthequestionincentralvenouscatheters.Clin Radiol.2004;59:349---55.
14.EzriT,WeisenbergM,SesslerDI,etal.Correctdepthof inser-tionofrightinternaljugularcentralvenouscathetersbasedon externallandmarks:avoidingtherightatrium.JCardiothorac VascAnesth.2007;21:497---501.
15.KimKO,JoJO,KimHS,etal.Positioninginternaljugularvenous cathetersusing theright thirdintercostalspace in children. ActaAnaesthesiolScand.2003;47:1284---6.
16.PeresPW.Positioningcentralvenouscatheters---aprospective survey.AnaesthIntensiveCare.1990;18:536---9.
17.KimMC,KimKS,ChoiYK, etal.Anestimationofright-and left-sidedcentralvenouscatheterinsertiondepthusing mea-surement of surface landmarks along the course of central veins.AnesthAnalg.2011;112:1371---4.
18.Wilson RG, Gaer JA. Right atrial electrocardiography in placement of central venous catheters. Lancet. 1988;1: 462---3.
19.AndropoulosDB,StayerSA,BentST,etal.Acontrolledstudy oftransesophagealechocardiographytoguidecentralvenous catheterplacementincongenitalheartsurgerypatients.Anesth Analg.1999;89:65---70.
20.Soames RW. Skeletal system. In: Williams PL, editor. Gray’s anatomy. New York: Churchill Livingstone; 1995. p.537.