REVISTA
BRASILEIRA
DE
ANESTESIOLOGIA
PublicaçãoOficialdaSociedadeBrasileiradeAnestesiologiawww.sba.com.br
SCIENTIFIC
ARTICLE
Effect
of
dexmedetomidine
on
acute
lung
injury
in
experimental
ischemia---reperfusion
model
Ömer
Burak
Küc
¸ükebe
a,
Deniz
Özzeybek
b,
Ruslan
Abdullayev
a,∗,
Adil
Ustao˘
glu
c,
Is
¸ıl
Tekmen
d,
Tuncay
Küme
eaAdıyamanUniversityResearchandEducationalHospital,DepartmentofAnesthesiologyandReanimation,Adıyaman,Turkey bDokuzEylülUniversityMedicalFaculty,DepartmentofAnesthesiologyandReanimation, ˙Izmir,Turkey
cZonguldakAtatürkHospital,DepartmentofAnesthesiologyandReanimation,Zonguldak,Turkey dDokuzEylülUniversityMedicalFaculty,DepartmentofHistologyandEmbryology, ˙Izmir,Turkey
eDokuzEylülUniversityMedicalFaculty,DepartmentofMedicalBiochemistry, ˙Izmir,Turkey
Received1March2015;accepted17August2015 Availableonline21March2016
KEYWORDS
Experimental; Dexmedetomidine; Reperfusioninjury; Acutelunginjury
Abstract
Purpose: Ischemia---reperfusioninjuryisoneoftheconsequencesoftourniquetapplicationfor
extremitysurgery.Theaimofthestudywastoestablishtheeffectofdexmedetomidineonthe acutelunginjuryfollowinglowerextremityexperimentalischemia---reperfusionmodelinrats.
Methods:Twenty-eight Wistar-Albino breed Rats were recruited after Ethics Committee
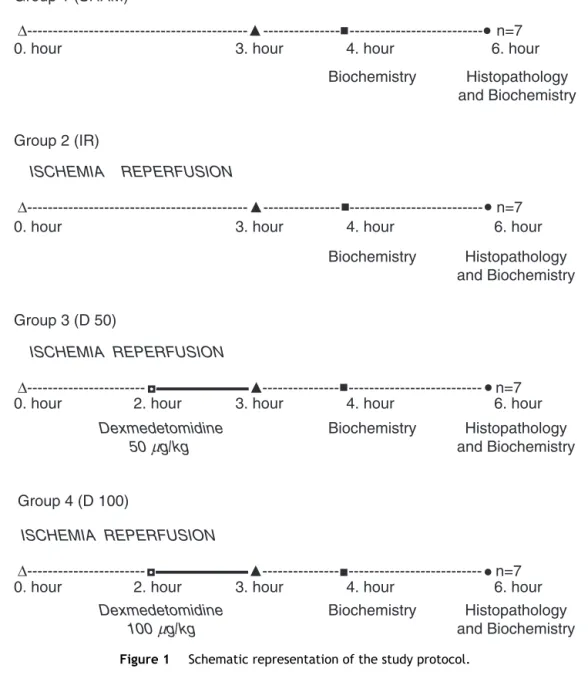
approval and allocatedinto 4 groups,each with 7subjects. Group 1(SHAM) received only anesthesia. Group 2 (IR) hadexperienced 3h ofischemia and3h ofreperfusion using left lowerextremitytourniquet afteranesthesia application.Groups3(D-50)and4(D-100)had undergonethesameproceduresasintheGroup2,exceptforreceiving50and100mg·kg−1,
respectively,dexmedetomidineintraperitoneally1hbeforethetourniquetrelease.Blood sam-pleswereobtainedfortheanalysisoftumornecrosingfactor-␣andinterleukin-6.Pulmonary tissuesampleswereobtainedforhistologicalanalysis.
Results:Nosignificantdifferenceregardingbloodtumornecrosingfactor-␣andinterleukin-6
valueswasfoundamongthegroups,whereaspulmonarytissueinjuryscoresrevealedsignificant difference.HistologicalscoresobtainedfromtheGroup2weresignificantlyhigherfromthose intheGroups1, 3and4withp-values 0.001foreachcomparison.Moreover, Group1scores werefoundtobesignificantlylowerthanthoseintheGroups3and4withp-values0.001and 0.011,respectively.NosignificantdifferencewasobservedbetweentheGroups3and4.
Conclusion: Dexmedetomidine is effective in reduction of the experimental
ischemia---reperfusion inducedpulmonary tissueinjury in rats, formedby extremity tourniquet appli-cation.
©2016SociedadeBrasileiradeAnestesiologia.Publishedby ElsevierEditoraLtda.Thisisan openaccessarticleundertheCCBY-NC-NDlicense (http://creativecommons.org/licenses/by-nc-nd/4.0/).
∗Correspondingauthor.
E-mail:[email protected](R.Abdullayev). http://dx.doi.org/10.1016/j.bjane.2015.08.002
PALAVRAS-CHAVE
Experimental; Dexmedetomidina; Lesãodereperfusão; Lesãopulmonar aguda
Efeitodedexmedetomidinasobrelesãopulmonaragudaemmodeloexperimental
deisquemia-reperfusão
Resumo
Objetivo:Alesãodeisquemia-reperfusãoéumadasconsequênciasdaaplicac¸ãodotorniquete
emcirurgiasdeextremidades.Oobjetivodoestudofoideterminaroefeitodedexmedetomidina emlesãopulmonaragudaapósmodeloexperimentaldeisquemia-reperfusãoemextremidade inferiorderatos.
Métodos: Vintee oito ratos albinosWistar foram recrutadosapós aprovac¸ão do Comitêde
Éticaealocadosemquatrogrupos,cadaumcomseteindivíduos.OGrupo1(Sham)recebeu apenasanestesia.OGrupo2(IR)foisubmetidoa3horasdeisquemiae3horasdereperfusão comousodetorniquete em extremidadeinferiorapósaaplicac¸ãodaanestesia.Osgrupos 3(D-50) e4 (D-100)foramsubmetidos aosmesmos procedimentos doGrupo 2, exceto por receberem50e100mg·kg−1dedexmedetomidina,respectivamente,porviaintraperitoneal1
horaantesdaliberac¸ãodotorniquete.Amostrasdesangueforamcoletadasparaanálisede TNF-␣eInterleucina-6(IL-6).Amostrasdetecidopulmonarforamcoletadasparaanálisehistológica.
Resultados: Nãohouvediferenc¸asignificativaquanto aosvalores sanguíneosdeTNF-␣e
IL-6entreosgrupos,enquantoosescoresdelesãoemtecidospulmonaresrevelaramdiferenc¸a significativa.OsescoreshistológicosobtidosnoGrupo2foramsignificativamentemaioresque osdosgrupos1,3e4,comvalores-pde0,001paracadacomparac¸ão.Alémdisso,osescores doGrupo1foramsignificativamentemenoresqueosdosgrupos3e4,comvalores-pde0,001 e0,011,respectivamente.Nãohouvediferenc¸asignificativaentreosgrupos3e4.
Conclusão:Dexmedetomidina mostrou eficácia na reduc¸ão de lesão em tecido pulmonar
induzidaporisquemia-reperfusãoexperimentalemratos,ocasionadaporaplicac¸ãode torni-queteemextremidade.
©2016SociedadeBrasileiradeAnestesiologia.PublicadoporElsevierEditoraLtda.Este ´eum artigoOpen Accesssobumalicenc¸aCCBY-NC-ND (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Introduction
Cessation of the blood flow, namely tissue ischemia,and
reperfusion after a period of time are the main
patho-physiological mechanisms responsible for organ damages
following some clinical conditions like organ
transplan-tation, cerebral ischemia, stroke, myocardial infarction,
thromboemboli,cardiopulmonarybypassand vascular
sur-geries, major trauma and hemorrhagic shock, as well as
surgicalprocedureswithtourniquetuse.1,2Ischemicdamage ismainlytheresultofthenecrosisofthecellsdueto
oxy-gencessation;oxygensupplyduringischemiaisnotenough
tomeet the metabolic needs of the cells and this
condi-tionresultsintheactivationoftheanaerobicmetabolism.3
When the tissue blood flow is provided again, i.e.
reper-fusion starts, it paradoxically increases the local tissue
damage,togetherwithaninflammatoryresponseresulting
indistantorgandamage.2,3Manyinflammatoryagentshave
been shown to be responsible for this damage, namely
ischemia---reperfusioninjury(IRI).2
Cytokines have been blamedfor distant organdamage
of IRI.4 Blood, kidney and lung tumor necrosing
factor-␣ (TNF-␣), interleukin (IL) IL-1 andIL-6 levelshave been
found to be high after lower extremity ischemia.5 The
mediatorsreleasedafterischemia---reperfusion(IR)resultin
localand distantorganinjuries through freeoxygen
radi-calsandleukocytes.6,7 Negativeimmunoregulatoryeffects
of noradrenaline have been demonstrated in the
forma-tion of monocyte/macrophage origin mediators (TNF-␣,
IL-1, IL-6) andthis effectwaslinkedtoitsboth  and␣2
adrenoceptors.8
Dexmedetomidineisastrongandselective␣2-adrenergic
agonist that is an active d-isomer of medetomidine
and metabolized in the liver. It has been approved to
be used for sedation in intensive care unit and
pos-sessessedativeandanalgesiccharacteristics.9,10Thereare
few studies in the literature regarding anti-inflammatory
effects of dexmedetomidine.11---16 Yagmurdur et al.14 have
demonstrateddexmedetomidine todecrease thelevels of
malondialdehydeandhypoxanthine(thatareformed after
IR), following tourniquet application for upper extremity
surgery. Although it has been shown that
dexmedetomi-dine has some protective effects for IRI locally, we have
notencountered astudy regardingits effectsonsystemic
inflammatoryresponseanddistantorgandamage.
We aimed to establish the effects of two different
doses of dexmedetomidine on the acute lung injury
fol-lowing lower extremity experimental IR model in rats.
The hypothesis was based on possible protective effects
of dexmedetomidine taking into consideration its
anti-inflammatoryeffects.
Methods
This studywascarriedoutin DokuzEylulUniversity
Medi-cal Faculty Multidisciplinary Animal Laboratory between
approval of Dokuz Eylul University Experimental Animal
Studies Ethics Committee, ˙Izmir, Turkey (24/11/2008, n◦
134, Chairperson Prof. M. Olguner). Twenty-eight adult
femaleWistar-Albinobreedratsweighting250---340gwere
usedforthestudy.Theanimalswereprovidedwithstandard
pellet foodand waterandwere keptin 12-hourcyclesof
lightanddarkforadaptationbeforethecommencementof
the study.The temperature and humiditywere also
stan-dardized.
The rats were fasted for 12h before the surgical
pro-cedure and were allowed to drink water only. Each rat
was weighted before the experiment and the doses of
dexmedetomidine were calculated. They were randomly
allocated into one of the 4 groups using closed envelope
method. Group 1 (SHAM, n=7) received only anesthesia
with blood sample obtainment at the 1st hour of
reper-fusionandbloodandtissuesampleobtainmentat theend
ofthereperfusion.Group2(IR,n=7)hadexperienced3h
ofischemiaand3hofreperfusionusingleftlowerextremity
tourniquetafteranesthesiaapplication.Bloodsamplewas
obtainedat the1st hourof reperfusionandat theendof
the reperfusion blood and tissue samples were obtained.
Group3(D-50,n=7)hadundergonethesameproceduresas
intheGroup 2,exceptforreceiving 50g/kg
dexmedeto-midine(Precedex,AbbottLaboratories Ltd.NorthChicago
ABD,100/mL)intraperitoneally1hourbeforethe
tourni-quetrelease.Group4(D-100,n=7)hadundergonethesame
proceduresasintheGroup2,exceptforreceiving100g/kg
dexmedetomidine intraperitoneally1h before the
tourni-quetrelease.Againthebloodsampleswereobtainedatthe
1sthoursofthereperfusionwithblood andtissuesamples
attheendofthereperfusionfortheGroups3and4.
Anesthesia was performed using 50mg·kg−1 ketamine
(Pfizer Pharma GMBH, Germany) and 10mg·kg−1 xylazine
hydrochloride (Alfazine, 2%, Egevet) mixture applied
intraperitoneally.Ischemiawasperformedusingelastic
ban-dage(1cmwidthand30cmlength)appliedtotheinguinal
region of the left lower extremity. The tourniquet was
deflated to establish reperfusion after the certain period
oftime.Theenvironmenttemperaturewaskeptstableand
the operation table was heated to protectthe rats from
hypothermiaandthebodytemperatureswerekeptbetween
36.8◦Cand37.5◦C.Theratswerehydratedwith3mL/kg/h
isotonicsodiumchloride subcutaneouslythroughouttheIR
procedure toavoid dehydration. The subjects were
sacri-ficedaftertheobtainment ofsamplesofbloodandtissue.
Theproceduredurationswerekeptequalinallthegroups.
Attheendof the1sthourof3-hourreperfusionperiod
1.5mLbloodwasdrawnfromthetailveinoftheratsforthe
analysisofTNF-␣andIL-6, wereputintosteriletubewith
ethylenediaminetetraaceticacid(EDTA)andcentrifugedfor
10min with1200rpm speed.Plasma ofthe blood samples
wereseparatedputintoEppendorftubes,freezedandkept
at 70◦C until theanalysis day. The rats received isotonic
sodiumchlorideintraperitoneallyequaltotheamountlost
for sampling. At the end of the reperfusion thorax was
opened by subdiaphragmatic approach. Blood sample for
TNF-␣andIL-6analysiswasobtainedin2mLvolumedirectly
fromtheheartandwaskeptusingthesamemethodas
men-tionedabove.Attheendoftheprocedure5mLof10%formol
wasslowlyappliedthroughthecardiacapexvia20Gneedle
andheartandlungbedwereexcisedafterthesacrification.
Asectionfromthemiddlezoneoftherightlungandtheleft
lungtotallywereputinto10%formolandkeptfixedforat
least24h.
Analysisofinflammatorymediators
The analysis of inflammatory mediators (TNF-␣ vs. IL-6)
was performed via Enzyme-Linked Immunosorbent Assay
(ELISA).Absorbentvalueswerereadat450nmintheELISA
device(Organon TechnicaMicrowell SystemReader 230S).
Theresultswereexpressedinpg/mL.
Histopathologicalanalysis
Pulmonarytissuesobtainedfromthesubjectswerestained
using hematoxylin-eosin method and examined by light
microscope(OlympusBH-2) under200×magnification.Six
randomregions wereselected fromeach sample and 0---4
point scoring were made taking into account
histopatho-logical findings like alveolar and interstitial hemorrhage,
alveolarandinterstitialneutrophileinfiltration,edemaand
atelectasis.Scoringwasmadeaccordingtotheinjuredarea
proportionas0:noinjury,1:<25%injury,2:25---50%injury, 3:50---75%injury,4:diffuseinjury.
Statisticalanalysis
ThedataobtainedwasevaluatedusingSPSS11.0software
(Statistical Package for the Social Sciences, Chicago,
Illi-nois). Kruskall Wallis and Chi-square tests were used for
comparisonof thegroups. Mann---WhitneyUtest wasused
forcomparisonofthegroupsseparatelyandBonferroni
cor-rectionwasusedwhenneeded.p-Valueslessthan0.05were
consideredstatisticallysignificant.
Results
Thisstudywascompletedwith28rats,eachgroup
contain-ingseven.Thetimeintervalforthestudywasthesameas
indicatedinMethodssection(Fig.1).
Table1representsTNF-␣andIL-6valuesandhistological scoresofthepulmonarytissue.Intergroupanalysisrevealed nostatistically significant differenceregarding TNF-␣ and IL-6valuesneitherinthe1st,norinthe3rdhoursof reper-fusion.
Statistical analysis of the pulmonary injury
histologi-cal scores was made using median values of the scores
obtainedfrom6microscopicareasexamined.Therewas
sta-tisticallysignificantdifferenceamongthegroupsregarding pulmonaryinjuryscores(p=0.001).Therewasobserved
dif-fuseinjury (score4) inall the specimensof theGroup 2.
HistologicalscoresobtainedfromtheGroup2were
signifi-cantlydifferentfromtheGroups1,3and4withp-valuesof
0.001foreachcomparison.Moreover,Group1scoreswere
foundtobesignificantlydifferentfromtheGroups3and4
withp-valuesof0.001and0.011,respectively.Nosignificant
differencewasobservedbetweentheGroups3and4.
In the microscopical examination; samples from the
Group1demonstratednormalalveolarsequence,
Group 1 (SHAM)
∆
---
---
--- n=7
6. hour
4. hour
3. hour
0. hour
6. hour
4. hour
3. hour
0. hour
6. hour
4. hour
3. hour
2. hour
2. hour
0. hour
6. hour
4. hour
3. hour
0. hour
Histopathology
and Biochemistry
Biochemistry
Histopathology
and Biochemistry
Biochemistry
Histopathology
and Biochemistry
Biochemistry
Group 2 (IR)
ISCHEMIA
REPERFUSION
∆
---
---
--- n=7
Group 3 (D 50)
ISCHEMIA REPERFUSION
∆
---
---
--- n=7
Dexmedetomidine
50
µ
g/kg
Histopathology
and Biochemistry
Biochemistry
Dexmedetomidine
100
µ
g/kg
Group 4 (D 100)
ISCHEMIA
REPERFUSION
∆
---
---
--- n=7
Figure1 Schematicrepresentationofthestudyprotocol.
Figure2 Group1,normalstructureofventilatedpulmonary tissue.
SamplesfromtheGroup2showedinterstitialand
intraalve-olar neutrophile infiltration, hemorrhage, interalveolar
septalthickening, interstitial edema, diffuse
emphysema-tous areas and congestion. Large magnification revealed
mostly atelectatic areas and areas with capillary stasis
withdecreasedventilation,collapsedalveoli,nonfunctional
parenchymal areas, dense parenchymal neutrophile and
macrophageinfiltrationintheseregions,diffuse
intraalve-olar hemorrhage in the capillary stasis areas and patchy
fibrosisareastogetherwithsparsenormallyventilatedfields (Figs.3and4).SamplesfromtheGroup3demonstrated dif-fuseinterstitialneutrophileinfiltration;interalveolarseptal
thickening,atelectasis,congestion,hemorrhageand
emphy-semalessthanintheGroup2.Normalpulmonarytissuewas
observedattheneighboringareas,despitemild
parenchy-malenlargementandneutrophileinfiltration.Someregions
revealed normal pulmonary tissue together with intense
parenchymalhemorrhage,emphysematous areasand
Table1 TNF-␣andIL-6valuesandhistologicalscores.
Group1 (SHAM)
n=7
Group2 (IR)
n=7
Group3 (D50)
n=7
Group4 (D100)
n=7
p
TNF-˛(pg/mL)
Reperfusion1h 9.40 (7.40---11.50)
10.10 (9.10---25.30)
9.70 (8.30---10.90)
9.70 (7.70---10.60)
0.55
Reperfusion3h 9.30 (8.20---10.90)
9.80 (9.30---22.90)
10.20 (8.70---11.80)
9.00 (8.90---12.10)
0.26
IL-6(pg/mL)
Reperfusion1h 27.10 (21.60---41.30)
17.30 (13.20---52.60)
19.00 (15.80---58.00)
25.20 (20.00---48.90)
0.11
Reperfusion3h 32.70 (21.60---64.70)
61.20
(17.40---120.30)
24.40 (14.00---91.80)
31.80 (21.40---47.70)
0.83
Histologicalscore 0.5b
(0.0---1.0)
4.0a
(4.0---4.0)
2.5 (2.0---3.0)
2.0 (0.5---3.5)
0.001
a SignificantdifferenceintheGroup2comparedwiththeGroups1,3and4,p<0.05. b SignificantdifferenceintheGroup1comparedwiththeGroups3and4,p<0.05.
Thevaluesarerepresentedinmedian(minimum---maximum).
Figure3 Group2,alveolarstructurehaslostitspattern(↑), emphysematous changes (A), parenchymal inflammatory cell infiltration(P˙I).
4 demonstrated mild interstitial neutrophile infiltration,
interalveolarseptalthickening,atelectasis,congestionand
hemorrhagetoa muchlesserextentthan inthe Group 2.
Someregionsrevealedcompletelynormalpulmonarytissue
(Fig.6).
Discussion
The main outcome of the study was that,
dexmedetomi-dinedecreasedhistologicalinjuryscoresrelatedtoIRinrats
experiencingischemiaandreperfusion,thatwasgenerated
by extremitytourniquet application. Although therewere
notobserveddifferencesamongthegroupsasregardsblood
inflammatorymediatorsTNF-␣andIL-6, therewere
signif-icant differenceregardinghistologicalappearancesof the
tissues.HistologicalscoresoftheGroup2werefoundtobe
high,indicatingtheeffectsoftheIRinjurytothepulmonary
Figure4 Group 2,denseneutrophileinfiltration, parenchy-mal enlargement, non-ventilated pulmonary areas ( ) and atelectaticareas(A).
Figure6 Group4,mildinflammatoryinfiltrationand thick-enedinteralveolarseptum(*)togetherwithnormalpulmonary tissue.
tissue.Groups 3and 4 demonstratedlower injury scores,
indicatingprotectiveeffectofdexmedetomidineagainstIRI.
Although some authors offer multiple ligation method
instead of tourniquet application because of the concern
ofvenous and lymphatic obstruction, muscle,nerve
dam-ageafterprolongedmechanical compression,17 tourniquet
methodisnon-invasiveand seemstobemore practicalin
theclinicalapplication.7,18
Different ischemia and reperfusion times had been
usedfor IRcreation in the literature. We had taken into
account resistance of the tissue against ischemia in our
study. For instance, prominent morphological changes in
the muscle tissue appear after 2h of ischemia and so,
thestudiesdealingwithmuscleIRIhadusedlongischemia
periods.19,20Importantcorrelationbetweenischemiaperiod
and ischemic injury was found.21 Taking into account
thattherehadbeen demonstratedirreversiblehistological
injury20 anddiffuseneutrophileinfiltration18 inthemuscle tissueafter3hofischemiaperiodinthestudiesdealingwith
IRIinthemuscle,wehadchosenourischemiaperiodtobe
3hinthestudy.
Reperfusionperiodalsowasfoundtobeanimportant
fac-torintheformationoflocalanddistanteffectsofIR.2,7,19
Yasin et al.7 had used different reperfusion times after
3hischemiaandfoundpositivecorrelationbetween
reper-fusionperiodanddistantorgandysfunctions.Theyhadalso
demonstratedhistological changes after the 3h of
reper-fusion,thatwerenotapparentinthefirst2h.On account
ofthiswehadchosenthereperfusiontimetobe3h. Promi-nenthistologicalchanges,asdiffuseneutrophileinfiltration,
alveolarsequencedistortion,edema,inthepulmonary
tis-sueoftheIRgrouphadsupportedourchoice.Thesefindings
were coherentwith the studies that usedthe same time
periods.7,18
TNF-␣ was shown to play an important role in the
pathogenesisofSystemicInflammatoryResponseSyndrome
(SIRS)andMultipleOrganFailure(MOF).5,22,23Similar
mech-anisms weresuggested in the localand distanteffects of
IRIandstudiesconductedhadshownTNF-␣toplayrolein
theorgandamagepathogenesis.3,7 Similarly, IL-6alsowas
showntoplayroleincomplexinflammatoryreactionrelated
totrauma,shock andinfection.24 Positive correlation was
demonstrated between plasma IL-6 concentrations and
magnitudeofsofttissuedamage.24IL-6levelswereshownto increaseincorrelationwithTNF-␣inthestudiesdealingwith
lower extremity IRmodels.5,6 Yasin etal.7 had suggested
that IRrelated inflammatoryresponse can beshown with
serumTNF-␣andIL-6levelsandthatthereispositive corre-lationbetweenthisincreaseanddistantorganinjuries.They hadevaluatedbloodTNF-␣andIL-6levelsatthe1st,2ndand
3rdhoursofreperfusionafter3-hourischemiaperiod.
TNF-␣wasfoundtoincreasesignificantlyattheendofthe1st
hourandreturntocontrolvaluesatthe2ndhour;whereas
IL-6wasfoundtoincreaseprogressivelyafterthe1sthour
ofreperfusionwithpeakattheendofthe3rdhour.Hence,
we hadevaluatedblood TNF-␣andIL-6levelsbothat the
endofthe1stand3rdhours.
There have been conducted many clinical and
experi-mentalstudieswithdexmedetomidineasitshowsanalgesic,
anxiolytic and sedative properties alltogether.25,26
More-over, it has been shown that dexmedetomidine possesses
antiinflammatory properties in the studies investigating
its effects in ischemic and toxic inflammatory models.11
Taniguchi et al.11 have demonstrated that
dexmedetomi-dinealleviateslunginjuryanddecreasesmortalityratesby
decreasing TNF-␣ and IL-6levels and neutrophile
infiltra-tioninthealveolarwallsintheexperimentalendotoxemic
septicshock model.Shen etal.27 haveinvestigatedTNF-␣
andIL-6levelsinlunginjurycausedbyexperimental
intesti-nal IRI model and demonstrated decreased production of
thesecytokinesinpulmonarytissueafterdexmedetomidine
administration.
Dexmedetomidine has been used via intraperitoneal
route before28 or during12---14 IRin ratIRmodels.Although
dexmedetomidine’s protective effects had been shown
regardless of its time of administration, there are
no studies in the literature comparing its application
periods.Furthermore,somestudiesinvestigatingtheeffects
of intraperitoneally administered dexmedetomidine have
shown that, IRperiods were notlonger than the
elimina-tiontimeofdexmedetomidine.13,28Takingintoconsideration thatthemainculpritintheformationoflunginjuryis
reper-fusion process, and that TNF-␣ levels begin to rise near
the end of the ischemiawith peaklevels at the 1st hour
ofreperfusion,7itwasrelevanttoapplydexmedetomidine
1hourbeforethereperfusion.
We have not come across certain dose intervals
of dexmedetomidine for its antiinflammatory effects in
the literature. The dose for dexmedetomidine, applied
intraperitoneally, wasdecided tobe 100g/kg, a highest
dose safely applied in the current literature,16,28 and the
second dose was decided to be 50g/kg, to evaluate its
possibledosedependenteffects.
Despite similar IR periods in the studies regarding rat
pulmonaryIRIafterextremitytourniquetapplication, differ-entresultsregardingTNF-␣levelshavebeenobserved.5,18,29
Seekampetal.5havedemonstratedthatTNF-␣levelswere
notdetectableinthebloodthroughoutthe4-hourischemia
period, but started torise at the 1st hour of reperfusion
with decline after the 2nd hour. In addition, IL-6 levels
started to rise at the 30th minute with peak at the end
of the 4th hour. Yassin et al.7 have stated that, TNF-␣
and IL-6levelsreachtheir peaklevelsat the 1st and3rd
hoursofreperfusion,respectively;TNF-␣levelsdropbelow
IL-6reachdetectablelevelsinplasmafromthe1sthourof reperfusion.
Duru etal.,18 Harkin etal.,30 Gaines etal.31 haveused
similar IR models and time periods; despite they have
demonstrated histopathological changes due to IR injury,
theycouldnotobservechangesinTNF-␣levels.Similarly,
Welbourn et al.29 could not observe TNF-␣ level changes
after reperfusion; they have concluded that TNF-␣ had
role in the IRI pathogenesis as histopathological changes
decreasedwiththeapplicationofanti-TNFserum.Wehave
alsofoundnodifferencesintheTNF-␣andIL-6levelsinthe
dexmedetomidineappliedgroups,comparedtoSHAMgroup,
despitesignificanthistopathologicaldifferences.This
condi-tionmaybeattributedtoinsufficientnumberof subjects.
Duruetal.18havestatedthat,thereasontheycouldnothave
demonstratedcytokine levelchanges wasthattheymight
havesparedTNF-␣peaklevels,astheyobtainedblood
sam-plesattheendofthe2ndhourofreperfusion.Gainesetal.31
attributedthistothebloodsampleinsufficiency.Welbourn
etal.29haveproposedthatTNF-␣canstayinthetissueafter
productioninthepulmonarymacrophagesandsocouldnot
alwaysbedetectedintheblood;itcanmediatepulmonary
tissueinjuryactivatingendotheliumlocally.
IRI generated bythetourniquet modelwas
histopatho-logically demonstrated in this study. The changes in the
IRgroupweresignificant comparedtotheSHAMandboth
dexmedetomidinegroups, andthisverifiedthatthemodel
wasappropriatelyconducted.Significantdifferencesinthe
findings in the dexmedetomidine groups comparedto the
IR group was interpreted as that dexmedetomidine had
decreasedpulmonaryinjury.
Although histopathological scores between the groups
withdexmedetomidine 50 and100g/kg were not
signif-icantly different, some normal pulmonary tissue areas in
themicroscopicalexaminationintheD100groupsuggested
thatthedrugmighthaveactedindosedependentmanner.
Studieswithlargersamplesizeswithdifferentdoses,
admin-istrationtimeandroutesmaybeconductedtoevaluatethis
effect.
Nolimitationsforthestudywereencountered.
In conclusion, in our experimental study of lower
extremitytourniquetinduced IRmodel,dexmedetomidine
was effective in preventing the IR induced lung injury.
Histopathological and IL-6 level differences between the
two groups with different doses of dexmedetomidine,
although not statistically significant, suggests to conduct
studieswithlargersample sizestoevaluatetheeffectsof
differentdoses.
Implication
statement
This experimental study demonstrates the ability of
dexmedetomidine to reduce experimental
ischemia---reperfusionrelatedinjuryin rats.Controlledtrials canbe
conductedinhumantoobservetheclinicalsignificanceof
thiseffect.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
References
1.CerraFB, LajosTZ,MontesM,etal.Hemorrhagicinfarction: areperfusion injuryfollowingprolonged myocardialischemic anoxia.Surgery.1975;78:95---104.
2.WelbournCR,GoldmanG,PatersonIS,etal.Pathophysiologyof ischaemiareperfusioninjury:centralroleoftheneutrophil.Br JSurg.1991;78:651---5.
3.Grace PA. Ischaemia---reperfusion injury. Br J Surg. 1994;81:637---47.
4.VilcekJ.Thecytokines:anoverview.In:ThomsonAW,editor. TheCytokineHandbook,vol.1,4thed.London:ElsevierScience AcademicPress;2003.p.3---18.
5.Seekamp A, Mulligan MS, Till GO, et al. Requirements for tumor necrosis factor-alpha and interleukin-1 in limb ischemia/reperfusion injuryand associatedlunginjury.AmJ Pathol.1993;143:453---63.
6.SeekampA,TillGO,MulliganMS,etal.Roleofselectinsinlocal and remotetissueinjury followingischemiaand reperfusion. AmJPathol.1994;144:592---8.
7.Yassin MM, Barros D’Sa AA, Parks G, et al. Lower limb ischemia---reperfusion injury triggers a systemic inflamma-toryresponse and multipleorgandysfunction. World JSurg. 2002;26:115---21.
8.MaesM,LinA,KenisG,etal.Theeffectsofnoradrenalineand alpha-2adrenoceptoragentsontheproductionofmonocytic products.PsychiatryRes.2000;96:245---53.
9.VennRM,BryantA,HallGM,etal.PreliminaryUKexperience ofdexmedetomidineanovelagentforpostoperativesedation intheintensivecareunit.Anaesthesia.1999;54:1136---42. 10.Bhana N, Goa KL, McClellan KJ. Dexmedetomidine. Drugs.
2000;59:263---70.
11.Taniguchi T, Kidani Y, Kanakura H, et al. Effects of dexmedetomidine on mortality rate and inflammatory responsestoendotoxin-inducedshockinrats.CritCareMed. 2004;32:1322---6.
12.JolkkonenJ,PuurunenK,KoistinahoJ,etal.Neuroprotection bythealpha2-adrenoceptoragonist,dexmedetomidine,inrat focalcerebralischemia.EurJPharmacol.1999;372:31---6. 13.EserO,FidanH,SahinO,etal.Theinfluenceof
dexmedeto-midine on ischemic rat hippocampus. Brain Res. 2008;1218: 250---6.
14.Yagmurdur H, Ozcan N, Dokumaci F, et al. Dexmedetomi-dinereducestheischemia---reperfusion injurymarkersduring upper extremity surgery with tourniquet. J Hand Surg Am. 2008;33:941---7.
15.YangCL,Tsai PS,Huang CJ. Effects ofdexmedetomidine on regulatingpulmonaryinflammationinaratmodelof ventilator-induced lung injury. Acta Anaesthesiol Taiwan. 2008;46: 151---9.
16.Kocoglu H, OzturkH,Ozturk H,et al. Effect of dexmedeto-midine on ischemia---reperfusion injury in rat kidney: a histopathologicstudy.RenFail.2009;31:70---4.
17.Tassiopoulos AP, Carlin RE, Gao Y, et al. Role of nitric oxide and tumor necrosis factor on lung injury caused by ischemia/reperfusion of the lower extremities. J Vasc Surg. 1997;26:647---56.
18.Duru S, Koca U, Öztekin S, et al. Antithrombin III pre-treatmentreduces neutrophil recruitment into thelung and skeletal muscle tissues in the rat model of bilateral lower limband reperfusion:apilotstudy.ActaAnaesthesiolScand. 2005;49:1142---8.
19.KhalilAA,AzizFA,HallJC.Reperfusioninjury.PlastReconstr Surg.2006;117:1024---33.
21.Petrasek PF, Homer-Vanniasinkam S, Walker PM. Determi-nants of ischemic injury to skeletal muscle. J Vasc Surg. 1994;19:623---31.
22.Seal JB, Gewertz BL. Vascular dysfunction in ischemia---reperfusioninjury.AnnVascSurg.2005;19:572---84.
23.YaoYM,ShengZY,YuY,etal.Thepotentialetiologicroleof tumornecrosisfactorinmediatingmultipleorgandysfunction inratsfollowingintestinalischemia---reperfusioninjury. Resus-citation.1995;29:157---68.
24.RoumenRM,HendriksT,vanderVen-JongeKJ,etal.Cytokine patternsinpatientsaftermajorvascularsurgery,hemorrhagic shock,andsevereblunttrauma.Relationwithsubsequentadult respiratorydistress syndromeandmultipleorganfailure.Ann Surg.1993;218:769---76.
25.Koroglu A, Demirbilek S, Teksan H, et al. Sedative, haemodynamicandrespiratoryeffectsofdexmedetomidinein childrenundergoingmagneticresonanceimagingexamination: preliminaryresults.BrJAnaesth.2005;94:821---4.
26.Arain SR, Ruehlow RM, Uhrich TD, et al. The efficacy of dexmedetomidine versus morphine for postoperative
analgesiaaftermajorinpatientsurgery.AnesthAnalg.2004;98: 153---8.
27.Shen J, Fu G, Jiang L, et al. Effect of dexmedeto-midine pretreatment on lung injury following intestinal ischemia---reperfusion.ExpTherMed.2013;6:1359---64. 28.Engelhard K, Werner C, Eberspacher E, et al. The effect
of the alpha 2-agonist dexmedetomidine and the N-methyl-d-aspartate antagonist S(+)-ketamine on the expression of apoptosis-regulating proteins after incomplete cerebral ischemia and reperfusion in rats. Anesth Analg. 2003;96: 524---31.
29.WelbournR,Goldman G,O’RiordainM,etal.Rolefor tumor necrosisfactorasmediatoroflunginjuryfollowinglowertorso ischemia.JApplPhysiol.1991;70:2645---9.
30.HarkinDW,BarrosD’SaAA, McCallionK,etal.Ischemic pre-conditioningbeforelowerlimbischemia---reperfusionprotects againstacutelunginjury.JVascSurg.2002;35:1264---73. 31.GainesGC,WelbornMB3rd,Moldawer LL,etal.Attenuation