B
r
IE
F
CO
M
M
U
N
IC
A
T
IO
Quality of sputum in the performance of polymerase
chain reaction for diagnosis of pulmonary tuberculosis
Authors
RosemeriMauricida Silva1
MariaLuizaBazzo2 MarianaChagas3 1Pneumologist,Master inMedicalSciencesand DoctorinPneumology. ProfessoroftheMedical SchooloftheUniversidade FederaldeSantaCatarina andUniversidadedo SuldeSantaCatarina. Coordinatorofthe ProgramofMaster’s DegreeinHealthSciences oftheUniversidadedoSul deSantaCatarina. 2DoctorinMicrobiology andProfessorofthe UniversidadeFederalde SantaCatarina. 3MasterinPharmacy, UniversidadeFederalde SantaCatarina.
Submittedon:08/19/2009 Approvedon:11/29/2009 Correspondence to: Dra.RosemeriMauricida Silva-RuaMoçambique, 852,RioVermelho, Florianópolis–SC CEP:88060415 Email:rosemaurici@ gmail.com Wedeclarenoconflict ofinterest.
INTRODUCTION
Pulmonary tuberculosis, despite of all knowledgegatheredonitspathogenesis,epi-demiology, and therapeutics over the years, remainsanimportantpublichealthproblem in Brazil and other developing countries. Therefore, implementation of newer diag- nosticmethodologiesandtherapeuticmeas-uresarefundamentalstepsforthereduction of its morbidity and mortality among the patients and for stopping its transmission chainwithinthecommunity.1
Presently, the identification of Myco-bacterium species relies on lengthy cultures and biochemical tests. Although molecular testsareavailablecommercially,theyarere-stricted to certain types of patient samples or the species ofMycobacterium isolated in culture.2
Patientswithfewbacillidependstrongly onthesputumcultureforthedefinitivedi-agnosis,whichtakesonaveragethreetosix weeks to be accomplished.3 Hence, faster alternative techniques are desirable, and amongthem,thepolymerasechainreaction (PCR)seemstobethemostpromising.
PCRhaspopularizedtheuseofmolecu-larbiologytechniquesinclinicallaboratories for diagnosing many infectious diseases.4
However,theperformanceofthistechnique depends considerably on the quality of the samplesexamined.Therefore,itwouldbeof uttermostimportancetoknowtheinfluence ofthesamplequalityinitsperformance,as well as determining criteria for acceptabil-ityofthesamplesinthediagnosisusingthis technique.
ABSTRACT
Setting:
fasteralternativetechniquesarerequiredtoimprovethediagnosisandcontrolofpul-monary tuberculosis.Objective: To evaluate the sample quality in the performance of PCR fordiagnosisofpulmonarytuberculosis.Method: duringoneyear,sputumsampleswerecol-lectedfrom72pulmonarytuberculosispatientsand12non-tuberculosiscontrols,whichwere admittedtotheNereuRamoshospital,Florianópoliscity,Brazil.Thesamplesweresubjected to Ziehl-Neelsen-stained sputum smear microscopy and Lowestein-Jensen medium culture, which were defined as gold standard tests for mycobacteria, and polymerase chain reaction (PCR).Thosesamplesthatpresentedmorethan40%ofviablecellsandlessthan25%ofepi-thelialcellsweredefinedashighqualitysamples.Results:PCRshowedsensitivityof55.6%, specificity of 41.7%, positive predictive value of 85.1%, negative predictive value of 13.5%, andaccuracyof53.6%.Highqualitysamplesshowedsensitivityof72.4%,specificityof50%, positivepredictivevalueof91.3%,negativepredictivevalueof20%,andaccuracyof69.7%. Lowqualitysamplesshowedsensitivityof44.2%,specificityof37.5%,positivepredictivevalue of79.2%,negativepredictivevalueof11.1%,andaccuracyof43.1%.Conclusion:useofhigh quality samples improved significantly the PCR performance, especially on their sensitivity andpositivepredictivevalues.
Keywords:tuberculosis,sputum,polymerasechainreaction.
Silva,Bazzo,Chagas
Polymerase Chain Reaction – PCR
DNAwasextractedbythealkalinelysismethod.4
Brief-ly,thesputumwassuspendedinGTE(Glucose50mM, 10mMEDTA,Tris/ClPH8.0,025mM),followedby cell lysis with SDS 1 %/NaOH 0.2 M. The suspension wasneutralizedwithpotassiumacetate3MpH4.8-5.0. ProteinaseK20mg/mLwasthenaddedtothesuspen-sionandDNAwasextractedwithphenol/chloroform/ isoamyl alcohol (25:24:1). The suspension was then treatedwithethanolplussodiumchlorideandcentri-fuged.Thesedimentwasre-suspendedin20μLofTE (10mM Tris pH 7.4, 1 mM EDTA) and kept at -20° C untiluse.
Theprimeranti-senseMYC-264andtheprimersense F-285,whichamplifya1027pairfragmentofgene16S rDNAfrommycobacteria,wereusedinthePCR.6,7The following conditions were met: 94° C for one minute, 60°Cforoneminute,35cyclesofoneminuteat72°C, and one final cycle of 94° C for one minute, 60° C for oneminuteand72°Cfortenminutes.Theamplification products were electrophoresed on a 1% (w/v) agarose gel, stained by ethidium bromide (1 μg/mL) and pho-tographed under 320ηm ultra-violet light (HOEFER- MacroVue UV-20), using a gel photodocumentation (DOC-PRINT®Biosystems).Theirapproximatesizewas determinedbycomparingitwith100pbmolecularsize standard(Invitrogen).
Positive controls included DNA from Calmette-Guérin bacillus (BCG) or Mycobacterium avium (ATCC-25291); negative controls included DNA from Escherichia coli (ATCC-25922) or pure water. As ad-ditionalcontrol,aPCRamplificationofAFB-negative sampleswasdonewithprimersspecificforeubacteria ZR-244eF-285.7
STUDY POPULATION AND METHODS
Duringoneyear,72pulmonarytuberculosisinpatients of hospital Nereu Ramos, Florianópolis city, Brazil, had their sputum evaluated. In addition, twelve non-tuberculosisinpatientswereusedascontrols.Thestudy was approved by the Human Ethic Committee of Uni-versity of South of Santa Catarina, under the number 05.458.4.01.III.
The samples were collected in the morning, before breakfast,andsentassoonaspossibletothelaboratory. Theyweresubjectedtosmearandcultureformycobac- teria(bothusedasgoldstandard),andtoPCRformy-cobacteria.
Sputum smear
The sputum smears were stained by the Ziehl-Neelsen techniqueandexaminedaccordingtotheguidelinesofthe World Health Organization.5 Briefly, heat-fixed sputum wasstainedwithhotcarbolfuchsin,decolorizedwithacid alcoholandthencounterstainedwithmethyleneblue.
Culture of mycobacteria in Löwenstein-Jensen (LJ) medium
The samples were subjected to culture according the Petroff protocol.5 Briefly, the samples were mixed with NaOH 4% (v/v), thoroughly shaken, and incubated for 30 minutes at 35°-37° C. Then, sterile distilled water (v/v) was added to the sample and the suspension was neutralizedwith1NHCl,containing0.004%ofphenol red.Thesuspensionwasthencentrifugedat3,000xgfor 20minutes,andthesedimentwasresuspendedin500μL ofsaline.Ahundredmicrolitersofthesedimentwasthen inoculatedontotwoLJmediumslopes.Thetubeswere incubatedat35°-37°Cforuptoeightweeks,whenthe tubeswithnogrowthwerediscardedasnegative.
Table 1. Results of PCR for high and low quality samples
Pulmonary TB Samples Control Samples
High quality low quality High quality low quality Total
n(%) n(%) n(%) n(%)
PCR (+) 21(25) 19(22.6) 2(2.4) 5(5.9) 47(56)
PCR (-) 8(9.5) 24(28.6) 2(2.4) 3(3.6) 37(44)
Quality of sputum samples
High quality samples were defined as those with more than40%ofviablecellsandlessthan25%ofepithelial cells.Theviabilityofcellsandthepercentageofepithe-lial cells were determined according to Pizzichiniet al. andLeeet al.,respectively.8,9
Performance of PCR
Sensitivity,specificity,positivepredictivevalue,negative predictivevalue,andaccuracyofPCRwerecalculatedby thesoftwareSPSS16.0®,usingtheresultsofcultureand sputumsmearasgoldstandard.
RESULTS
Thirty-threesamples(39.3%)wereofhighquality,while fifty-onesamples(60.7%)wereoflowquality.PCRwas positivein47(56%)patientsandnegativein37(44%) patients.Table1showstheresultsofthePCRinhighand lowqualitysamples,respectively.
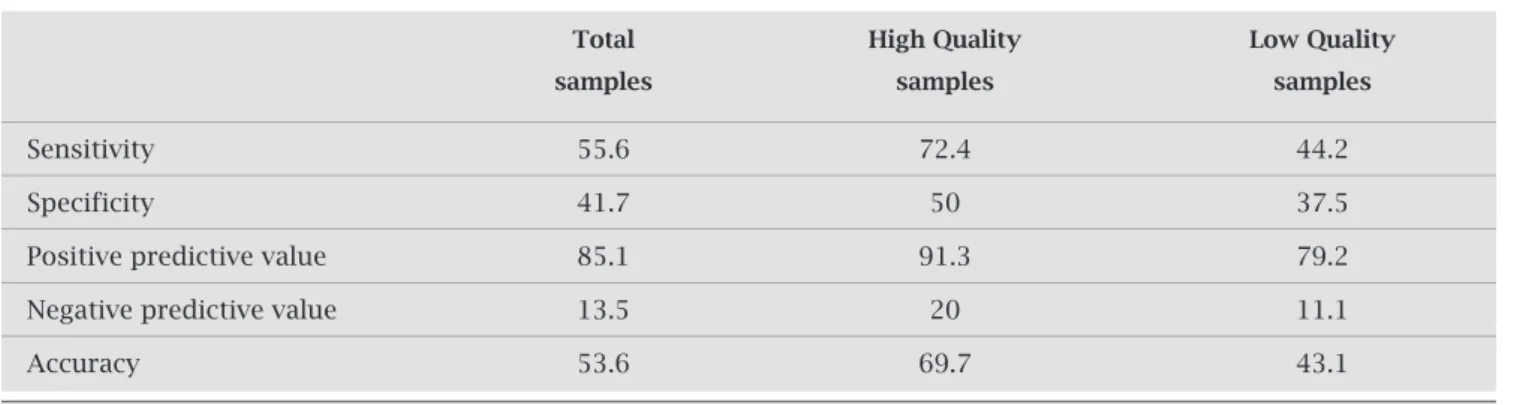
Whenallsamplesweretestedtogether,PCRshowed sensitivityof55.6%,specificityof41.7%,positivepredic-tivevalueof85.1%,negativepredictivevalueof13.5%,and accuracyof53.6%.Insamplesofhighquality,PCRshowed asensitivityof72.4%,specificity50%,positivepredictive valueof91.3%,negativepredictivevalueof20%,andac-curacyof69.7%.Insamplesoflowquality,PCRshoweda sensitivityof44.2%,specificityof37.5%,positivepredic-tivevalueof79.2%,negativepredictivevalueof11.1%,and accuracyof43.1%(Table2).
DISCUSSION
Theresultsofthisstudyshowthatthequalityofthespu-tuminfluencessignificantlytheperformanceofPCRfor the diagnosis of pulmonary tuberculosis. The selection ofsamplesofhighqualityresultedinanimprovedPCR,
especially when the sensitivity and positive predictive valueparameterswheretakenintoaccount.Highquality samplespresentedsensitivitysimilartothatfoundinto another study of clinical samples, which used primers specificfortheIS6110regionofM. Tuberculosis.10
Low quality sputum can represent a problem in the dailydiagnosisroutine.Atleast25%ofsputumsamples sent to laboratories for culture may not be adequate, sincesomeofthemaresometimesheavilycontaminated withsaliva,leadingtogreatvariabilityinresultsandlow reliability.11,12
PCR assay reduces the time for diagnosis and may increase the detection of mycobacteria in samples with negativesmearresults.However,variationsintheproce- duresofin-housePCRcouldexplainthewidelyvariabil-ity of the sensitivduresofin-housePCRcouldexplainthewidelyvariabil-ity and specificduresofin-housePCRcouldexplainthewidelyvariabil-ity reported in several studies.13,14,15
Theinfluenceofrespiratorytractmicrobiotaonthe performance of PCR remains disputable. According to someauthors,fungiandbacteriafromthesesitescanaf-fecttheresultsofPCRfromsputum.16However,others have reported high PCR sensitivity and specificity for tuberculosisdiagnosis,despitethefactthatthesamples wereclearlycontaminatedwiththesemicroorganisms.17
Inourstudy,weutilizedonlyonesampleforthesame sputum. However, we could change this protocol, since some authors suggest that the sensitivity could be in-creasediftheassaycouldbedonewithmoresamplesfor thesamesputum.18,19
When testing the samples, we were not able to dif- ferentiateamongdifferentspeciesofMycobacteriumbe-causetheamplifiedregionisconservedinallspeciesof thegenus.Unlikeotherregionsamplified,16SrDNAex-pressesitselfinfewercopiesthantheIS6110sequences, but its amplification allows the rapid identification of subtypes by heteroduplex technique, which is in agree-mentwiththeobjectivesofthisstudy.20,21,22
Table 2. Performance of PCR for high quality and low quality samples
Total High Quality low Quality
samples samples samples
Sensitivity 55.6 72.4 44.2
Specificity 41.7 50 37.5
Positive predictive value 85.1 91.3 79.2
Negative predictive value 13.5 20 11.1
Besidestheamplifiedregion,otherfactorssuchasthe amountofbacillicaninfluencetheperformanceofPCR. Inthisregard,Wuet al,usingnested-PRAforhsp65gene, identified100%ofthesampleswith3+ofbacilli,95%of sampleswith2+bacilli,andonly53%ofsampleswith 1+orlessbacilli.23
Thefactthatthisstudyusedsputuminsteadofcul- turemayhavecontributedtolowerresultsthanthosere-ported in the literature. However, the purpose of using sputum was an attempt to improve the technique effi- ciencyinthistypeofsamplebyspeedingupthediagno-siswithouttheneedfortheculture.
CONCLUSION
Our results indicate that selection of samples of high quality resulted in an improvement in performance of PCR for the diagnosis of pulmonary TB, especially re-garding its sensitivity and positive predictive value pa-rameters.
ACKNOWLEDGMENTS
ThisworkwassupportedbyFundaçãodeApoioàPesqui-saCientíficaeTecnológicadoEstadodeSantaCatarina (FAPESC,grant771_911584).
REFERENCES
1. StopTBPartnershipandWHO.AmsterdamDeclarationto Stop TB, 2000 (www.stoptb.org/stop_tb_initiative/assets/ documents/decla.pdf,accessedinNovember2008). 2. Yeboah-Manu D,Yates MD, Wilson SM. Application of a
simple multiplex PCR to aid in routine work of the My-cobacterium reference laboratory. J Clin Microbiol 2001; 39:4166-8.
3. GallinaM,TroupiotiP,RoccoG,SensalariG,LibanoriE. PredictingcultureresultsforMycobacteriumtuberculosis complex:amplifiedMycobacteriumtuberculosisdirecttest andacid-fastbacillimicroscopy.Chest2000;118:28-32. 4. SambrookJ,RussellDW,SambrookJ.MolecularCloning:a
LaboratoryManual,3rded.NewYork:ColdSpringHarbor LaboratoryPress,2001.3vol.
5. WHO/TB/2003.320 - WHO/CDS/CSR/RMD/2003.3.
Guidelines for surveillance of drug resistance in tubercu-losis.2nded.Editedby:AzizMA,LaszloA,RaviglioneM, Rieder H, Espinal M, Wright A. World Health Organiza-tion.Geneva:2003.
6. BöddinghausB,RogallT,FlorhrT,BlockerH,BottgerEC. Detectionandidentificationofmycobacteriabyamplifica-tionofrRNA.JClinMicrobiol1990;28:1751-59.
7. RogallT,FlohrT,BottgerEC.DifferentiationofMycobac-terium species by direct sequencing of amplified DNA. J GenMicrob1990;136:1915-20.
8. Pizzichini E, Pizzichini MMM, Efhtimiadis A, Hargreave FE, Dolovich J. Measurement of inflammatory indices in induced sputum: effects of selection of sputum to mini-mize salivary contamination. Eur Respir J 1996; 9:1174-80.
9. LeeGR,BithelTC,FoersterJ,AthensJW,LukensJN.He-matologia Clínica de Wintrobe. São Paulo: Ed. Manole, 1998.
10. Araj GF, Talhouk RS, Itani LY, JaberW, Jamaleddine GW.
ComparativeperformanceofPCR-basedassayversusmi-croscopyandculturefordirectdetectionofM. tuberculosis
in clinical specimens in Lebanon. Int J Tuberc Lung Dis. 2000;4:877-81.
11. Skerrett JS. Diagnostic testing for community-acquired pneumonia.ClinChestMed1999;20:531-48.
12. ChuardC,FracheboudD,RegameyC.Effectofsputumin-duction by hypertonic saline on specimen quality. Diagn MicrobiolInfectDis2001;39:211-4.
13. Flores LL, Pai M, Colfors JR, Riley LW. In-house nucleic acid amplification tests for the detection of Mycobacte-rium tuberculosis in sputum species: meta-analysis and meta-regression.BMCMicrobiol2005;5:55.
14. Sarmiento OL, Weigle KA, Alexander J, Weber DJ, Miller WC.Assessmentbymeta-analysesofPCRfordiagnosisof smear-negative pulmonary tuberculosis. J Clin Microbiol 2003;41:3233-40.
15. AssisNCS,LopesML,CardosoNC,CostaMM,SouzaCO, LimaKVB.Diagnósticomoleculardatuberculosepulmo-nar.JBrasPatolMedLab2007;43:1-7.
16. SantosRMC,OguskuMM,MirandaJM,DosSantosMC, SalemJI.Avaliaçãodareaçãoemcadeiadapolimeraseno diagnósticodatuberculosepulmonarempacientesindíge-nasenãoindígenas.JBrasPneumol2006;32:234-40. 17. Lima DM, Bollela VR, Jácomo BJT, Martinez R, Fonseca
BAL.IdentificationofMycobacteriumspeciesincontami-natedculturesbypolimerasechainreaction.CHEST2005; 127:1283-8.
18. Kivihya-NduggaL,VanCleeffM,JumaEet al.Comparison
ofPCRwiththeroutineprocedurefordiagnosisoftuber- culosisonapopulationwithhighprevalenceoftuberculo-sis and human immunodeficiency virus. J Clin Microbiol 2004;42:1012-5.
19. WijengaertSV,DedisteA,GerardM,VandenbergO,Zissis G.Criticalnucleicacidamplificationtechniquestotestfor Mycobacteriumtuberculosisinrespiratorytractsamples.J ClinMicrobiol2004;42:837-8.
20. Tortoli E. Impact of genotypic studies on Mycobacterial taxonomy:thenewMycobacteriaofthe1990s.ClinMicro-biolRev2003;16:319-54.
21. Waléria-AleixoA,KroonEG,CamposMAS,Marguti-Pinto ME, Bonjardim CA, Ferreira PC. Heteroduplex Mobility AssayforRapid,SensitiveandSpecificDetectionofMyco-bacteria.DiagMicrobiolInfectDis2000;36:225-35. 22.
BazzoML.Métododeidentificaçãoecaracterizaçãodemi-cobactérias para uso em diagnóstico de rotina nos labo- ratóriosdesaúdeedeterminaçãodaresistência.PhDThe-sis. Institute of Biological Sciences, Federal University of MinasGerais,Brazil,2006.