Caring for the future: decrease in infant mortality in Maranhão State
Texto
Imagem
Documentos relacionados
To describe the historical evolution of the infant mortality rate and the infant mortality rate for diseases of the perinatal period and those of neonatal mortality by birth weight
Ao Dr Oliver Duenisch pelos contatos feitos e orientação de língua estrangeira Ao Dr Agenor Maccari pela ajuda na viabilização da área do experimento de campo Ao Dr Rudi Arno
Neste trabalho o objetivo central foi a ampliação e adequação do procedimento e programa computacional baseado no programa comercial MSC.PATRAN, para a geração automática de modelos
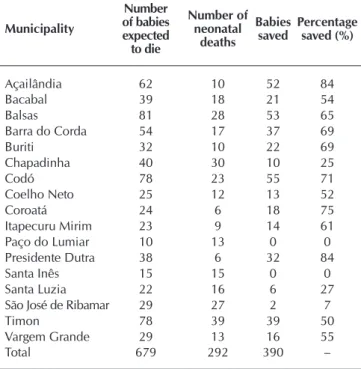
Objetivo: Relatar a experiência e atendimento realizado pelo Programa “Cuidando do futuro” para redução da mortalidade infantil em 17 municípios do Maranhão, numa proposta
Para que as funções maternas e paternas ocorram em condições suficientemente boas, Winnicott (1983) preconiza a importância do equilíbrio do meio ambiente onde a criança es- tá
Among less exalted circles, I myself detect an increasingly alarming dissonance between the language of devotion, doctrine and liturgy and the way people really
Finally, this thesis addresses the implications of a high dimensionality not only “by columns”, in form of nonlinear decision functions, by “by rows” as well, which would
Para tanto foi realizada uma pesquisa descritiva, utilizando-se da pesquisa documental, na Secretaria Nacional de Esporte de Alto Rendimento do Ministério do Esporte
