1
Universidade de Lisboa
Faculdade de Medicina de Lisboa
Clinical implications of cerebral age-related white matter cerebral changes
Ana Isabel Figueira Verdelho
Dissertation supervised by Prof. Doutor José M. Ferro
PhD in Medicine
Speciality in Neurology
The contents and opinions expressed in this manuscript are the full responsibility of the author. The Medical School of Lisbon has no responsibility for the contents.
2
A impressão desta dissertação foi aprovada pelo Conselho Científico da
Faculdade de Medicina de Lisboa em reunião de 25 de Setembro de 2012.
3
AGRADECIMENTOS
O trabalho que se apresenta a discussão só foi possível graças ao apoio de muitos, que em diversos momentos se cruzaram no meu percurso.
Alguns deles foram imprescindíveis, e aqui lhes deixo uma nota de agradecimento. Muitos outros ficarão por citar.
Devo salientar em primeiro lugar o Prof. Dr. José Ferro, meu orientador, que tanto incentivou a minha vontade de investigar, desafiando-me sempre para ir mais longe e exigindo constantemente uma capacidade que acreditou existir. A sua atitude, apoio, e disponibilidade para o diálogo científico foram sem dúvida essenciais para que este momento tivesse lugar.
À Dra. Sofia Madureira, indispensável companheira de trabalho, pelos agradáveis anos de investimento em conjunto, sem o qual esta tese não teria sido possível.
À Prof. Dra. Carla Moleiro, que ajudou na abordagem estatística, de uma forma que parecesse fácil.
Ao Prof. Dr. Jorge Campos, pela colaboração na aquisição das imagens dos participantes.
Ao Dr. Carlos Morgado, que esteve sempre disponível para discutir dúvidas do foro neuro-radiológico.
Ao Prof. Dr. Didier Leys, que há 12 anos me acolheu no Centro Hospitalar de Lille, tendo proporcionado condições humanas e científicas inigualáveis para investigar.
Ao Prof. Dr. Carlos Garcia, o primeiro que me apresentou a versão humanista da Neurologia clínica e de investigação, e que evoco com saudade.
Ao Prof. Dr. Alexandre Mendonça pelo rigor e pela disponibilidade. Tem sido um apoio fundamental e constitui uma felicidade com ele poder trabalhar.
Aos muitos dos colegas neurologistas que referenciaram doentes, e que ao longo do tempo foram críticos muito positivos do trabalho.
4 Ao Prof. Dr. Manuel Gonçalves Pereira, que impulsionou e tornou decisiva a conclusão deste percurso.
À Dra Ana Catarina Santos, pela partilha de gabinete, de conhecimentos estatísticos, e de muito mais.
À Luísa Mendonça, pela ajuda e paciência na formatação,à Marisa Costa e à Alcina Fraga, que ajudaram no processo burocrático necessário. À Isabel Santos, que encontra os artigos mais difíceis.
Aos investigadores do grupo europeu LADIS, pelo continuado esforço de cooperação, que verdadeiramente desafiou fronteiras linguísticas, culturais e científicas.
Aos doentes que generosamente participaram no estudo, e que o tornaram possível. São eles, afinal, o destinatário de todo o investimento científico e pessoal.
Aos meus pais, porque a eles devo quase tudo.
5 Dedico esta tese à
Maria, ao Zé Miguel e ao Pedrinho
6 Declaration of interest: The LADIS Study was partially supported by the European Union within the Vth European Framework Program ‘Quality of life and management of living resources’, between 1998 and 2002, contract No. QLRT-2000-00446.
7
CONTENTS
Chapter 1. Introduction and methods I. Introduction
II. Presenting the hypotheses under study III. Methodology
Chapter 2. Testing the hypotheses under study I. General data from the LADIS study II. Exploring the hypotheses under study
Chapter 3. Discussion
I. Summary of main results
II. Strengths and limitations of the study III. Discussion of the hypotheses under study IV. Other contributors for cognitive function
V. More sensitive methods to detect White Matter Changes (WMC) VI. Implications for clinical practice and for research
8
AUTHORSHIP
The results presented in this dissertation were retrieved from the following manuscripts:
Verdelho A, Madureira S, Ferro JM, Basile AM, Chabriat H, Erkinjuntti T, Fazekas F, Hennerici M, O'Brien J, Pantoni L, Salvadori E, Scheltens P, Visser MC, Wahlund LO, Waldemar G, Wallin A, Inzitari D; LADIS Study. Differential impact of cerebral white matter changes, diabetes, hypertension and stroke on cognitive performance among non-disabled elderly. The LADIS study. J Neurol Neurosurg Psychiatry.
2007;78:1325-30
Verdelho A, Madureira S, Moleiro C, Ferro JM, Santos CO, Erkinjuntti T, Pantoni L, Fazekas F, Visser M, Waldemar G, Wallin A, Hennerici M, Inzitari D; LADIS study White matter changes and diabetes predict cognitive decline in the elderly: the LADIS study. Neurology 2010; 75, 160-167.
Verdelho A, Madureira S, Moleiro C, Santos CO, Ferro JM, Erkinjuntti T, Poggesi A, Pantoni L, Fazekas F, Scheltens P, Waldemar G, Wallin A, Inzitari D. Self-Perceived Memory Complaints Predict Progression to Alzheimer Disease. The LADIS Study. J
Alzheimers Dis. 2011;27:491-8.
Verdelho A, Madureira S, Moleiro C, Ferro JM, O’Brien JT, Poggesi A, Leonardo Pantoni, Franz Fazekas, Philip Scheltens, Gunhild Waldemar, Anders Wallin, Timo, Erkinjuntti, Domenico Inzitari, on behalf of the LADIS Study. Depressive symptoms predict cognitive decline and dementia in older people independently of cerebral white matter changes. Submitted to the American Journal of Psychiatry
Verdelho A, Madureira S,, Ferro JM, Baezner H, Blahak C, Erkinjuntti T Pantoni L, Fazekas FScheltens P, Waldemar G, Wallin AHennerici MInzitari D. Physical activity prevents progression for dementia, mainly vascular dementia. Results of the LADIS study. Stroke, in press (accepted in august 2012).
9
11
CHAPTER I. INTRODUCTION AND METHODS
I. INTRODUCTION
I.I. Defining white matter changes
Cerebral age-related white matter changes (WMC) designate the changes of the radiological appearance of cerebral white matter, detected either in CT scan or in MRI, of probably vascular aetiology, that are frequently described in elderly people (1-3). The clinical significance of those changes has gained attention in the last three decades and remains a controversial issue.
I.II. Historical evolution
The implication of white matter changes in cognition started more than a century ago: in 1894 Otto Binswanger described the clinical picture of progressive cognitive decline in a syphilitic man with walking difficulties and depression, and described the macroscopic aspects of the brain (4,5). Binswanger did not provide, at that time, a microscopic observation. Interestingly, it was Alois Alzheimer who some years after described a similar patient and provided the histological description, attributing the white matter changes to arteriosclerosis of the long penetrating vessels and calling it “Binswanger’s disease” (6). Almost simultaneously P. Marie described the “état
lacunaire”, a clinical picture of sudden focal signs with good recovery, slow gait with
small steps, pseudobulbar dysfunction and progressive dementia due to multiple lacunes (7), a very close-related condition frequently associated with “Binswanger’s disease”.
Later, in 1962, Olszewski, after reviewing Binswanger's original report, proposed the term “subcortical arteriosclerotic encephalopathy” to describe "a form of cerebral arteriosclerosis in which vessels of the white matter and subcortical grey matter are affected predominantly" (8).
In 1979 Rosemberg published the first imagiological report using CT scan of a patient with diffuse white matter changes with neuropathological changes compatible with Binswanger’s description (9). Since then, data from radiological studies provided more
12 and more information about white matter changes: WMC were identified in computed tomography as periventricular or subcortical areas of hypodensity on the white matter.
In 1986 Hachinski introduced the term leukoaraiosis (from the Greek “rarefaction” of “white”) in an attempt to standardise the designation of the attenuation of cerebral white matter seen through radiological methods (10), irrespective of the causative pathological process.
Sze et al in 1986 studied histologically the foci of high signal intensity at the frontal horns found in MRI of 56 asymptomatic subjects (of all ages) and found that they consisted in an elevated water content concluding that the increased MRI intensity found were normal findings in all T2-weighted spin-echo magnetic resonance scans (11).
In 1987 Babikian and Ropper conducted a careful review, describing clinical characteristics of all patients with pathological description compatible with “Binswanger’s disease” and found that all patients shared common pathological changes in the white matter (12).
At that time the question was if Binswanger’s disease could be a single entity, or otherwise a syndrome caused by different pathophysiologic mechanisms. In the same year Roman described “Senile dementia of the Bisnwanger type as a potentially reversible vascular form of dementia in the elderly” (13). By then, the term “multi-infarct dementia”, introduced by Hachinski some years before was almost synonymous with vascular dementia. Binswanger’s disease remained an obscure entity without specific clinical or neuropathological criteria that clearly could not be applied to all patients with radiological changes of the white matter.
Kertesz and co-workers in 1988 (14) distinguished periventricular hyperintensities into rims and caps: rims being periventricular hyperintensities surrounding the lateral ventricles, and caps those surrounding the poles of lateral ventricles. According to these authors, those lesions could have different clinical implications and vascular risk factors associated, with caps and severe rims frequently associated with pathological changes and more frequently found in patients with strokes and haemorrhages while mild rims could be frequent in elderly asymptomatic subjects. This group also described “unidentified bright objects”, meaning punctuate and/or confluent hyperintense areas frequently seen in the deep and sub-cortical white matter on
T2-13 weighted images that were frequently associated with acute vascular ischemic or hemorrhagic events, as severe rims and caps (14).
Leifer et al in 1990 described data from 7 patients that presented small periventricular zones of increased T2 signal corresponded to a periventricular cap and concluded that this was a normal and frequent appearance in young ages (15).
In 1990 Bennett proposed criteria for the antemortem diagnosis of what he and co-workers designated “a poorly understood form of vascular dementia: Binswanger’s disease” (16). These criteria included dementia, radiological findings and other signs of subcortical cerebral dysfunction or evidence of vascular disease (16). Those criteria were never widely accepted and used in clinical settings.
It was clear by then that Binswanger’s description was too limited and could not be applied to the extent of the clinical picture that was beginning to emerge. Radiologic techniques showed several vascular lesions that could explain different clinical pictures. One of the most likely hypotheses was that Binswanger’s disease could simply be descriptive of the shared end result of a number of diverse neuropathologies that affect subcortical white matter.
The NINDS-AIREN diagnostic criteria for vascular dementia included, in 1993, extensive white matter changes of vascular origin as one of the lesions associated with vascular dementia (17). With the progression of the concept of cerebral vascular disease, and the generalisation of the broader concept of vascular cognitive impairment, the NINDS-CNS Vascular Cognitive Impairment Harmonization standards were published in 2006. According to that set of recommendations, systematic measurement of white matter changes is recommended, although the non-pathognomonic value of vascular radiological changes in vascular cognitive impairment is recognized (18).
I.III. Neuropathology of WMC
When Otto Binswanger published his first patient, he described the macroscopic observation of the brain that consisted in “granular deposits in the dura mater at the base of the skull, enlargement of the lateral ventricles, marked atrophy of the cerebral white matter, multiple ependymal thickenings and intracranial atherosclerosis”(4-6).
14 The characteristic pathologic abnormalities are located in the white matter of the cerebral and cerebellar hemispheres and in the arteries and arterioles within the brain. The external surface of the brain often appears normal (5). “In severe cases, on gross inspection the white matter appears firm, rubbery, puckered, granular, and wrinkled and often has a gray or yellowish tint” (19). The ventricles are usually enlarged. Reduction of corpus callosum and multiple lacunar infarcts in the basal gray nuclei, thalami, pons, and cerebral white matter can co-exist. Myelin stains best display the white matter abnormalities (4-6, 8,13). “In some cases, the white matter is diffusely pale, indicating severe widespread loss of myelin. The periventricular regions usually show the most severe myelin loss; the convolutional white matter and the U fibres of the deeper gyri are almost entirely spared. The anterior frontal lobe white matter is probably more often heavily involved than the posterior portions of the cerebral hemispheres, but, in some patients, temporal, parietal, and occipital lobe white matter can be more severely demyelinated. In most patients the abnormalities are roughly symmetric but patchy and multifocal. Focal regions of white matter demyelination may be confluent, producing large lesions in one cerebral lobe. The white matter pathways in the brainstem are usually spared. Involvement of the cerebellar white matter is quite variable” (6,13).
More recently, authors have tried to find a correlation between the pathological findings of the radiological changes in CT and MRI. There is a debate if deep subcortical white matter changes have the same clinical and pathological significance as periventricular white matter changes.
A recent study approached the MRI-pathological correlation, based on the radiological classical division between rims and caps, and found that the aetiological findings associated with periventricular hyperintensities seen in rims included “myelin pallor, dilatation of perivascular spaces and increased extracellular spaces” (20). Discontinuity of the ependymal lining and subependymal glisosis (20) could be seen in the lateral ventricular wall. Leifer et al described histologically “periventricular caps as subependymal glial accumulations, with some loss of the ependymal lining and a surrounding pale-staining area of finely textured myelin and axons with an altered glial pattern, identifiable anatomically as the subcallosal fasciculus”. This histological pattern of subependymal glial accumulations and fine fibres is, according to this author, normal and is often associated with fibrotic small blood vessels (15). The changes seen in caps are similar, and associated with increased interstitial fluid caused by ischemic
15 vascular damage or impairment of transportation of interstitial fluid into the ventricle (14).
Deep white matter changes have been more frequently associated with vascular risk factors and the co-existence of small lacunar infarcts. They are also associated with myelin pallor and dilatation of perivascular spaces of the medullary arteries (20).
I. IV. Pathogenesis of white matter changes
There is no consensus on the characteristics and on the pathogenesis of brain damage expressed by white matter changes associated with age (21). It has been assumed that white matter changes are the expression of the dysfunction of brain small vessels. These small vessels (small arteries and arterioles) can originate superficially or deeply (pial), consisting in terminal vessels of medium-sized arteries, or can originate deeply directly from larger arteries (arterial perforators) (21).
A recent review tried to understand the pathologic mechanism, using in vivo experimental models. Although the authors found that no model could describe all features of the human disease, they proposed the chronic hypertensive models as being closer to the human profile (22). A recent study found reduced structural integrity of the endothelium, that led vessels to be more permeable and which compromised the brain-blood barrier in areas of WMC (23). In this study, reduced vascular integrity was the best predictor of increasing WMC severity, with a significant decrease in vascular integrity found in areas of WMC compared with normal white matter, supporting the vascular aetiology of the changes in white matter (23). In fact, the ischemic nature of the lesions of the white matter has been advocated as one of the leading causes of vessel dysfunction that can lead to demyelination, a form of incomplete infarct or selective necrosis of the white matter (24) or either a complete acute ischemia that could origin lacunes (25).
Other mechanisms involved in the ischemic form of the disease could be local subclinical inflammation (23,26,27), oligodendrocytes apoptosis (28), which originates axon loss, gliosis, dilated perivascular spaces and spongiosis.
Pathogenesis of deep and subcortical white matter is not completely elucidated, but is generally considered to be due to chronic ischemia or brief and repeated ischemic insults of moderate severity (20).
16
I.V. Radiological characteristics
WMC were identified in computed tomography (CT) as bilateral periventricular or subcortical areas of hypodensity, patchy or diffuse, that do not follow specific vascular territories and are not adjacent to focal areas of cortical damage or ventricular enlargement in order to distinguish them from focal large infarcts on the white matter (10, 21).
In magnetic resonance imaging (MRI) white matter lesions are seen as hyperintensities on T2 weighted and fluid-attenuated inversion recovery images, involving the supratentorial hemispheric white matter: periventricular white matter, the corona radiata, the centrum semiovale, but can also occur infratentorial in the pons (29). They appear either punctuate or confluent, with different severity, have irregular margins and do not follow specific vascular territories.
White matter changes can be isolated or confluent, usually symmetrical but may not be equally distributed, with irregular margins, with no expression in T1 sequences, no enhancement with contrast. U-fibres are usually well preserved despite diffuse changes in white matter changes (21, 29).
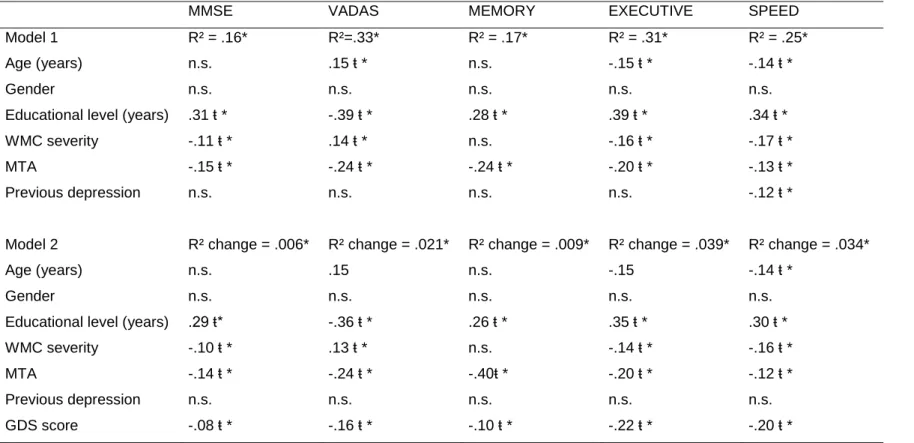
Periventricular changes include caps around the frontal horns of the lateral ventricles and pencil-thin lining or a smooth halo along the side of lateral ventricles (fig. 1) (29).
17 Fig.1 Types of periventricular and subcortical white matter lesions
Punctuate lesion (subcortical)
Pencil-thin lining (periventricular)
Caps (periventricular)
Early confluent lesions (subcortical)
Smooth halo (periventricular)
18
I.VI. Epidemiology of WMC
Age-related white matter changes are described in MRI of almost 100% of elderly individuals in population-based studies (1,2,3). In the Rotterdam scan study only 5% of the 1077 subjects aged between 60–90 years, randomly sampled from the general population, were free of any white matter changes (1). Among the 3301 subjects older than 65 years-old from the community included in the Cardiovascular Health study, only 4.4% were free of any abnormal signal in the white matter (2). Among the subjects included in the Helsinki Aging study (55-85 years old), most of the white matter changes described in non-diseased elderly people living at home were mild (3) in nature, and a clear increase with age was reported, similar to other studies (1,2.3,30). Caps and pencil-thin lining periventricular and punctuate subcortical white matter changes are the most common signal changes in elderly subjects and occur in more than half of asymptomatic persons below 55 years-old in population studies (29).
Some demographic and vascular risk factors are associated with higher risk of developing more severe WMC, and among these, mainly with aging, hypertension and stroke (2, 3, 31).
Frequency and severity of WMC in different degenerative dementias remains a controversial issue: Some authors found WMC more frequent in Lewy body dementia and dementia associated with Parkinson disease (32,33), mainly associated with periventricular hyperintensities (34), comparing with Alzheimer disease. Others found WMC more frequent in both pathologies without differences in the severity of WMC (35,36). In demented older patients periventricular white matter changes have been reported in almost all patients irrespective of dementia type (29), and subcortical lesions are described in 96% of vascular dementia patients, 89% of Alzheimer disease patients and in 85% of patients with Lewy body dementia (33).
I. VII.Clinical expression of WMC
Since the first imagiological descriptions of white matter changes, several studies approached white matter changes with clinical significance and by the end of the 90s some data sustained a possible association between white matter changes and cognitive decline, gait disturbances, urinary dysfunction, personality changes and depression (21), however contradictory results inhibited the consensus in this topic (37).
19
I. VII.a. Cognitive implications of WMC
Cerebral age-related white matter changes (WMC) have been described in brain imaging of demented and non-demented elderly subjects (1-3,38,39). Several reports implicated WMC in cognitive deficits in independent elderly subjects, mainly in executive functions, attention, speed and motor control (40,41) but also in global measures of cognition (2,38,40), visuoconstructional (38,40) and memory tasks (31,42). WMC were associated with progression for dementia and decline in specific neuropsychological domains, mainly attention, executive functions and processing speed (42-48). However, the association was not consistent across all studies (49) and others were negative when controlling for other confounders, such as age and medial temporal lobe atrophy (49-53). Moreover, the difficulty in understanding the implication of white matter disease in cognition becomes more evident when white matter changes become identified using imagiological methods in perfectly independent and otherwise healthy older subjects without obvious cognitive impairment.
I. VII.b. Meaning of memory complaints in subjects with WMC
Memory complaints are frequent among elderly subjects, and although this complaint is very disturbing for elderly people, the meaning of memory complaints is still under discussion (54). Some studies tried to correlate subjective memory complaints with memory objectively tested and controversial results have been published (55-59). Results from studies have indicated that the meaning of memory complaints can be different according to the age of subjects. Memory complaints were associated with depressive symptoms (54,55,60), anxiety, psychological traits and stress (56), and this association is stronger in younger individuals. Memory complaints were also associated with brain morphological changes such as white matter changes (61-63), hippocampal volume (62-65) and Alzheimer’s disease (36) pathology in post-mortem studies (66,67). Memory complaints were found to be a predictor of future dementia in some studies (57, 68-70) but not in others (59, 71,72), and in one recent study half of the Alzheimer disease patients had no subjective memory complaints three years before diagnosis of AD (73).
I. VII.c.Influence of vascular risk factors in cognition in subjects with WMC
Vascular risk factors, namely hypertension, stroke, and diabetes have been implicated in cognitive decline and dementia (74-82).
20 Epidemiological studies indicate that vascular risk factors play a role in the development of cognitive impairment and dementia, including degenerative dementia (83-86). Hypertension in mid-life has been consistently associated with later development of cognitive decline and dementia, not only of vascular dementia, but also of degenerative dementia as Alzheimer disease (74,77,84,87-89). The relationship between late-onset hypertension and cognitive decline and dementia is less clear: some studies were negative for this association (78,79,90) or sustain that a very low systolic and/or diastolic value was associated with higher risk of cognitive decline (87,88). In cross-sectional studies hypertension in late-life was associated with worse performance in several cognitive tests mainly related with executive functions and attention, digit symbol test and word fluency (91) but also difficulties in some global cognitive functioning (Mini Mental State Examination (MMSE) (92,93) and CAMCOG (Cambridge examination for mental disorders of the elderly—cognitive section) scores (94).
One possible explanation for these discrepancies is that the relationship between hypertension and cognitive decline changes with time (89): hypertension in mid-life probably is associated with chronic vascular damage that later originates cognitive impairment, while late-hypertension does not have this impact. On the other hand, trials focusing on the prevention of dementia using antihypertensive medication have failed to show a consistent protective effect (95,96). From the six main randomized placebo-controlled studies, 4 were negative for a protective effect (97-100), one found a small effect on the prevention of dementia (101) and the other (102) found a protective effect only for poststroke dementia. In fact those studies were probably performed in older ages than what was desirable to prevent dementia (subjects older than 60 years), and the follow-up was short, not long enough to have sufficient patients developing dementia.
There is growing interest in the cognitive impact of diabetes, with several reports of an association between diabetes and higher risk of cognitive impairment and dementia (85,86,103,104). Observational studies suggest that diabetic subjects have a two fold increase in risk mild cognitive impairment and dementia comparing to non-diabetics (80,93). Even among non-demented subjects, diabetics have worse cognitive performance when compared to non-diabetics (105). Diabetes was initially implicated in the progression for dementia due to the higher risk of vascular disease, but this higher frequency has been also mediated through metabolic changes due to the insulin and glycemia pathways that are implicated in the metabolic production of beta-amiloide
21 protein and tau protein (104), so directly implicated in pathogenesis of Alzheimer’s disease (80,106). However, controversial data was published and diabetes was associated with slower rate of cognitive decline in Alzheimer disease (107). A recent systematic review stressed that the risk of dementia in diabetes is increased when associated to other vascular risk factors, phenomena that was also identified for other risk factors (108).
Stroke (irrespective of being large territorial or lacunar stroke) has been associated with cognitive impairment in prospective community studies (81,109-111) and some studies found a two-fold risk of dementia, not only for vascular dementia and vascular cognitive impairment, but also for degenerative dementias such as Alzheimer’s disease (112). The clear impact of stroke on the development of specific types of dementia is not well established and post-stroke dementia remains an open field of discussion.
Controversial data exist about the relationship between alcohol intake and dementia: low or moderate alcohol intake was associated with reduced risk of Alzheimer’s disease in a systematic review with meta-analysis, compared to the risk of dementia in non-drinkers (113). Non-drinkers had a small higher risk compared also to excessive drinkers. In fact, we can be suspicious of these results, and interpret them as due to a bias, hypothesizing that non-drinkers are former excessive drinkers that stopped consuming due to health problems (113).
Smoking habits have also been studied in their implication for the risk of dementia. Smoking habits could have a beneficial effect mediated through the stimulating effect of nicotine. In fact, the acute administration of nicotine in non-smoking young adults with attentional deficit was associated with improvement in attention, executive functions and working memory, an effect probably mediated through the activation of the cholinergic system (114). Indeed, in a study with elderly people from Taiwan, a better cognitive profile was observed in smokers (115). Very recently an improvement in measures of attention, memory and mental processing was found after 6 months of transdermal nicotine in non-smoking subjects with amnestic mild cognitive impairment, in a double-blind randomized trial (116). However, the deleterious effect of smoking, mediated through oxidative stress, triggering aterogenesis and inflammation could, even indirectly, mediate increase risk for cognitive decline. In a meta-analysis of 19 observational prospective studies, smoking increased the risk for dementia, not only vascular dementia, but also for degenerative dementias, an effect found mainly comparing active smokers against never-smokers (117). This risk could potentially be more pronounced among persons without the APOE_4 allele than among APOE_4
22 carriers (118). One of the most interesting findings is that the risk for developing dementia provided by the association of multiple vascular risk factors is much higher when compared to the risk provided from each vascular risk factor (108,119). This suggests an additive effect between several vascular risk factors and the progression of Alzheimer’s disease. To sustain this hypothesis, treatment of several risk factors simultaneously is more effective than the treatment of a single vascular risk factor (121,122) in several reports. But the individual contribution of each vascular risk factor for cognitive decline and dementia, taking into account WMC remained unsettled.
I. VII.d. WMC and depressive symptoms
Late onset depressive symptoms and depression have been associated with WMC (123). Furthermore, depressive symptoms have been recently pointed out as additional risk factors for several diseases, including fatal and non-fatal stroke and cardiovascular mortality (124,125). One of the intriguing aspects is if vascular factors precede late-onset depressive symptoms of if it is the other way around. This relationship is not clearly understood, and several explanations have been proposed in previous studies.
Some studies proposed biological explanations for the association between depressive symptoms and cognitive decline, including hyperactivity of the hypothalamic–pituitary– adrenal axis with enhanced adrenal responsiveness to ACTH and glucocorticoid negative feedback with subsequent hypercortisolemia (126), reduced heart rate, glucose intolerance, increased platelet reactivity (127), poorer endothelial function and more severe atherosclerosis (128), and presence of inflammatory proteins (129) secondary to depression.
Using structural magnetic resonance imaging, late-onset depression was associated with significant left regional hippocampal volume reduction, possibly concentrated in the subiculum and in posterior-lateral aspects of the CA1 (130), smaller amygdala volumes (131), small orbitofrontal cortex volume (132), bilateral caudate nucleus reduction (133), especially in the anterior portions, compared to non-depressed controls. In a small study, the association between regional caudate atrophy could be mediated though WMC that ultimately led to caudate atrophy (134).
Data from functional studies (using fMRI) has also been controversial. One study in late-onset depression showed greater connectivity in frontal (precentral, subgyral, middle frontal, and paracentral lobule), sub-lobar (thalamus and insula), limbic
23 (cingulate), parietal (postcentral gyrus, precuneus, inferior parietal lobule, and supramarginal gyrus), and temporal (superior temporal gyrus) compared to non-depressed controls (135). In another study, late-life acute non-depressed patients had diminished activity in the dorsolateral prefrontal cortex (left BA46) and diminished functional connectivity between the dorsolateral prefrontal cortex and the dorsal anterior cingulate cortex, compared to non-depressed controls when performing an executive-control task (136).
Another possible explanation is the association between depression and higher frequency of vascular risk factors, such as hypertension and glucose intolerance, reduced heart rate variability and failure of adrenergic activity regulation, mediated trough some of the mechanism mentioned before (126-129). Additionally, some antidepressants can be associated with cardiac arrhythmias and ECG abnormalities. One other possible explanation for the higher risk of cerebrovascular pathology in patients with depression is the effect of behavioural factors—for example, unhealthy lifestyle, involving reduced physical activity and diet type as well as poor medication adherence (137): a meta-analysis found depression to be a risk factor for non-compliance with medical treatment, with an odds ratio of 3.03 (95% confidence interval 1.96 to 4.89) which can also lead to worse risk factor control. These facts support the vascular depression hypothesis: late depressive symptoms could be an expression of vascular damage and not a result of a depressive disorder. In that perspective, late depressive symptoms could result from the disruption of fronto-striatal circuits caused by cerebral vascular pathology.
On the other hand, depressive symptoms have been associated with worse cognitive performance in non-demented elderly subjects (138,139), with worse performance in executive functions (138,140), attention and processing speed (140,141).
Moreover, cognitive impairment persists even after remission of late-life depression, and older individuals who were previously cognitively intact before depression are likely to be cognitively impaired in the remitted state of depression (142,143). However, conflicting data exist concerning depressive symptoms and risk of cognitive decline and dementia (139,144-148). A meta-analysis concluded that history of depression was a risk factor for Alzheimer’s disease rather than a prodromal phase (149), but a recent community-cohort study could not find evidence to support this hypothesis (150). Some studies have found an increasing risk for AD (148,151), whereas others found that the risk was associated with vascular dementia but not with AD (152), and due to a close
24 temporal association suggested depression as a prodromal symptom of vascular dementia (152).
Few studies have investigated neuropsychological performance in depressed subjects taking into account cerebral white matter changes (WMC) and vascular risk factors. Two recent prospective studies failed to find vascular disease as a mediator to cognitive impairment and Alzheimer’s disease in depressive patients, although confirmed depressive symptoms as a risk factor for Alzheimer’s disease or mild cognitive impairment (144, 153). Others suggested that late onset depressed patients performed worse in neuropsychological testing and had more severe WMC (154-157).
I. VII.e. WMC and urinary function
Urinary disturbances are a common sequela of stroke (158) and micturition dysfunctions are often seen with brain vascular pathology (159). Previous studies have reported urinary incontinence as one of the disturbances possibly associated with WMC (160-163), probably due to the damage of the frontal subcortical circuit. In one study performed in patients with Alzheimer’s, larger volumes of WMC were associated with urinary incontinence (164). In the two studies that assessed urinary function with urodynamic tests, detrusor hyperreflexia was found to be the dysfunction more specifically linked with WMC (165,166). Available knowledge indicates that bladder control is under complex visceral sensory-motor program control (167) and that lesions in the white matter tracts may reduce inhibitory input to the micturition reflex pathway and elicits detrusor, causing urinary dysfunction.
I. VII.f. WMC, gait impairment and physical exercise
WMC have been associated with impaired balance, gait problems and falls (168). Lesions in cerebral white matter can be responsible for the disruption of the complex motor circuit network that connects basal ganglia and brainstem structures with the frontal cortex, where integrity is needed for motor and gait coordination.
On the other hand, physical activity can prevent functional decline associated with age and promote global health status. Recent reports suggested that physical activity can prevent cognitive decline and progression for dementia, including Alzheimer’s disease (169-174) and the explanation for this relationship still remains a matter of debate (175). Several reasons can explain the protective effect of physical activity on the evolution for cognitive impairment. Beneficial effects of physical exercise can be observed in mental and social stimulation and can be integrated in a healthier life
25 status to justify the association (176). More biological explanations have been proposed: physical activity can improve cerebral blood flow, reduce vascular risk factors, decrease secretion of stress hormones and stimulate plasticity (177). Recently physical activity was associated with enhancement of endothelial function, counteracting the loss of vasodilatory function associated with aging (178,179). Some data support a decreased progression of intima-media thickness associated with physical activity (180). No studies specifically approached the impact of physical activity in subjects with WMC.
I. VIII. Measuring WMC
Several scales were developed in order to measure WMC. The idea of an accurate and reproducible scale to measure WMC has been proposed for many years but there is no consensus in this regard. Computerized and semi-computerized measurement of the extent of WMC could be an optimal solution, however, these methods are in fact limited because they are highly time-consuming and expensive and require specific technical equipment. Moreover, although computerized methods can be very attractive for large samples and trials, their use is very limited in clinical practice. Visual rating is fast and can be applied to images of different quality obtained on different scanners because the rater can correct for variations in image contrast, resolution, and to some extent, even for differences in angulation, so their use is in fact more user-friendly. The major difficulties in visual scales is that they rely on interrater variability that has to be taken into account when using this approach. Visual scales are quite similar, but results are not superimposed.
A review comparing 6 visual rating scales of WMC found that they were very highly correlated (181) but despite this, the authors could not conclude about the possible relationship between WMC rating with the clinical expression of those changes. In an effort to produce a reliable measure of WMC, a European collaborative group on white matter changes developed a single scale applicable to both CT and MR scale that theoretically could homogenise studies on WMC (182). However, WMC detected by CT or MRI are not exactly exchangeable because MRI is far more sensitive than CT in detecting WMC. Even among MRI studies, discordances may derive from the use of different pulse sequences and different magnetic field strengths. In addition to this, results from the scoring using the former scale are again not comparable to other published scales. One of the possible explanations for the differences described for
26 clinical implications, correlates and progression of WMC found between studies can be the use of different methods, including rating of WMC.
In appendix 1 we provide an overview of common scales for rating WMC, according to the review of Pantoni et al (181).
I.IX. Unsolved issues before our study
Several questions remained unanswered when we started our study, namely concerning long term cognitive implications of WMC detected imagiologically in subjects living in full autonomy. Furthermore, no convincing data was available regarding information on the risk for evolution for any type of dementia taking into account the global spectrum of risk factors presented by a subject.
Another unsolved issue was if memory complaints could represent early clinical manifestations of WMC. Memory complaints could mean difficulties in shifting attention, difficulties in mental flexibility or in reasoning and not difficulties in the process of memory. In fact to our best knowledge no previous study approached the meaning of memory complaints in subjects with WMC. In the same sense, no publication approached the specific effect over time of physical activity on the prevention of dementia in subjects with WMC living independently.
Since the first description provided by Binswanger, depression came out as clearly linked to white matter changes, and the depression vascular hypothesis has been largely debated. There are two unsolved issues in this regard: first, if late onset depression can be a marker of vascular disease, and second, if taking WMC into account, whether the association between depressive symptoms and cognitive impairment will be lost.
27
II. PRESENTING THE HYPOTHESES UNDER STUDY
The hypotheses of this study are:
1. Do age-related WMC and vascular risk factors influence neuropsychological performance of non-disabled elderly people living independently?
In subjects with WMC, the severity of WMC could be a mediator between vascular risk factors and cognitive decline. Our aim was to study the influence of WMC and vascular risk factors on the neuropsychological performance of non-disabled independent elderly people with WMC. We further aimed to analyse if vascular risk factors had an independent effect on cognitive performance or, when controlling for WMC, if the effect of vascular risk factors in cognition disappears.
2. Are WMC severity and vascular risk factors predictors of cognitive impairment and dementia over time in subjects with WMC who were initially autonomous and living independently? Do vascular dementia and Alzheimer disease have different predictors in subjects with WMC followed longitudinally?
Our aim was to ascertain if WMC severity is a predictor of cognitive impairment and dementia over time and if vascular risk factors are predictors of cognitive impairment and dementia, taking into account white matter changes. We also aimed to ascertain if vascular dementia and Alzheimer’s disease had different predictors.
3. Are self-perceived memory complaints in elderly people with cerebral white matter changes living independently a marker of future dementia?
We hypothesised that self-reported memory complaints in elderly subjects with white matter changes living independently could represent other non-memory deficits and predicted both Alzheimer’s disease as well as vascular dementia, independently of other confounders.
4 Are late onset depressive symptoms a marker of vascular damage and do they represent an initial stage of cognitive decline of vascular origin?
We hypothesized that WMC could be a mediator between depressive symptoms and neuropsychological performance in non-demented elderly people. Our aim was to
28 ascertain the influence of depressive symptoms on cognitive performance in a large sample of elderly subjects with WMC, to search if influence of depressive symptoms in cognition was lost when considering the effect of WMC severity, and to analyse this relationship over time.
5. Does regular physical activity prevents dementia in elderly subjects with WMC?
We hypothesized that physical exercise could prevent evolution towards cognitive impairment and dementia in a cohort of old people with white matter changes living independently that were followed prospectively during 3 years with comprehensive cognitive evaluation and careful control of concomitant factors implicated in disability.
29
III. METHODOLOGY
In order to clarify the clinical significance of white matter changes, a European multicentre collaboration was established in 2000 with the support of the European Union (5th European Framework Program ‘Quality of life and management of living resources’), and the LADIS study was promoted (183).
The LADIS study was designed to answer one main objective: to assess the role of WMC as an independent predictor of the transition from an autonomous functional status to disability in elderly subjects and the role of WMC progression in this transition (183). The study has been carried out in 11 European centres (Amsterdam, Copenhagen, Florence, Graz, Göteborg, Lisbon, Helsinki, Huddinge, Mannheim, Newcastle-upon-Tyne and Paris) that shared a common interest in the investigation of the clinical consequences of vascular changes in the brain. The first step was to design the study: defining procedures for assessing clinical outcomes, optimizing technical aspects that involved the methods design, selection and harmonization of the instruments, taking into account the cultural and linguistic differences. A hand book was constructed to guide the use of all instruments and the selection of the staff in each centre (183). To better deal with all the possible clinical implications, work packages were identified according to the main focuses of the study (methodology, disability, neuroimaging, cognition, mood and gait), each with one coordinator and collaborators (see list of LADIS staff in appendix 2). The Lisbon centre was responsible for the coordination of work package 4 (cognition), and a neuropsychological test battery was constructed designed for the specific application in subjects with cognitive vascular pathology (184).
Inclusion criteria and instruments
Inclusion criteria for the study were: (i) 65–84 years of age; (ii) presence of WMC of any degree on MRI, according to the scale of Fazekas (185); and (iii) no disability, as determined by the Instrumental Activities of Daily Living scale (IADL) (186). Patients were referred for the study with minor neurological, cognitive, mood or motor complaints, incidental findings on cranial imaging caused by non-specific events, without impact on daily living activities or were otherwise volunteers (183).
Subjects were evaluated at baseline and yearly during 3 years with a comprehensive protocol including registry of demographic and vascular risk factors, co-morbidities, evaluation of depression and quality of life and the neuropsychological battery
30 (183,184). For those patients who could not attend the clinical visit, a phone interview collecting clinical data and IADL (186) was performed with the patient and the carer, and the Telephone Interview for Cognitive Status (TICS) (187) performed with the patient, whenever possible. A delayed follow-up took part in 2008–2009 based on telephone interviews that included a clinical questionnaire and the Telephone Interview for Cognitive Status (187).
Investigators were provided with a specifically developed handbook with guidelines for applying criteria and tools. Data collected included demographic characteristics, education (expressed as years of schooling), occupational status, longest job in life, marital status, living conditions and physical activity. Patients were specifically asked if they had gait or bladder disturbances. Several other age-related co-morbidities, known as possible determinants of disability in the elderly, were assessed as they might be possible confounders: thyroid diseases, head injuries, falls in the last year, hip fractures, visual impairment, hearing loss, recurrent vertigo, any hospital admission over the last 3 years and currently used drugs were registered in a structured way.
Vascular risk factors considered were the following: previous hypertension: World Health Organization guidelines for the management of hypertension were followed to identify subjects with diagnosis of previous known hypertension (values > 140/90 mm Hg in subjects not taking antihypertensive medication, based on multiple blood pressure measurements, taken on several separate occasions) (188); diabetes mellitus was defined based on previous diagnosis and/or current treatment with insulin or oral hypoglycaemic medications, or at least 8-hour fasting plasma glucose 7.0 mmol/L or 126 mg/dL (189); hyperlipidemias were defined as total cholesterol >200, LDL >130, HDL <35 mg/dL, and triglyceride >200 mg/dL, in at least two measurements (190); myocardial infarction, documented by history, ECG or cardiac enzymes (191); angina pectoris (192,193); heart failure (194); atrial fibrillation (195); lower limb arteriopathy and peripheral vascular disease (196); history of stroke and/or TIA (197); cigarette smoking, expressed as smoked pack-years; alcohol consumption, expressed as g/day consumed, with one drink containing 10 g of alcohol. Both cigarette smoking and alcohol consumption were collected considering past and current habits.
We also considered incident stroke if a stroke occurred during the 3 year follow-up.
Depression was defined according to the Diagnostic and Statistical Manual of Mental Disorders (DSM) IV criteria (198), and severity of depressive symptoms was classified using the Geriatric Depression Scale (GDS) (199) and the Cornell scale for depression
31 in dementia (200). There was a systematic approach of the motor function using several clinical measures that included the Short Physical Performance Battery (SPPB) (201), single leg stance time, and walking speed (202).
Neuropsychological evaluation and Cognitive criteria
The LADIS neuropsychological battery took into consideration that the tests should be adequate to measure the deficits expected to be found in subjects with WMC: more dependent on executive functions, process of focusing attention, speed and motor control and the tests should be sensitive to this profile of cognitive decline (184). Additionally, selected tests had to be available and familiar in the majority of the centres; the battery had to be innovative, easy to administer, comprehensive, but not too long; all centres had to use the same version of each test, and the original English version of tests had to be translated into each local language (184).
Several steps were followed to create the LADIS neuropsychological battery: 1. a review of previous studies investigating subjects with ARWMC using comprehensive cognitive assessments; 2. a selection of the most frequently used instruments, 3 a survey for all participant centres concerning the availability of the test, the version of the test, the experience in using it and the existence of local or national validated norms.
The resulting neuropsychological battery included the Mini-Mental State Examination (MMSE) (203) as a global measure of cognitive function; the VADAS-Cog (which was a recently developed instrument used to assess the cognitive performance of patients with vascular dementia, composed by the well-known Alzheimer’s Disease Assessment Scale (ADAS-Cog) plus delayed recall, symbol digit, digit span, mazes, digit cancellation and verbal fluency) (204) as a comprehensive instrument to assess orientation, language, ideational and constructional praxis, immediate memory and delayed recall, attention and speed of mental processing); and the Stroop (205) and Trail Making (TM) (206) tests as additional measures of executive functions.
Additionally, in the follow-up clinical visits, patient cognitive status was classified into the following groups: 1. demented; 2 cognitive impairment not demented; 3 no cognitive impairment. For this purpose, we used the following criteria and definitions:
32 We considered two types of cognitive decline not dementia: 1. amnestic mild cognitive impairment (MCI), according to Petersen et al (defined as memory complaint, preferably corroborated by an informant; impaired memory function for age and education, preserved general cognitive function, intact activities of daily living and no dementia) (207) and 2. vascular cognitive impairment without dementia (VCIND) (defined as evidence of cognitive impairment and clinical consensus to identify significantly related vascular features; exclusion of dementia when impairments were not sufficiently severe to interfere with social or occupational functioning or when impairments were more focal than the global requirement for a diagnosis of dementia) (208).
We considered the following criteria for subtypes of dementia: probable Alzheimer’s disease according to the NINCDS-ADRDA Work Group (209), probable vascular dementia according to NINDS-AIREN criteria (17), subtype of subcortical vascular dementia according to Erkinjuntti et al. (210) and frontotemporal dementia according to McKhann et al. (211). The criteria of Alzheimer’s disease with vascular component was made when the investigator judgement considered that the clinical picture presented both aspects of Alzheimer’s disease and vascular dementia.
33
MRI study
MRI was performed at entry and at the end of the study in all subjects following a standard protocol (183). MRI studies include T1, T2, proton-density-weighted and fluid-attenuated inversion recovery pulse sequences. The exact sequence parameters were determined at the specific sites to give optimal contrast between the normal brain and WMC. For confirmation, representative images were checked centrally before the study. Diffusion tensor and magnetization transfer techniques were employed by selected centres to further characterize tissue changes (183).
The degree of WMC severity on MRI was rated using the visual scale of Fazekas et al (185) taking into account only deep and subcortical white matter lesions. To improve the homogeneity of ratings, centres were provided with an online atlas containing rules and examples for assessing WMC severity. Lesions were classified into 3 categories: mild WMC (single lesions below 10 mm; areas of ‘grouped’ lesions smaller than 20 mm in any diameter); moderate WMC (single lesions between 10 and 20 mm; areas of ‘grouped’ lesions more than 20 mm in any diameter; no more than ‘connecting bridges’ between individual lesions); severe WMC (single lesions or confluent areas of hyperintensity 20 mm or more in any diameter) (185). The local rating in each centre was used to balance the enrolment across the 3 severity WMC groups. In parallel, WMC severity was determined centrally at the Department of Neurology, Vrije Universiteit Medical Center, Amsterdam, the Netherlands, by raters blinded to the clinical details. This rating is used for all analyses in the context of WMC. The exact rating procedures and the correlation between local and central readings were performed and were good.
Volumetric analysis of WMC was performed by a single rater on the same axial FLAIR images, including the infratentorial region (212). Medial temporal lobe atrophy was assessed on coronal T1 weighted sequences using the MTA scale (213). Brain atrophy was evaluated by a single rater at baseline on FLAIR images with a template-based rating scale ranging from 1=no atrophy to 8=severe atrophy separately for cortical (sulcal) and subcortical (ventricular) regions. In case of asymmetry, the side with a more severe atrophy was used for rating. The sum of cortical and sulcal atrophy score was taken as a measure of global atrophy (see table 1).
34
Table 1.Instruments used in clinical visits
Disability Instrumental Activities of Daily Living scale (IADL) (186) Disability assessment of dementia scale (DAD) (214)
Quality of life Euro QoL EQ-5D (215)
Depression and severity of depressive symptoms
Diagnostic and Statistical Manual of Mental Disorders (DSM) IV criteria (198) Geriatric Depression Scale (GDS) (199)
Cornell scale for depression in dementia (200).
Motor performance Short Physical Performance Battery (201) Single leg stance (202)
Gait velocity (202)
Neuropsychological battery
Cognitive criteria
MMSE (203)
VADAS-cog (Alzheimer’s Disease Assessment Scale (ADAS-Cog) plus delayed recall, symbol digit, digit span, mazes, digit cancellation and verbal fluency) (204)
Stroop Test (205) Trail Making Test (206)
Telephone Interview for Cognitive Status (TICS) (187)
Mild cognitive impairment (MCI) (207)
Vascular cognitive impairment without dementia (VCIND) (208) Alzheimer disease (NINCDS-ADRDA Work Group) (209) Vascular dementia (NINDS-AIREN criteria) (17)
Subtype of subcortical vascular dementia (Erkinjuntti et al) (210) Frontotemporal dementia (211) MRI protocol Axial/coronal T1, T2, PD, FLAIR sequences Diffusion tensor Magnetization transfer techniques WMC: Fazekas Scale (185) Scheltens Scale (216)
European Task Force WMC Scale (217)
Volumetry (semiquantitative measurement) (212)
Infarcts
Visual assessment of number and location of lacunar and nonlacunar infarcts (218)
Atrophy
Graz Visual Rating Scale (global) (219)
Scheltens Visual Scale (medial temporal lobe atrophy) (213)
Further detailed methodology and statistical analysis for each of the hypotheses tested are presented in the next chapter, together with the hypotheses exploration.
35
REFERENCES
1. Leeuw FE, de Groot JC, Achten E, Oudkerk M, Ramos LM, Heijboer R, Hofman A, Jolles J, van Gijn J, Breteler MM. Prevalence of cerebral white matter lesions in elderly people: a population based magnetic resonance imaging study. The Roterdam scan study. J Neurol Neurosurg Psychiatry 2001;70:9–14.
2. Longstreth WT Jr, Manolio TA, Arnold A, Burke GL, Bryan N, Jungreis CA, Enright PL, O'Leary D, Fried L. Clinical correlates of white matter findings on cranial magnetic resonance imaging of 3301 elderly people. The Cardiovalscular Health Study. Stroke 1996;27:1274–82.
3. Ylikoski A, Erkinjuntti T, Raininko R, Sarna S, Sulkava R, Tilvis R. White matter hyperintensities on MRI in the neurologically nondiseased elderly. Analysis of cohorts of consecutive subjects aged 55 to 85 years living at home. Stroke 1995;26:1171-7.
4. Caplan LR. Binswanger's disease--revisited. Neurology. 1995;45:626-33.
5. Blass JP, Hoyer S, Nitsch R. A translation of Otto Binswanger article, The delineation of the generalized progressive paralyses. Arch Neurol 1991;48:961-72.
6. Schorer CE. Alzheimer and Kraeplin describe Binswanger's disease. J Neuropsychiatry Clin Neurosci 1992;4:55-8.
7. Marie P. Des foyers lacunaires de desintegration et des differents autres etats cavitaires du cerveau. Rev Med 1901;31:281-98.
8. Olszewski J. Subcortical arteriosclerotic encephalopathy. World Neurol 1962;3:359-75.
9. Rosenberg GA, Kornfeld M, Stovring J, Bicknell JM. Subcortical arteriosclerotic encephalopathy (Binswanger): computerized tomography.Neurology. 1979;29:1102-6.
10. Hachinski VC, Potter P, Merskey H. Leuko-araiosis: an ancient term for a new problem. Can J Neurol Sci 1986;13:533-4.
11. Sze G, De Armond SJ, Brant-Zawadzki M, Davis RL, Norman D, Newton TH. Foci of MRI signal (pseudo lesions) anterior to the frontal horns: histologic correlations of a normal finding. AJR Am J Roentgenol 1986;147:331-7.
12. Babikian V, Ropper AH. Binswanger's disease: a review. Stroke. 1987;18:2-12.
13. Román GC. Senile dementia of the Binswanger type. A vascular form of dementia in the elderly. JAMA. 1987;258:1782-8.
14. Kertesz A, Black SE, Tokar G, Benke T, Carr T, Nicholson L. Periventricular and subcortical hyperintensities on magnetic resonance imaging. 'Rims, caps, and unidentified bright objects'. Arch Neurol 1988;45:404-8.
15. Leifer D, Buonanno FS, Richardson EP Jr. Clinicopathologic correlations of cranial magnetic resonance imaging of periventricular white matter. Neurology 1990;40:911-8.
16. Bennett DA, Wilson RS, Gilley DW, Fox JH. Clinical diagnosis of Binswanger's disease. J Neurol Neurosurg Psychiatry. 1990;53:961-5.
17. Román GC, Tatemichi TK, Erkinjuntti T, Cummings JL, Masdeu JC, Garcia JH, Amaducci L, Orgogozo JM, Brun A, Hofman A, et al. Vascular dementia: diagnostic criteria for research studies. Report of the NINDS-AIREN International Workshop. Neurology 1993;43:250-60.
18. Hachinski V, Ladecola C, Petersen RC, Breteler MM, Nyenhuis DL, Black SE, Powers WJ, DeCarli C, Merino JG, Kalaria RN, Vinters HV, Holtzman DM, Rosenberg GA, Wallin A, Dichgans M, Marler JR, Leblanc GG. National Institute of Neurological Disorders and Stroke-Canadian Stroke Network vascular cognitive impairment harmonization standards. Stroke 2006;37:2220-41.
36 20. Matsusue E, Sugihara S, Fujii S, Ohama E, Kinoshita T, Ogawa T. White matter changes in elderly
people: MR-pathologic correlations. Magn Reson Med Sci 2006;5:99-104.
21. Pantoni L. Cerebral small vessel disease: from pathogenesis and clinical characteristics to therapeutic challenges. Lancet Neurol 2010;9:689-701.
22. Hainsworth AH, Markus HS. Do in vivo experimental models reflect human cerebral small vessel disease? A systematic review. J Cereb Blood Flow Metab 2008;28:1877–91.
23. Young VG, Halliday GM, Kril JJ. Neuropathologic correlates of white matter hyperintensities. Neurology 2008;71:804-11.
24. Brun A, Englund E. A white matter disorder in dementia of the Alzheimer type: a pathoanatomical study. Ann Neurol 1986;19:253–62.
25. Fisher CM. Lacunar strokes and infarcts: a review. Neurology 1982;32: 871–7.
26. Rosenberg GA. Inflammation and white matter damage in vascular cognitive impairment. Stroke 2009;40:S20–23.
27. Simpson JE, Ince PG, Higham CE, Gelsthorpe CH, Fernando MS, Matthews F, Forster G, O'Brien JT, Barber R, Kalaria RN, Brayne C, Shaw PJ, Stoeber K, Williams GH, Lewis CE, Wharton SB; MRC Cognitive Function and Ageing Neuropathology Study Group.Microglial activation in white matter lesions and nonlesional white matter of ageing brains. Neuropathol Appl Neurobiol 2007;33:670–83.
28. Brown WR, Moody DM, Thore CR, Challa VR. Apoptosis in leukoaraiosis. AJNR Am J Neuroradiol 2000;21:79–82.
29. Schmidt R, Schmidt H, Haybaeck J, Loitfelder M, Weis S, Cavalieri M, Seiler S, Enzinger C, Ropele S, Erkinjuntti T, Pantoni L, Scheltens P, Fazekas F, Jellinger K. Heterogeneity in age-related white matter changes. Acta Neuropathol 2011;122:171-85.
30. Lindgren A, Roijer A, Rudling O, Norrving B, Larsson EM, Eskilsson J, Wallin L, Olsson B, Johansson BB. Cerebral lesions on magnetic resonance imaging, heart disease, and vascular risk factors in subjects without stroke. A population-based study. Stroke. 1994;25:929-34.
31. Breteler MM, van Swieten JC, Bots ML, Grobbee DE, Claus JJ, van den Hout JH, van Harskamp F, Tanghe HL, de Jong PT, van Gijn J. Cerebral white matter lesions, vascular risk factors, and cognitive function in a population-based study: The Rotterdam Study. Neurology 1994;44:1246-52.
32. Silbert LC, Kaye J. Neuroimaging and cognition in Parkinson's disease dementia. Brain Pathol 2010;20:646-53.
33. Barber R, Scheltens P, Gholkar A, Ballard C, McKeith I, Ince P, Perry R, O'Brien J. White matter lesions on magnetic resonance imaging in dementia with Lewy bodies, Alzheimer's disease, vascular dementia, and normal aging. J Neurol Neurosurg Psychiatry 1999;67:66-72.
34. Barber R, Gholkar A, Scheltens P, Ballard C, McKeith IG, O'Brien JT. MRI volumetric correlates of white matter lesions in dementia with Lewy bodies and Alzheimer's disease. Int J Geriatr Psychiatry 2000;15:911-6.
35. Meyer JS, Huang J, Chowdhury MH. MRI confirms mild cognitive impairments prodromal for Alzheimer’s, vascular and Parkinson-Lewy body dementias. J Neurol Sci 2007;257:97–104.
36. Burton EJ, McKeith IG, Burn DJ, Firbank MJ, O'Brien JT. Progression of white matter hyperintensities in Alzheimer disease, dementia with lewy bodies, and Parkinson disease dementia: a comparison with normal aging. Am J Geriatr Psychiatry 2006;14:842-9.
37. Pantoni L, Garcia JH. The significance of cerebral white matter abnormalities 100 years after Binswanger's report. A review. Stroke 1995;26:1293-301.