Int J Anat Res 2014, 2(1):221-24. ISSN 2321-4287 221
Original Article
DIFFERENTIAL DIAGNOSIS OF A CASE OF BILATERAL CYSTIC
SW ELLING OF NECK IN AN ABORTED FETUS
M aruti ram Annamraju *
1, Subhadra Devi Velichety
2.
ABSTRACT
Address for Correspondence: M arut i ram Annamraju, Assistant Professor of Anat omy, S.V.M edical College, Tirupat i, Andhra Pradesh, India. E-M ail: marut [email protected]
Access this Article online
Quick Response code Web site:
*1 Assistant Professor of Anat omy, S.V.M edical College, Tirupat i, Andhra Pradesh, India.
2 Professor of Anat omy, Sri Venkateswara Inst it ute of M edical Sciences, Tirupat i, Andhra Pradesh,
India.
Objective:To analyse t he anat om ical and radiological observat ions in a fet us w it h bi lat eral cyst ic sw elling of neck.
M aterials and M ethods: A t otal of 30 abort ed fet uses w ere st udied for academ ic purpose ranging from age 12 w eeks t o 36 w eeks. A m ale abort ed fet us of 24 w eeks w it h huge sw elling in cer vicot horacic region w as invest igat ed by radiological and ult rasonographic exam inat ion. A detai led foetal aut opsy w as conduct ed for associat ed anom alies.
Observat ion: A huge cyst ic sw elling w as observed in t he post erior region of neck and upper t horax w it h m andibulo facial defect . About 1.2cm defect w as not ed in occipital bone w it h herniat ion of echogenic brain cont ent s and hypoechoic collect ion in t o t he occipital region.
Conclusion: Prenat al diagnosis of Cyst ic hygrom a and Encephalocele can be m ade from 9t h w eek onw ards,
w hich w i ll be helpful for planning deliver y or t o deal w it h neonat al com plicat ions.
KEYW ORDS: Cyst ic Hygrom a; Encephalocele; Spina bifida; M ult iple Pt erygium .
INTRODUCTION
Int ernat ional Journal of Anatomy and Research, Int J Anat Res 2014, Vol 2(1):221-24. ISSN 2321- 4287
Received: 16 Jan 2014
Peer Review : 16 July 2014 Published (O):30 M arch 2014 Accepted: 19 Feb 2014 Published (P):30 M arch 2014 Internat ional Journal of Anat omy and Research
ISSN 2321-4287 w w w.ijmhr.org/ ijar.ht m
Lym ph angio m as ar e co ngeni t al l ym p hat i c malformat ions t hat occur most commonly in the head, neck or axilla ; how ever , t hey may arise anyw here in t he developing lymphat ic system and const it ut e 5.6% of all benign lesions of infancy and childhood[1].
En cep h al o cel e ref ers t o a gro u p o f rar e congenit al anom alies of t he cent ral nervous syst em w here brain t issue prot rudes from a defect in t he skull. Encephalocele can occur in isol at io n, as w ell as w i t h ot her u nr el at ed congenital defect s or as part of a w ell described syndrome[2].
M ATERIALS AND M ETHODS
After approval by t he inst it ut ional et hical com-mittee 30 aborted foet uses of 12 w eeks t o 36
w eeks gestat ional age and bot h sexes w ere col-lect ed from Governm ent M at ernit y Hospit al w it h prior inform ed consent from parent s or close fam ily m em bers. Am ong t hese a m ale aborted fet us of 24 w eeks age w eighing 1.25 kg presented a huge bilateral neck sw elling w it h mult iple pterygium-w ebbing.
OBSERVATIONS:
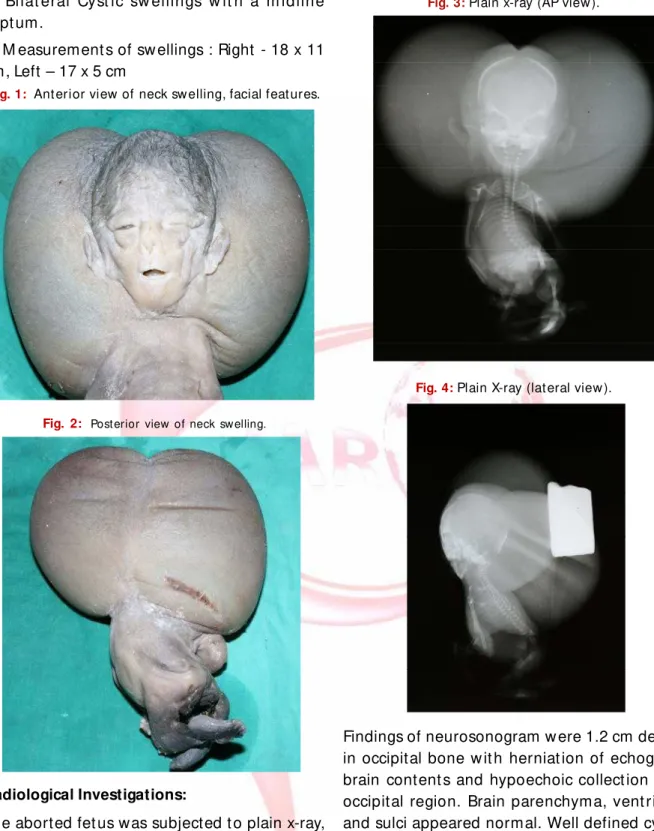
Following external feat ures w ere observed in this case.(Figs.1& 2)
1. Hypertelorism. 2. Saddle nose. 3. M icrognat hia. 4. Uplifted auricle.
Int J Anat Res 2014, 2(1):221-24. ISSN 2321-4287 222
6. Bi lat eral Cyst ic sw ellings w it h a m idline sept um.
7. M easurement s of sw ellings : Right - 18 x 11 cm, Left – 17 x 5 cm
Fig. 1: Ant erior view of neck sw elling, facial feat ures.
Fig. 2: Post erior view of neck swelling.
Radiological Investigations:
The aborted fet us was subjected t o plain x-ray, neurosonogram and CT scan. The follow ing observat ions w ere recorded.
Findings of plain x-ray (AP view ) (Fig.3) w ere Bilateral w ell defined soft t issue densit y lesion in posterolateral aspect of neck, hyper flexion an d ro t at io n of do rso-lum bar sp ine, No n-visualizat ion of posterior element s in t he region of cervical and upper t horacic spine. Plain x-ray (lat eral view ) (Fig.4) revealed bony defect in occipital bone in cont inuit y w it h t he soft t issue densit y w it h no evidence of calcificat ion.
Fig. 3: Plain x-ray (AP view ).
Fig. 4: Plain X-ray (lat eral view ).
Findings of neurosonogram w ere 1.2 cm defect in occipital bone w it h herniat ion of echogenic brain content s and hypoechoic collect ion int o occipital region. Brain parenchyma, vent ricles and sulci appeared normal. Well defined cyst ic lesions w it h thick internal echoes noted on eit her side of head & neck in continuit y with soft tissues of neck.
Findings of CT scan w ere 1.5 cm bony defect in occipital region w it h 5.5 x 3.8 cm w ell defined hypo dense lesion of 15-22 HU post erior t o occipital bone. Herniat ion of soft t issue densit y of 37-40 HU not ed t hrough t he defect in t he occipital bone int o t he hypo dense lesion. Well defined soft t issue densit y lesion of 14-20 HU of head and neck measuring Right side 11.5x7cm,
Int J Anat Res 2014, 2(1):221-24. ISSN 2321-4287 223
Left side 10.4x6.7cm. The above sw elling was in communicat ion w it h soft t issue of neck.
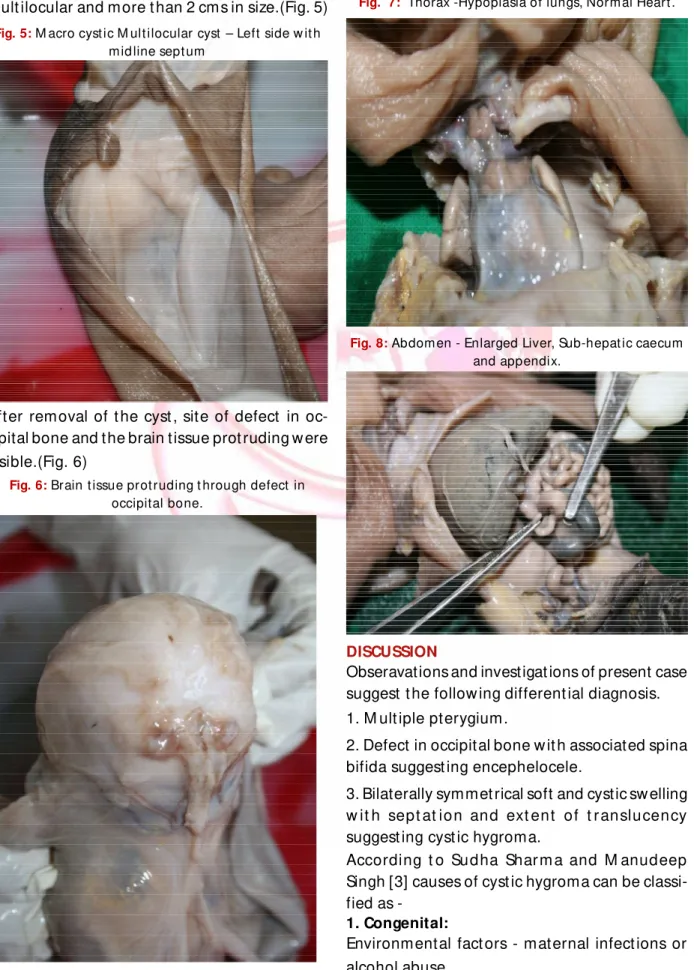
Later aut opsy of t he fet us was performed w hich revealed t hat t he sw elling had a midline sept um and bot h right and lef t side t he cyst s w ere mult ilocular and more t han 2 cms in size.(Fig. 5)
Fig. 5: M acro cyst ic M ult ilocular cyst – Left side w it h m id line sept um
After removal of t he cyst , site of defect in oc-cipital bone and the brain tissue prot ruding w ere visible.(Fig. 6)
Fig. 6: Brain t issue prot ruding t hrough defect in
occipital bone.
In t he t horax hypoplasia of lungs and norm al heart w ere observed(Fig.7). In t he abdomen t he liver was enlarged and caecum along w it h ap-pendix w ere sub-hepat ic in posit ion(Fig.8). The kidneys and suprarenals w ere normal.
Fig. 7: Thorax -Hypoplasia of lungs, Norm al Heart .
Fig. 8: Abdom en - Enlarged Liver, Sub-hepat ic caecum
and appendix.
DISCUSSION
Obseravations and investigat ions of present case suggest t he follow ing different ial diagnosis. 1. M ult iple pterygium.
2. Defect in occipital bone w it h associated spina bifida suggest ing encephelocele.
3. Bilaterally symmet rical soft and cystic sw elling w it h sept at ion and ext ent of t r anslucency suggest ing cyst ic hygroma.
According t o Sudha Shar m a and M anudeep Singh [3] causes of cyst ic hygroma can be classified as
-1. Congenital:
Environmental fact ors - maternal infect ions or alcohol abuse.
Int J Anat Res 2014, 2(1):221-24. ISSN 2321-4287 224
Genet ic fact ors:
a) Chromosomal anomalies - Trisomy 13,18,21 and Turner syndrome.
b) Non-chrom osom al (Syndrom ic) - Noonan, Kl in ef el t ers, Fr y n s, m u lt i p le p t er ygi u m syndromes and achondroplasia.
2. Acquired:
Tr au m a(i n clu d i ng sur ger y ) In f l am m at i o n obst ruct ion of a lymphat ic drainage pat hway. Cy st ic hygrom a, asso ciat ed w it h a nor m al karyot ype, can be inherited as an aut osomal recessive t rait [4].
Pathogenesis of cystic hygrom a: includes 3 major t heories
Failure of lymphat ics t o connect t o t he venous system[5].
Abnormal budding of lymphat ic t issue[6]. Sequest ered lym phat ic rest s t hat ret ain t heir embryonic grow t h potent ial[7].
Van der Putte[8] st udied aborted fet uses w it h cervical cyst ic hygroma and Turner syndrome. He co nf i r m ed t h at n o ly m p hat i c v eno u s com m u ni cat i o n s w ere p resent n ear t h e jugulosubclavian junct ions on eit her side. Causes of Encephalocele may be[9]
• Neural t ube defect s – spina bifida in 7.3% of cases.
• 75% of cases t here w ill be Occipital bone defect .
• Folate deficiency in early w eeks of gestat ion. Early maternal hypert hermia is one cause in t he genesis of isolated occipital encephalocele[10]. It m ay be u lt rasono graph ical ly d if f i cult t o different iate occipital Encephalocele from cyst ic hygr o m a, t er at o m a, scal p oed em a, haemangioma, brachial cleft cyst and clover leaf skull in t he prenatal period[9].
Com p u t er i sed To m o gr ap hy i s u sef u l b u t M agn et ic Reso n an ce Im agi n g i s best f o r d em o n st r at i n g b r ain t issu e i n t h e Encephalocele[9].
Conflicts of Interests: None
REFERENCES
[ 1] . Davi d P. Zad vi nski s, M anf er d T. Ben so n et .al: Congenit al M alfor m at ions of t he Cervico-t horacic Lym p h at i c sy st e m : Em b r y o l o gy an d Pat hogenesis.Radiographics 1992; 12:1175-1189. [2]. Courtney A. Roeland et .al: Are Encephalocele Neural
Tube Defect s?. Pediat rics,2006;118 (3):916-923. [3] . Sudha Shar m a, M andeep Singh. Anencephaly w it h
Cyst i c Hygr o m a: An t e n at al De t e ct i o n . JK Science,2000; 2 (2):107-109.
[4] . Teague, Kat herine E., et al: Recur rent fetal cyst ic hygrom a w it h norm al chrom osom es: case report and review of t he lit erat ure. Journal of M at ernal-Fet al and Neonatal M edicine 9.6 (2000): 366-369. [5]. Weingast GR. Congenital lym phangiectasia w it h fet al cyst ic hygrom a: r epor t of t w o cases w it h coexist ent Dow n’s syndrom e. JCU 1988; 16:663-668.
[6]. Lee K. Surgery of cyst s and t um ors of t he neck. In: Papar ell a M , Sh unr ick D, ed s. Ot ol ar yngo logy. Phi ladelphia: Saunders, 1980;
[ 7] . Phi l ips H. Int r aut er in e fet al cyst ic hygr om at a: sonographic det ect ion. AJR 1981; 136: 799-802. [ 8] . van den Put t e SCJ. Lym phat ic m alfor m at ion in
hum an fet uses. Virchow s Arch IA 1977; 376:233-246.
[ 9] . Ogbeide,O.U. :Prenatal Ult rasound Diagnosis Of Discordant Occipit al Encephalocele In M ult iple Pr e gn an cy- A Case Re p o r t . Ben i n Jo u r n al o f Post graduat e M edicine 10.1 (2008).
[ 10] .Fisher, Nancy L., and David W. Sm it h: Occipit al e n ce p h al o ce l e an d ear l y gest at i o n al
hyperthermia. Pediatrics 68.4 (1981): 480-483.
CONCLUSION
Feat ures of t he present case w ere suggest ive of a rare var iant of let hal m ult iple pt er ygium syndrom e w it h localized bilat eral (sept at ed) mult ilocular, macrocyst ic postero-lateral cyst ic hygroma of neck w it h occipital Encephalocele. Pr enat al diagnosis of cyst ic hygrom a help obstet rician for planning delivery w hich reduces infant morbidit y and mortalit y. It is even helpful t o d eal w it h Neo n at al co m pl i cat i o n i n consultat ion w it h pediat ric surgeon.
How to cite this article
:
M arut i ram Annamraju, Subhadra Devi Velichet y. DIFFERENTIAL DIAGNOSIS OF A CASE OF BILATERAL CYSTIC SWELLING OF NECK IN AN ABORTED FETUS. Int J Anat Res 2014;2(1):221-24.