www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Impact
of
cartilage
graft
size
on
success
of
tympanoplasty
夽
Waleed
Abdelhameed
∗,
Ibrahim
Rezk,
Alhussein
Awad
SohagUniversity,DepartmentofOtorhinolaryngology,Sohag,Egypt
Received23February2016;accepted19June2016 Availableonline12July2016
KEYWORDS Prospectivestudyof cartilagegraft; Sizeofperforation; Tympanoplasty
Abstract
Introduction:In thelastdecade,therehasbeenanincreasinguseofcartilagegraftsinthe primary repair oftympanic membraneperforations. The majoradvantages ofcartilage are itsstiffnessanditsverylowmetabolicrequirements,whichmakeitparticularlysuitablefor difficultconditions,suchassubtotalperforations,adhesiveotitisandreoperation.
Objective: Toanalyze the impact ofdifferent perforation sizes requiring different sizes of cartilageontheanatomicalandfunctionaloutcomeaftertympanoplasty.
Methods:Throughthisprospectivenon-controlled,non-randomizedstudy,50patients under-wentcartilagetype1tympanoplasty(20femalesand30males),withameanageof19.3±9.8 years.Accordingtosizeofperforation,patientsweresubdividedintothreegroups,GroupIhad perforation>50%oftympanicmembranearea,inGroupIIpatientstheperforationswere25---50% oftympanicmembranearea,andinGroupIIItheperforationswere≤25%oftympanic mem-brane.AllpatientshadpreandpostoperativePureToneAverageandAirBoneGapfrequencies (0.5,1,2,4kHz).Allpatientswerefollowedupatleast12monthsafteroperation.
Results:Theanatomicalsuccessrateamongallpatientswas92%,allgroupsshowedstatistical significantimprovementbetweenpreandpostoperativeairbonegap,nosignificantcorrelation betweensizeofcartilagegraftanddegreeofairbonegapimprovementwasnoticedamong thethreegroups.
Conclusion: Size ofa cartilage graft has no impact on degree of hearing improvement or anatomicalsuccessrateaftertympanoplasty.
© 2016 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Published by Elsevier Editora Ltda. This is an open access article under the CC BY license (http:// creativecommons.org/licenses/by/4.0/).
夽
Pleasecitethisarticleas:AbdelhameedW,RezkI,AwadA.Impactofcartilagegraftsizeonsuccessoftympanoplasty.BrazJ Otorhino-laryngol.2017;83:507---11.
∗Correspondingauthor.
E-mail:[email protected](W.Abdelhameed).
PeerReviewundertheresponsibilityofAssociac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial.
http://dx.doi.org/10.1016/j.bjorl.2016.06.005
PALAVRAS-CHAVE Estudoprospectivode enxertode
cartilagem; Tamanhoda perfurac¸ão; Timpanoplastia
Impactodotamanhodoenxertodecartilagemnosucessodatimpanoplastia
Resumo
Introduc¸ão:Naúltimadécada, temhavidoum interessecrescentenautilizac¸ãodeenxertos decartilagemcomoopc¸ãoparaoreparodeperfurac¸õesprimárias demembranatimpânica. Asprincipaisvantagensdacartilagemsãoasuarigidezemetabolismobraditrófico,oquea tornaparticularmenteadequadaparacondic¸õesdifíceis,taiscomoperfurac¸õessubtotais,otite adesivaereoperac¸ões.
Objetivo:Analisar o impacto de diferentes tamanhos de perfurac¸ão, portanto, diferentes tamanhosdecartilagemsobreodesfechoanatômicoefuncionaldatimpanoplastia.
Método: Através desteestudo prospectivo,não controlado, não randomizado,50 pacientes foramsubmetidosatimpanoplastiadecartilagemtipo1(20mulherese30homens),comidade médiade19,3±9,8anos.Deacordocomotamanhodaperfurac¸ão,ospacientesforam subdi-vididosemtrêsgrupos,GrupoIcomperfurac¸ão>50%daáreadamembranatimpânica,GrupoII comperfurac¸ãode25%-50%daáreadamembranatimpânica,GrupoIIIcomperfurac¸ão≤25% da membrana timpânica.Todos apresentavamAudiometria tonal purapré e pós-operatório - gap Aéreo-Ósseo para frequências testadas (0,5, 1, 2, 4 kHz). Todos os pacientesforam acompanhadosporpelomenos12mesesapósaoperac¸ão.
Resultados: Ataxadesucessoanatômicoentretodosospacientesfoide92%,todososgrupos apresentarammelhoriaestatisticamentesignificanteentrepréepós-operatórionostrêsgrupos, não houvecorrelac¸ãosignificante entreotamanhodoenxerto decartilagemeobservou-se algumgraudemelhoriadogapnos3grupos.
Conclusão:Otamanhodoenxertodecartilagemnãotemimpactosobreograudemelhoriada audic¸ãoounataxadesucessoanatômicoapóstimpanoplastia.
© 2016 Associac¸˜ao Brasileira de Otorrinolaringologia e Cirurgia C´ervico-Facial. Publicado por Elsevier Editora Ltda. Este ´e um artigo Open Access sob uma licenc¸a CC BY (http:// creativecommons.org/licenses/by/4.0/).
Introduction
The fasciatemporalis isthe mostcommonly usedgraft in primarytympanoplasty,withsuccessratebetween93%and 97%,especiallyinwell-aeratedmiddleears.1,2
Inthelastdecade,howevertherehasbeenanincreasing interestinusingcartilagegraftsastheprimaryalternative.3 The major advantages of cartilage are its stiffness and bradytrophicmetabolism, whichmake it particularly suit-ablefor difficultconditions,suchassubtotalperforations, adhesiveotitisandreoperation.4
This material is also characterizedby its resistance to resorption,retractionandnegativepressureinthemiddle ear,itsconnectiontothesurroundingtissueanditselasticity suitableforsoundtransmission.5---8
The sizeof theperforation isthoughttoplay arolein determiningthesuccessofmyringoplasty.Forsomeauthors, largeperforationsareoften associatedwithlowersuccess rate possiblydue to surgical difficulties. Obviously,these perforationsrequiremoregraftmaterialandareoften asso-ciated with poorer condition of the remaining tympanic membrane.9,10
However, for other authors, the preoperative perfora-tionsize does not correlate withthe success rate of the operation.11,12
Manystudiesdiscussedtheeffectofperforationsizeon thesuccessoftympanoplasty.Ourliteraturesearchsuggests nostudieslookedforthesameeffectonusingcartilageas agraft.
Objective
To analyze impact of different perforation sizes hence differentsizesofcartilagegraftontheanatomicaland func-tionaloutcomeoftympanoplasty.
Patients
and
methods
Subjects
A prospective non-controlled, non-randomized study was conducted at ENTdepartment, Sohag University Hospital. The protocol of investigation had been approved by our EthicsofResearchCommittee(Number12/2013).The inves-tigatorshadobtainedwrittenconsentfromeachparticipant or their guardians. It included fifty patients undergoing type 1 cartilage tympanoplasty, fromAugust 2013 toJuly 2014.
Inclusioncriteria:patientswhohadchronicotitismedia, and need type1tympanoplasty, withdry ear,and normal middleearmucosa,atleast3monthspreoperatively.
Exclusion criteria: patients who had previous ear surgery, or requiring concomitant mastoidectomy, those with atalectatic tympanic membranes or with cholesteatoma.
8 7
5
8 13
9
0 2 4 6 8 10 12 14
1 2
3
Females Males
Figure1 Sexofpatientsamongthreegroups,G1(perforation size>50%ofTMarea),G2(perforationsizebetween25%and50% ofTMarea),G3(perforationsize≤25%ofTMarea).
Surgery
Sizeofperforationwascalculatedat timeofoperationby applyinga pieceof Silastictofit snugly withperforation, thentakenoutandmeasuredatlongitudinalandtransverse diameters.Withconsideringthatadulttympanicmembrane size to be 10mm×9mm, patients were subdivided into three groups according to perforation size, Group I with perforationsizemorethan45mm2(>50%oftympanic mem-branearea),GroupIIwithperforationsizebetween23mm2 and45mm2(25---50%oftympanicmembranearea),GroupIII perforationwas≤25%oftympanicmembranearea(23mm2), thisisshowninFig.1andTable1.
Thepatientswereoperateduponbythefirsttwosenior authors,allprocedureswereperformedundergeneral anes-thesia, using a post auricular approach, and grafts from tragus were harvested. The cartilage thickness did not exceed0.5mm.
The cartilage perichondrium graft was prepared by dissecting perichondrium off one side only, keeping the attachmentof other side, thegraft wasplacedby under-lay technique withelevated perichondriumdraping on to posteriorcanalwall.
Outcomemeasures
Wemeasured anatomical andfunctional success, thefirst wasdefinedasfullhealingofgraftedtympanicmembrane foratleast12monthspostoperatively.
Patientsrepeatedtheaudiogramat 6.9months postop-eratively;hearingoutcomeswerecalculatedfromthemost recentaudiogram,bycomparingpreandpostoperativePure Tone Average---AirBone Gap (PTA---ABG), hearing gain was definedasthedifferencebetweenboth.
Statisticalanalysis
DatawereanalyzedusingStatisticalPackagefortheSocial Sciencesversion18.0(SPSSInc,Chicago,IL,USA).Weused pairedt-test forstudying change ofPTA---ABG,andpartial correlationtostudy therelation betweensizeofcartilage graftanddegreeofimprovementinABG.Accordingto num-bersof16,20and14patientsinthethreestudiedgroups, thepowerofstudywas0.95033(95%).
Results
Fifty patients underwent cartilage tympanoplasty (20 females and 30 males),their age range was(9---65 years) withameanof19.3±9.8years.Thirtysevenpatientshad unilateralperforation,while13hadbilateral perforations. Hearinglosswasthemainsymptomin(82%),recurrent otor-rheain (75%), and tinnitusin (9%) of patients. Right side wasthe operated sidein 21patients, andleftside inthe remaininggroup.Patients’datawereshowninTable1.All patientswerefollowedupatleast12monthsafteroperation withrange(12---20months),withnorecordedlostfollowup amongthem.
Theanatomicalsuccessratedefinedasgrafttakeafter12 monthsoffollowup,amongallpatientswas92%,4patients underwentrevision surgery10---12monthspostoperatively. Twoof them werein firstgroup, andone patientin each remaininggroups,nostatisticaldifferencewasnotedamong thethreegroupsregardingfailurepercentage.
Regardingfunctionaloutcome,allgroupsshowed statisti-calsignificantimprovementbetweenpreandpostoperative (PTA---ABG),themeanABGpreoperativelyinallpatientswas 22.5dB, thatof postoperative was12.6dB (p=0.000), for
Table1 Demographiccharactersofpatientsamongthreegroups.
Sex Meanage Meanperforationsize MeanABGdiff.
Firstgroup(>50%ofTMarea)
Males8 19.6±6.07y 51.8±10.41mm2 9.53±5.6dB Females8
Secondgroup(25---50%ofTMarea)
Males13 20.2±11.65y 32.15±5.64mm2 10.76±6.59dB Females7
Thirdgroup(≤25%ofTMarea)
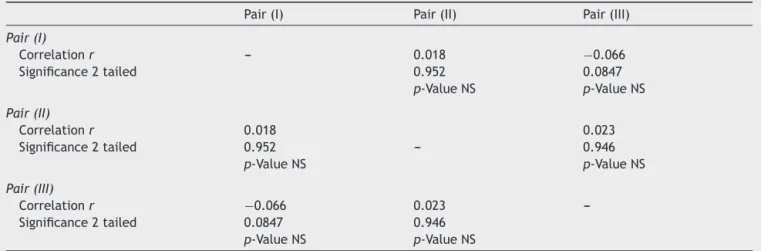
Table2 ThepartialcorrelationbetweensizeofperforationandABGimprovementpostoperativelybetweenthreegroups. Pair(I) Pair(II) Pair(III)
Pair(I)
Correlationr --- 0.018 −0.066
Significance2tailed 0.952 0.0847
p-ValueNS p-ValueNS
Pair(II)
Correlationr 0.018 0.023
Significance2tailed 0.952 --- 0.946
p-ValueNS p-ValueNS
Pair(III)
Correlationr −0.066 0.023
---Significance2tailed 0.0847 0.946
p-ValueNS p-ValueNS
EachpairrepresentsmeanofsizeofperforationofthatgroupwithmeanofABGimprovementinsamegroup;r,correlationcoefficient;
p-valuebetweengroups>0.05NS(nonsignificant).
12.6 22.5
11.2 22.2
13.4 23.4
21.36
12.18
0 5 10 15 20 25
Post All Pre All Post G3 Pre G3 Post G2 Pre G2 Post G1 Pre G1
Figure2 ABG mean indBs pre and postoperatively ofthe threegroups,andforthetotalnumberofpatients.
each group the ABG pre and postoperatively is shown in
Fig.2.The meanof ABGdifference(Pre-Postop) wasalso demonstratedinTable1.
On searching for the correlation between the sizes of perforation, hence size of cartilage graft, and degree of improvementinABG,nosignificantcorrelationwasnoticed, amongthethreegroupsasoutlinedinTable2.
Discussion
Amorerigid,andmoreresorption-andretraction-resistant graft material, may provide better success rate. There-fore, cartilage graft materials are preferred for large perforations.13Kazikdasetal.found95.7%graftsuccessrate forpalisadecartilagegraft,comparedwith75%for tempo-ralisfasciagrafts.14
Theanatomicalsuccessrateinourpatientswas92%,this iscomparablewithratesmentionedinliteraturefor carti-lagetympanoplasty,93%instudyofYurttasetal.and92.3% instudybyOnaletal.13,15
Previous studies have assessed the relationship between the size of tympanic membrane perforations andhearingloss,withconflictingdataandwithoutproper methodology.16
Intheliterature,Pannuetal.reporteddifferentresults, demonstratingan increase in hearing loss withincreasing
sizesoftympanicperforationin100patients.17Also,Ibekwe etal.analyzed67patientswithatotalof77perforations, theyconcludedthatthelargerthetympanicmembrane per-foration,thegreaterthelossinsoundperception.18
On the other hand, Ribeiro et al. found nosignificant relationshipbetweenthesizeoftympanicperforationsand hearing loss in the four analyzed frequencies 0.5, 1, 2, 4kHz.16 We searched for the link betweencartilage graft sizeandchangeofABGaftertympanoplasty, Noimpactof sizeofcartilage graftondegreeof ABGimprovementwas revealed.
Ifa largercartilage plateis used for reconstruction, a smaller thickness of transplant is necessary. For optimal acoustic transferbehavior, thecartilage shouldbe cut as thinlyaspossible,19soweusedcartilagegraftwiththickness notmorethan0.5mm.
Gerberetal.mentioned that replacingalarge portion of tympanicmembrane withcartilagewould add stiffness and/or massthatwould affectindividualfrequencies, but not significantly impact averaged audiometric data such as air bone gap.20 Our work proved that, as significant improvementofABGwasachievedamongthethreegroups postoperatively.
Our patients with big sized perforation showed least improvementofABGcomparedwithothergroups.Thismay be explained according to the hypothesis that increasing sizeofperforationwillincreasethedegreeofhearingloss. But their significant improvement of ABGpostoperatively, proves alsothat cartilagesize hasnoimpactonaveraged audiometricdatasuchasABG.
On studying the correlation between size of graft and degree of improvement of ABG, nosignificant correlation was found. This is coinciding with hypothesis of Ribeiro et al. who did not find any correlation between size of perforation and degree of hearingloss amongfour tested frequencies.16
Conclusion
Size of cartilage graft has no impact on degree of hearingimprovementoranatomicalsuccessrateafter tym-panoplasty.
Limitations
To make our results more generalized,we need to inves-tigate higher numberof patients. This is not feasible, as cartilageisnotthesolegraftingmaterialusedatour depart-ment.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgments
This work wasdone in ENTDepartment,Sohag Facultyof Medicine,Sohag,Egypt.Onthepatientswhohadtype1 Car-tilageTympanoplastySurgeryintheperiodbetweenAugust 2013andJuly2014.
The authors assert that all procedures contributing to this work comply with the ethical standards of relevant nationalandinstitutionalguidelinesonhuman experimen-tation (Ethics of Research Committee, Sohag Faculty of Medicine),andwithHelsinkideclarationof1975asrevised in2008.
References
1.MohamadSH,Khan I,Hussain SS. Iscartilage tympanoplasty moreeffectivethanfasciatympanoplasty?Asystemicreview. OtolNeurotol.2012;33:699---705.
2.Lee JC, Lee SR, Nam JK, Lee TH, Kwon JK. Comparison of different grafting techniques in type 1 tympanoplasty in cases of significant middle ear granulation. Otol Neurotol. 2012;33:586---90.
3.De Freitas MR, De Oliveira TC. The role of different types of grafts in tympanoplasty. Braz J Otorhinolaryngol. 2014;80:275---6.
4.Neumann A, Kevenhoerster K, Gostian AO. Long term results of palisade cartilage tympanoplasty. Otol Neurotol. 2010;31:936---9.
5.VelepicM,Starcevic R,TicacR, KujundzicM.Cartilage tym-panoplasty in children and adults: long term results. Int J PediatrOtorhinolaryngol.2012;76:663---6.
6.Yilmaz MS, Guven M, Kayabasoglu G, Varli A. Comparison of the anatomic and hearing outcomes of cartilage type 1 tympanoplastyinpediatricandadultpatients.EurArch Otorhi-nolaryngol.2013;27:113---6.
7.HartzellLD,DornhofferJL.Timingoftympanoplastyinchildren withchronicotitismediawitheffusion.CurrOpinOtolaryngol HeadNeckSurg.2007;137:284---8.
8.Nicholas BD, O’Reilly RC. Is cartilage preferable to fascia myringoplastyinchildren?Laryngoscope.2010;120:2136---7.
9.Knapik M, Saliba I. Pediatric myringoplasty: study of fac-tors affecting outcome. Int J Pediatr Otorhinolaryngol. 2011;75:818---23.
10.OnalK,UguzMZ,KazikdasKC,GursoyST,GokeH.A multivari-ateanalysisofotological,surgicalandpatientsrelatedfactors in determining success in myringoplasty. Clin Otolaryngol. 2005;30:115---20.
11.UyarY,KelesB,KocS,OzturkK,ArbagH.Tympanoplastyin pedi-atricpatients.IntJPediatrOtorhinolaryngol.2006;70:1805---9.
12.CaslinM,O’ReillyRC, MorletTT,McCormickM.Pediatric car-tilageinterleavetympanoplasty.OtolaryngolHeadNeckSurg. 2007;137:284---8.
13.YurttasV, YakutF, KutluhanA, Bozdemir K. Preparation and placementof cartilage islandgraft in tympanoplasty.Braz J Otorhinolaryngol.2014;80:522---7.
14.Kazikdas KC, Onal K, Boyraz I, Karabulut E. Cartilage tympanoplasty for management of subtotal perforations: a comparison with the temporalis fascia technique. Eur Arch Otorhinolaryngol.2007;264:985---9.
15.Onal K, Arslanoglu S, Songu M,Demiray U, DemirpehlivanI. Functional results oftemporalis fascia versus cartilage tym-panoplasty in patientswithbilateral chronic otitismedia. J LaryngolOtol.2012;126:22---5.
16.RibeiroFA,GaudinoVR,PinheiroCD,MarcalGJ,MitreEL. Objec-tivecomparisonbetweenperforationandhearingloss.BrazJ Otorhinolaryngol.2014;80:386---9.
17.PannuKK,ChadhaS,KumarD,PreetiD.Evaluationofhearing lossintympanicmembraneperforation. IndianJOtolaryngol HeadNeckSurg.2011;63:208---13.
18.IbekweTS,NwaorgaOG,IjaduolaTG. Correlatingthesizeof tympanic membrane perforationwith hearing loss. BMC Ear NoseThroatDisord.2009;9:1.
19.LeeCF,ChenJH,ChouYF,Hsu LP,ChenPR,LiuTC. Optimal graftthicknessfordifferentsizesoftympanicmembrane per-forationincartilagetympanoplasty:afiniteelementanalysis. Laryngoscope.2007;117:725---30.