www.bjorl.org
Brazilian
Journal
of
OTORHINOLARYNGOLOGY
ORIGINAL
ARTICLE
Association
between
maternal
smoking,
gender,
and
cleft
lip
and
palate
夽
,
夽夽
Daniella
Reis
Barbosa
Martelli
a,
Ricardo
D.
Coletta
b,
Eduardo
A.
Oliveira
c,
Mário
Sérgio
Oliveira
Swerts
d,
Laíse
A.
Mendes
Rodrigues
a,
Maria
Christina
Oliveira
c,
Hercílio
Martelli
Júnior
a,d,∗aCiênciasdaSaúde,CentrodeCiênciasBiológicasedaSaúde,UniversidadeEstadualdeMontesClaros(Unimontes),Montes
Claros,MG,Brazil
bPatologiaBucal,FaculdadedeOdontologiadePiracicaba,UniversidadeEstadualdeCampinas(UNICAMP),Piracicaba,SP,Brazil cPediatria,FaculdadedeMedicinadaUniversidadeFederaldeMinasGerais(UFMG),BeloHorizonte,MG,Brazil
dUniversidadeJosédoRosárioVellano(UNIFENAS),Alfenas,MG,Brazil
Received29March2014;accepted7September2014 Availableonline22July2015
KEYWORDS
Cleftlip; Cleftpalate; Smoking; Pregnancy
Abstract
Introduction:Cleftlipand/orpalate(CL/P)representthemostcommoncongenitalanomalies oftheface.
Objective:Toassesstherelationshipbetweenmaternalsmoking,genderandCL/P.
Methods: Thisisanepidemiologicalcross-sectionalstudy.Weinterviewed1519mothersdivided intotwogroups:Cases:mothersofchildrenwithCL/P(n=843)andControls:mothersofchildren withoutCL/P(n=676).Allmotherswereclassifiedassmokerornon-smokersubjectsduringthe firsttrimesterofpregnancy.Todetermineanassociationamongmaternalsmoking,gender,and CL/P,oddsratioswerecalculatedandtheadjustmentwasmadebyalogisticregressionmodel. Results:An associationbetweenmaternal smokingandthepresenceofcleftwasobserved. Therewasalsoastrongassociationbetweenmalegenderandthepresenceofcleft(OR=3.51; 95%CI2.83---4.37).Bybinarylogisticregressionanalysis,itwasdemonstratedthatbothvariables wereindependentlyassociatedwithclefts.Inamultivariateanalysis,malegenderandmaternal smokinghada2.5-anda1.5-timegreaterchanceofhavingacleft,respectively.
夽
Pleasecitethisarticleas:MartelliDRB,ColettaRD,OliveiraEA,SwertsMSO,RodriguesLAM,OliveiraMC,etal.Associationbetween maternalsmoking,gender,andcleftlipandpalate.BrazJOtorhinolaryngol.2015;81:514---9.
夽夽Institution:ProgramadePós-graduac¸ãoemCiênciasdaSaúdedaUniversidadeEstadualdeMontesClaros(Unimontes),MontesClaros,
MG,Brazil.
∗Correspondingauthor.
E-mail:[email protected](H.MartelliJúnior).
http://dx.doi.org/10.1016/j.bjorl.2015.07.011
Conclusion: Ourfindingsareconsistentwithapositiveassociationbetweenmaternalsmoking during pregnancy andCL/Pinmale gender.The resultssupport theimportanceof smoking preventionandintroductionofcessationprogramsamongwomenwithchildbearingpotential. © 2015Associac¸ãoBrasileira de Otorrinolaringologiae CirurgiaCérvico-Facial. Publishedby ElsevierEditoraLtda.Allrightsreserved.
PALAVRAS-CHAVE
Fendalabial; Fendapalatina; Hábitodefumar; Gravidez
Associac¸ãoentretabagismomaterno,gêneroefendaslabiopalatinas
Resumo
Introduc¸ão: Fendas labiaise/ou palatinas(FL/P) representamasanomaliascongênitasmais comunsdaface.
Objetivo: Avaliararelac¸ãoentretabagismomaterno,gêneroeFL/P.
Método: Realizou-se um estudo epidemiológico, de corte transversal. Foram entrevistadas 1.519mães,divididasemdoisgrupos:Casos:mãesdecrianc¸ascomFL/P(n=843);eControles: mãesdecrianc¸assemFL/P(n=676).Todasasmãesforamclassificadascomofumantesounão fumantesduranteoprimeirotrimestredegravidez.Paradeterminaraassociac¸ãoentre tabag-ismomaterno,gêneroeFL/P,oddsratiosforamcalculadaseoajusterealizadopelomodelode regressãologística.
Resultados: Observou-seassociac¸ãoentretabagismomaterno,efendas.Houvetambémforte associac¸ãoentresexomasculinoepresenc¸adefendas(OR=3,51;95%IC2,83---4,37).Regressão logísticabináriademonstrouqueambasasvariáveisforamindependentementeassociadascom aocorrênciadefendas.Naanálisemultivariada,osexomasculinoteve2,5vezesmaischance deapresentarfendasetabagismomaternoteve1,5vezmaischancedessaocorrência. Conclusão:Osresultadossãoconsistentescomaassociac¸ãopositivaentretabagismomaterno durantea gravideze aocorrência deFL/P nogênero masculino. Osresultados suportam a importânciadaprevenc¸ãodotabagismoeaaplicac¸ãodeprogramasentremulherescom poten-cialdegravidez.
©2015Associac¸ãoBrasileiradeOtorrinolaringologiaeCirurgiaCérvico-Facial.Publicado por ElsevierEditoraLtda.Todososdireitosreservados.
Introduction
Nonsyndromiccleftlipand/orpalate(NSCL/P,MIM#119530) represents the most frequent congenital malformationin theheadandneckregion,withaprevalencerangingfrom 1:500to1:2500livebirths.1Itsprevalencevariesaccording
toethnicity(Africans0.3:1000;Europeans1.3:1000;Asians
2.1:1000; Native Americans 3.6:1000) and socioeconomic
level.2InBrazil,theprevalenceofNSCL/Prangesfrom0.36
to1.54:1000livebirths.3,4
NSCL/Pisanimmediatelyrecognizabledisruptionof
nor-malfacialstructure.Althoughnotamajorcauseofmortality
in developed countries, NSCL/P does cause considerable
morbidity in affected children and imposes a substantial
financial burden, especially for families of low
socioeco-nomic status.5 Individuals with NSCL/P may experience
problems withfeeding, speaking, hearing, social
integra-tion,andcancer.1,6
NSCL/P etiology,whichinvolves both geneticand
envi-ronmental factors, is highly complex; its molecular basis
remainslargelyunknown.2,7Theidentificationofmodifiable
riskfactorsforNSCL/Pisthefirststeptowardprimary
pre-vention.Riskfactorssuchasmaternalexposuretotobacco
smoke,alcohol use,poor nutrition,gender, maternal age,
viral infection, medicinal drugs, and teratogens in the
workplaceor at home in early pregnancy have previously
beeninvestigated.1,8---11
Theassociation betweenmaternalsmokingandNSCL/P
hasbeen assessedinmanystudies,andameta-analysisof
thesestudies suggestsapositiveassociation.12,13 Different
studieshavebeenconductedworldwidetoevaluateNSCL/P
distribution,oftenresultinginvaryingprevalencerates.14,15
Ina Brazilian population study,predominance of cleft lip
andpalate(52.6%)wasdemonstrated,followedbycleftlip
(33.12%)andcleftpalate(14.28%).16Theincidenceofcleft
lipandpalateandcleftlipisgreaterinmales,whilecleft
palateshowsprevalenceinfemales.16,17
Very fewstudies have evaluatedthe influenceof
envi-ronmentalfactorsin theBrazilianNSCL/Ppopulation. The
purpose of this study was to evaluate the relationship
betweenmaternalsmoking,gender,andNSCL/Pina
Brazil-ianpopulation.
Methods
The design of the study was an epidemiological,
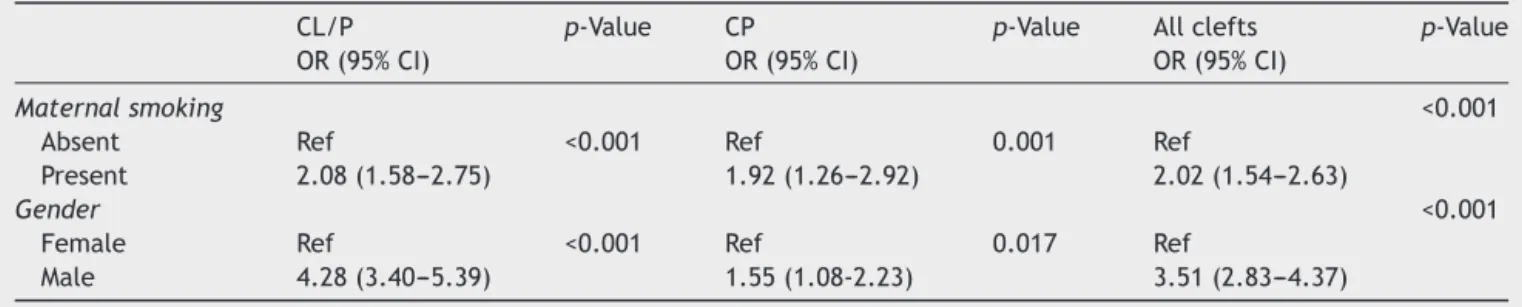
Table1 Univariateanalysisofthedistributionofcleftlipwithorwithoutcleftpalate(CL/P),cleftpalate(CP),andallclefts accordingtomaternalsmokingstatusandinfantgender.
CL/P p-Value CP p-Value Allclefts p-Value
OR(95%CI) OR(95%CI) OR(95%CI)
Maternalsmoking <0.001
Absent Ref <0.001 Ref 0.001 Ref
Present 2.08(1.58---2.75) 1.92(1.26---2.92) 2.02(1.54---2.63)
Gender <0.001
Female Ref <0.001 Ref 0.017 Ref
Male 4.28(3.40---5.39) 1.55(1.08-2.23) 3.51(2.83---4.37)
from the same institution (Centre for Rehabilitation of Craniofacial Anomalies and Dental Clinics, State of Minas Gerais, Brazil), between February 2009 and August 2012, in an attempt to select cases and control individualswithsimilarethnicitiesandsocial-culture back-grounds.
Theauthorsinterviewed1519mothers,whoweredivided into twogroups: cases: mothers of children with NSCL/P (n=843);andcontrols:mothersofchildrenwithoutNSCL/P (n=676).Allmotherswerefurtherclassifiedassmokersor non-smokersduringthefirsttrimesterofpregnancy.All chil-dren with associated anomalies or syndromes or a family historyofgeneticdiseaseswereexcluded fromthisstudy. ThemothersofchildrenwithNSCL/Pwereevaluatedinthe Centerfor Rehabilitationof Craniofacial Anomalies, while themothersofchildrenwithoutNSCL/Pwereevaluatedin dentalclinics.
The clefts were categorized into three groups, with the incisive foramen as reference: (1) cleft lip (CL): includescompleteorincompletepre-foramenclefts,either unilateral or bilateral; (2) cleft lip and palate (CLP): includes unilateral or bilateral transforamen clefts and pre-or post-foramenclefts;(3)cleft palate(CP):includes all post-foramen clefts, complete or incomplete.18 For
analysis purposes, CL and CLP (CL/P---cleft lip with or
without cleft palate) were merged as one group, with
CP as the other group.11,19 The children were evaluated
by professionals with considerable experience with oral
cleft.
Theinformationcollectedwasstoredinadatabaseand
analyzedusingSPSS® version18.0(SPSSforWindows).The
analysiswasconductedintwosteps.Statisticalanalysiswas
initiallybasedonthepresentationofdescriptivedataand
the distribution of categorical variables. Prevalence odds
ratio(OR)and95%confidenceintervals(95%CI)wereused
todetermineassociationsamongmaternalsmoking,gender,
andoccurrenceofNSCL/P.Theassociationbetween
mater-nalsmokingandcleftswastestedineachgenderseparately.
Next,the association between the gender andthe
occur-renceofNSCL/Pwastestedseparatelyamongthosewhose
motherssmoked and amongthosewhose mothers didnot
smoke.Finally, alogistic regression modelwasapplied to
identifyvariablesthatwereindependentlyassociatedwith
occurrenceofNSCL/P.
This study was approved by the Ethics Committee in
Researchof the University (#259-2010). Informed consent
wasobtainedfromsubjectsorguardiansbefore
participat-inginthestudy.
Results
A total of 1519 women were interviewed, including 680
mothers of infants with nonsyndromic CL/P, 163
moth-ers of infants with nonsyndromic CP, and 676 mothers of
infantswithnomajorbirthdefects(controls).Of1519
chil-dren included in the analysis, therewas a predominance
offemales (57%).Ofthesechildren,843 presentedclefts,
including680bornwithCL/Pand163 withisolatedCP.Of
the 1519mothers, 307(20%) weresmokers,with212/843
(25%) in the case group and 95/676 (14%) in the control
group.Therewasanassociationbetweenmaternalsmoking
andclefts(OR=2.02;95%CI1.54---2.63).Maternalsmoking
wasalsoassociatedwithCL/P(OR=2.08;95%CI1.58---2.75)
and with CP(OR=1.92; 95% CI 1.26---2.92) (Table 1). The
majorityofinfantswithCL/Pweremale(61%),andfemales
predominated amongchildrenwithCP(63.8%).Therewas
alsoastrongassociationbetweenmalegenderandthe
pres-enceofclefts(OR=3.51;95%CI2.83---4.37).Thisassociation
wasconsistent amongthe differenttypes ofclefts (CL/P:
OR=4.28;95%CI3.40---5.39;CP:OR=1.55;95%CI1.08---2.23)
(Table1).
Association between maternal smoking and clefts was
assessed in each gender separately. Although maternal
smoking increasedthe risk of clefts in both genders, this
increasewassignificantonlyforfemales(OR=2.48;95%CI
1.73---3.54) (Table 2). By contrast, there was an
associa-tion between malegender and clefts amongthosewhose
mother smoked and among those whose mothers did not
smoke.It wasfound thattheoccurrence ofcleft was
sig-nificantlyhigherinmalesbothamongthosewhosemother
smoked and among those whose mothers did not smoke
(mother smokes: OR=2.10; 95% CI 1.28---3.45 and
non-smokersmother:OR=3.89;95%CI3.05---4.97).
By binary logistic regression analysis, it was
demon-stratedthatbothvariables(genderandmaternalsmoking)
were independently associated with clefts. In this
mul-tivariable analysis, the male gender had approximately
2.5-foldgreaterchanceofclefts(OR=2.39;95%CI2.0---2.87;
p<0.001) and maternal smoking had 1.5 times greater
chance (OR=1.49; 95% CI 1.15---1.93; p=0.002). Of note,
therewasanincreasingoddsratioacrosssubgroups
strati-fiedbygenderofthechildrenandmaternalsmokingstatus:
female/non-smokingmother(OR=0.63;95%CI0.54---0.73),
female/smoking mother (OR=1.56; 95% CI 1.13---2.16),
male/non-smoking mother (OR=2.43; 95% CI 2.01---2.95),
and male/smoking mother (OR=3.37; 95% CI 2.31---4.91)
Table2 Analysesoftheassociationbetweenmaternalsmokingandtheoccurrenceofnonsyndromiccleftlipand/orpalatein eachgenderseparately,aswellasassociationbetweengenderandtheoccurrenceofcleftsinrelationtomaternalsmoking.
Variable Case Control OR 95%CI p
Female
Non-smokingmother 275 435 1.00
Mothersmokes 94 60 2.48 1.73---3.54 <0.001
Male
Non-smokingmother 356 146 1.00
Mothersmokes 118 35 1.38 0.90---2.12 0.149
Non-smokingmother
Female 275 435 1.00
Male 356 146 3.85 3.02---4.92 <0.001
Mothersmokes
Female 94 60 1.00
Male 118 35 2.15 1.30---3.53 0.003
5
4
3
Odds r
atio
2
1
0
ns/female Smoking/female ns/male Smoking/male
Risk groups
Figure1 Associationbetweenmaternalsmokingstatusandgenderwiththepresenceoffacialcleftdeformities(ns,non-smoking). Thesquaresrepresentthe95%confidenceintervals.
simultaneouseffectsofbothvariablesstratifiedintothese foursubgroups.
Discussion
Thepatientsdescribedinthisstudywererecruitedfromthe Centerfor Rehabilitationof Craniofacial Anomalies,Minas GeraisState, Brazil. ThisService is considered oneof the largestcleftrepaircentersinBrazil,andperformsall proce-duresofrehabilitationthatpassthroughtheBrazilianPublic HealthSystem.9,11Withapopulationexceeding190million
and3millionbirthseveryyear,NSCL/Pisanimportant
pub-lichealth probleminBrazil,withapproximately4000new
casesofNSCL/Peveryyear.11
Although the environmental and genetic risk factors
associated with NSCL/P remain unclear, the
understand-ing of the mechanisms involved in this malformation is
evolving.1,2 Maternal smoking has been repeatedly
asso-ciated with increased risk of NSCL/P, and meta-analysis
supportsanoverallORforhavingcleftsof∼1.3among
off-spring of mothers who smoke.12,20,21 The present findings
confirm the literature data. In this analysis, the chance
of cleft in the children whose mothersmoked was2-fold
greater compared with children of non-smoking mothers.
Littleetal.12performedameta-analysisoftheassociation
betweenmaternalsmokingduringpregnancyandoralclefts
usingdatafrom24case-control andcohortstudies. A
rel-ative risk of 1.34 (95% CI 1.25---1.34) wasfound between
maternalsmokingandCL/Pandarelativeriskof1.22(95%
CI1.10---1.35)betweenmaternalsmokingandCP.Similarly,
Honeietal.13haveshownthatpericonceptionalsmokingwas
associatedwith CLP (OR=1.3; 95% CI 1.0---1.6),and more
stronglyassociated withbilateral CLP (OR=1.7; 1.2---2.6),
withaweakerassociationobservedforCP.
Cigarette smoke contains nicotine,polycyclic aromatic
hydrocarbons,tar,carbonparticles,andcarbonmonoxide.
Theexposureofembryonictissuesdependsonthenumber
ofcigarettessmoked,frequencyofpuffing,depthof
inhala-tion, and maternal embryonic transfer and metabolism.
The mechanisms by which cigarette smoke detrimentally
affectspregnancyoutcomeareinadequatelyunderstood.22
Increased risks from exposure to maternal smoking
dur-ingpericonceptionalperiodraisethepossibilitythatgenes
in certain metabolic pathways may play a role in the
developmentofNSCL/P.Specifically,markersintheGSTT1
(glutathioneS-transferasetheta)orNOS3(nitricoxide
presenceofmaternalsmoking.20,21,23TheGSTT1markersare
genedeletionvariants,whichsuggestdeficienciesin
detox-ificationpathwaysmayunderliesomeofthesusceptibility.
Smokinghasalsorecentlybeen associatedwithvariantsin
theIRF6gene.17
Withrespecttothedistributionofcleftsinthetwogroups
(CL/P and CP), it wasfound thatof the843 NSCL/P, 680
(80.7%) were CL/P and 163 (19.3%) were isolated CP. In
most published studies, the percentage of subjects with
CL/PwashighercomparedtothatofCPalone,includingthe
Brazilianstudies.24,25Thepresentauthorsgroup,inanother
study,found similar results in the distribution of NSCL/P
(CL/P=81.61% andCP=18.37%).11 Among the843children
with clefts evaluated, 474 (56.2%) were male and 369
(43.8%)werefemale.Inanotherstudy,itwasdemonstrated
that CP was more frequent in females (28.7% vs. 13.6%;
1.77:1),whileCLP(59.8%vs.45.5%;1.56:1)andCL(25.7%
vs. 26.6%; 1.23:1) predominated in males (p=0.001).17 It
was also determined, by multinomial logistic regression,
that the chance of occurrence of CL in males was
2.19-foldhigherin relation toCPin females, while therisk of
CLP in males was2.78-fold higher than the risk of CP in
females.16Inwhitepopulations,thismajorityofmaleswith
CL/Pbecomesmoreevidentwiththeincreasingseverityof
thecleftandlessevidentwhenmorethanonesiblinginthe
familyisaffected.26
Recently,Leietal.27 haveshown,inapopulation-based
epidemiologicalstudyinTaiwan,thathigherprevalenceof
CL/PorCPwasobservedwithmultiplepregnancies,being
male for CL/P, being female for CP, gestational age ≤37
weeks,andlowerbirthweight(<1.5kg).Accordingtotheir
findings,malenewbornsandfemalenewbornswerestrongly
associatedwithCL/PandCP,respectively(bothp<0.0001).
In the present analysis, maternal smoking increased the
chanceofcleftsinbothgenders;however,thisincreasewas
significant onlyfor females (OR=2.48; 95% CI1.73---3.54).
Possibly,thisfindingisrelatedwiththefactthattherewas
anassociationbetweenmalegenderandcleftsamongthose
whosemothersmokedandamongthosewhosemothersdid
not smoke. Of particular interest, when this sample was
stratified by maternal smoking status and child’s gender,
therewasaconsistentincreasinoddsratioacrossthe
sub-groups,from thematernal non-smoking/female gender to
thematernalsmoking/malegenderpairs.
Concerning the limitations of this study,there was no
quantitative assessment of maternal exposure to passive
smoking, quantification of the number of cigarettes
con-sumedbythemother,andthedurationofthesmokinghabit.
In addition, the database did not provide information on
maternal conditions and perinatal features (suchas birth
weightandgestationalage),whichclearlymayplayarole
indevelopmentoffacialcleftdeformities.Limitationsstill
existbetweenthepairingsmadebetweenthecaseand
con-trolgroups,eventhoughconductedatthesameinstitution.
Conclusion
In summary, these findings are consistent with a positive
association between maternal smoking during pregnancy
andNSCL/Pintheoffspring.Itisalsonotedthatmale
chil-drenhavea3.5-foldgreaterchanceofbeingbornwithclefts
comparedwithfemales.Theidentificationofmodifiablerisk
factorsforNSCL/P,suchasmaternalsmoking,isthefirststep
towardprimaryprevention.Theconsistencyofthefindings
for NSCL/P andmaternal smokingsuggests anopportunity
for prevention of these serious defects. The results
pre-sentedheresupporttheimportanceofsmokingprevention
andcessationprogramsamongallwomenwithchildbearing
potential.
Funding
This study was supported the by Fundac¸ão de Amparo
à Pesquisa do Estado de Minas Gerais --- FAPEMIG
Pro-cad/Casadinho---CNPq-Capes.
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Acknowledgments
This work wassupported by grants fromthe Minas Gerais
StateResearchFoundation---FAPEMIG,Brazil;theNational
Council for Scientific and Technological Development
---CNPq,Brazil;the Coordinationfor Improvementof Higher
EducationPersonnel(CAPES),Brazil;andProcad/Casadinho
---Capes/CNPq.
References
1.Dixon MJ,Marazita ML, Beaty TH, Murray JC. Cleft lipand palate: understandinggeneticand environmental influences. NatRevGenet.2011;12:167---78.
2.RahimovF,JugessurA,Murray JC.Geneticsofnonsyndromic orofacialclefts.CleftPalateCraniofacJ.2012;49:73---91.
3.Martelli-JuniorH,PortoLV,MartelliDR,BonanPR,FreitasAB, Coletta R.Prevalence of nonsyndromicoral cleftsina refe-rencehospital in thestate ofMinasGerais, Brazil,between 2000---2005.BrazOralRes.2007;21:314---7.
4.Rodrigues K, Sena MF, Roncalli AG, Ferreira MA. Prevalence oforofacial cleftsandsocialfactorsinBrazil.BrazOralRes. 2009;23:38---42.
5.WehbyG,CassellCH.Theimpactoforofacialcleftsonquality oflifeandhealthcareuseandcosts.OralDis.2010;16:3---10.
6.VieiraAR,KhaliqS,LaceB.Riskofcancerinrelativesof chil-drenbornwithisolatedcleftlipandpalate.AmJMedGenetA. 2012;158:1503---4.
7.Brito LA, Paranaiba LMR, Bassi CFS, Massoti C, Malcher C, SchesingerD,et al.Region 8q24 isa susceptibility locusfor nonsyndromicoralcleftinginBrazil.BirthDefectsResA:Clin MolTeratol.2012;94:464---8.
8.BoylesAL,DeRooLA,LieRT,TaylorJA,JugessurA,MurrayJC, etal.Maternalalcoholconsumption,alcoholmetabolismgenes, andtheriskoforalclefts:apopulation-basedcase-controlstudy inNorway,1996---2001.AmJEpidemiol.2010;172:924---31.
9.Bufalino A, Paranaíba LMR, Aquino SN, Martelli-Júnior H, SwertsMSO,ColettaRD.Maternalpolymorphismsinfolicacid metabolic genes are associated with nonsyndromic cleft lip and/orpalateintheBrazilianpopulation.BirthDefectsResA: ClinMolTeratol.2010;88:980---6.
11.Martelli DRB, Cruz KM, BarrosLM, Silveira MF, Swerts MSO, Maternal Martelli-Júnior H. paternal age, birth order and interpregnancyintervalevaluationforcleftlip-palate.BrazJ Otorhinolaryngol.2010;76:107---12.
12.LittleJ,CardyA,MungerRG.Tobaccosmokingandoralclefts: ametaanalysis.BullWorldHealthOrgan.2004;82:213---8.
13.Honein MA, Rasmussen SA, Reefhuis J, Romitti PA, Lammer EJ, Correa A. Maternal smoking and environmental tobacco smokeexposureandtheriskoforofacialclefts.Epidemiology. 2007;18:226---33.
14.ChristensenK,JuelK,HerskindAM,MurrayJC.Longtermfollow upstudyofsurvivalassociatedwithcleftlipandpalateatbirth. BMJ.2004;328:1405.
15.DerijckeA,EerensA,CarelsC.Theincidenceoforalclefts:a review.BrJOralMaxillofacSurg.1996;34:488---94.
16.Martelli DR, Machado RA, Swerts MS, Rodrigues LA, Aquino SN, Martelli-Júnior H. Non-syndromic cleft lip and palate: relationshipbetweensexandclinicalextension.BrazJ Otorhi-nolaryngol.2012;78:116---20.
17.WuT,LiangKY,HetmanskiJB,RuczinskiI,FallinMD,Ingersoll RG,etal.EvidenceofgeneenvironmentinteractionfortheIRF6 geneand maternal multivitaminsupplementation in control-lingtheriskofcleftlipwith/withoutcleftpalate.HumGenet. 2010;128:401---10.
18.SpinaV,PsillakisJM,LapaFS,FerreiraMC.Classificationofcleft lipandcleftpalate.Suggestedchanges.RevHospClinFacMed SaoPaulo.1972;27:5---6.
19.Christensen K, Fogh-AndersenP. Cleft lip(+/− cleft palate) in Danish twins, 1970---1990. Am J Med Genet. 1993;47: 910---6.
20.ShiM,ChristensenK,WeinbergCR,RomittiP,BathumL,Lozada A,etal.Orofacialcleftriskisincreasedwithmaternal smok-ingandspecificdetoxificationgenevariants.AmJHumGenet. 2007;80:76---90.
21.ShiM,ChristensenK,WeinbergCR,RomittiP,BathumL,Lozada A,etal.Reviewongeneticvariantsandmaternalsmokingin theetiologyoforalcleftsandotherbirthdefects.BirthDefects ResC:EmbryoToday.2008;84:16---29.
22.Van Rooij IA, Wegerif MJ,Roelofs HM, Peters WH, Kuijpers-Jagtman AM, Zielluis GA, et al. Smoking, genetics poly-morphisms in biotransformation enzymes, and nonsyndromic oral clefting: a gene-environment interaction.Epidemiology. 2001;12:502---7.
23.ZhuH,KartikoS,FinnellRH.Importanceofgene-environment interactions in the etiology of selected birth defects. Clin Genet.2009;75:409---20.
24.FreitasJA,DalbenGdaS,SantamariaMJr,FreitasPZ.Current dataonthecharacterizationoforalcleftsinBrazil.BrazOral Res.2004;18:128---33.
25.MartelliDR,BonanPR,SoaresMC,ParanaíbaLR,Martelli-Júnior H.Analysisoffamilialincidenceofnon-syndromiccleftlipand palateinaBrazilianpopulation.MedOralPatolOralCirBucal. 2010;15:898---901.
26.Niswander JD, MacLean CJ, Chung CS, Dronamraju K. Sex ratio and cleft lip with or without cleft palate. Lancet. 1972;2:858---60.