Relationship between cognition
and frailty in elderly
A systematic review
Allan Gustavo Brigola1, Estefani Serafim Rossetti1, Bruna Rodrigues dos Santos2, Anita Liberalesso Neri3, Marisa Silvana Zazzetta4, Keika Inouye4, Sofia Cristina Iost Pavarini4
ABSTRACT. Objective: The aim of this study was to analyze the relationship between cognition and frailty in the elderly. Methods: A systematic review on the currently existing literature concerning the subject was carried out. The search strategy included LILACS, SCOPUS, SciELO, PsycINFO, PubMed and Web of Science databases. Results: A total of 19 studies were selected for review, from which 10 (52.6%) were cross-sectional and 9 (47.4%) longitudinal, and the majority Brazilian. All of the studies established a link between cognition and frailty. There was a relationship between components of frailty and the cognitive domains. Risk of Mild Cognitive Impairment (MCI), dementia and mortality were all evidenced in the relationship between frailty and cognitive impairment. Conclusion: The theory remains limited, but results show the variables that appear to be linked to cognition and frailty in elderly. This data can help in implementing actions to improve the quality of life among elderly.
Key words: cognition, frail elderly, elderly health, dementia.
RELAÇÃO ENTRE COGNIÇÃO E FRAGILIDADE EM IDOSOS: UMA REVISÃO SISTEMÁTICA
RESUMO. Objetivo: Este estudo objetivou analisar a relação entre cognição e fragilidade em pessoas idosas. Métodos: Realizou-se uma revisão sistemática da literatura sobre o assunto. A estratégia de busca incluiu as bases LILACS, SCOPUS, SciELO, PsycINFO, PubMed e Web of Science. Resultados: Foram selecionados 19 estudos para revisão. Dos estudos, 10 (52,6%) eram transversais e 9 (47,4%) longitudinais, sendo a maioria brasileiros. Todos os estudos estabeleceram relação entre cognição e fragilidade. Componentes da fragilidade e os domínios cognitivos apresentaram-se relacionados. Risco de Comprometimento Cognitivo Leve (CCL), demência e mortalidade foi evidenciado a partir da relação entre fragilidade e alterações cognitivas. Conclusão: A literatura continua limitada, mas os resultados mostram as variáveis que parecem estar relacionadas à cognição e fragilidade em pessoas idosas. Esses dados poderão auxiliar na implantação de ações para melhorar a qualidade de vida desses idosos.
Palavras-chave: cognição, idoso fragilizado, saúde do idoso, demência.
INTRODUCTION
F
railty in the elderly can be deined as a multifactorial syndrome that occurs due to a decrease in metabolic activities and re-serves, diiculty in maintaining homeostasis, and vulnerability to stressors, leading to in-creased risk for disabilities.1Advanced age is not a synonym of frailty and this is not present in all elderly, however,
it can be airmed that with the aging global population, a sharp increase in the prevalence of frailty can be expected.2
he risk factors and outcomes of frailty in-clude falls, hospitalizations and mortality in frail elderly, which may occur in the presence of comorbidities1,3,4 or the absence of chronic diseases.5 he prevalence of frailty in elderly ranges from 5% to 58%.3
This study was conducted at the Programa de Pós Graduação em Enfermagem da Universidade Federal de São Carlos, Cidade de São Carlos, São Paulo, Brasil.
Programa de Pós Graduação em Enfermagem da Universidade Federal de São Carlos, Cidade de São Carlos, São Paulo SP, Brasil: 1 Bacharel, Mestrando do
Pro-grama de Pós Graduação em Enfermagem da Universidade Federal de São Carlos; 2Graduando em Gerontologia da Universidade Federal de São Carlos; 3 Professor
Doutor, Docente do Programa de Pós Graduação em Gerontologia da Faculdade de Ciências Médicas da Universidade Estadual de Campinas; 4 Professor Doutor, Docente do Departamento de Gerontologia da Universidade Federal de São Carlos.
Allan Gustavo Brigola. Rua Urias Cardoso de Toledo, 133 – 13563-528 São Carlos SP – Brasil. E-mail: [email protected]
Disclosure: The authors report no conflicts of interest.
Received November 17, 2014. Accepted in final form February 27, 2015.
Recently, the main research group6 that studies the theme published a deinition of physical frailty in elder-ly: “a medical syndrome with multiple causes and con-tributors that is characterized by diminished strength, endurance, and reduced physiologic function that creases an individual’s vulnerability for developing in-creased dependency and/or death”.
To evaluate frailty, the model most widely used is frailty as a phenotype measurable by ive biological cri-teria: unintentional weight loss of more than 4.5 kilo-grams or 5% of body weight in the past year; fatigue, or exhaustion while doing regular activities; low hand-grip strength, which can indicate muscular weakness; decreased gait velocity, also reported as slowness when walking 4.6 meters on a lat surface; and low physical activity in comparison with one year ago, indicating low rate of energy expenditure.1
he inclusion of cognitive evaluation in frailty diag-nosis has been discussed in some investigations, and in this sense there are studies that have included cognitive performance as a component to evaluate frailty.3,7,8
Cross-sectional studies demonstrate the link be-tween frailty and cognitive performance1 and longitu-dinal studies show the relationship between frailty and the emergence of cognitive changes, cognitive impair-ment and deimpair-mentia.9,10
he review conducted by Robertson, Savva and Kenny (2013), showing the relationship between frailty and decline in cognitive function, sought to establish the causal mechanisms and also found a relationship between worsening of cognitive domains and frailty. Perception peed, episodic memory, semantic memory and working memory have been associated with frail-ty. Commands, immediate memory, attention, verbal luency and the clock drawing test are associated with worse performance in frail older adults. In the review, there were studies pointing to the existence and nonex-istence of a relationship between memory and frailty.11
Drawing on this recent review of the data,11 the aim of the present study was to analyze the relationship be-tween cognition and frailty in the elderly, focusing on studies conducted in low-middle income countries.
METHODS
he present study comprised a systematic literature re-view, conducted based on previously established steps of search strategies, identiication, screening, selection and eligibility of studies. Some criteria published on methods for the preparation of systematic reviews were adopted.12
he search for scientiic articles took place between
January and August 2014, using the LILACS, SCOPUS, SciELO, PsycINFO, PubMed and Web of Science data-bases. he descriptors for the search were obtained from MeSH and DeCS. he following operations on the da-tabases were performed: (cognition AND frail elderly). Additional strategies with controlled and uncontrolled operators were employed: (cognition AND frailty AND elderly), (cognition AND frailty syndrome AND elderly), (cognition AND health vulnerability AND elderly).
he following inclusion criteria were used for ar-ticle selection: publications in peer-reviewed journals published between January 2010 and August 2014, in English, Spanish or Portuguese. Reviews and meta-anal-ysis articles were not included in the process of study selection. he search and inclusion of studies were per-formed independently and blindly by two evaluators (AGB and ESR), who evaluated the database compiled titles, abstracts or both, resolving discrepancies in con-sensus meetings.
he studies that met the following criteria were considered eligible: (1) cross-sectional and longitudinal studies with elderly; (2) studies that investigated the association between cognition and/or cognitive impair-ment (CI) - studies about deimpair-mentia and Mild Cognitive Impairment (MCI) were included - with frailty and/or frailty criteria; and (3) studies that evaluated cognition and frailty through validated methods in the literature.
Identiication on databases was carried out using the search strategies outlined previously. Studies dupli-cated across databases were excluded. he studies to be included in the eligibility stage were selected by reading titles, abstracts or both. he eligibility criteria were then applied by critically reading the studies in full. hose studies that did not meet the criteria or did not address the research question were excluded.
RESULTS
A summary of the methods used and the indings is giv-en in Figure 1. Of the number of articles initially idgiv-enti- identi-ied in the database (n = 509), a total of 19 studies were selected for this review.
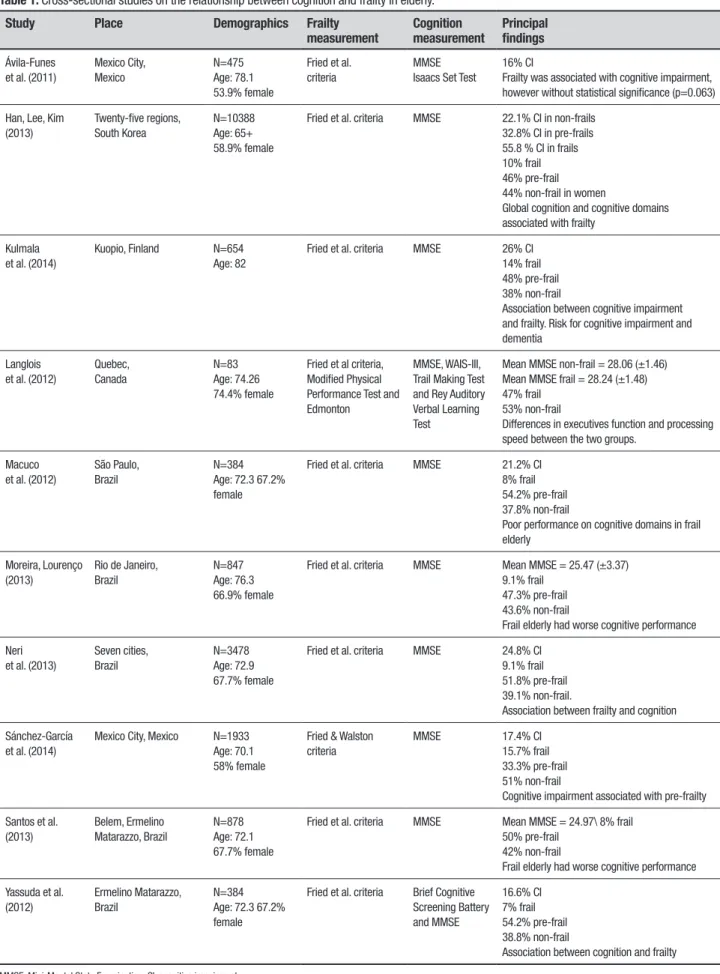
Table 1. Cross-sectional studies on the relationship between cognition and frailty in elderly.
Study Place Demographics Frailty
measurement Cognition measurement Principal findings
Ávila-Funes et al. (2011)
Mexico City, Mexico
N=475 Age: 78.1 53.9% female
Fried et al. criteria
MMSE Isaacs Set Test
16% CI
Frailty was associated with cognitive impairment, however without statistical significance (p=0.063) Han, Lee, Kim
(2013)
Twenty-five regions, South Korea
N=10388 Age: 65+ 58.9% female
Fried et al. criteria MMSE 22.1% CI in non-frails 32.8% CI in pre-frails 55.8 % CI in frails 10% frail 46% pre-frail 44% non-frail in women
Global cognition and cognitive domains associated with frailty
Kulmala et al. (2014)
Kuopio, Finland N=654 Age: 82
Fried et al. criteria MMSE 26% CI 14% frail 48% pre-frail 38% non-frail
Association between cognitive impairment and frailty. Risk for cognitive impairment and dementia
Langlois et al. (2012)
Quebec, Canada
N=83 Age: 74.26 74.4% female
Fried et al criteria, Modified Physical Performance Test and Edmonton
MMSE, WAIS-III, Trail Making Test and Rey Auditory Verbal Learning Test
Mean MMSE non-frail = 28.06 (±1.46) Mean MMSE frail = 28.24 (±1.48) 47% frail
53% non-frail
Differences in executives function and processing speed between the two groups.
Macuco et al. (2012)
São Paulo, Brazil
N=384 Age: 72.3 67.2% female
Fried et al. criteria MMSE 21.2% CI 8% frail 54.2% pre-frail 37.8% non-frail
Poor performance on cognitive domains in frail elderly
Moreira, Lourenço (2013)
Rio de Janeiro, Brazil
N=847 Age: 76.3 66.9% female
Fried et al. criteria MMSE Mean MMSE = 25.47 (±3.37) 9.1% frail
47.3% pre-frail 43.6% non-frail
Frail elderly had worse cognitive performance Neri
et al. (2013)
Seven cities, Brazil
N=3478 Age: 72.9 67.7% female
Fried et al. criteria MMSE 24.8% CI 9.1% frail 51.8% pre-frail 39.1% non-frail.
Association between frailty and cognition Sánchez-García
et al. (2014)
Mexico City, Mexico N=1933 Age: 70.1 58% female
Fried & Walston criteria
MMSE 17.4% CI 15.7% frail 33.3% pre-frail 51% non-frail
Cognitive impairment associated with pre-frailty Santos et al.
(2013)
Belem, Ermelino Matarazzo, Brazil
N=878 Age: 72.1 67.7% female
Fried et al. criteria MMSE Mean MMSE = 24.97\ 8% frail 50% pre-frail
42% non-frail
Frail elderly had worse cognitive performance Yassuda et al.
(2012)
Ermelino Matarazzo, Brazil
N=384 Age: 72.3 67.2% female
Fried et al. criteria Brief Cognitive Screening Battery and MMSE
16.6% CI 7% frail 54.2% pre-frail 38.8% non-frail
Association between cognition and frailty
studies while Table 2 shows the information for longi-tudinal studies.
Of the cross-sectional studies, 90% categorized the elderly according to frailty levels, whereas 8 (80%) used the frailty evaluation proposed by Fried et al. (2001),1 and all included the Mini-Mental State Examination
(MMSE) of Folstein, Folstein and McHugh (1975)13 in their cognitive evaluation. Except for the Ávila-Funes et al. (2011)14 study, the association between cognitive al-terations and frailty was statistically proven.
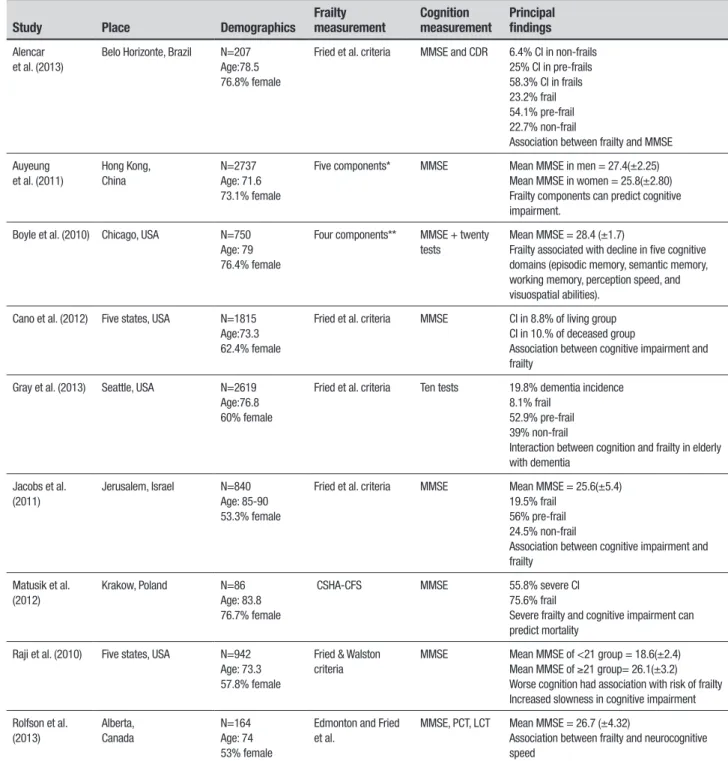
Of the longitudinal studies, 44.4% categorized the elderly according to frailty levels, 4 used the frailty
eval-Table 2. Longitudinal studies on the relationship between cognition and frailty in elderly.
Study Place Demographics Frailty measurement Cognition measurement Principalfindings
Alencar et al. (2013)
Belo Horizonte, Brazil N=207 Age:78.5 76.8% female
Fried et al. criteria MMSE and CDR 6.4% CI in non-frails 25% CI in pre-frails 58.3% CI in frails 23.2% frail 54.1% pre-frail 22.7% non-frail
Association between frailty and MMSE Auyeung
et al. (2011)
Hong Kong, China
N=2737 Age: 71.6 73.1% female
Five components* MMSE Mean MMSE in men = 27.4(±2.25) Mean MMSE in women = 25.8(±2.80) Frailty components can predict cognitive impairment.
Boyle et al. (2010) Chicago, USA N=750 Age: 79 76.4% female
Four components** MMSE + twenty tests
Mean MMSE = 28.4 (±1.7)
Frailty associated with decline in five cognitive domains (episodic memory, semantic memory, working memory, perception speed, and visuospatial abilities).
Cano et al. (2012) Five states, USA N=1815 Age:73.3 62.4% female
Fried et al. criteria MMSE CI in 8.8% of living group CI in 10.% of deceased group
Association between cognitive impairment and frailty
Gray et al. (2013) Seattle, USA N=2619 Age:76.8 60% female
Fried et al. criteria Ten tests 19.8% dementia incidence 8.1% frail
52.9% pre-frail 39% non-frail
Interaction between cognition and frailty in elderly with dementia
Jacobs et al. (2011)
Jerusalem, Israel N=840 Age: 85-90 53.3% female
Fried et al. criteria MMSE Mean MMSE = 25.6(±5.4) 19.5% frail
56% pre-frail 24.5% non-frail
Association between cognitive impairment and frailty
Matusik et al. (2012)
Krakow, Poland N=86 Age: 83.8 76.7% female
CSHA-CFS MMSE 55.8% severe CI 75.6% frail
Severe frailty and cognitive impairment can predict mortality
Raji et al. (2010) Five states, USA N=942 Age: 73.3 57.8% female
Fried & Walston criteria
MMSE Mean MMSE of <21 group = 18.6(±2.4) Mean MMSE of ≥21 group= 26.1(±3.2) Worse cognition had association with risk of frailty Increased slowness in cognitive impairment Rolfson et al.
(2013)
Alberta, Canada
N=164 Age: 74 53% female
Edmonton and Fried et al.
MMSE, PCT, LCT Mean MMSE = 26.7 (±4.32)
Association between frailty and neurocognitive speed
ment. Frailty was associated with cognitive impairment, however without statistical signiicance (p=0.063). he results showed that before the frailty components are adjusted, except for weight loss, all were associated with activities of daily living. It was concluded that cognitive impairment and low physical activity are the main con-tributing factors to frailty.14
Also in Mexico, 1933 seniors evaluated by Sánches-Garcia et al. (2014) had a prevalence of 15.7% frailty, 33.3% pre-frailty and 51% non-frailty. he majority (58%) of the elderly were women, with a mean age of 70.1 years. A total of 17.4% had cognitive impairment and 22.7% showed depression symptoms. Cognitive impairment was associated with both frailty and pre-frailty in the elderly assessed.15
Brazilian studies have shown similar results con-cerning sociodemographic characteristics, frailty preva-lence and cognitive impairment. Moreira and Lourenço (2013) conducted a study in Rio de Janeiro city with a random sample of 847 seniors. Participants were predominantly women (66.9%), with a mean age of 76.6 years, 62.6% Caucasian and 44.1% married. he prevalence of frailty was 9.1%, while 47.3% of partici-pants were pre-frail and 43.6% non-frail. Mean MMSE score was 25.47 (±3.37). Multivariate logistic regres-sion showed a strong association between cognition and frailty. he frail elderly, predominantly widowed women, had worse cognitive performance.16 Another Brazilian study with 3478 community elders showed very similar results. In the multicentric study by Neri et al. (2013), the majority were women (67.7%), mar-ried (48%) or widowed (36.4%), living with their child’s family (52.6%), householders (64.5%) with 1 to 4 years of formal education (49%), 28.8% illiteracy and 24.8% cognitive impairment. Of the sample, 9.1% were frail, 51.8% pre-frail, 39.1% non-frail, and 25.4% had cogni-tive impairment. Among the frail elderly, there was a higher proportion of women and individuals who were aged 80 years or older, widowed, illiterate and with cog-nitive impairment.17
he study published by Santos et al. (2013) evalu-ated 878 elderly without cognitive impairment. he age range was 65-92 years, the majority 594 (67.7%) fe-male, of mixed race — “mulattoes, caboclos” and brown — (50.9%), married (44.5%), or widowed (35.1%). Re-garding frailty, 42% were non-frail, 50% pre-frail and 8% frail, with an average MSSE score of 24.97 points. he MMSE results showed statistically signiicant dif-ferences between frail, pre-frail and non-frail elders, and the regression analysis for the MMSE showed that frail elderly difered from non-frail whereas the same
Figure 1. Summary of selection of articles for review.
Duplicate articles removed (n=186)
Articles excluded through reading
titles / abstract (n=296)
Articles excluded (n=08), for failing to meet the objectives of the review Articles identified
(n=509)
Articles selected (n=323)
Articles selected for eligibility
(n=27)
Articles selected for review
(n=19)
uation proposed by Fried et al. (2001)1 and 8 studies in-cluded the MMSE in their cognition evaluation. Of the 9 longitudinal studies, 8 were conducted outside Latin America.
Out of all the studies reviewed, 10 (52.6%) reported speciic results of an association between frailty com-ponents and cognitive domains. Among these studies, 50% found slowness, 40% muscular weakness, 20% exhaustion and 10% linked weight loss, low chair stand speed and step length with cognitive impairments. Re-garding cognitive domains, memory subtypes (episodic, semantic, working, storage, encoding and immediate) were most strongly associated with frailty (30%), fol-lowed by processing/perception speed (20%), temporal orientation (20%) and visuospatial skills (20%). he ex-ecutive functions, verbal luency, attention, commands, language and judgment were associated in 10% of these studies.
One study reviewed found an association between frailty and the diagnosis of MCI, two highlighted risk of dementia in frail elderly, with the greatest risk being for non-Alzheimer’s Disease (AD) dementia, and three found increased prevalence of mortality in frail elderly with cognitive impairment.
impair-disparity did not occur between pre-frail and non-frail groups.18
Cognitive domains and speciic frailty criteria were present in the following studies. In Canada, Langlois et al. (2012) compared frail and non-frail elderly for physi-cal, cognitive and psychological dimensions. A total of 39 frail and 44 non-frail seniors were compared on vari-ous physical activity, cognition and quality-of-life mea-sures. he mean MMSE score in non-frails was 28.06 (±1.46) and frails was 28.24 (±1.48). he study showed diferences between the groups regarding executive functions and processing speed, with frail individu-als having the worst performance. Furthermore, frail elderly reported lower self-perceived physical ability, cognition, afectivity, housekeeping eicacy and physi-cal health.19 Han, Lee, Kim (2013) found, in a study of 10338 elderly from South Korean communities, that all cognitive domains were inversely correlated with the risk of frailty. he results also showed that 58.9% of the sample consisted of women, 9.3% were frail, 42.3% pre-frail and 48.4% non-frail. he frailty prevalence was higher among women (10%) compared to men (8.3%), where 37.1% of men and 46% of women were pre-frail and 54.7% of men and 43.9% of women non-frail. he prevalence of CI was 22.1% in non-frails, 32.8% in pre-frails and 55.8 % in pre-frails. Cognitive impairments were associated with high levels of frailty and risk of frailty. High scores for temporal, register, attention and judg-ment orientations were associated with a lower risk of frailty in both sexes, while in women, memory, language and visuospatial ability were also associated with low probability of frailty.20
In a poor Brazilian community, Yassuda et al. (2012) analyzed 384 older adults using frailty measures and cognition as evaluated by the Brief Cognitive Assess-ment Tool (memorization of 10 black and white pic-tures, animal, verbal luency category and the Clock Drawing Test) and by the MMSE. he prevalence of MMSE impairment was 16.6% for the overall sample, 11.6% for non-frails, 16.8% for pre-frails and 42.8% for frails. he frail elderly had the worst cognitive per-formance when compared to pre and non-frail elderly. Muscular strength was associated with MMSE perfor-mance, while the slowness frailty criteria was associated with verbal luency and the Clock Drawing Test.21 Macu-co et al. (2012), based on the same sample, found a prev-alence of frailty of 8%. Of the participants, 54.2% were classiied as pre-frail and 37.8% as non-frail. Regarding cognition, 21.2% had cognitive impairment, whereas 15.6% of non-frail, 22.3% of pre-frail and 38.7% of the frail scored below the cut-of on the MMSE. he frailest
individuals had the worst performance on the MMSE. Being considered frail was associated with worse perfor-mance in temporal orientation, immediate memory and command diiculty.22
A Finnish study proposed that a risk of more severe cognitive impairment, resulting in dementia diagnosis was associated with frailty level. Kulmala et al. (2014) in a study of 654 older adults found a 14% frailty preva-lence. Of the elderly assessed, 171 (26%) had cognitive deicits and 134 (21%) were diagnosed with dementia. he cognitive impairment prevalence in frail elderly was 64%. Frailty was associated with cognitive impairment. he regression analysis showed that frail elderly were eight times more likely to develop cognitive impair-ment, six time more likely to develop vascular dementia and four times more likely to develop dementia due to AD.23
Longitudinal studies. he longitudinal studies, beyond the cognition and frailty relationship, revealed that compo-nents of frailty were associated with poorer performance in cognitive domains, as well as showing frailty risk for cognitive impairment, onset of dementia and the risk of mortality during the follow-up of participants.
he Canadian study of Rolfson et al. (2013) evalu-ated the interaction between neurocognitive speed and operationalized frailty in two diferent ways. A sample of 164 participants without dementia were followed an-nually for three years. Besides the evaluation by MMSE, neurocognitive speed was deined by other tests. Frailty was assessed using the Edmonton Frail Scale and the cri-teria of Fried et al. (2001).1 Regression analysis showed that both evaluations of frailty were associated with low neurocognitive velocity, however, only the evaluation criteria by Fried et al. (2001)1 was associated with the cognitive assessment by MMSE. Another important re-sult was that, while monitoring the sample, neurocogni-tive speed decreased with increased frailty when evalu-ated by the criteria of phenotype frailty.24
appendicular muscle mass and walking speed were proven insigniicant. In women, all frailty measures, except for appendicular muscle mass and weight loss, were signiicantly associated with MMSE. Further-more, weaker grip strength remained signiicant after adjusting for age, years of formal education and MMSE performance.25
A follow-up study conducted in Brazil was also in-cluded. Alencar et al. (2013) evaluated the association between frailty and cognitive impairment and the inci-dence of cognitive impairment in a sample of 207 elderly, with or without cognitive impairment, followed for 12 months. Cognition was evaluated by the MMSE and the Clinical Dementia Rating (CDR) scale. In the irst evalu-ation, 76.8% were women, mean age was 78.5 years, and 47 (22.7%) participants were classiied as non-frail, 112 (54.1%) pre-frail and 48 (23.2%) were classiied as frail. Around 6.4% of non-frail, 25% of pre-frail and 58.3% of frail had cognitive impairment. Of the initial 207 par-ticipants, 187 were reevaluated (12% lost to follow-up). Frailty was associated with subsequent decline in cog-nitive function and cogcog-nitive impairment on the CDR. In the study, there was no relationship between frailty and the incidence of cognitive decline, however the pro-portion of new cases of cognitive impairment was 4.9% among non-frail, 8.9% in pre-frail and 13.3% in frail.26
Raji et al. (2010), in a study with a 10-year follow-up, examined whether poor cognition could predict frailty risk in non-frail elderly from ive American states (Texas, New Mexico, California, Colorado and Arizona). A total of 942 non-frail elderly were interviewed, 57.8% of whom were women, with a mean age of 73.3 years. A modiied version of the Fried and Walston evalua-tion of frailty was used. he version encompassed four items, including involuntary weight loss, exhaustion, fatigue and weakness. he sample was divided into two groups (MMSE<21 and MMSE≥21). In general, estima-tion equaestima-tion models testing the relaestima-tionship between MMSE and risk of becoming frail over a period of 10 years showed signiicance. his association persisted regardless of age, sex, marital status, education, time and medical conditions, indicating that non-frail elderly with low cognition had a 9% higher chance per year of becoming frail, in comparison to the individuals with good cognition. An important inding was that from the irst follow-up to the second, 30.9% of the elderly with cognitive changes and 26.3% of the elderly without cog-nitive impairment fulilled the criteria for weight loss. From the second follow-up to the last, slowness had increased 25% in the cognitive changes group versus 18.1% in the non-impaired group.27
Frailty was shown as a risk factor for Mild Cognitive Impairment (MCI) by Boyle et al. (2010), that followed 750 elderly without baseline cognitive impairment for 12 years. Frailty was evaluated according to four cri-teria: grip strength, walking speed, body composition and fatigue. he greater the impairment on these cri-teria, the frailer the elder. Cognition was more widely evaluated by the MMSE and other tests. Regarding the sample, mean age was 79 years, formal education 14.5 years and 76.4% were women. he men were less frail than the women and frailty was inversely associated with global cognitive performance. During the follow-up, 40% of participants developed MCI, and the pres-ence of each physical frailty component was associated with a faster rate of global cognitive decline and with the ive evaluated domains (episodic memory, semantic memory, working memory, perception speed and visuo-spatial abilities). Furthermore, results also showed that lower grip strength and walking speed were associated with the risk of irst occurrence of MCI.28
Risk for low occurrence of dementia inluenced by frailty was shown in Mexico by Gray et al. (2013). he study sample comprised 2619 participants aged ≥ 65 years, without dementia at study baseline. Frailty was measured according to criteria by Fried et al. (2001),1 and cognition was assessed based on ten neuropsycho-logical tests. Of the sample, 8.1% were frail and 39% non-frail. For other causes of dementia, interaction was found between cognitive score and frailty. Over a mean follow-up of 6.5 years, 521 (19.8%) participants developed dementia (of which 448 developed AD). In the age, gender, education and race-adjusted model, the risk of frailty rate was 1.78. In the fully adjusted mod-els, frailty risk rate was 1.20 for all-cause dementia, 1.08 for AD and 2.57 for non-AD. Frailty was associated with higher risk of developing non-Alzheimer’s dementia. Slow walking speed was associated with the risk of non-Alzheimer’s dementia. However, the regression analysis showed that muscular weakness and exhaustion repre-sented signiicant dementia risks.29
as-Figure 2. Model of association between factors, frailty, cognitive impair-ment and their outcomes in older adults.
sociated with cognitive impairment and was predictive of subsequent mortality.30
Matusik et al. (2012) followed 66 women and 20 men residing at nursing homes in Poland. Frailty preva-lence was 75.6%, where 34.9% had severe frailty, 23% moderate frailty and 17.4% mild frailty. Severe cogni-tive impairment was present in 55.8% of the elderly. he residents with severe frailty and severe cognitive im-pairment accounted for 33.7% of the sample and 50% of the deceased within 12 months. he follow-up showed that the one-year mortality was higher in those with se-vere frailty and sese-vere cognitive impairment compared with other residents. he authors concluded that frailty, dementia and cognitive impairment were predictors of higher mortality rate in institutionalized seniors.31
Finally, in North America, Cano et al. (2012) ex-amined the association between frailty and cognitive changes as mortality predictors within a 10-year period in a sample of 1815 Mexican-American elderly. By the end of the follow-up, 690 cases of death of participants in the initial sample were conirmed. Among the surviv-ing seniors (n=917), the mean age was 73.3 years and 62.4% were women. Out of the sample, 8.3% of the liv-ing group and 10.2% of the deceased group had cogni-tive impairment. MMSE scores decreased over time and the percentage of frail individuals increased linearly. Frailty and cognitive changes were associated. However, frailty and cognitive impairment were independent risk factors after controlling for the others variables. he results showed that frailty was a higher risk factor for mortality than cognitive impairment, where mortality rate was higher in frail elderly than on pre-frail or non-frail groups. Individuals who were male, older, married, with hip injuries and frail elderly were signiicantly more likely to be in the deceased group during the follow-up.32
Some peculiarities are evident, especially in cross-sectional studies. he prevalence of frailty in Latin American studies of the elderly was around 10% and cognitive impairment ranged from 16% to 25% in the samples. Mean scores on the MMSE were around 25 points while in other countries the average points on the test is greater. In these other countries, the preva-lence of cognitive impairment was from 20% to 55%. he prevalence of frailty was similar across all studies.
Lastly, several factors may contribute to higher frailty levels and consequently worse cognitive perfor-mance. Among them are advanced age, low education, low inancial income, female gender, widowed/unmar-ried, low body weight and poor nutritional status, de-pendence in functional and daily living activities, symp-toms of depression, presence of comorbidities, worse
perceived health, use of medications and drugs and the use of health services.14-32
DISCUSSION
According to the results of the reviewed studies, a mod-el, illustrated in Figure 2, was produced in order to bet-ter understand the frailty-associated factors. Frailty is a condition or outcome inluenced by several factors elu-cidated by the reviewed studies. In the scope of frailty, muscular strength and walking speed are impaired, as is cognitive performance, with memory being the most impaired. Among the major outcomes of this are MCI, dementia and the greater risk of mortality in the elderly. Figure 2 illustrates the increased risk for cognitive im-pairment showing that its severity may be inluenced by higher levels of frailty in the elderly.
where some of the associated factors identiied in this review are present in the cycle, such as depression, de-pendency, comorbidities (diseases) socioeconomic dis-advantages (low social engagement) and low nutritional status (chronic undernutrition).11
Also, the same review highlighted the need for stud-ies determining which measures of frailty could be used to best identify the risk of cognitive decline in aging.11 he systematic review of Sternberg et al. (2011) empha-sized the importance of inclusion of disability, cognition and mood in frailty elements.33 An overview of Bouillon et al. (2013) reported that the reliability and validity of frailty measures are rarely examined, but the Fried et al. criteria is the most frequently used,34 a situation also observed in this review. Furthermore, a Korean study reported that the Fried et al. criteria is better than other types of evaluation, but a new frailty index called KFI (KLoSHA Frailty Index) was an excellent frailty mea-sure, correlated with hospitalization and able to predict subsequent functional decline.35 However, a good mea-sure that evaluates frailty and its risk for cognitive im-pairment in elderly is required.
Based on this systematic review of the literature, drawing on studies from a large number of databases, it can be concluded that cognition is associated with frailty, especially when operationalized as a physical syndrome marked by vulnerability to stressors in the elderly.
Frailty components, particularly slowness and mus-cular weakness, are associated with cognitive function-ing where memory seems to be the most afected cogni-tive function. Cognicogni-tive impairment is more prevalent in frail elderly, and the greater the frailty, the higher the risk for MCI and dementia. he concomitant presence of frailty and cognitive changes can strongly predict mortality in the elderly.
his review explored a substantial number of stud-ies from Brazil and Latin America, mostly cross-sec-tional investigations. Strengths of the study include
the sample characteristics of low educational level and poor inancial support and the relationship of these fac-tors with cognitive function and frailty in this group. In theory, the elderly in the poorest communities are more vulnerable than elderly from wealthier communities, but longitudinal studies should be conducted in devel-oping countries.
he scarcity of studies reviewing the subject repsents a study limitation regarding the discussion of re-sults. It is hoped that the present results prompt further research on the relationship between physical and men-tal health and the aging process, and that this serves as input for the creation, evaluation and discussion of ac-tions involving attention and care in Gerontology.
Author contributions. Allan Gustavo Brigola – Delimitação do tema, delimitação dos métodos, busca de artigos, análise e interpretação dos dados, redação, revisão críti-ca e aprovação inal. Estefani Seraim Rossetti – Delimi-tação do tema, delimiDelimi-tação dos métodos, busca de arti-gos, análise e interpretação dos dados, redação, revisão crítica e aprovação inal. Bruna Rodrigues dos Santos – Delimitação do tema, delimitação dos métodos, reda-ção, revisão crítica e aprovação inal. Anita Liberalesso Neri – Delimitação do tema, delimitação dos métodos, redação, revisão crítica e aprovação inal. Marisa Silvana Zazzetta – Delimitação do tema, delimitação dos méto-dos, redação, revisão crítica e aprovação inal. Keika In-ouye – Delimitação do tema, delimitação dos métodos, redação, revisão crítica e aprovação inal. Soia Cristina Iost Pavarini – Delimitação do tema, delimitação dos métodos, redação, revisão crítica e aprovação inal.
Support. Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP).
Acknowledgements. À Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP).
REFERENCES
1. Fried LP, Tangen CM, Walston J, et al. Frailty in older adults: evidence for a phenotype. J Gerontol 2001;56:146-156.
2. Ahmed N, Mandel R, Fain MJ. Frailty: an emerging geriatric syndrome. Am J Med 2007;120:748-753.
3. Sternberg SA, Schwartz AW, Karunananthan S, Bergman H, Clarfield AM. The identification of frailty: a systematic literature review. J Am Geriatr Soc 2011;59:2129-2138.
4. Solfrizzi V, Scafato M, Frisardi V, et al. Frailty syndrome and all-cause mortality in demented patients: the Italian longitudinal study on aging. Age 2012;34:507-5017.
5. Rockwood K, Mitnitski A, Frailty in relation to the accumulation of defi-cits. J Gerontol 2007;62:722-727.
6. Morley JE, Vellas B, van Kan GA, et al. Frailty consensus: a call to action. J Am Med Dir Assoc 2013;14:392-397.
7. Rockwood, K, Howlett SE, MacKnight C, et al. Prevalence, attributes,
and outcomes of fitness and frailty in community-dwelling older adults: report from the Canadian Study of Health and Aging. J Gerontol 2004; 59:1310-1317.
8. Rockwood K, Song X, MacKnight C, et al. A global clinical measure of fitness and frailty in elderly people. Canad Med Assoc J 2005;173: 489-495.
9. Buchman AS, Scheider JA, Leugans S, Bennett DA. Physical frailty in older persons is associated with Alzheimer disease pathology. Neurology 2008:71;499-504.
10. Ávila-Funes JA, Amieva H, Barberger-Gateau, P, et al. Cognitive impair-ment improves the predictive validity of the phenotype of frailty for adverse health outcomes. J Am Geriatr Soc 2009;57:453-461. 11. Robertson A, Savva GM, Kenny RA. Frailty and cognitive impairment:
12. Moher D, Liberati A, Tetzlaff J, Altman DG, The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA Statement. J Clin Epidemiol 2009;62:1006-1012. 13. Folstein MF, Folstein SE, McHugh PR. Mini-Mental State: a practical
method for grading the cognitive state of patients for the clinician. J Psychiatr Res 1975;12:189-198.
14. Ávila-Funes JA, Pina-Escudero SD, Aguilar-Navarro S, Gutierrez-Robledo LM, Ruiz-Arregui L, Amieva H. Cognitive impairment and low physical activity are the components of frailty more strongly associated with disability. J Nutr Health Aging 2011;15:683-689.
15. Sánches-García S, Sánches-Arenaz R, García-Peña C, et al. Frailty among community-dwelling elderly Mexican people: prevalence and association with sociodemographic characteristics, health state and the use of health services. Geriatr Gerontol Int 2014;14:395-402. 16. Moreira VG, Lourenço RA. Prevalence and factors associated with
frailty in an older population from the city of Rio de Janeiro, Brazil: the FIBRA-RJ Study. Clinics 2013;68: 979-985.
17. Neri AL, Yassuda MS, Araújo LF, et al. Metodologia e perfil sociodemo-gráfico, cognitivo e de fragilidade de idosos comunitários de sete cidades brasileiras: Estudo FIBRA. Cad Saúde Pública 2013;29:778-792. 18. Santos AA, Mansano-Schlosser TCS, Ceolim MF, Pavarini SCI. Sono,
fragilidade e cognição: estudo multicêntrico com idosos brasileiros. Rev Bras Enf 2013;66:351-357.
19. Langlois F, Vu TTM, Kergoat MJ, Chassé K, Dupuis G, Bherer L. The multiple dimensions of frailty: physical capacity, cognition and quality of life. Int Psychogeriatr 2012;24:1429-1436.
20. Han ES, Lee Y, Kim J. Association of cognitive impairment with frailty in community dwelling older adults. Int Psychogeriatr 2013;26:155-163. 21. Yassuda MS; Lopes A, Cachioni M, et al. Frailty criteria and cognitive
performance are related: data from the FIBRA study in Ermelino Mata-razzo, Sao Paulo, Brazil. J Nutr Health Aging 2012;16:55-61. 22. Macuco CRM, Batistoni SST, Lopes A, et al. Mini-Mental State
Exami-nation performance in frail, pre-frail, and non-frail community dwelling older adults in Ermelino Matarazzo, São Paulo, Brazil. Int Psychogeriatr 2012;24:1725-1731.
23. Kulmala J, Nykänen I, Mänty M, Hatikainen S. Association between frailty and dementia: a population-based study. Gerontology 2014;60: 16-21.
24. Rolfson DB, Wilcock G, Mitnitki A, et al. An assessment of neurocogni-tive speed in relation to frailty. Age Ageing 2013;42:191-196. 25. Auyeung TW, Lee JSW, Kwork T, Woo J. Physical frailty predicts future
cognitive decline – a four-year prospective study in 2737 cognitively normal older adults. J Nutr Health Aging 2011;15:690-694.
26. Alencar MA, Dias JMD, Figueiredo LC, Dias RC.Frailty and cognitive impairment among community-dwelling elderly. Arq Neuropsiquiatr 2013;71:362-367.
27. Raji MA, Snih SA, Ostir GV, Markides KS, Ottenbacher KJ. Cognitive status and future risk of frailty in older mexican americans. J Gerontol-Series A Biol Sci Med Sci 2010; 65:1228-1234.
28. Boyle PA, Buchman AS, Wilson RS, Leurgans SE, Bannett DA. Physical frailty is associated with incident mild cognitive impairment in commu-nity-based older persons. J Am Geriatr Soc 2010;58:248-255. 29. Gray SL, Anderson AM, Hubbard AR, et al. Frailty and Incident
Dementia. J GerontolSeries A Biol Sci Med Sci 2013;68:1083-1090. 30. Jacobs JM, Cohen A, Ein-Mor E, Maaravi Y, Stessman E. Frailty,
cogni-tive impairment and mortality among the oldest old. J Nutr Health Aging 2011;15:678-682.
31. Matusik P, Tomaszewski K, Chmielowska K, et al. Arch GerontolGeriatr 2012;55:22-24.
32. Cano C, Ternent RS, Snih SA, Markides K, Ottenbacher KJ. Frailty and cognitive impairment as predictors of mortality in older Mexican Ameri-cans. J Nutr Health Aging 2012;16;142-147.
33. Sternberg SA, Schwartz AW, Karunanantha S, Bergman H, Clarfield AM. The identification of frailty: a systematic literature review. J Am Geriatr Soc 2011;59:2129-2138.
34. Bouillo K, Kivimaki K, Hamer M, et al. Measures of frailty in population-based studies: an overview. BMC Geriatrics 2013;13:1-11.