w w w . r b o . o r g . b r
Original
Article
Treatment
of
chronic
plantar
fasciitis
with
extra
corporeal
shock
wave
therapy:
ultrasonographic
morphological
aspect
and
functional
evaluation
夽
Roberto
Androsoni
∗,
Alfonso
Apostólico
Netto,
Rafael
Rocha
Macedo,
Ricardo
Pozzi
Fasolin,
Guilherme
Boni,
Rodrigo
Fileto
Gavaldão
Moreira
HospitalIFOR,SãoBernardodoCampo,SP,Brazil
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received2April2013 Accepted11April2013
Keywords:
Fasciitis,plantar Highenergyshock waves/therapeuticuse Ultrasonography Evaluation Morphology
a
b
s
t
r
a
c
t
Objective:This paperhasthe purposeto analyzeprospectively thetreatment resultsin patientswithchronicplantarfasciitisresistanttoconservativetreatmentwhounderwent extracorporealshockwavetherapy(ESWT).
Methods:Weevaluated30patients(36feet);16(53.3%)patientsweremaleand14(47.7%) femalewithmeanageof48.7y.o.,varyingfrom33to78y.o.;16(53.3%)presenttheproblem ontheleftside,14(46.7%)ontherightonesand6(20%)bilateral;thesymptomatologyvaried from6to60months,withtheaverageof13.58months.Thesepatientsweresubmittedto aweeklyESWTsessionfor4consecutiveweeks.Wemeasuredtheplantarfasciathickness millimeterswithultrasoundandweappliedAmericanOrthopaedicFootandAnkleSociety (AOFAS)scaleforankleandhindfoot,andRoles&MaudsleyscalesinpreESWT,afterone, threeandsixmonthsafteranddecreaseintheplantarfasciathicknessbytheultrasound (p=0.011)alongthedifferentmomentsstudied.
Results:Weobservedimprovementoftheevaluatedcriteria(p<0.001)andplantarfascia thicknessbyultrasound(p=0.011)atdifferenttimepointsstudied.
Conclusion:TheESWTcanbeconsideredanimportanttoolintheprimaryoradjuvant treat-mentofthechronicplantarfasciitiswhenassociatedwithconventionaltherapies.This methodologyissafe, non-invasiveandprovidesprecociousrehabilitationandreturnto regularactivitiesconsideringtheresultsofthestatisticalanalysis.Thisresourceprovides decreaseinthethicknessoftheplantarfascia.
©2013SociedadeBrasileiradeOrtopediaeTraumatologia.PublishedbyElsevierEditora Ltda.Allrightsreserved.
夽
WorkperformedatHospitalIFOR,SãoBernardodoCampo,SP,Brazil.
∗ Correspondingauthor.
E-mail:[email protected](R.Androsoni).
Tratamento
da
fasciíte
plantar
crônica
pela
terapia
de
ondas
de
choque:
avaliac¸ão
morfológica
ultrassonográfica
e
funcional
Palavras-chave:
Fasciíteplantar
Ondasdechoquedealta energia/usoterapêutico Ultrassonografia Avaliac¸ão Morfologia
r
e
s
u
m
o
Objetivo:Estetrabalhotevecomoobjetivoanalisarprospectivamenteosresultadosdo trata-mentocomterapiadeondasdechoque(TOC)empacientesportadoresdefasciíteplantar crônicaresistenteaotratamentoconservador.
Métodos: Obtivemos30pacientes(36pés),16(53,3%)dosexomasculinoe14(47,7%)do feminino,cujaidade,emmédia,foide48,37anos,comvariac¸ãode33a78anos;16(53,3%) apresentavamaafecc¸ãonopéesquerdo,14(46,7%)nodireitoeseis(20%)bilateralmente;a sintomatologiavarioudeseisa60meses,commédiade13,58meses.Ospacientesforam submetidosaumasessãosemanaldeTOCporquatrosemanasconsecutivas.Mensuramos aespessuradafásciaplantaremmilímetrospeloultrassomeusamosaescaladaAmerican OrthopaedicFootandAnkleSociety(AOFAS)paratornozeloeretropéeaescaladeRoles &Maudsleynosmomentospré-TOC,apósoprimeiro,oterceiroeosextomesesapósa aplicac¸ão.
Resultados: Observamosmelhoriadoscritériosavaliados(p<0,001)edaespessuradafáscia plantarpeloultrassom(p=0,011)nosdiferentesmomentosestudados.
Conclusão: ATOCpodeserconsideradaimportanteinstrumentonotratamentoprimário ouadjuvantedafasciíteplantarcrônica,quandoaliadaàsterapiasconvencionais.Essa metodologiaésegura, nãoinvasivaepromove reabilitac¸ãoe retornoprecocesàs ativi-dadeshabituaispelosresultadosdasanálisesestatísticas.Proporcionatambémreduc¸ão daespessuradafásciaplantar.
©2013SociedadeBrasileiradeOrtopediaeTraumatologia.PublicadoporElsevier EditoraLtda.Todososdireitosreservados.
Introduction
Plantarfasciitisischaracterizedasadegenerativecondition oftheproximalplantaraponeurosis.Thesitemostfrequently involved isat the medialtuberosity ofthe calcaneus. The pathological findings from this nosological entity include degenerativetissuechangescharacterizedbyfibroblastic pro-liferationandpresenceofinflammatorytissue.1–3 Itisnow
acceptedthatthisfasciopathyshouldbeclassifiedasatype ofenthesopathy,eventhoughits physiopathologyispoorly understood.
Severaltherapeuticoptionshavebeendescribed,among which conservative treatment istaken to be the preferred method. Satisfactory results have thus been achieved in around90%ofthepatients.
Useofanti-inflammatorymedications,analgesicsandlocal infiltrationofcorticoidsandplatelet-richplasma(PRP)is rec-ommended.Furthermore,useofinsoles,heelsupports,splints andnighttimebraces,alongwithphysiotherapy,isalso recom-mended,withtheaimofaidinginachievingremissionofthe inflammatoryandpainfulcondition.4–6
Morerecently,somestudieshavedemonstratedthat appli-cationofadehydratedhumanamnioticmembrane(dHAM) iseffective.Otherstudieshavedemonstratedsimilarefficacy throughapplicationofhighmolecularweighthyaluronicacid. Changestolifestylehabits,suchasweightreductionanduse ofappropriate footwear, and also posturalchanges during work,7–10arefurtherrecommendations.
The other 10% of the patients, whose condition is not resolvedthroughconservativetreatment,canbeconsidered tobecasesofrecalcitrantfasciopathy.Inthesecases,surgical
treatmentmaybeuseful,inordertoachieveopenor endo-scopic release of the plantarfascia,11 with excision of the
diseasedtissue.Insomespecificcases,simultaneousnerve decompressionisindicated.
Inanattempttoavoidaninvasiveprocedure,therehave been manystudiesonshockwavetherapyinchroniccases. Thistechniquehasbeenshowntobeeffectiveforimproving thesymptomsandqualityoflifeofpatientswiththis condi-tion.Thebasicideaofshockwavetherapyistostimulatethe tissueregenerationprocessinthebonesandtendons.12,13Its
efficacyisnotedespeciallyinthetissuessurroundingthebone andtendons,andalsoatthebone-tendoninterface (enthe-sis).Releaseoffreeradicals,nitricoxide(NO)andsubstance Pattheapplicationsite,alongwithinhibitionoftheenzyme COXII,producesananti-inflammatoryeffect.Inexperiments ontissuessubjectedpreviouslytoshockwavetherapy, analy-sisunderamicroscopehasdemonstratedintenselyincreased neovascularizationandangiogenesis.
Thepresentstudywasconductedwiththeaimof prospec-tively analyzing the results from shockwave treatment on patientswithrecalcitrantfasciopathy,usingvalidated evalu-ationmethods.
Materials
and
methods
Firstly,aresearchprojectedwasdesignedandsubmittedfor assessmentbytheScientificCommitteeofHospitalIFOR.This wasdulyapproved.
methodssuchasanalgesic andanti-inflammatory medica-tions,physiotherapyandadditionaluseofbracesorinsoles hadbeensystematicallyapplied.
Theinclusion criteria were that the subjects should be patientsofeithersexinwhomadiagnosisofplantarfasciitis hadbeenmadebymeansofclinicalandimagingevaluations, withevolutionofmorethansixmonths.Individualswiththe followingwerenotincluded:otherconcomitantconditionsof thefootandankle;comorbiditiessuchasdiabetesmellitus, neuropathiesorinsensitivefoot;previoussurgery;and non-acceptanceofparticipationinthestudyafterhavingreadthe freeandinformedconsentstatement.
Thus,webuiltupagroupof30patients(36feet),ofwhom 16(53.3%)weremaleand14(47.7%)werefemale,withmean ageof48.37years,rangingfrom33to78years.Withregard tolaterality,weobservedthat16patients(53.3%)presented theconditionontheirleftfootand14(46.7%)ontheirright foot,andthatbilateralityoccurredinsixsituations(20%).The bodymassindex(BMI)rangedfrom20.89to40.60kg/m2,with
ameanof28.48kg/m2.Inoursample,thelengthoftimewith
symptomsrangedfromsixto60months,withameanof13.58 months.
Weperformedradiographicexaminationsonthefeet,with weight-bearing, on the side affected by the condition. We observedthatoutofthe30patientsevaluated,16(53.3%) pre-sentedplantarosteophytesinthecalcaneus.Themeanlength oftheseosteophyteswas0.5cm, fromevaluatingthe radio-graphsonthefeet.
Thepatientsunderwentoneweeklysessionofshockwave therapyforfourconsecutiveweeks.Theapparatususedinthe studywastheSwissDolorcast®,madebytheSwisscompany
EMS.Ageneratorofradialtypewasused,and2000impulses wereproducedineachsession,atapressureof0.18mJ/mm2.
Theapplication sitefor this therapywas the mostpainful pointonthefoot,whichhadbeenindicatedbythepatient. Forthisapplication,wedevelopedadiagramcomposedoffour quadrants(Fig.1).Theoddquadrants(1and3)corresponded totheproximalanddistalmedialplantarregionandtheeven quadrants(2and4)totheproximalanddistallateralplantar regionofthecalcaneus.Weobservedthat17patients(56.6%) indicatedthatquadrantnumber3wasthemostpainfularea, nine(30%)number1,four(13.3%)number2and one(3.3%) number4.
Navicular Base 5.ºMTT
Medial Lateral
1
3 4
2
Fig.1–Diagramoftheplantarregionoftheheel,divided intoquadrants.Quadrant1,distalmedialplantarregion; quadrant2,distallateralplantarregion;quadrant3, proximalmedialplantarregion;quadrant4,proximal lateralplantarregion.
Before
After: 1 month 3 months 6 months
1- Excellent (an excellent result without pain and with complete mobility) 2- Good (a good result with occasional pain)
3- Fair (a fair result with pain after activity) 4- Poor (a poor result with limitation on daily activities)
Fig.2–Roles&Maudsleyevaluation.
Forevaluatingtheresultsafterthepatients’treatment,we usedthescaleoftheAmericanOrthopaedicFootandAnkle Society(AOFAS)(annex1)forevaluatingtheankleand hind-foot,andalsotheRoles&Maudsleyscoreevaluationmethod (Fig.2).Thesequestionnaireswereappliedbyaprofessional whohadnotadministeredtheshockwavetreatment.
Theevaluationsontheplantarfasciawereperformedby asingleimagingdiagnosticsprofessional,using ultrasonog-raphyontheplantarregionofthefeet.Thethicknessofthis anatomicalstructurewasmeasuredatfourtimes:beforethe treatmentand30,90and180daysafterthetreatment.
An ultrasound device with a high-frequencytransducer (7–12MHz)wasused.Atransversalmeasurementin millime-terswasmadeontheplantarfascia,onecentimeterfromthe pointofgreatestacousticshadow,whichcorrespondedtothe calcanealtubercle.Theshockwavetherapywasappliedbya singleprofessional.
Theresultsobtainedwerecompiledandanalyzed statisti-callybyaprofessionalwhowasaspecialistinthisfield.
Results
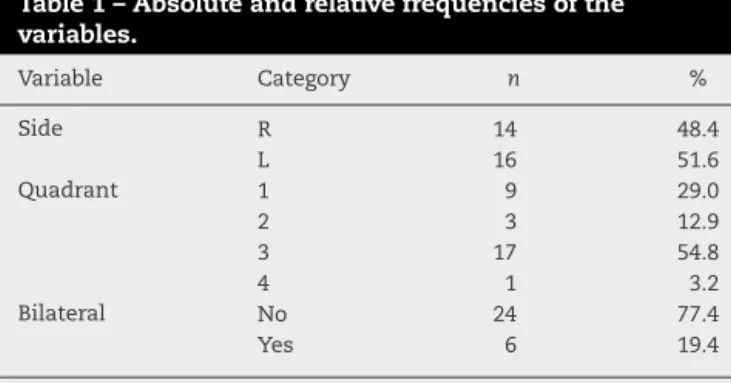
Table1demonstratesthedescriptiveresults,whichtakeinto consideration the side affected by the condition, cases of bilateralityandthequadrantsinwhichtheshockwaveswere applied.
Table2showsthethicknessesoftheplantarfasciaatthe differentevaluationtimesandtheresultfromthestatistical analysis.From analysisofvariancewithrepeated measure-ments,weobservedthatthereweresignificantchangesinthe ultrasonographicresults(p=0.011)betweenthedifferent eval-uationtimes.Theexaminationperformedinthefirstmonth differedfromtheexaminationinthethirdmonth(p=0.003)
Table1–Absoluteandrelativefrequenciesofthe variables.
Variable Category n %
Side R 14 48.4
L 16 51.6
Quadrant 1 9 29.0
2 3 12.9
3 17 54.8
4 1 3.2
Bilateral No 24 77.4
Yes 6 19.4
Table2–Descriptivevaluesfromultrasonography.
Time n Mean SD Minimum Maximum
Before 17 0.68 0.36 0.30 2.00
1month 17 0.64 0.19 0.38 1.10
3months 17 0.60 0.20 0.33 1.10
6months 17 0.57 0.18 0.28 0.97
SD,standarddeviation.
0.00 0.20 0.40 0.60 0.80 1.00 1.20
Before
1 month
3 months
6 months
USG
Fig.3–Graphicalrepresentationoftheevolutionofthe ultrasonography(USG).
andsixthmonth(p=0.003),withvaluesthatweresignificantly
greaterthanintheothertwo.
Fig.3presentstheevolutionoftheultrasonographic thick-nessatthedifferenttimes.
Table3showstheresultsfromanalysisofvariancewith repeatedmeasurements,whichindicatethattherewere sig-nificant changes inthe resultsfrom the AOFAS scale over thecourseoftheevaluations(p<0.001).Thetimebeforethe treatmentpresentedasignificantdifferenceinrelationtothe othertimes(onemonth:p<0.001;threemonths:p<0.001;and sixmonths:p<0.001).Thevaluebefore shockwavetherapy wassignificantlylower than the valuesattheother times. Therewas astatisticallysignificantdifference betweenthe first monthevaluationand the other times(threemonths:
p<0.001;and sixmonths:p<0.001).In thefirst month,the resultsweresignificantlylower than inthethirdand sixth monthsoffollow-up.Thevaluesobtainedinthethirdmonth ofevaluationweresignificantlygreaterthanthosepresented inthesixthmonthofevaluation(p<0.001).
Fig.4showstheresultsfromtheAOFASscaleatthe differ-entevaluationtimes.
Table4demonstratestheresultsfromthestatistical anal-ysis on the Roles & Maudsley scale, using the Friedman
Table3–DescriptivevaluesfromAOFASscale.
Time n Mean SD Minimum Maximum
Before 30 58.87 14.26 36 83
1month 30 68.20 9.97 44 84
3months 30 78.23 13.53 44 97
6months 30 82.83 17.14 36 100
SD,standarddeviation.
0 20 40 60 80 100 120
Before
1 month
3 months
6 months
AOFAS
Fig.4–Graphicalrepresentationoftheevolutionofthe AOFASscale.
nonparametrictest,anditshowsthatthereweresignificant
changesoverthecourseoftheevaluations(p<0.001).Thetime
beforeshockwavetherapydidnotpresentanystatistically
sig-nificantdifferenceinrelationtothefirstmonthofevolution
(p>0.05).Thereweredifferencesinthethirdmonth(p<0.05)
andsixthmonth(p<0.05),withsignificantlygreatervaluesat
thesetwotimes.Theresultsfromthefirstmonthdidnotdiffer
fromtheothertimes(threemonths:p>0.05;andsixmonths:
p>0.05).Inaddition,theresultsfromthethirdmonthdidnot
differfromthosepresentedinthesixthmonth(p>0.05).
Fig.5demonstratestheevolutionoftheresultsfromthe Roles&Maudsleyscaleatthedifferentevaluationtimes.
Discussion
UseofshockwavetherapyhasbeenapprovedbytheFoodand DrugAdministration(FDA),intheUnitedStates,14andbythe
NationalSanitarySurveillanceAgency(AgênciaNacionalde VigilânciaSanitária,ANVISA),inBrazil.
Theexact mechanism forthe effectof shockwave ther-apy on conditions of the locomotor system still remains undefined.
4.00
3.50
3.00
2.50
2.00
R&M
1.50
1.00
Before 1 month 3 months 6 months
Table4–DescriptivevaluesfromRoles&Maudsleyscale.
Time n Mean SD Minimum Maximum P25 Median P75
Before 30 3.28 0.59 2.00 4.00 3.00 3.00 4.00
1month 30 2.79 0.56 2.00 4.00 2.00 3.00 3.00
3months 30 2.31 0.76 1.00 3.00 2.00 2.00 3.00
6months 30 2.14 1.19 1.00 4.00 1.00 2.00 3.50
SD,standarddeviation.
It is believed that shockwaves promote a biological
responseinwhichseveralphenomenaoccur:
neovasculariza-tion,releaseofproliferatingcellnuclearantigen,endothelial
growthfactors,endothelialnitrousoxide15(blockingofnerve
impulses)andmorphogeneticboneprotein.These phenom-ena promoteincreasedblood supply and boneand tendon repair. Localmicrotraumasprovide stimulation and activa-tionofthetissuehealingprocess,whichleadstoactivationof fibroblastproliferationandremovalofcalcareousdeposits.16
Theefficiencyofshockwaveshasbeen demonstrated in a variety of conditions of the locomotor system. Among these,pseudarthrosiscanbehighlighted,withasuccessrate of around 75%. Other indications include: bone necrosis, tendinosis(calcaneal),insertionenthesopathy,epicondylitis, bursitisandcalcareoustendinitisoftheshoulder.17
Sofar,inpreliminarystudies,thesuccessrateregarding pain elimination shown byshockwave therapy has ranged from48%to81%.12
Withregardtothebenefitprovidedbyshockwavetherapy accordingtothetimeelapsedsinceapplication,weobserved thatprogressionofthe successrateshasbeenreported, as follows:57%afterthreemonths,14 48%18 to83%12 aftersix
months,58%after12months19and77.4%after24months.13
Theseresultscorroboratethedataobservedinourstudy, althoughweonlymadeevaluationsuntilthesixthmonthafter application.
Intheliterature,avarietyofbenefitsfromusingthis ther-apeuticoption havebeenindicated.Sincethis methodisa nonoperativeintervention,thepotentialcomplications inher-enttosurgeryceasetoexist.Therecoverytimeissignificantly shorterandtheindividualhasthepossibilityofreturningto hishabitualactivitiesonthedayafterapplication.20Wealso
taketheviewthatthisresourcecouldbeusedasalast pos-sibilitybeforeindicatinganinvasiveprocedure.Successrates comparablewiththoseofsurgeryandotherconventional ther-apieshavebeendemonstratedforshockwavetherapy.8,21
The following are contraindications against applying shockwave therapy: blood dyscrasia,use ofanticoagulants, presenceoftumors,presenceofinfectiousprocessand chil-drenandadolescentswhenthegrowthplateisstillopen.
Regardingthefunctionalaspectofwalking,itwasfoundin onestudythat51%ofthepatientswhounderwentthe treat-mentwerecapableofwalkingwithoutpainsixmonthslater, incomparisonwithindividualswhowerenottreatedorwho receivedplacebo.Afterfiveyears,58%ofthepatientsneeded toundergosurgicalreleaseoftheirplantarfascia,whileonly 13%ofthegrouptreatedwithshockwavetherapyrequiredthis action.22
InanotherstudyinwhichtheauthorsusedtheAOFASscale tocompare theresultsbetweentwogroups,nostatistically
significant differences were found and the patients with chronicplantarfasciitisdidnotdemonstrateanysignificant deficitsofrangeofmotionbeforeorafterthetreatment.23
Inourstudy,whenweusedtheAOFASscale,weobserved that there was a progressive improvement in the results betweenthedifferentevaluationtimes(76.7%),asshownin
Fig.5.
Some studies have indicated that the ideallocation for applying shockwaves would bethe extremity ofthe calca-neusorthecenterofthespurofthisbonestructure,sincethis portionwouldcorrespondtothethickestpartoftheplantar fascia.However,othershaveconsideredthattheideallocation fortheapplicationwouldbethepointoforiginofthepain.24
Inevaluatingtheexactlocationwheretheapplicationis needed,wenotedthatsomeauthorshadcomparedthe ther-apeuticresultsbetweendeterminationoftheapplicationsite bymeansoffluoroscopyandthroughthepatient’sownreport. Theresultwasthattherewasnosignificantdifferencein clin-icalevolutionwhendifferentmethodswereusedtoidentify thebestlocation,andthesuccessrateswereconsideredtobe excellentorgood,accordingtothecriteriaofRoles&Maudsley, threemonthsaftertheapplication.24
Ourresultsweresimilarwhenweusedthesecriteria,with whichweobservedprogressiveimprovement.
From the analysison ourmaterial,we developeda dia-gramconsistingoffourquadrants,inwhichtheregionmost oftenindicatedasbeingpainfulwastheposteromedialregion, whichcorrespondedto54.8%oftheareasofapplication.We considerthatthismethodologyisreproducibleandthatitgave risetofavorableratesofgoodresults.
Throughthis,itcanbesuggestedthatuseofshockwave therapy should be considered to be a therapeutic option. Togetherwithshockwavetherapy,exercisesshouldbedone athomeinordertostretchtheposteriorchain.Studieshave demonstratedthattheresultsobtainedthroughconcomitant useofshockwavetherapyandstretchingoftheposteriorchain aresuperiortothosedoneseparately.
Inanotherstudy,magneticresonance imagingwasused tostructurally evaluatethe plantarfasciathicknessamong asymptomaticpatientswhohadpreviouslyundergoneopen orendoscopicreleaseoftheplantarfascia.Thethicknessof this structurewastwotothreetimes greaterthan normal, despitecompleteresolutionoftheperifascialedemaand plan-tarfasciitis.25
stretchingoftheplantarfascia,causedbythemalleabilityand elasticityintrinsictothisstructure.
Throughthisresource,wewereunabletoassesswhether the heel spur had any influence on the distribution and absorptionofshockwaves.
However,weemphasizethatthe highcostsofmagnetic resonanceimagingmaybediminishedthroughusing ultra-sound.
Fromourstudy,wetaketheviewthatshockwavetherapy canbeconsideredtobeanimportantinstrumentforprimary oradjuvanttreatmentofchronicplantarfasciitis,whenallied withconventionaltherapies.Weconsiderthatthis method-ology issafeand noninvasive, does notpresent significant complicationsandpromotesrehabilitationandanearlyreturn tohabitualactivities.
In a society in which the pace of work is increasing alarmingly,fewindividuals are abletoremain absentfrom workactivitiesforprolongedperiods.Inthisregard, shock-wavetherapywasshowntobeaneffectiveresource,through avoidingtheneedforasurgicalprocedurethatwouldleave them off work for a long period. Another important fac-tortobeconsideredisthatsurgicaltreatmentimplieshigh costs.
Conclusion
Thisstudyshowed thattherewasastatisticallysignificant decreaseinthethicknessoftheplantarfasciainthepatients whounderwentshockwavetherapy(p=0.011).
According to the AOFAS scale for the hindfoot and the Roles & Maudsley scale, the patients in this study achievedstatisticallysignificantimprovementsintheirscores (p<0.001).
Conflicts
of
interest
Theauthorsdeclarenoconflictsofinterest.
Appendix
A.
AOFASscaleforclinicalevaluationoftheankleandhindfoot
Parameter
1.Pain(40points)
None 40
Mild,occasional 30
Moderate,everyday 20
Severe,almostalwayspresent 0
2.Function(50points)
2.1.Limitationonactivitiesandneedforsupport Nolimitations;nosupports 10 Nolimitationsonactivities,recreational
limitations;nosupports
7
Limitationondailyandrecreational activities;useofstick
4
Significantlimitationondailyactivities; useofcrutches,walkingframeor wheelchair
0
2.2.Maximumwalkingdistance(inblocks)
Morethan6 5
From4to6 4
From1to3 2
Lessthan1 0
2.3.Walkingsurface
Nodifficultyonanysurface 5 Somedifficultyonuneven
ground,stairsorslopes
3
Severedifficultyonuneven ground,stairsorslopes
0
2.4.Gaitabnormalities
Noneormild 8
Obvious 4
Severe 0
2.5.Sagittalmobility(flexion+extension) Normalorminimallimitation
(30◦ormore)
8
Moderatelimitation(15to29◦) 4 Severelimitation(lessthan15◦) 0 2.6.Mobilityofhindfoot(inversionandeversion)
Normalormildlimitation(75to 100%)
6
Moderatelimitation(25to74%) 3 Severelimitation(lessthan25%) 0 2.7.Stabilityofankleandhindfoot
(anteroposterior+varus-valgus)
Stable 8
Unstable 0
3.Alignment(10points)
Good–plantigradefootwith ankleandhindfootaligned
10
Fair–plantigradefootwith somemisalignmentand withoutpain
5
Poor–non-plantigradefootwith significantmisalignmentand symptoms
0
r
e
f
e
r
e
n
c
e
s
1.JardeO,DieboldP,HavetE,BouluG,VernoisJ.Degenerative lesionsoftheplantarfascia:surgicaltreatmentby fasciectomyandexcisionoftheheelspur:areporton38 cases.ActaOrthopBelg.2003;69(3):267–74.
2.LeachRE,SeaveyMS,SalterDK.Resultsofsurgeryinathletes withplantarfasciitisFootAnkle.1986;7(3):156–61.
3.LemontH,AmmiratiKM,UsenN.Plantarfasciitis:a degenerativeprocess(fasciosis)withoutinflammation.JAm PodiatrMedAssoc.2003;93(3):234–7.
4.GillLH.Plantarfasciitis:diagnosisandconservative management.JAmAcadOrthopSurg.1997;5(2):109–17.
5.SchepsisAA,LeachRE,GorzycaJ.Plantarfasciitis.Etiology, treatment,surgicalresults,andreviewoftheliterature.Clin OrthopRelatRes.1991;(266):85–96.
7. FureyJG.Plantarfasciitis:thepainfulheelsyndrome.JBone JointSurgAm.1975;57(5):672–3.
8. MartinRL,IrrgangMS,ContiSF.Outcomestudyofsubjects withinsertionalplantarfasciitis.FootAnkleInt.
1998;19(12):803–11.
9. ShikoffMD,FiguraMA,PostarSE.Aretrospectivestudyof195 patientswithheelpain.JAmPodiatrMedAssoc.1986;76:71–5.
10.WolginM,CookC,GrahamC,MauldinD.Conservative treatmentofplantarheelpain:long-termfollow-up.Foot AnkleInt.1994;15(3):97–102.
11.BarrettSL,DaySV,PignettiTT,RobinsonLB.Endoscopic plantarfasciotomy:amulti-surgeonprospectiveanalysisof 652cases.JFootAnkleSurg.1995;34(4):400–6.
12.HammerDS,RuppS,KreutzA,PapeD,KohnD,SeilR. Extracorporealshockwavetherapy(ESWT)inpatientswith chronicproximalplantarfasciitis.FootAnkleInt.
2002;23(4):309–13.
13.RompeJD,HopfC,NafeB,BurgerR.Low-energy extracorporealshockwavetherapyforpainfulheel:a prospectivecontrolledsingle-blindstudy.ArchOrthop TraumaSurg.1996;115(2):75–9.
14.OgdenJA,AlvarezR,LevittR,LeeCrossGL,MarlowM.Shock wavetherapyforchronicproximalplantarfasciitis.Clin OrthopRelatRes.2001;387:47–59.
15.ThielM.Applicationofshockwavesinmedicine.ClinOrthop RelatRes.2001;387:18–21.
16.KayaBK.Plantarfasciitisinathletes.JSportRehabil. 1996;5(4):305–20.
17.Benton-WeilW,BorrelliAH,WeilJrLS,WeilSrLS. Percutaneousplantarfasciectomy:aminimallyinvasive
procedureforrecalcitrantplantarfasciitis.JFootAnkleSurg. 1998;37(4):269–72.
18.RompeJD,KullmerK,EyselP,RiehleHM,BurgerR,NafeB. NiedrigenergetischeextrakorporaleStobwellentherapie (ESWT)beimplantarenfersensporn.OrthopPraxis. 1996;32(4):271–5.
19.KrischekO,RompeJD,HerbsthoferB,NafeB.
Symptomatischeniedrig-energetischeStobwellentherapiebei Fersenschmerzenundradiologischnachweisbaremplantaren Fersen-sporn.ZOrthop.1998;136:169–74.
20.OgdenJA,AlvarezRG,MarlowM.Shockwavetherapyfor chronicplantarfasciitis:ameta-analysis.FootAnkleInt. 2002;23(4):301–8.
21.DaviesMS,WeissGA,SaxbyTS.Plantarfasciitis:how successfulissurgicalintervention?FootAnkleInt. 1999;20(12):803–7.
22.LeagueAC.Currentconceptsreview:plantarfasciitis.Foot AnkleInt.2008;29(3):358–66.
23.TheodoreGH,MatthiasB,AmendolaA,BachmannC,Fleming LL,ZingasC.Extracorporealshockwavetherapyforthe treatmentofplantarfasciitis.FootAnkleInt.2004;25(5): 290–7.
24.DorotkaR,SabetiM,Jimenez-BojE,GollA,SchubertS,Trieb K.Locationmodalitiesforfocusedextracorporealshockwave applicationinthetreatmentofchronicplantarfasciitis.Foot AnkleInt.2006;27(11):943–7.